
Scar Tissue after a Cesarean Section—The Management of Different Complications in Pregnant Women


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
- 1
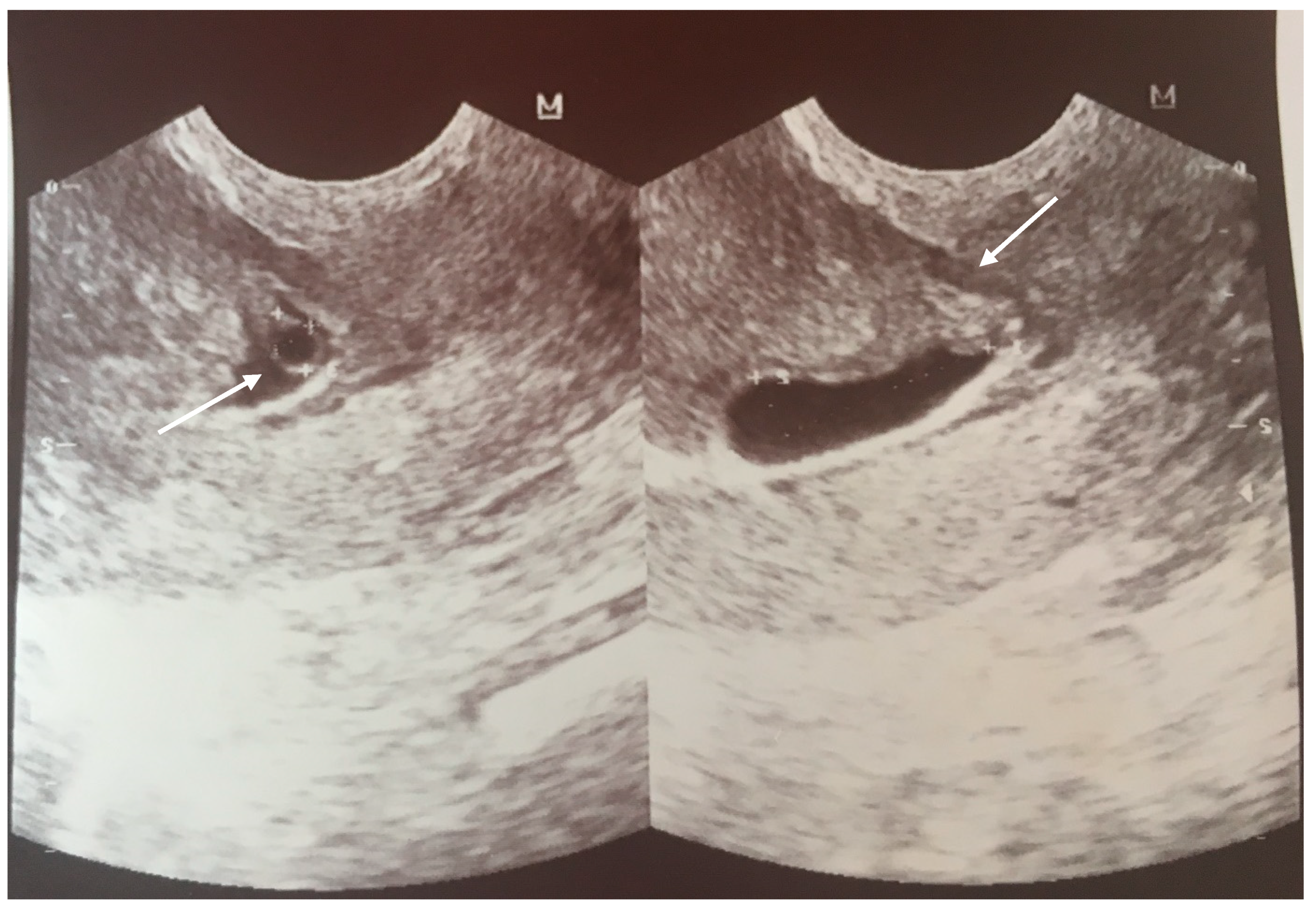
- an empty uterine cavity with clear endometrium and empty endocervical canal,
- 2
- the detection of a gestational sac within the anterior lower segment of the uterus embedded in the cesarean scar,
- 3
- an absent or thin (<5 mm) myometrium layer between the gestational sac and the bladder,
- 4
- 5
- the pathologies of the adnexa should be excluded, and there should be no detection of fluid in the Douglas pouch unless in the case of a massive hemorrhage or rupture of the uterus [5].
1.1. Case 1
1.2. Case 2
2. Discussion
- Expectant management only after detailed explanation about risks (rupture, bleeding palcenta percreta)
- Conservative methods like medical treatment, or/and mechanical interventions depending on what the facilities can provide
- The decision for the procedure is influenced by the available management and expertise of the center when complications occur.
