
5-Methyltetrahydrofolate and Vitamin B12 Supplementation Is Associated with Clinical Pregnancy and Live Birth in Women Undergoing Assisted Reproductive Technology

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Covariate Assessment
2.3. Laboratory Assessment
Sperm Processing
2.4. Clinical Procedures and Outcome Assessment
Statistical Analysis
3. Results
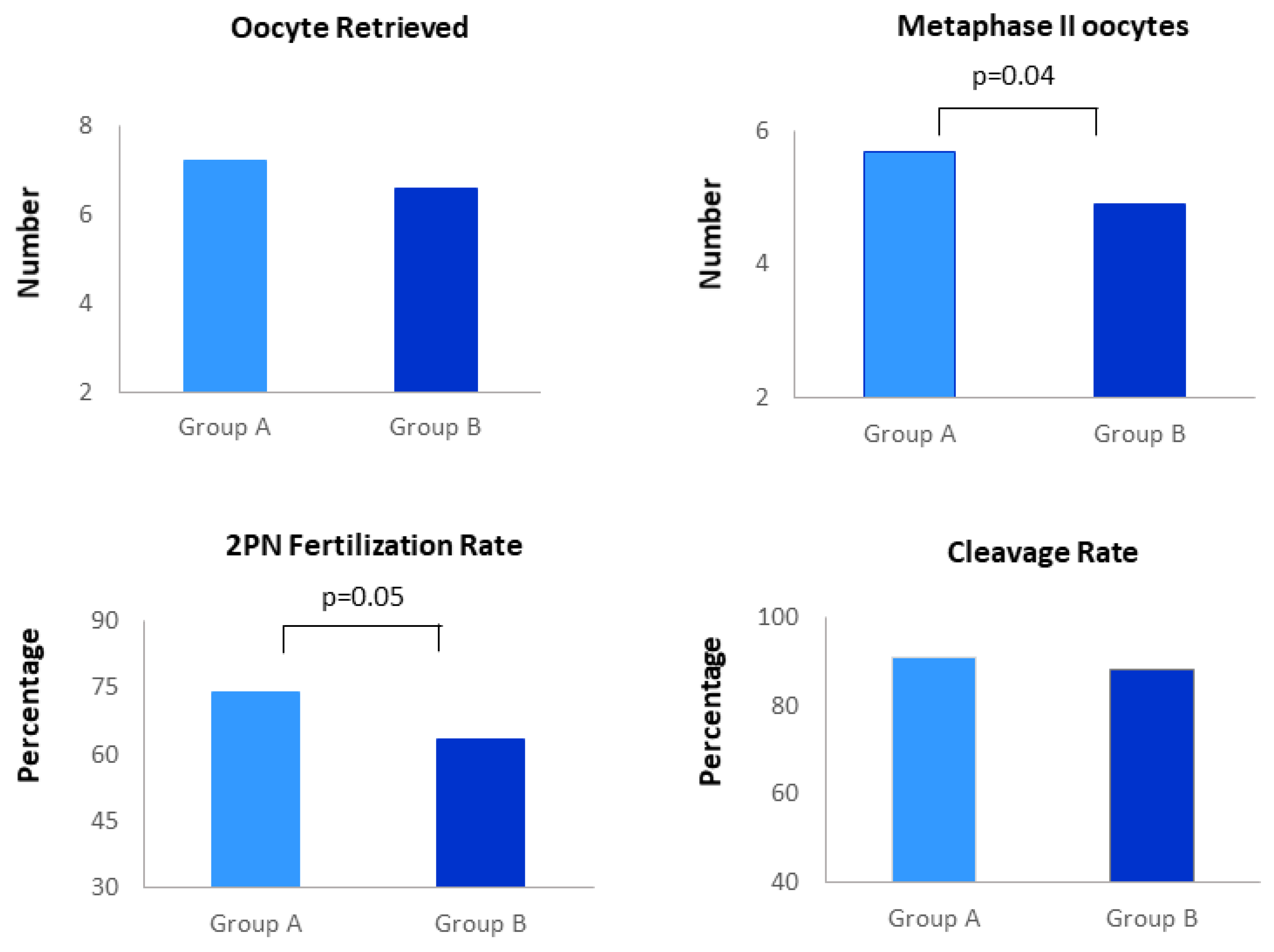
3.1. Embryology Laboratory Outcomes
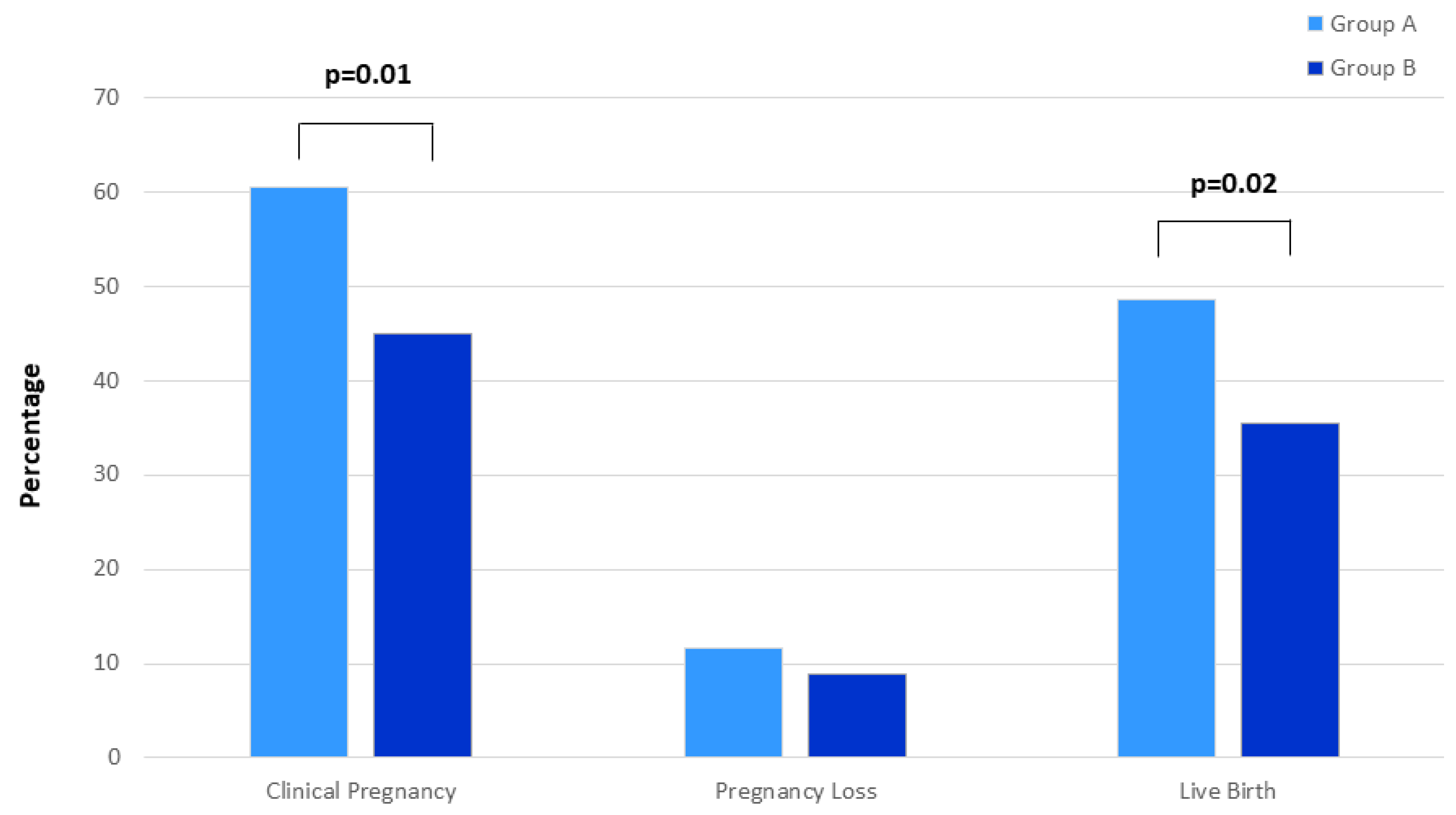
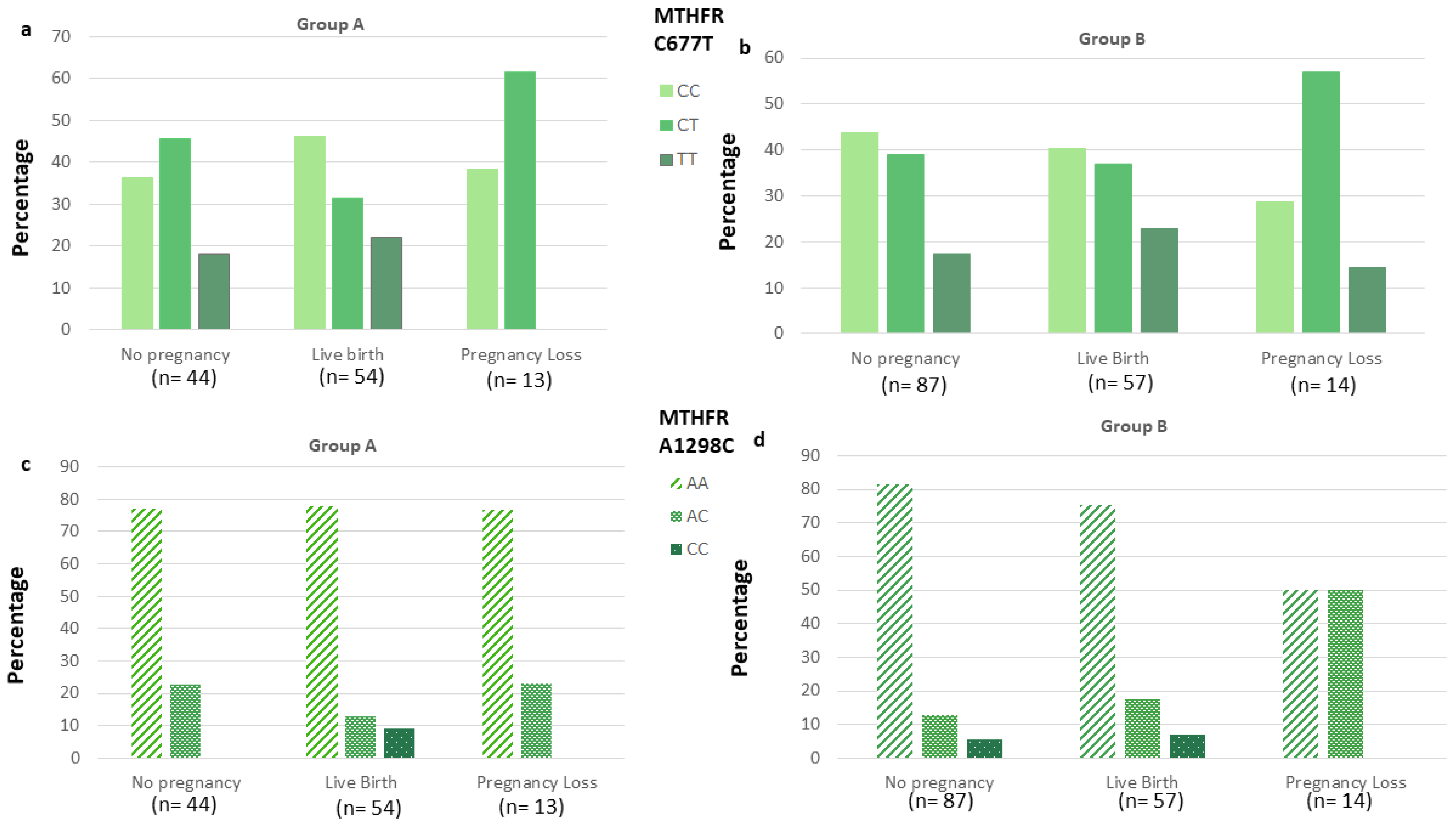
3.2. Pregnancy Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ebisch, I.M.; Thomas, C.M.; Peters, W.H.; Braat, D.D.; Steegers-Theunissen, R.P. The importance of folate, zinc and antioxidants in the pathogenesis and prevention of subfertility. Hum. Reprod. Update 2007, 13, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Forges, T.; Monnier-Barbarino, P.; Alberto, J.M.; Guéant-Rodriguez, R.M.; Daval, J.L.; Guéant, J.L. Impact of folate and homocysteine metabolism on human reproductive health. Hum. Reprod. Update 2007, 13, 225–238. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Chiu, Y.H.; Williams, P.L.; Ford, J.B.; Toth, T.L.; Hauser, R.; Chavarro, J.E.; EARTH Study Team. Association between serum folate and vitamin B-12 and outcomes of assisted reproductive technologies. Am. J. Clin. Nutr. 2015, 102, 943–950. [Google Scholar] [CrossRef] [Green Version]
