
Is Instrumental Compression Equally Effective and Comfortable for Physiotherapists and Physiotherapy Students than Manual Compression? A Comparative Cross-Sectional Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
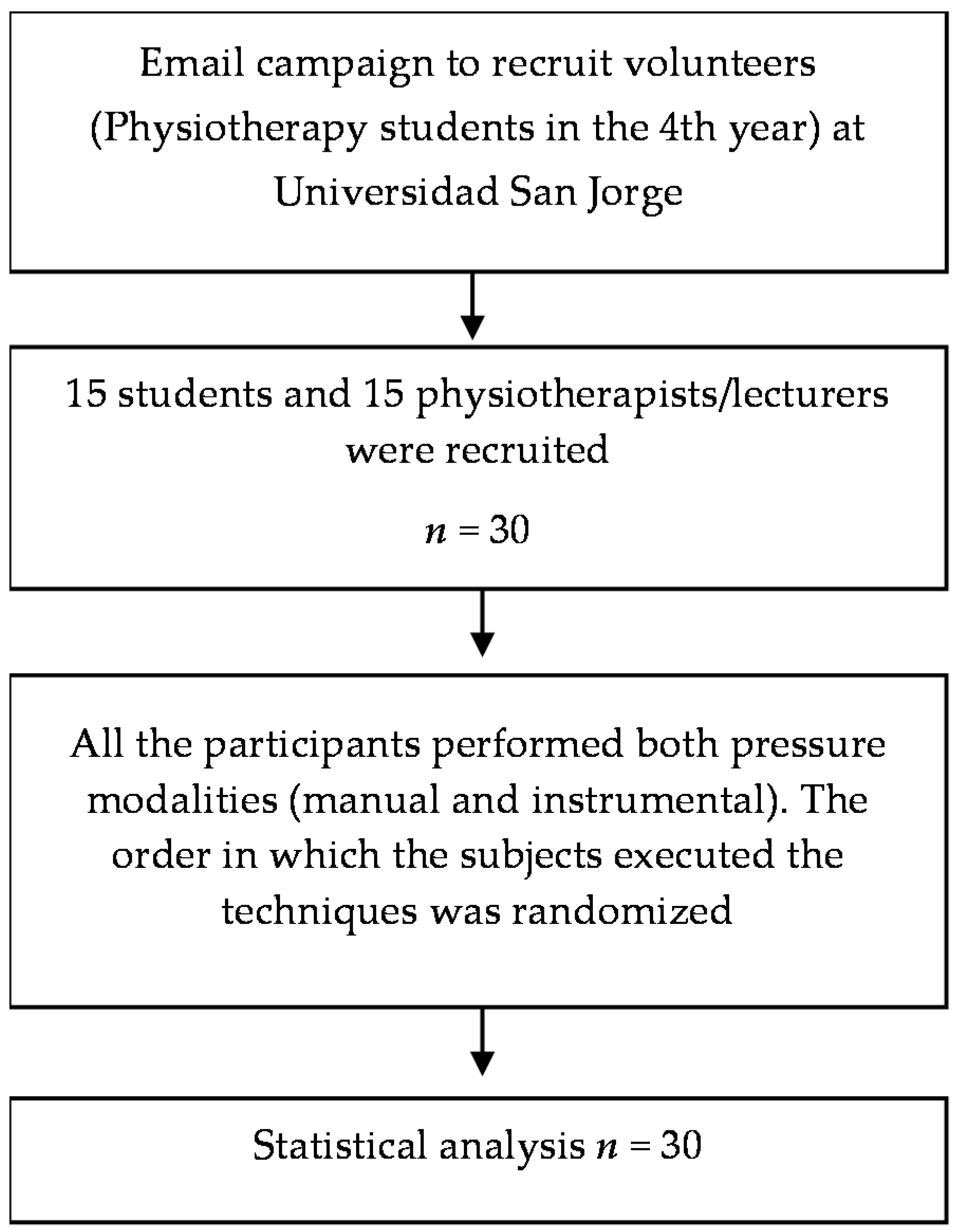
2.1. Study Design
2.2. Participants
2.3. Procedure
2.4. Instruments
2.5. Outcomes
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
2.6. Sample Size
2.7. Statistical Analysis
3. Results
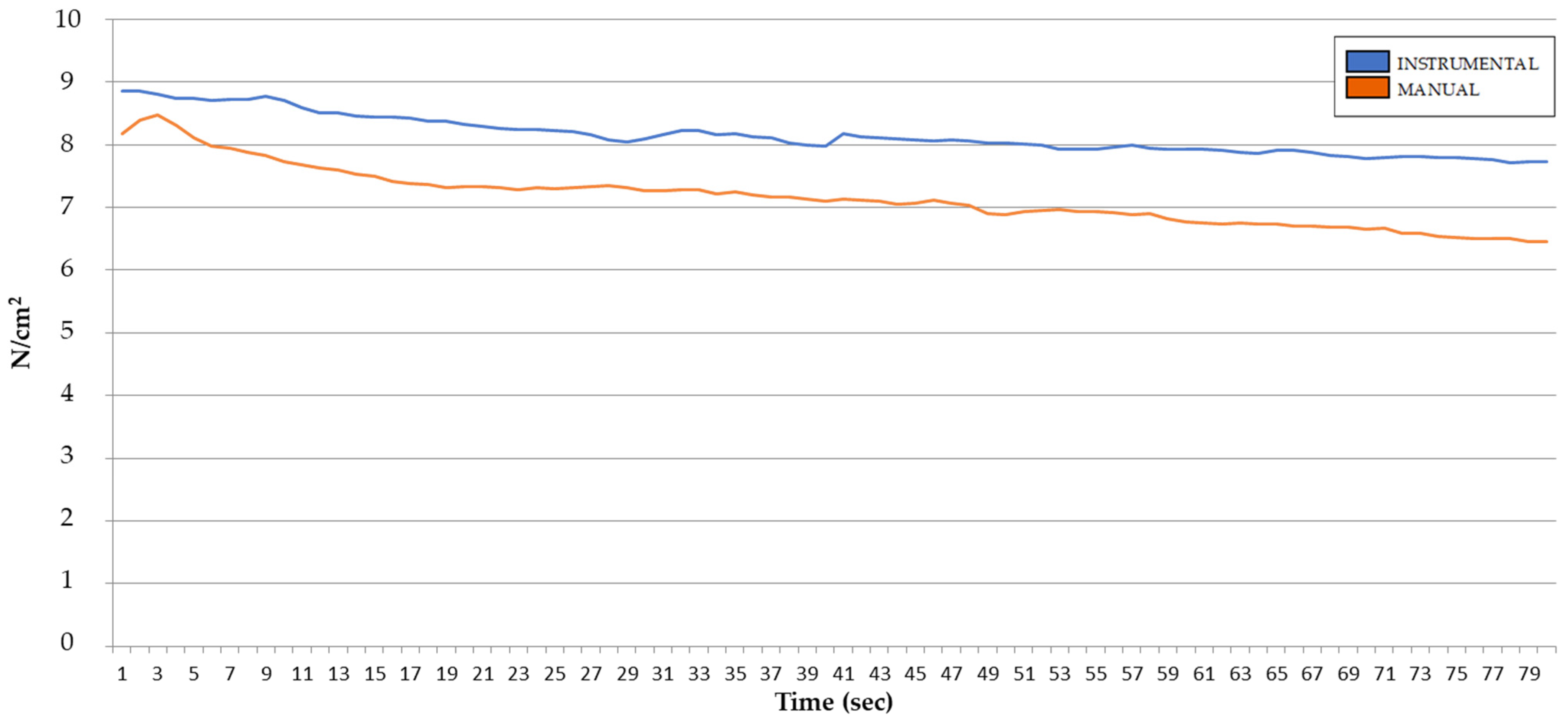
3.1. Variability of Pressure during the Technique
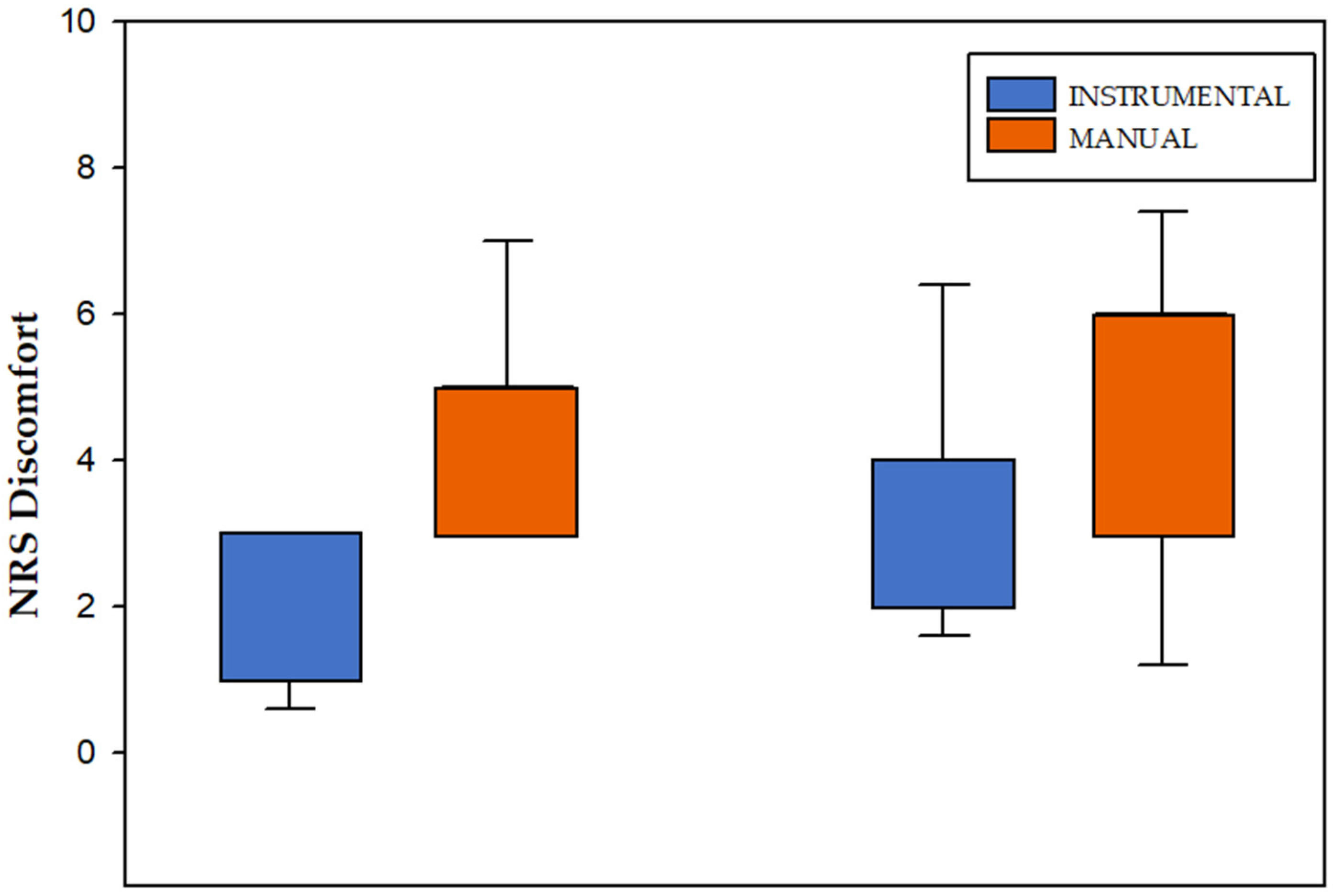
3.2. NRS Discomfort Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desai, M.J.; Bean, M.C.; Heckman, T.W.; Jayaseelan, D.; Moats, N.; Nava, A. Treatment of myofascial pain. Pain Manag. 2013, 3, 67–79. [Google Scholar] [CrossRef]
- Villafañe, J.H.; Herrero, P. Conservative treatment of Myofascial Trigger Points and joint mobilization for management in patients with thumb carpometacarpal osteoarthritis. J. Hand Ther. 2016, 29, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro da Silva, F.; Moreira, G.M.; Zomkowski, K.; Amaral de Noronha, M.; Flores Sperandio, F. Manual Therapy as Treatment for Chronic Musculoskeletal Pain in Female Breast Cancer Survivors: A Systematic Review and Meta-Analysis. J. Manip. Physiol. Ther. 2019, 42, 503–513. [Google Scholar] [CrossRef]
- Bernetti, A.; Agostini, F.; de Sire, A.; Mangone, M.; Tognolo, L.; Di Cesare, A.; Ruiu, P.; Paolucci, T.; Invernizzi, M.; Paoloni, M. Neuropathic Pain and Rehabilitation: A Systematic Review of International Guidelines. Diagnostics 2021, 11, 74. [Google Scholar] [CrossRef]
- Ganesh, G.S.; Singh, H.; Mushtaq, S.; Mohanty, P.; Pattnaik, M. Effect of cervical mobilization and ischemic compression therapy on contralateral cervical side flexion and pressure pain threshold in latent upper trapezius trigger points. J. Bodyw. Mov. Ther. 2016, 20, 477–483. [Google Scholar] [CrossRef]
