
Health Patterns among Migrant and Non-Migrant Middle- and Older-Aged Individuals in Europe—Analyses Based on Share 2004–2017


Abstract
:1. Introduction
2. Methods
2.1. Data
2.2. Measures
2.3. Analyses
3. Results
3.1. Associations between Health Indicators, Age, Gender and Migrant Status
3.2. Subgroup Analyses and Time Trends
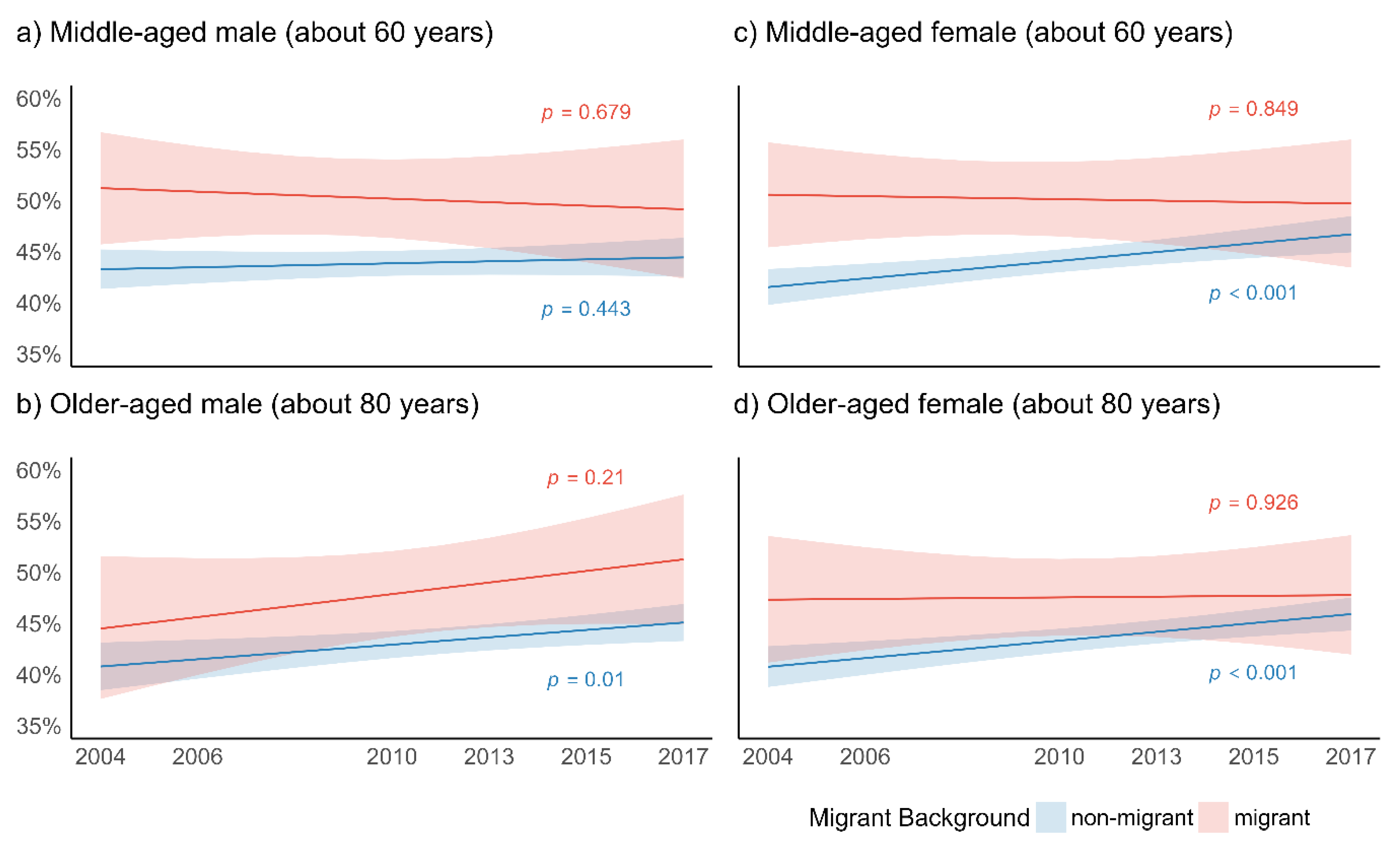
3.2.1. Global Activity Limitation Index
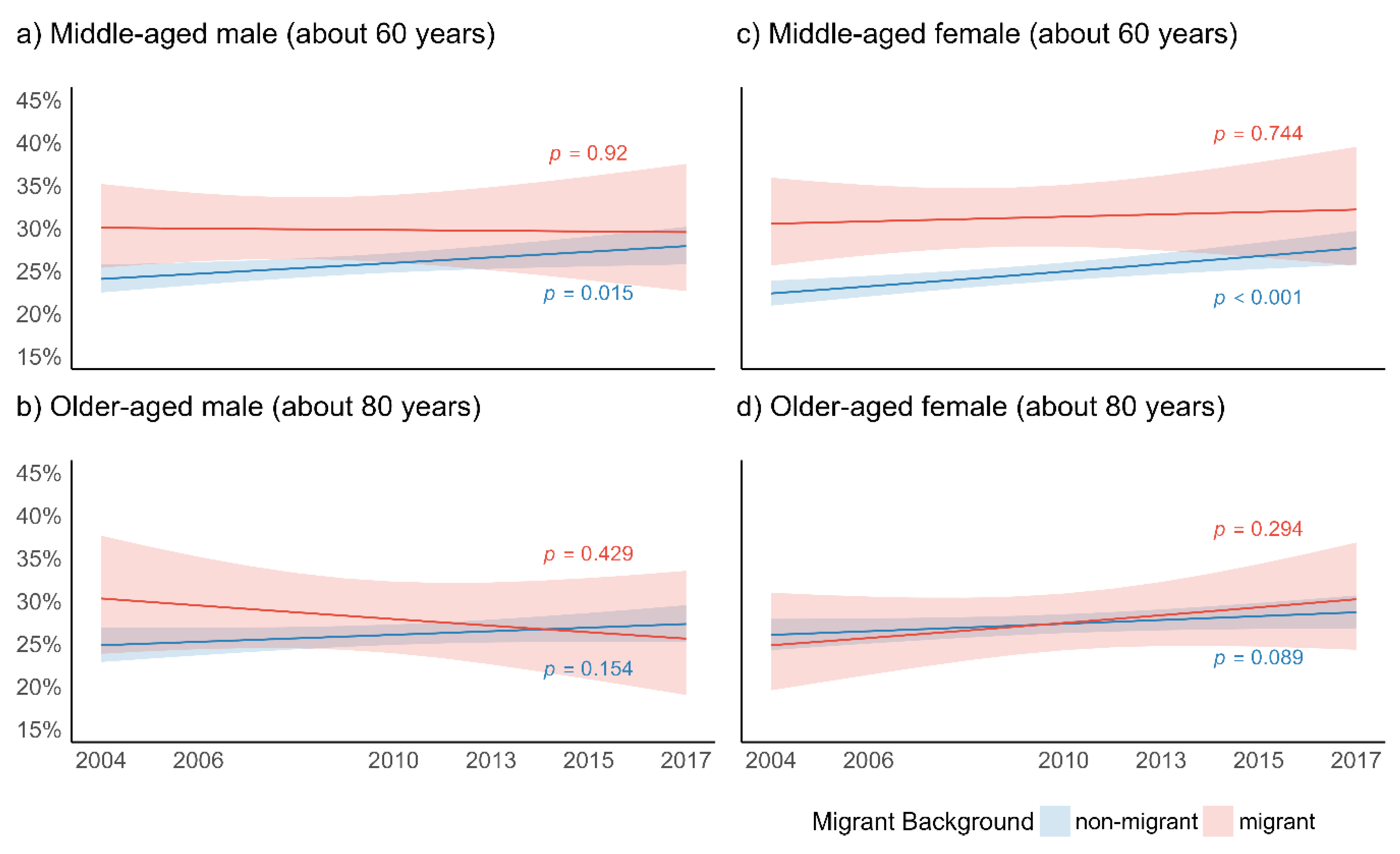
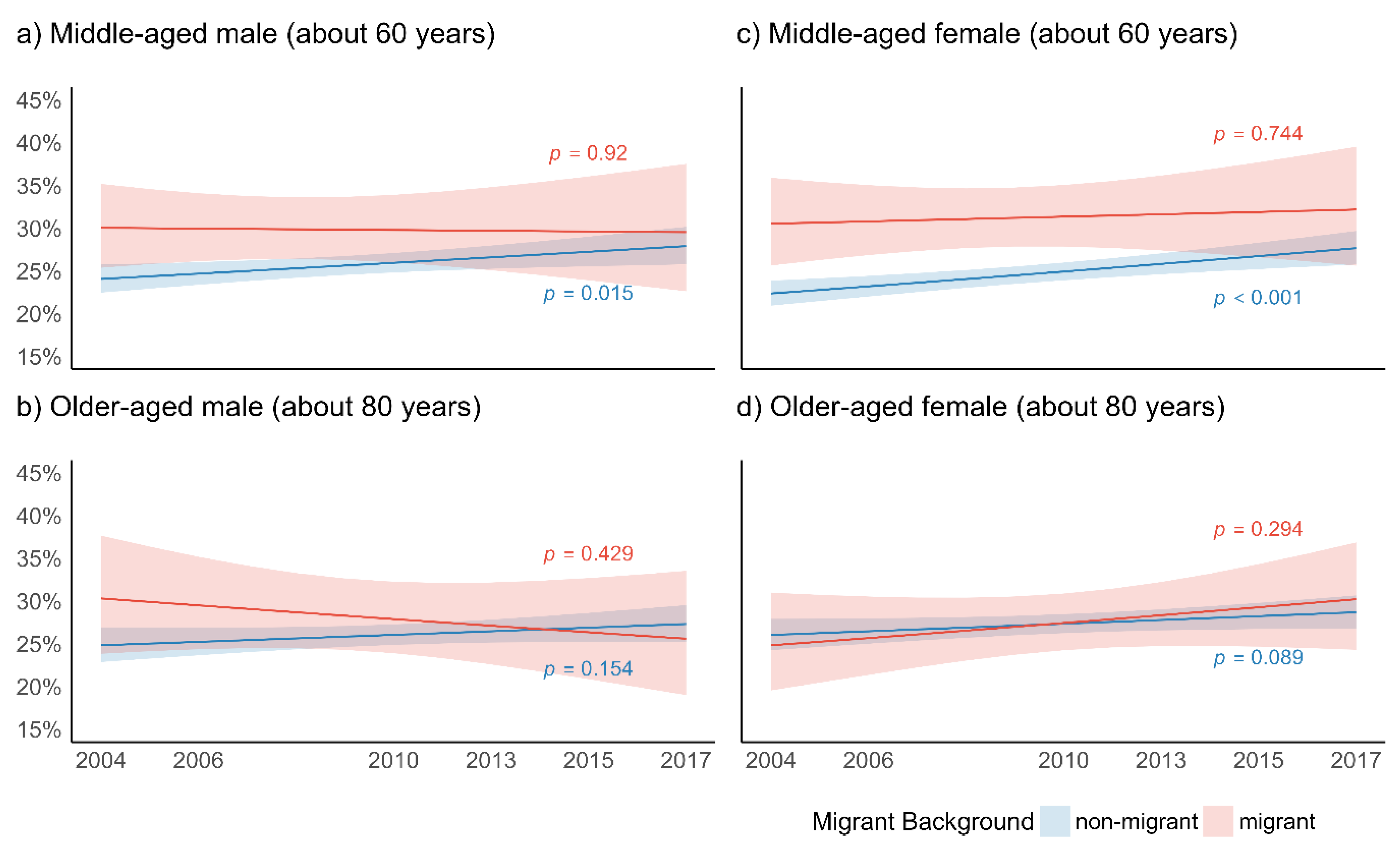
3.2.2. Depression
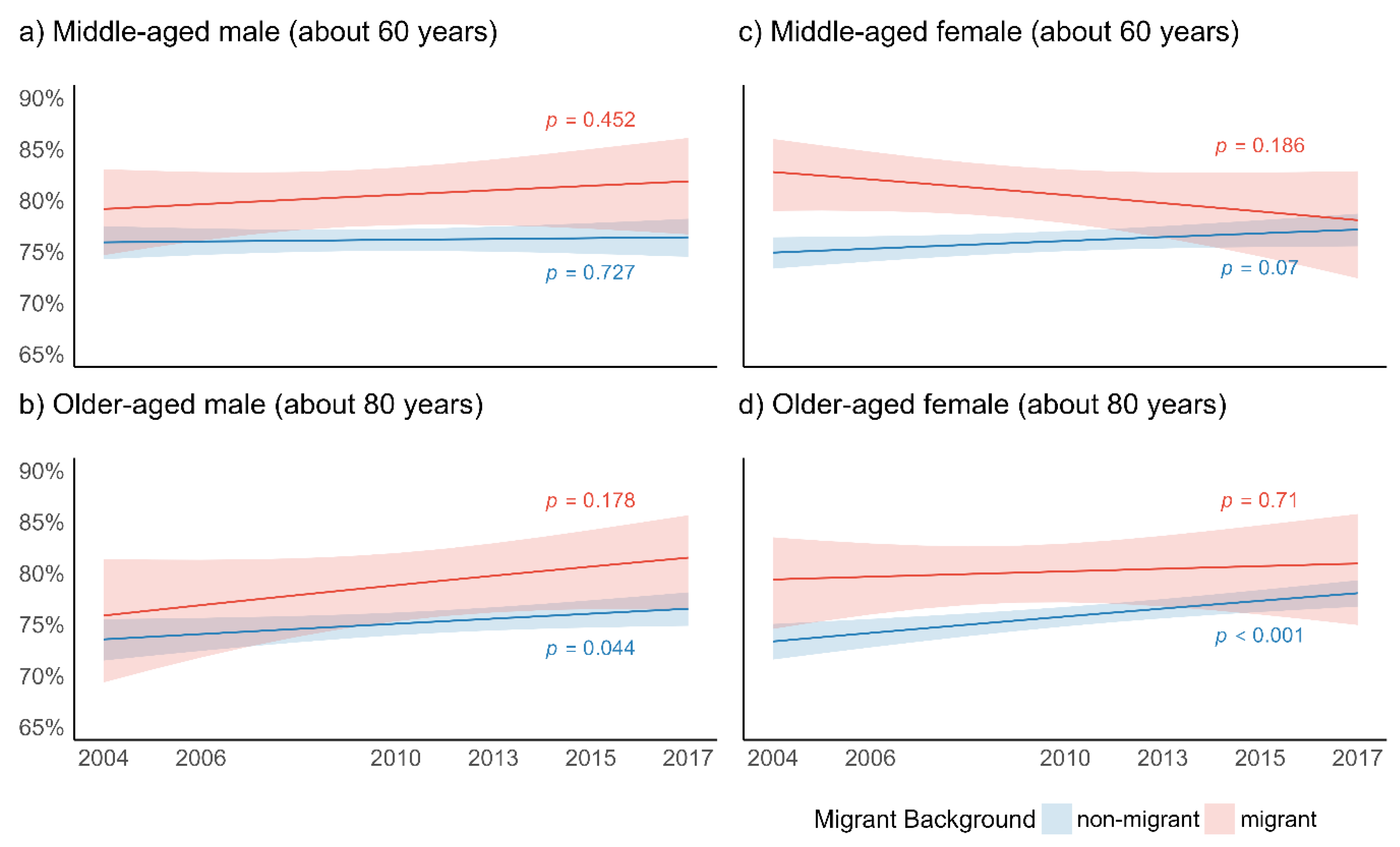