3. Conclusions
4. Clinical Implication
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CS | cesarean section |
| CSP | cesarean scar pregnancy |
| CTGF | connective tissue growth factor |
| GS | gestational sac |
| FGF | fibroblast growth factor |
| LUS | lower uterine segment |
| PAS | placenta accrete spectrum |
| RMT | residual myometrial thickness |
| wks | weeks’ gestation |
| VBAC | vaginal birth after a cesarean section |
| VEGF | vascular endothelial growth factor |
| TNF-α | tumor necrosis factor α |
| TGF-ß | transforming growth factor β |
References
- Donnez, O.; Donnez, J.; Orellana, R.; Dolmans, M.M. Gynecological and obstetrical outcomes after laparoscopic repair of a cesarean scar defect in a series of 38 women. Fertil. Steril. 2017, 107, 289–296.e2. [Google Scholar] [CrossRef]
- Harb, H.M.; Knight, M.; Bottomley, C.; Overton, C.; Tobias, A.; Gallos, I.D.; Shehmar, M.; Farquharson, R.; Horne, A.; Latthe, P.; et al. Caesarean scar pregnancy in the UK: A national cohort study. BJOG 2018, 125, 1663–1670. [Google Scholar] [CrossRef]
- Stasiełuk, A.; Langowicz, I.; Kosińska-Kaczyńska, K.; Pietrzak, B.; Wielgoś, M. Is the epidemic of cesarean sections the result of more liberal indications? Ginekol. Pol. 2012, 83, 604–608. [Google Scholar]
- Uharček, P.; Brešťanský, A.; Ravinger, J.; Máňová, A.; Zajacová, M. Sonographic assessment of lower uterine segment thickness at term in women with previous cesarean delivery. Arch. Gynecol. Obstet. 2015, 292, 609–612. [Google Scholar] [CrossRef]
- Kwaśniewska, A.; Stupak, A.; Krzyżanowski, A.; Pietura, R.; Kotarski, J. Cesarean scar pregnancy: Uterine artery embolization combined with a hysterectomy at 13 weeks’ gestation—A case report and review of the literature. Ginekol. Pol. 2014, 85, 961–967. [Google Scholar] [CrossRef]
- Naji, O.; Daemen, A.; Smith, A.; Abdallah, Y.; Saso, S.; Stalder, C.; Sayasneh, A.; McIndoe, A.; Ghaem-Maghami, S.; Timmerman, D.; et al. Changes in Cesarean section scar dimensions during pregnancy: A prospective longitudinal study. Ultrasound Obstet. Gynecol. 2013, 41, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Varner, M. Cesarean Scar Imaging and Prediction of Subsequent Obstetric Complications. Clin. Obstet. Gynecol. 2012, 55, 988–996. [Google Scholar] [CrossRef]
- Pollio, F.; Staibano, S.; Mascolo, M.; Salvatore, G.; Persico, F.; De Falco, M.; Di Lieto, A. Uterine dehiscence in term pregnant patients with one previous cesarean delivery: Growth factor immunoexpression and collagen content in the scarred lower uterine segment. Am. J. Obstet. Gynecol. 2006, 194, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Roberge, S.; Demers, S.; Girard, M.; Vikhareva, O.; Markey, S.; Chaillet, N.; Moore, L.; Paris, G.; Bujold, E. Impact of uterine closure on residual myometrial thickness after cesarean: A randomized controlled trial. Am. J. Obstet. Gynecol. 2016, 214, 507.e1–507.e6. [Google Scholar] [CrossRef] [PubMed]
- Pomorski, M.; Fuchs, T.; Rosner-Tenerowicz, A.; Zimmer, M. Standardized ultrasonographic approach for the assessment of risk factors of incomplete healing of the cesarean section scar in the uterus. Euro. J. Obstet. Gynecol. Reprod. Biol. 2016, 205, 141–145. [Google Scholar] [CrossRef]
- Osser, O.V.; Jokubkiene, L.; Valentin, L. High prevalence of defects in Cesarean section scars at transvaginal ultrasound examination. Ultrasound Obstet. Gynecol. 2009, 34, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Vachon-Marceau, C.; Demers, S.; Bujold, E.; Roberge, S.; Gauthier, R.J.; Pasquier, J.-C.; Girard, M.; Chaillet, N.; Boulvalin, M.; Jastrow, N. Single versus double-layer uterine closure at cesarean: Impact on lower uterine segment thickness at next pregnancy. Am. J. Obstet. Gynecol. 2017, 217, 65.e1–65.e5. [Google Scholar] [CrossRef] [PubMed]
- Rotas, M.A.; Haberman, S.; Levgur, M. Cesarean scar ectopic pregnancies: Etiology, diagnosis, and management. Obstet. Gynecol. 2006, 107, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Overview. Ectopic Pregnancy and Miscarriage: Diagnosis and Initial Management: Summary of Updated NICE Guidance. Available online: https://www.nice.org.uk/guidance/ng126 (accessed on 19 April 2020).