- Simons, D.G. Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. J. Electromyogr. Kinesiol. 2004, 14, 95–107. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Dommerholt, J. International Consensus on Diagnostic Criteria and Clinical Considerations of Myofascial Trigger Points: A Delphi Study. Pain Med. 2018, 19, 142–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dommerholt, J.; Finnegan, M.; Hooks, T.; Grieve, R. A critical overview of the current myofascial pain literature-September 2016. J. Bodyw. Mov. Ther. 2016, 20, 879–892. [Google Scholar] [CrossRef] [PubMed]
- Dommerholt, J.; Hooks, T.; Chou, L.W.; Finnegan, M. A critical overview of the current myofascial pain literature-January 2018. J. Bodyw. Mov. Ther. 2018, 22, 184–191. [Google Scholar] [CrossRef]
- Simons, D.; Travell, J.; Simons, L. Myofascial Pain and Dysfunction: The Trigger Point Manual. Upper Half of Body, 2nd ed.; Travell, J., Simons, D., Eds.; Williams&Wilkins: Baltimore, MD, USA, 1999; Volume 1. [Google Scholar]
- Cagnie, B.; Castelein, B.; Pollie, F.; Steelant, L.; Verhoeyen, H.; Cools, A. Evidence for the Use of Ischemic Compression and Dry Needling in the Management of Trigger Points of the Upper Trapezius in Patients with Neck Pain: A Systematic Review. Am. J. Phys. Med. Rehabil. 2015, 94, 573–583. [Google Scholar] [CrossRef]
- Ransone, J.W.; Schmidt, J.; Crawford, S.K.; Walker, J. Effect of manual compressive therapy on latent myofascial trigger point pressure pain thresholds. J. Bodyw. Mov. Ther. 2019, 23, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Abu Taleb, W.; Rehan Youssef, A.; Saleh, A. The effectiveness of manual versus algometer pressure release techniques for treating active myofascial trigger points of the upper trapezius. J. Bodyw. Mov. Ther. 2016, 20, 863–869. [Google Scholar] [CrossRef]