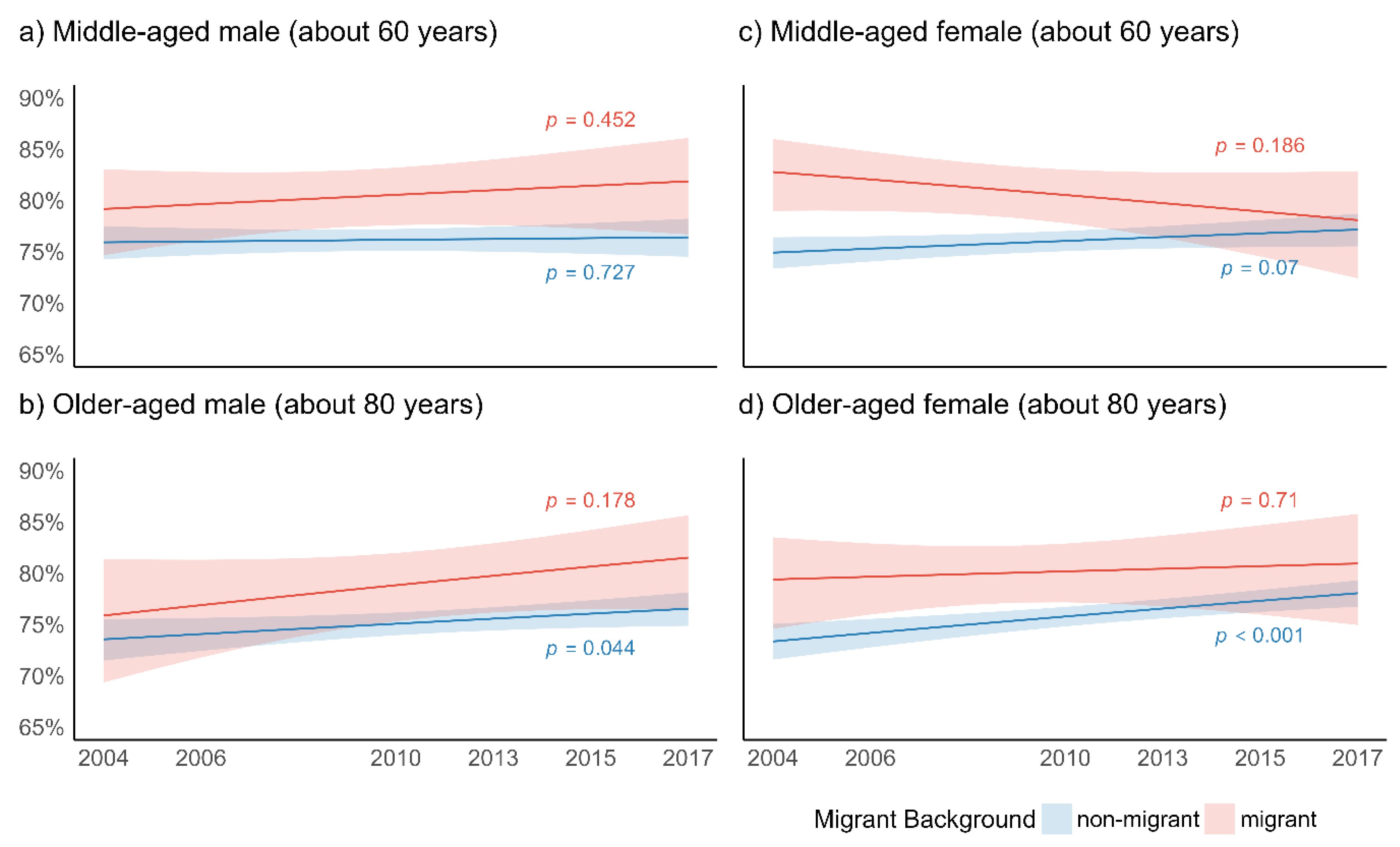
3.2.3. Self-Rated Health
4. Discussion
4.1. Summary
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lanzieri, G. Fewer, Older and Multicultural? Projections of the EU Populations by Foreign/National Background. In Eurostat Methodologies and Working Papers; European Union: Luxmburg, 2011. [Google Scholar] [CrossRef]
- Migration Data Portal. Total Number of International Migrants at Mid-Year 2020. Available online: https://www.migrationdataportal.org/data?m=1&i=stock_abs_&t=2020 (accessed on 24 August 2021).