- McLaren, R.; McCalla, S.; Irani, M. Conservative Management of Cesarean Scar Ectopic Pregnancy with Fetal Heart Activity and a Very High β-hCG. Case Rep. Obstet. Gynecol. 2015, 2015, 3. [Google Scholar]
- Timor-Tritsch, I.E.; Monteagudo, A.; Santos, R.; Tsymbal, T.; Pinetda, G.; Arslan, A.A. The diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am. J. Obstet. Gynecol. 2012, 207, 44.e1–44.e13. [Google Scholar] [CrossRef]
- Osborn, D.A.; Williams, T.R.; Craig, B.M. Cesarean scar pregnancy: Sonographic and magnetic resonance imaging findings, complications, and treatment. J. Ultrasound Med. 2012, 31, 1449–1456. [Google Scholar] [CrossRef]
- Basic, E.; Basic-Cetkovic, V.; Kozaric, H.; Rama, A. Ultrasound evaluation of uterine scar after cesarean section. Acta Inform. Med. 2012, 20, 149–153. [Google Scholar] [CrossRef]
- Practice Bulletin No. 175. In Ultrasound in Pregnancy Obstetrics & Gynecology; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2016; Volume 128, pp. 241–256.
- Alalfy, M.; Osman, O.M.; Salama, S.; Lasheen, Y.; Soliman, M.; Fikry, M.; Ramadan, M.; Alaa, D.; Elshemy, S.; Abdella, R. Evaluation of the Cesarean Scar Niche In Women With Secondary Infertility Undergoing ICSI Using 2D Sonohysterography Versus 3D Sonohysterography and Setting a Standard Criteria; Alalfy Simple Rules for Scar Assessment by Ultrasound To Prevent Health Problems for Women. Int. J. Womens Health 2020, 12, 965–974. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Cali, G.; Palacios-Jaraquemada, J.M.; Maymon, R.; Arslan, A.A.; Patil, N.; Popiolek, D.; Mittal, K.R. Cesarean scar pregnancy and early placenta accreta share common histology. Ultrasound Obstet. Gynecol. 2014, 43, 383–395. [Google Scholar] [CrossRef]
- Malik, M.F.; Hoyos, L.R.; Rodriguez-Kovacs, J.; Gillum, J.; Johnson, S.C. Placenta Increta Complicating Persistent Cesarean Scar Ectopic Pregnancy following Failed Excision with Subsequent Preterm Cesarean Hysterectomy. Case Rep. Obstet. Gynecol. 2016, 2016, 4071840. [Google Scholar] [CrossRef]
- Cignini, P.; Giorlandino, M.; Caserta, L.; Dominici, L.; Giorlandino, C. The importance of early diagnosis in cesarean scar pregnancy. J. Prenat. Med. 2007, 1, 29–31. [Google Scholar] [PubMed]
- Elep, R.V.; Dalawangbayan, A.M.L.F. Evolution of a cesarean scar pregnancy into a placenta accreta at term: A case report. PJOG 2017, 41, 29–36. [Google Scholar]
- Cecchini, F.; Tassi, A.; Londero, A.P.; Baccarini, G.; Driul, L.; Xodo, S. First Trimester Uterine Rupture: A Case Report and Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 2976. [Google Scholar] [CrossRef]
- Sinha, P.; Mishra, M. Caesarean scar pregnancy: A precursor of placenta percreta/accrete. J. Obstet. Gynaecol. 2012, 32, 621–623. [Google Scholar] [CrossRef] [PubMed]
- Calì, G.; Timor-Tritsch, I.E.; Palacios-Jaraquemada, J.; Monteaugudo, A.; Buca, D.; Forlani, F.; Familiari, A.; Scambia, G.; Acharya, G.; D’Antonio, F. Outcome of Cesarean scar pregnancy: A systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2017, 51, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Tao, X.; Zhu, Y.C.; Yu, X.L.; Zou, Y.H.; Yang, H.X. Cesarean scar pregnancy analysis of 42 cases. Zhonghua Fu Chan Ke Za Zhi 2009, 44, 566–569. [Google Scholar] [PubMed]
- Magnus, M.C.; Wilcox, A.J.; Morken, N.H.; Weinberg, C.R.; Håberg, S.E. Role of maternal age and pregnancy history in risk of miscarriage: Prospective register based study. BMJ 2019, 364, l869. [Google Scholar] [CrossRef]
- Vissers, J.; Hehenkamp, W.; Lambalk, C.B.; Huirne, J.A. Post-Caesarean section niche-related impaired fertility: Hypothetical mechanisms. Hum. Reprod. 2020, 35, 1484–1494. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Calì, G.; D’Antonio, F.; Kaelin Agten, A. Cesarean Scar Pregnancy. Obstet. Gynecol. Clin. 2019, 46, 797–811. [Google Scholar] [CrossRef]