- Fryer, G.; Hodgson, L.J.J.o.B.; Therapies, M. The effect of manual pressure release on myofascial trigger points in the upper trapezius muscle. J. Bodyw. Mov. Ther. 2005, 9, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Hou, C.R.; Tsai, L.C.; Cheng, K.F.; Chung, K.C.; Hong, C.Z. Immediate effects of various physical therapeutic modalities on cervical myofascial pain and trigger-point sensitivity. Arch. Phys. Med. Rehabil. 2002, 83, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Pecos-Martin, D.; Ponce-Castro, M.J.; Jiménez-Rejano, J.J.; Nunez-Nagy, S.; Calvo-Lobo, C.; Gallego-Izquierdo, T. Immediate effects of variable durations of pressure release technique on latent myofascial trigger points of the levator scapulae: A double-blinded randomised clinical trial. Acupunct. Med. 2019, 37, 141–150. [Google Scholar] [CrossRef]
- Milhem, M.; Kalichman, L.; Ezra, D.; Alperovitch-Najenson, D. Work-related musculoskeletal disorders among physical therapists: A comprehensive narrative review. Int. J. Occup. Med. Environ. Health 2016, 29, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Hanten, W.P.; Olson, S.L.; Butts, N.L.; Nowicki, A.L. Effectiveness of a home program of ischemic pressure followed by sustained stretch for treatment of myofascial trigger points. Phys. Ther. 2000, 80, 997–1003. [Google Scholar] [CrossRef]
- Gulick, D.T.; Palombaro, K.; Lattanzi, J.B. Effect of ischemic pressure using a Backnobber II device on discomfort associated with myofascial trigger points. J. Bodyw. Mov. Ther. 2011, 15, 319–325. [Google Scholar] [CrossRef]
- Urbaniak, G.C.; Plous, S. Research Randomizer (Version 4.0) [Computer Software]. 2013. Available online: https://www.randomizer.org/Link (accessed on 14 February 2017).