- Razum, O.; Zeeb, H.; Akgün, H.S.; Yilmaz, S. Low Overall Mortality of Turkish Residents in Germany Persists and Extends into a Second Generation: Merely a Healthy Migrant Effect? Trop. Med. Int. Health 1998, 3, 297–303. [Google Scholar] [CrossRef]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and Health in an Increasingly Diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Gkiouleka, A.; Huijts, T. Intersectional Migration-Related Health Inequalities in Europe: Exploring the Role of Migrant Generation, Occupational Status & Gender. Soc. Sci. Med. 2020, 267, 113218. [Google Scholar] [CrossRef] [PubMed]
- La Parra-Casado, D.; Stornes, P.; Solheim, E.F. Self-Rated Health and Wellbeing among the Working-Age Immigrant Population in Western Europe: Findings from the European Social Survey (2014) Special Module on the Social Determinants of Health. Eur. J. Public Health 2017, 27 (Suppl. S1), 40–46. [Google Scholar] [CrossRef]
- Arnold, M.; Razum, O.; Coebergh, J.-W. Cancer Risk Diversity in Non-Western Migrants to Europe: An Overview of the Literature. Eur. J. Cancer 2010, 46, 2647–2659. [Google Scholar] [CrossRef] [PubMed]
- Gkiouleka, A.; Avrami, L.; Kostaki, A.; Huijts, T.; Eikemo, T.A.; Stathopoulou, T. Depressive Symptoms among Migrants and Non-Migrants in Europe: Documenting and Explaining Inequalities in Times of Socio-Economic Instability. Eur. J. Public Health 2018, 28 (Suppl. S5), 54–60. [Google Scholar] [CrossRef] [PubMed]
- Lebano, A.; Hamed, S.; Bradby, H.; Gil-Salmerón, A.; Durá-Ferrandis, E.; Garcés-Ferrer, J.; Azzedine, F.; Riza, E.; Karnaki, P.; Zota, D.; et al. Migrants’ and Refugees’ Health Status and Healthcare in Europe: A Scoping Literature Review. BMC Public Health 2020, 20, 1039. [Google Scholar] [CrossRef] [PubMed]
- Janssen, F.; Bardoutsos, A.; El Gewily, S.; De Beer, J. Future Life Expectancy in Europe Taking into Account the Impact of Smoking, Obesity, and Alcohol. eLife 2021, 10, e66590. [Google Scholar] [CrossRef] [PubMed]
- Aichberger, M.; Schouler-Ocak, M.; Mundt, A.; Busch, M.; Nickels, E.; Heimann, H.; Ströhle, A.; Reischies, F.; Heinz, A.; Rapp, M. Depression in Middle-Aged and Older First Generation Migrants in Europe: Results from the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur. Psychiatry 2010, 25, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Lanari, D.; Bussini, O. International Migration and Health Inequalities in Later Life. Ageing Soc. 2012, 32, 935–962. [Google Scholar] [CrossRef]
- Reus-Pons, M.; Mulder, C.H.; Kibele, E.U.; Janssen, F. Differences in the Health Transition Patterns of Migrants and Non-Migrants Aged 50 and Older in Southern and Western Europe (2004–2015). BMC Med. 2018, 16, 57. [Google Scholar] [CrossRef]
- Reus-Pons, M.; Kibele, E.U.; Janssen, F. Differences in Healthy Life Expectancy between Older Migrants and Non-Migrants in Three European Countries over Time. Int. J. Public Health 2017, 62, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.H.; O’Rand, A.M.; Adkins, D.E. Race-Ethnicity and Health Trajectories: Tests of Three Hypotheses across Multiple Groups and Health Outcomes. J. Health Soc. Behav. 2012, 53, 359–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evandrou, M.; Falkingham, J.; Feng, Z.; Vlachantoni, A. Ethnic Inequalities in Limiting Health and Self-Reported Health in Later Life Revisited. J. Epidemiol. Community Health 2016, 70, 653–662. [Google Scholar] [CrossRef] [Green Version]
- Shuey, K.M.; Willson, A.E. Cumulative Disadvantage and Black-White Disparities in Life-Course Health Trajectories. Res. Aging 2008, 30, 200–225. [Google Scholar] [CrossRef]
- Haas, S.; Rohlfsen, L. Life Course Determinants of Racial and Ethnic Disparities in Functional Health Trajectories. Soc. Sci. Med. 2010, 70, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Levchenko, Y. Aging into Disadvantage: Disability Crossover among Mexican Immigrants in America. Soc. Sci. Med. 2021, 285, 114290. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, M.; Razum, O.; Tezcan-Güntekin, H.; Krasnik, A. Aging and Health among Migrants in a European Perspective. Public Health Rev. 2016, 37, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnein, M.; Milewski, N.; Doblhammer, G.; Nusselder, W.J. Health Inequalities of Immigrants: Patterns and Determinants of Health Expectancies of Turkish Migrants Living in Germany. In Health among the Elderly in Germany; Doblhammer, G., Ed.; New Evidence on Disease, Disability and Care Need; Verlag Barbara Budrich: Opladen, Germany, 2015; Volume 46, pp. 157–190. [Google Scholar]
- Milewski, N.; Doblhammer, G. Mental Health among Immigrants: Is There a Disadvantage in Later Life. In Health among the Elderly in Germany; Doblhammer, G., Ed.; New Evidence on Disease, Disability and Care Need; Verlag Barbara Budrich: Opladen, Germany, 2015; Volume 46, pp. 191–212. [Google Scholar]
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 1. Published online 2020. Available online: http://www.share-project.org/data-documentation/waves-overview/wave-1.html (accessed on 14 November 2021).