- Murto, T.; Kallak, T.K.; Hoas, A.; Altmäe, S.; Salumets, A.; Nilsson, T.K.; Skoog Svanberg, A.; Wånggren, K.; Yngve, A.; Stavreus-Evers, A. Folic acid supplementation and methylenetetrahydrofolate reductase (MTHFR) gene variations in relation to in vitro fertilization pregnancy outcome. Acta Obs. Gynecol. Scand 2015, 94, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Varadi, S. Pernicious anaemia and infertility. Lancet 1967, 2, 1305. [Google Scholar] [CrossRef]
- El-Nemr, A.; Sabatini, L.; Wilson, C.; Lower, A.M.; Al-Shawaf, T.; Grudzinskas, J.G. Vitamin B12 deficiency and IVF. J. Obs. Gynaecol. 1998, 18, 192–193. [Google Scholar] [CrossRef] [PubMed]
- Boxmeer, J.C.; Macklon, N.S.; Lindemans, J.; Beckers, N.G.; Eijkemans, M.J.; Laven, J.S.; Steegers, E.A.; Steegers-Theunissen, R.P. IVF outcomes are associated with biomarkers of the homocysteine pathway in monofollicular fluid. Hum. Reprod. 2009, 24, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Haggarty, P.; McCallum, H.; McBain, H.; Andrews, K.; Duthie, S.; McNeill, G.; Templeton, A.; Haites, N.; Campbell, D.; Bhattacharya, S. Effect of B vitamins and genetics on success of in-vitro fertilisation: Prospective cohort study. Lancet 2006, 367, 1513–1519. [Google Scholar] [CrossRef]