- Myburgh, C.; Larsen, A.H.; Hartvigsen, J. A systematic, critical review of manual palpation for identifying myofascial trigger points: Evidence and clinical significance. Arch. Phys. Med. Rehabil. 2008, 89, 1169–1176. [Google Scholar] [CrossRef]
- Clarke, M.N.; Ni Mhuircheartaigh, D.A.; Walsh, G.M.; Walsh, J.M.; Meldrum, D. Intra-tester and inter-tester reliability of the MicroFET 3 hand-held dynamometer. Physiother. Pract. Res. 2011, 32, 13–18. [Google Scholar] [CrossRef]
- Calvo, S.; Herrero, P.; Tyrrell, J.; Ayuda, V.; Pérez-Palomares, S.; Galán-Díaz, R.; Secorro, N.; Nicolo Gagni, N. Instrumental Myofascial Therapy, Practical Manual; Fisio Consultores SL: Zaragoza, Spain, 2019. [Google Scholar]
- Centro Español de Metrología. (BIPM) OIdPyM. El Sistema Internacional de Unidades (SI). In Metro OIdlCd, 2nd ed.; Ministerio de Industria, Turismo y Comercio: Madrid, Spain, 2008. [Google Scholar]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. 11), S240–S252. [Google Scholar] [CrossRef]
- Rossettini, G.; Rondoni, A.; Schiavetti, I.; Tezza, S.; Testa, M. Prevalence and risk factors of thumb pain in Italian manual therapists: An observational cross-sectional study. Work 2016, 54, 159–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulick, D.T. Instrument-assisted soft tissue mobilization increases myofascial trigger point pain threshold. J. Bodyw. Mov. Ther. 2018, 22, 341–345. [Google Scholar] [CrossRef]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect Size Estimates: Current Use, Calculations, and Interpretation (vol 141, pg 2, 2011). J. Exp. Psychol.-Gen. 2012, 141, 30. [Google Scholar] [CrossRef]
- Campa-Moran, I.; Rey-Gudin, E.; Fernández-Carnero, J.; Paris-Alemany, A.; Gil-Martinez, A.; Lerma Lara, S.; Prieto-Baquero, A.; Alonso-Perez, J.L.; La Touche, R. Comparison of Dry Needling versus Orthopedic Manual Therapy in Patients with Myofascial Chronic Neck Pain: A Single-Blind, Randomized Pilot Study. Pain Res. Treat. 2015, 2015, 327307. [Google Scholar] [CrossRef] [PubMed]