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 2. Published online 2020. Available online: http://www.share-project.org/data-documentation/waves-overview/wave-2.html (accessed on 14 November 2021).
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 4. Published online 2020. Available online: http://www.share-project.org/data-documentation/waves-overview/wave-4.html (accessed on 14 November 2021).
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 5. Published online 2020. Available online: http://www.share-project.org/data-documentation/waves-overview/wave-5.html (accessed on 14 November 2021).
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 6. Published online 2020. Available online: http://www.share-project.org/data-documentation/waves-overview/wave-6.html (accessed on 14 November 2021).
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 7. Published online 2020. Available online: http://www.share-project.org/data-documentation/waves-overview/wave-7.html (accessed on 14 November 2021).
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S.; SHARE Central Coordination Team. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- SHARE. SHARE Release Guide 1.0.0 of Wave 8; MEA: Munich, Germany, 2021.
- van Oyen, H.; Van der Heyden, J.; Perenboom, R.; Jagger, C. Monitoring Population Disability: Evaluation of a New Global Activity Limitation Indicator (GALI). Soz. Praventivmed. 2006, 51, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.J.; Reischies, F.; Beekman, A.T.; Fuhrer, R.; Jonker, C.; Kivela, S.L.; Lawlor, B.A.; Lobo, A.; Magnusson, H.; Fichter, M.; et al. Development of the EURO-D Scale—A European, Union Initiative to Compare Symptoms of Depression in 14 European Centres. Br. J. Psychiatry 1999, 174, 330–338. [Google Scholar] [CrossRef]
- UNESCO. International Standard Classification of Education ISCED 1997; UNESCO: Paris, France, 1997. [Google Scholar]
- Lumley, T.; Scott, A. Fitting Regression Models to Survey Data. Stat. Sci. 2017, 32, 265–278. [Google Scholar] [CrossRef]
- Bell, A.; Jones, K. Explaining Fixed Effects: Random Effects Modeling of Time-Series Cross-Sectional and Panel Data. Political. Sci. Res. Methods 2015, 3, 133–153. [Google Scholar] [CrossRef] [Green Version]
- Aiken, L.S.; West, S.G. Multiple Regression: Testing and Interpreting Interactions; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- R: A Language and Environment for Statistical Computing. Available online: https://www.gbif.org/tool/81287/r-a-language-and-environment-for-statistical-computing (accessed on 23 September 2021).
- Lumley, T. Complex Surveys: A Guide to Analysis Using R; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Lüdecke, D. Ggeffects: Tidy Data Frames of Marginal Effects from Regression Models. J. Open Source Softw. 2018, 3, 772. [Google Scholar] [CrossRef] [Green Version]
- Lenth, R.V. Emmeans: Estimated Marginal Means Aka Least Square Means. R Package Version 1.6.3. Available online: https://github.com/rvlenth/emmeans (accessed on 31 October 2021).
- Gubernskaya, Z. Age at Migration and Self-Rated Health Trajectories after Age 50: Understanding the Older Immigrant Health Paradox. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 70, 279–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahonen, E.Q.; Benavides, F.G.; Benach, J. Immigrant Populations, Work and Health—A Systematic Literature Review. Scand. J. Work Environ. Health 2007, 33, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Spallek, J.; Zeeb, H.; Razum, O. What Do We Have to Know from Migrants’ Past Exposures to Understand Their Health Status? A Life Course Approach. Emerg. Themes Epidemiol. 2011, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Honkaniemi, H.; Juárez, S.P.; Katikireddi, S.V.; Rostila, M. Psychological Distress by Age at Migration and Duration of Residence in Sweden. Soc. Sci. Med. 2020, 250, 112869. [Google Scholar] [CrossRef]
- Read, S.; Grundy, E.; Foverskov, E. Socio-Economic Position and Subjective Health and Well-Being among Older People in Europe: A Systematic Narrative Review. Aging Ment. Health 2016, 20, 529–542. [Google Scholar] [CrossRef] [Green Version]