- Vujkovic, M.; de Vries, J.H.; Lindemans, J.; Macklon, N.S.; van der Spek, P.J.; Steegers, E.A.; Steegers-Theunissen, R.P. The preconception Mediterranean dietary pattern in couples undergoing in vitro fertilization/intracytoplasmic sperm injection treatment increases the chance of pregnancy. Fertil. Steril. 2010, 94, 2096–2101. [Google Scholar] [CrossRef]
- Van Aerts, L.A.; Klaasboer, H.H.; Postma, N.S.; Pertijs, J.C.; Copius Peereboom, J.H.; Eskes, T.K.; Noordhoek, J. Stereospecific in vitro embryotoxicity of l-homocysteine in pre- and post-implantation rodent embryos. Toxicol. Vitr. 1993, 7, 743–749.9. [Google Scholar] [CrossRef]
- Kramer, M.S.; Kahn, S.R.; Rozen, R.; Evans, R.; Platt, R.W.; Chen, M.F.; Goulet, L.; Séguin, L.; Dassa, C.; Lydon, J.; et al. Vasculopathic and thrombophilic risk factors for spontaneous preterm birth. Int. J. Epidemiol. 2009, 38, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Nelen, W.L.; Bulten, J.; Steegers, E.A.; Blom, H.J.; Hanselaar, A.G.; Eskes, T.K. Maternal homocysteine and chorionic vascularization in recurrent early pregnancy loss. Hum. Reprod. 2000, 15, 954–960. [Google Scholar] [CrossRef] [Green Version]