- Lew, J.; Kim, J.; Nair, P. Comparison of dry needling and trigger point manual therapy in patients with neck and upper back myofascial pain syndrome: A systematic review and meta-analysis. J. Man Manip. Ther. 2021, 29, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Nordin, N.A.; Leonard, J.H.; Thye, N.C. Work-related injuries among physiotherapists in public hospitals: A Southeast Asian picture. Clinics 2011, 66, 373–378. [Google Scholar] [CrossRef]
- Glover, W.; Mcgregor, A.H.; Sullivan, C.; Hague, J.N.G.M.J.P. Work-related musculoskeletal disorders affecting members of the Chartered Society of Physiotherapy. Physiotherapy 2005, 91, 138–147. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Characteristics | Students (n = 15) | Physiotherapists (n = 15) | Total (n = 30) |
|---|---|---|---|
| Age (SD) | 23.50 (3.16) | 32.50 (5.73) | 28.03 (6.45) |
| Sex (males/females) | 6/9 | 4/11 | 10/20 |
| Professional experience (years) | 0 | 10.80 (6.09) | 10.80 (6.09) |
| Interval (s) | Technique | Mean (SD) | 95% CI Mean (Inferior; Superior) | p-Value | Effect Size (ES) |
|---|---|---|---|---|---|
| 1–80 | Instrumental | 8.22 (4.04) | (7.07; 10.5) | 0.043 * | 0.253 |
| Manual | 7.27 (3.46) | (7.01; 9.59) |
| Interval (s) | Technique | Mean (SD) | 95% IC Mean (Inferior; Superior) | p-Value * |
|---|---|---|---|---|
| 1–5 | Instrumental | 8.80 (4.62) | (7.07; 10.50) | 0.361 |
| Manual | 8.30 (3.45) | (7.01; 9.59) | ||
| 6–10 | Instrumental | 8.73 (4.57) | (7.02; 10.40) | 0.083 |
| Manual | 7.87 (3.48) | (6.57; 9.17) | ||
| 11–15 | Instrumental | 8.50 (4.33) | (6.88; 10.11) | 0.050 |
| Manual | 7.58 (3.41) | (6.31; 8.86) | ||