- Sadana, R.; Blas, E.; Budhwani, S.; Koller, T.; Paraje, G. Healthy Ageing: Raising Awareness of Inequalities, Determinants, and What Could Be Done to Improve Health Equity. Gerontologist 2016, 56 (Suppl. S2), S178–S193. [Google Scholar] [CrossRef] [Green Version]
- Peixoto, J. Migration and Policies in the European Union: Highly Skilled Mobility, Free Movement of Labour and Recognition of Diplomas. Int. Migr. 2001, 39, 33–61. [Google Scholar] [CrossRef]
- Lulle, A.; Janta, H.; Emilsson, H. Introduction to the Special Issue: European Youth Migration: Human Capital Outcomes, Skills and Competences. J. Ethn. Migr. Stud. 2021, 47, 1725–1739. [Google Scholar] [CrossRef] [Green Version]
- Börsch-Supan, A.; Alcser, K.H. (Eds.) The Survey of Health, Aging and Retirement in Europe-Methodology; Mannheim Research Institute for the Economics of Aging (MEA): Mannheim, Germany, 2005. [Google Scholar]
- Maskileyson, D.; Seddig, D.; Davidov, E. The EURO-D Measure of Depressive Symptoms in the Aging Population: Comparability across European Countries and Israel. Front. Polit. Sci. 2021, 3, 90. [Google Scholar] [CrossRef]
- Bremer, D.; Lüdecke, D.; Vonneilich, N.; von dem Knesebeck, O. Social Relationships and GP Use of Middle-Aged and Older Adults in Europe: A Moderator Analysis. BMJ Open 2018, 8, e018854. [Google Scholar] [CrossRef] [PubMed]
- Singh-Manoux, A.; Martikainen, P.; Ferrie, J.; Zins, M.; Marmot, M.; Goldberg, M. What Does Self Rated Health Measure? Results from the British Whitehall II and French Gazel Cohort Studies. J. Epidemiol. Community Health 2006, 60, 364–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeSalvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality Prediction with a Single General Self-Rated Health Question. A Meta-Analysis. J. Gen. Intern. Med. 2006, 21, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miilunpalo, S.; Vuori, I.; Oja, P.; Pasanen, M.; Urponen, H. Self-Rated Health Status as a Health Measure: The Predictive Value of Self-Reported Health Status on the Use of Physician Services and on Mortality in the Working-Age Population. J. Clin. Epidemiol. 1997, 50, 517–528. [Google Scholar] [CrossRef]
- Johnson, R.J.; Wolinsky, F.D. The Structure of Health Status among Older Adults: Disease, Disability, Functional Limitation, and Perceived Health. J. Health Soc. Behav. 1993, 34, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Wendt, C. Mapping European Healthcare Systems: A Comparative Analysis of Financing, Service Provision and Access to Healthcare. J. Eur. Soc. Policy 2009, 19, 432–445. [Google Scholar] [CrossRef] [Green Version]
- Cvajner, M.; Echeverría, G.; Sciortino, G. What Do We Talk When We Talk about Migration Regimes? The Diverse Theoretical Roots of an Increasingly Popular Concept. In Was ist ein Migrationsregime? What Is a Migration Regime? Pott, A., Rass, C., Wolff, F., Eds.; Migrationsgesellschaften; Springer Fachmedien: Wiesbaden, Germany, 2018; pp. 65–80. [Google Scholar] [CrossRef]
- Esping-Andersen, G. The Three Worlds of Welfare Capitalism; Polity Press: Cambridge, UK, 2008. [Google Scholar]
- Giannoni, M.; Franzini, L.; Masiero, G. Migrant Integration Policies and Health Inequalities in n Europe. BMC Public Health 2016, 16, 463. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Wave 1 (2004) | Wave 2 (2006) | Wave 4 (2010) | Wave 5 (2013) | Wave 6 (2015) | Wave 7 (2017) | Total | p-Value for Difference | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Non-Migrants (n = 19,585) | Migrants (n = 2554) | Non-Migrants (n = 21,241) | Migrants (n = 2334) | Non-Migrants (n = 37,043) | Migrants (n = 4136) | Non-Migrants (n = 40,535) | Migrants (n = 5452) | Non-Migrants (n = 40,975) | Migrants (n = 4955) | Non-Migrants (n = 49,464) | Migrants (n = 4843) | Non-Migrants (all waves, n = 208,843) | Migrants (all waves, n = 24,274) | |
| Mean Age (SD) | 64.8 (10.4) | 64.9 (10.2) | 64.8 (10.4) | 64.3 (10.4) | 65.7 (10.5) | 65.4 (9.7) | 67.8 (10.5) | 67.6 (10.3) | 68.4 (10.8) | 68.0 (10.2) | 69.5 (10.4) | 69.7 (10.0) | 67.0 (10.7) | 66.6 (10.3) | 0.007 a |