- Berker, B.; Kaya, C.; Aytac, R.; Satiroglu, H. Homocysteine concentrations in follicular fluid are associated with poor oocyte and embryo qualities in polycystic ovary syndrome patients undergoing assisted reproduction. Hum. Reprod. 2009, 24, 2293–2302. [Google Scholar] [CrossRef] [Green Version]
- Ebisch, I.M.; Peters, W.H.; Thomas, C.M.; Wetzels, A.M.; Peer, P.G.; Steegers-Theunissen, R.P. Homocysteine, glutathione and related thiols affect fertility parameters in the (sub)fertile couple. Hum. Reprod. 2006, 21, 1725–1733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension global hypertension practice guidelines. J. Hypertens 2020, 38, 982–1004. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef] [PubMed]
- ESHRE Guideline Group on RPL; Bender Atik, R.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Nelen, W.; Peramo, B.; Quenby, S.; et al. ESHRE guideline: Recurrent pregnancy loss. Hum. Reprod. Open 2018, 2018, hoy004. [Google Scholar] [CrossRef]
- Bashiri, A.; Halper, K.I.; Orvieto, R. Recurrent Implantation Failure-update overview on etiology, diagnosis, treatment and future directions. Reprod. Biol. Endocrinol. 2018, 16, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Sperm: Fifth Edition. Available online: https://www.who.int/reproductivehealth/publications/infertility/9789241547789/en/ (accessed on 20 June 2021).