| 16–20 | Instrumental | 8.39 (4.33) | (6.77; 10.00) | 0.033 * |
| Manual | 7.36 (3.39) | (6.10; 8.62) | ||
| 21–25 | Instrumental | 8.25 (4.25) | (6.66; 9.83) | 0.052 |
| Manual | 7.31 (3.46) | (6.02; 8.60) | ||
| 26–30 | Instrumental | 8.12 (4.00) | (6.62; 9.60) | 0.084 |
| Manual | 7.31 (3.65) | (5.95; 8.67) | ||
| 31–35 | Instrumental | 8.19 (3.99) | (6.70; 9.68) | 0.049 * |
| Manual | 7.26 (3.60) | (5.91; 8.60) | ||
| 36–40 | Instrumental | 8.05 (3.68) | (6.60; 9.49) | 0.064 |
| Manual | 7.16(3.54) | (5.83; 8.48) | ||
| 41–45 | Instrumental | 8.12 (3.94) | (6.64; 9.59) | 0.041 * |
| Manual | 7.09 (±3.42) | (5.81; 8.36) | ||
| 46–50 | Instrumental | 8.05 (3.92) | (6.58; 9.51) | 0.032 * |
| Manual | 7.01 (3.37) | (5.75; 8.25) | ||
| 51–55 | Instrumental | 7.96 (3.90) | (6.50; 9.41) | 0.036 * |
| Manual | 6.95 (3.33) | (5.70; 8.19) | ||
| 56–60 | Instrumental | 7.95 (3.94) | (6.48; 9.42) | 0.022 * |
| Manual | 6.86 (3.28) | (5.63; 8.08) | ||
| 61–65 | Instrumental | 7.90 (3.87) | (6.45; 9.34) | 0.016 * |
| Manual | 6.75 (3.21) | (5.54; 9.94) | ||
| 66–70 | Instrumental | 7.84 (3.89) | (6.39; 9.29) | 0.017 * |
| Manual | 6.69 (3.28) | (5.46; 7.91) | ||
| 71–75 | Instrumental | 7.80 (3.86) | (6.35; 9.24) | 0.009 * |
| Manual | 6.58 (3.25) | (5.36; 7.79) | ||
| 76–80 | Instrumental | 7.74 (3.72) | (6.35; 9.13) | 0.005 * |
| Manual | 6.48 (3.19) | (5.29; 7.67) |
| Interval (s) | 6–10 | 11–15 | 16–20 | 21–25 | 26–30 | 31–35 | 36–40 | 41–45 | 46–50 | 51–55 | 56–60 | 61–65 | 66–70 | 71–75 | 76–80 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Technique | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value | D | p-Value |
| Instrumental | −0.07 | 0.067 | −0.30 | 0.013 * | −0.41 | 0.005 * | −0.55 | 0.007 * | −0.68 | 0.001 * | −0.61 | 0.001 * | −0.75 | <0.001 * | −0.68 | 0.003 * | −0.75 | 0.003 * | −0.84 | 0.001 * | −0.85 | 0.002 * | −0.90 | 0.001 * | −0.96 | 0.001 * | −1.00 | 0.001 * | −1.06 | <0.001 * |