| Age (70 and older), % | 31.9 | 32.0 | 31.4 | 27.7 | 34.9 | 32.2 | 40.3 | 40.0 | 42.8 | 40.1 | 46.1 | 48.5 | 38.5 | 36.9 | 0.013 b |
| Female Gender, % | 53.9 | 54.0 | 53.5 | 56.5 | 55.7 | 52.5 | 55.6 | 53.7 | 55.9 | 58.2 | 57.3 | 57.5 | 55.5 | 55.4 | 0.941 b |
| Mean Household Size (SD) | 2.2 (1.0) | 2.2 (1.0) | 2.1 (1.0) | 2.1 (0.9) | 2.2 (1.0) | 2.1 (0.9) | 2.1 (1.0) | 2.1 (0.9) | 2.1 (1.0) | 2.0 (1.0) | 2.0 (1.0) | 1.90 (1.0) | 2.1 (1.0) | 2.1 (1.0) | 0.279 c |
| Education | <0.001 b | ||||||||||||||
| lower/upper secondary, % | 53.3 | 38.5 | 48.9 | 37.6 | 45.8 | 34.5 | 43.2 | 33.8 | 42.2 | 32.9 | 39.7 | 30.2 | 45.0 | 34.6 | |
| post-secondary, % | 30.7 | 37.6 | 34.7 | 39.1 | 37.0 | 40.3 | 36.9 | 36.9 | 38.8 | 38.6 | 41.1 | 39.9 | 36.9 | 38.7 | |
| tertiary, % | 16.0 | 24.0 | 16.4 | 23.3 | 17.2 | 25.2 | 19.9 | 29.3 | 19.0 | 28.5 | 19.2 | 29.8 | 18.1 | 26.7 | |
| Health Indicators | |||||||||||||||
| Global Activity Limitation Index, % limited | 43.7 | 51.6 | 44.9 | 48.7 | 49.0 | 51.3 | 45.2 | 47.4 | 45.9 | 49.2 | 47.5 | 51.0 | 46.2 | 49.9 | <0.001 b |
| Depression, % depressed | 27.6 | 32.1 | 27.9 | 28.4 | 30.5 | 30.6 | 28.4 | 30.0 | 29.6 | 31.6 | 31.4 | 29.8 | 29.0 | 30.5 | 0.074 b |
| Self-Rated Health, % less than good | 76.3 | 79.4 | 78.6 | 81.7 | 79.5 | 80.8 | 76.3 | 79.8 | 77.3 | 78.1 | 79.0 | 80.7 | 77.9 | 80.1 | 0.004 b |
| Parameter | Limited Global Activity Limitation Index (GALI) (Model 1) | Depression (Model 2) | Poorer Self-Rated Health (Model 3) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p | Odds Ratio | 95% CI | p | Odds Ratio | 95% CI | p | |
| (Intercept) | 0.95 | (0.89, 1.01) | 0.088 | 0.53 | (0.50, 0.57) | <0.001 | 4.85 | (4.51, 5.21) | <0.001 |
| Wave | 1.03 | (1.02, 1.03) | <0.001 | 1.03 | (1.02, 1.04) | <0.001 | 1.02 | (1.01, 1.03) | <0.001 |
| Migrant (ref. non-migrant) | 1.24 | (1.15, 1.34) | <0.001 | 1.19 | (1.09, 1.29) | <0.001 | 1.28 | (1.17, 1.40) | <0.001 |
| Age (between subjects) | 0.98 | (0.95, 1.01) | 0.184 | 1.03 | (1.00, 1.07) | 0.086 | 0.98 | (0.95, 1.02) | 0.359 |
| Female Gender (ref. male) | 1.01 | (0.98, 1.05) | 0.367 | 1.00 | (0.97, 1.04) | 0.863 | 1.02 | (0.98, 1.06) | 0.256 |
| Education (ref. lower/upper secondary) | |||||||||
| post-secondary | 0.73 | (0.70, 0.77) | <0.001 | 0.57 | (0.54, 0.60) | <0.001 | 0.60 | (0.57, 0.64) | <0.001 |
| tertiary | 0.52 | (0.49, 0.55) | <0.001 | 0.40 | (0.38, 0.43) | <0.001 | 0.33 | (0.31, 0.35) | <0.001 |
| Household Size | 1.00 | (0.99, 1.02) | 0.656 | 0.98 | (0.96, 1.00) | 0.055 | 1.00 | (0.98, 1.02) | 0.893 |
| Age (within subject) | 1.02 | (1.00, 1.04) | 0.020 | 0.99 | (0.97, 1.02) | 0.539 | 1.02 | (1.00, 1.04) | 0.080 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vonneilich, N.; Bremer, D.; von dem Knesebeck, O.; Lüdecke, D. Health Patterns among Migrant and Non-Migrant Middle- and Older-Aged Individuals in Europe—Analyses Based on Share 2004–2017. Int. J. Environ. Res. Public Health 2021, 18, 12047. https://doi.org/10.3390/ijerph182212047
Vonneilich N, Bremer D, von dem Knesebeck O, Lüdecke D. Health Patterns among Migrant and Non-Migrant Middle- and Older-Aged Individuals in Europe—Analyses Based on Share 2004–2017. International Journal of Environmental Research and Public Health. 2021; 18(22):12047. https://doi.org/10.3390/ijerph182212047
Chicago/Turabian StyleVonneilich, Nico, Daniel Bremer, Olaf von dem Knesebeck, and Daniel Lüdecke. 2021. "Health Patterns among Migrant and Non-Migrant Middle- and Older-Aged Individuals in Europe—Analyses Based on Share 2004–2017" International Journal of Environmental Research and Public Health 18, no. 22: 12047. https://doi.org/10.3390/ijerph182212047
APA StyleVonneilich, N., Bremer, D., von dem Knesebeck, O., & Lüdecke, D. (2021). Health Patterns among Migrant and Non-Migrant Middle- and Older-Aged Individuals in Europe—Analyses Based on Share 2004–2017. International Journal of Environmental Research and Public Health, 18(22), 12047. https://doi.org/10.3390/ijerph182212047