- Douglas Wilson, R.; Van Mieghem, T.; Langlois, S.; Church, P. Guideline No. 410: Prevention, Screening, Diagnosis, and Pregnancy Management for Fetal Neural Tube Defects. J. Obs. Gynaecol. Can. 2021, 43, 124–139.e8. [Google Scholar] [CrossRef]
- Paffoni, A.; Castiglioni, M.; Ferrari, S.; La Vecchia, I.; Ferraris Fusarini, C.; Bettinardi, N.; Noli, S.; Parazzini, F.; Somigliana, E. Homocysteine pathway and in vitro fertilization outcome. Reprod. Toxicol. 2018, 76, 12–16. [Google Scholar] [CrossRef]
- Murto, T.; Skoog Svanberg, A.; Yngve, A.; Yngve, A.; Nilsson, T.K.; Altmäe, S.; Wånggren, K.; Salumets, A.; Stavreus-Evers, A. Folic acid supplementation and IVF pregnancy outcome in women with unexplained infertility. Reprod. Biomed Online 2014, 28, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Henriksson, P. Cardiovascular problems associated with IVF therapy. J. Intern Med. 2021, 289, 2–11. [Google Scholar] [CrossRef]
- Refsum, H.; Nurk, E.; Smith, A.D.; Ueland, P.M.; Gjesdal, C.G.; Bjelland, I.; Tverdal, A.; Tell, G.S.; Nygård, O.; Vollset, S.E. The Hordaland Homocysteine Study: A community-based study of homocysteine, its determinants, and associations with disease. J. Nutr. 2006, 136, 1731S–1740S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serapinas, D.; Boreikaite, E.; Bartkeviciute, A.; Bandzeviciene, R.; Silkunas, M.; Bartkeviciene, D. The importance of folate, vitamins B6 and B12 for the lowering of homocysteine concentrations for patients with recurrent pregnancy loss and MTHFR mutations. Reprod. Toxicol. 2017, 72, 159–163. [Google Scholar] [CrossRef]
- Rizzo, G.; Laganà, A.S.; Rapisarda, A.M.; La Ferrera, G.M.; Buscema, M.; Rossetti, P.; Nigro, A.; Muscia, V.; Valenti, G.; Sapia, F.; et al. Vitamin B12 among Vegetarians: Status, Assessment and Supplementation. Nutrients 2016, 8, 767. [Google Scholar] [CrossRef] [Green Version]
- Zappacosta, B.; Persichilli, S.; Iacoviello, L.; Di Castelnuovo, A.; Graziano, M.; Gervasoni, J.; Leoncini, E.; Cimino, G.; Mastroiacovo, P. Folate, vitamin B12 and homocysteine status in an Italian blood donor population. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 473–480. [Google Scholar] [CrossRef]
- La Vecchia, I.; Paffoni, A.; Castiglioni, M.; Ferrari, S.; Bortolus, R.; Ferraris Fusarini, C.; Bettinardi, N.; Somigliana, E.; Parazzini, F. Folate, homocysteine and selected vitamins and minerals status in infertile women. Eur. J. Contracept Reprod. Health Care 2017, 22, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Akamine, K.; Mekaru, K.; Gibo, K.; Nagata, C.; Nakamura, R.; Oishi, S.; Miyagi, M.; Heshiki, C.; Aoki, Y. Impact of the one-carbon metabolism on oocyte maturation, fertilization, embryo quality, and subsequent pregnancy. Reprod. Med. Biol. 2020, 20, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Heindryckx, B.; Van der Elst, J.; De Sutter, P.; Dhont, M. Treatment option for sperm- or oocyte-related fertilization failure: Assisted oocyte activation following diagnostic heterologous ICSI. Hum. Reprod. 2005, 20, 2237–2241. [Google Scholar] [CrossRef] [Green Version]