| Manual | −0.42 | 0.008 * | −0.71 | 0.001 * | −0.94 | <0.001 * | −0.99 | <0.001 * | −0.98 | 0.001 * | −1.04 | <0.001 * | −1.14 | <0.001 * | −1.21 | <0.001 * | −1.29 | <0.001 * | −1.35 | <0.001 * | −1.44 | <0.001 * | −1.55 | <0.001 * | −1.61 | <0.001 * | −1.72 | <0.001 * | −1.81 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Palomares, S.; Jiménez-Sánchez, C.; Serrano-Herrero, I.; Herrero, P.; Calvo, S. Is Instrumental Compression Equally Effective and Comfortable for Physiotherapists and Physiotherapy Students than Manual Compression? A Comparative Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12121. https://doi.org/10.3390/ijerph182212121
Pérez-Palomares S, Jiménez-Sánchez C, Serrano-Herrero I, Herrero P, Calvo S. Is Instrumental Compression Equally Effective and Comfortable for Physiotherapists and Physiotherapy Students than Manual Compression? A Comparative Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(22):12121. https://doi.org/10.3390/ijerph182212121
Chicago/Turabian StylePérez-Palomares, Sara, Carolina Jiménez-Sánchez, Ignacio Serrano-Herrero, Pablo Herrero, and Sandra Calvo. 2021. "Is Instrumental Compression Equally Effective and Comfortable for Physiotherapists and Physiotherapy Students than Manual Compression? A Comparative Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 22: 12121. https://doi.org/10.3390/ijerph182212121
APA StylePérez-Palomares, S., Jiménez-Sánchez, C., Serrano-Herrero, I., Herrero, P., & Calvo, S. (2021). Is Instrumental Compression Equally Effective and Comfortable for Physiotherapists and Physiotherapy Students than Manual Compression? A Comparative Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(22), 12121. https://doi.org/10.3390/ijerph182212121