- Paterson, K.; Odejinmi, F.; Shahid, A. Clinical Dilemmas and Risks of Misdiagnosis and Mismanagement Associated with Endogenous Caesarean Scar Pregnancy: A Case Series and Literature Review. Glob. J. Reprod. Med. 2017, 3, 555602. [Google Scholar] [CrossRef][Green Version]
- Nezhat, C.; Falik, R.; Li, A. Surgical management of niche, isthmocele, uteroperitoneal fistula, or cesarean scar defect: A critical rebirth in the medical literature. Fertil. Steril. 2017, 107, 69–71. [Google Scholar] [CrossRef]
- Vikhareva Osser, O.; Valentin, L. Risk factors for incomplete healing of the uterine incision after caesarean section. BJOG 2010, 117, 1119–1126. [Google Scholar] [CrossRef]
- Cohen, A.; Cohen, Y.; Laskov, I.; Maslovitz, S.; Lessing, J.B.; Many, A. Persistent abdominal pain over uterine scar during labor as a predictor of delivery complications. Inter. J. Gynecol. Obstet. 2013, 123, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Boujenah, J.; Tigaizin, A.; De La Hosseraye, C.; Oldani, E.; Carbillon, L. From cesearean scar dehiscence to large incomplete uterine rupture in the second trimester. Gynecol. Obstet. Fertil. 2015, 43, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Dosedla, E.; Calda, P. Can the final sonographic assessment of the cesarean section scar be predicted 6 weeks after the operation? Taiw. J. Obstet. Gynecol. 2016, 55, 718–720. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jacobson, M.T.; Osias, J.; Velasco, A.; Charles, R.; Nezhat, C. Laparoscopic repair of a uteroperitoneal fistula. JSLS 2003, 7, 367–369. [Google Scholar] [CrossRef][Green Version]
- Hayakawa, H.; Itakura, A.; Mitsui, T.; Okada, M.; Suzuki, M.; Tamakoshi, K.; Kikkawa, F. Methods for myometrium closure and other factors impacting effects on cesarean section scars of the uterine segment detected by the ultrasonography. Acta Obstet. et Gynecol. Scand. 2006, 85, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Yasmin, S.; Sadaf, J.; Fatima, N. Impact of methods for uterine incision closure on repeat cesarean section scar of lower uterine segment. J. Coll. Physicians Surg. Pak. 2011, 21, 522–526. [Google Scholar]
- Sevket, O.; Ates, S.; Molla, T.; Ozkal, F.; Uysal, O.; Dansuk, R. Hydrosonographic assessment of the effects of 2 different suturing techniques on healing of the uterine scar after cesarean delivery. Int. J. Gynaecol. Obstet. 2014, 125, 219–222. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stupak, A.; Kondracka, A.; Fronczek, A.; Kwaśniewska, A. Scar Tissue after a Cesarean Section—The Management of Different Complications in Pregnant Women. Int. J. Environ. Res. Public Health 2021, 18, 11998. https://doi.org/10.3390/ijerph182211998
Stupak A, Kondracka A, Fronczek A, Kwaśniewska A. Scar Tissue after a Cesarean Section—The Management of Different Complications in Pregnant Women. International Journal of Environmental Research and Public Health. 2021; 18(22):11998. https://doi.org/10.3390/ijerph182211998
Chicago/Turabian StyleStupak, Aleksandra, Adrianna Kondracka, Agnieszka Fronczek, and Anna Kwaśniewska. 2021. "Scar Tissue after a Cesarean Section—The Management of Different Complications in Pregnant Women" International Journal of Environmental Research and Public Health 18, no. 22: 11998. https://doi.org/10.3390/ijerph182211998
APA StyleStupak, A., Kondracka, A., Fronczek, A., & Kwaśniewska, A. (2021). Scar Tissue after a Cesarean Section—The Management of Different Complications in Pregnant Women. International Journal of Environmental Research and Public Health, 18(22), 11998. https://doi.org/10.3390/ijerph182211998