- ESHRE Special Interest Group of Embryology and Alpha Scientists in Reproductive Medicine. The Vienna consensus: Report of an expert meeting on the development of ART laboratory performance indicators. Reprod. Biomed Online 2017, 35, 494–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Group A, n = 111 | Group B, n = 158 |
|---|---|---|
| Age yrs | 37.4 (±3.3) | 36.6 (±4) |
| BMI 25–29.99 kg/m2, n, (%) | 27 (24.3) | 36 (22.8) |
| Smoking habit, n (%) | 31 (27.9) | 39 (24.7) |
| Dyslipidemia, n (%) | 49 (44.1) | 79 (50) |
| Hypertension, n (%) | 1 (0.9) | 4 (2.5) |
| Sedentary behaviour, n (%) | 78 (70.3) | 102 (64.6) |
| Migraine with aura, n (%) | 2 (1.8) | 10 (6.3) |
| History of recurrent pregnancy loss ≥ 2, n (%) | 12 (10.8) | 27 (17.1) |
| History of recurrent ART failure ≥ 2, n (%) | 39 (35.1) | 61 (38.6) |
| Endometriosis, n (%) | 14 (12.6) | 23 (14.6) |
| PCOS, n (%) | 6 (5.4) | 15 (9.5) |
| Celiac disease, n (%) | - | - |
| Hashimoto’s thyroiditis, n (%) | 6 (5.4) | 5 (3.2) |
| Family history of CV disease, n (%) | 32 (28.8) | 46 (29.1) |
| Variables | Group A, n = 111 | Group B, n = 158 |
|---|---|---|
| Homocysteine > 13 µmol/L Factor V Leiden heterozygotes, n (%) | 17 (15.3) | 23 (14.6) |
| 9 (8.1) | 13 (8.2) | |
| Prothrombin G20210A mutation heterozygotes, n (%) PC, PS, AT deficiency, n (%) | 4 (3.6) | 8 (5.1) |
| 4 (3.6) | 4 (2.5) | |
| MTHFR C677T, CC, n (%) CT, n (%) TT, n (%) | 46 (41.5) 45 (40.5) 20 (18) | 65 (41.1) 63 (39.9) 30 (19) |
| MTHFR A1298C AA, n (%) AC, n (%) CC, n (%) | 87 (78.4) 19 (17.1) 5 (4.5) | 121 (76.6) 28 (17.7) 9 (5.7) |
| Variables | Group A | Group B | ||
|---|---|---|---|---|
| Clinical Pregnancy | ||||
| OR (95% CI) | p | OR (95% CI) | p | |
| Age < 40 yrs. | 3.12 (1.09–9.85) | 0.05 | 4.91 (1.47–16.45) | 0.01 |
| Smoking habit | 0.40 (0.15–1.08) | 0.07 | 0.99 (0.39–2.49) | 0.9 |
| Dyslipidemia | 0.97 (0.35–2.68) | 0.9 | 1.48 (0.69–3.19) | 0.3 |
| BMI 25–29.99 kg/m2 | 1.36 (0.36–5.09) | 0.6 | 1.11 (0.48–2.56) | 0.8 |
| Inherited thrombophilia | 0.82 (0.16–4.35) | 0.8 | 1.92 (0.51–7.19) | 0.3 |
| MTHFR polymorphisms | 0.57 (0.17–1.91) | 0.4 | 1.81 (0.79–4.17) | 0.2 |
| Antithrombotic therapy | 1.34 (1.09–4.56) | 0.6 | 1.42 (0.61–3.28) | 0.4 |
| Live Birth | ||||
| OR (95% CI) | p | OR (95% CI) | p | |
| Age < 40 yrs | 1.37 (0.47–4.02) | 0.6 | 3.04 (0.92–10.08) | 0.07 |
| Smoking habit | 0.64 (0.24–1.68) | 0.4 | 1.05 (0.42–2.67) | 0.9 |
| Dyslipidemia | 0.81 (0.31–2.09) | 0.7 | 1.13 (0.52–2.44) | 0.8 |
| BMI 25–29.99 kg/m2 | 2.43 (0.70–8.38) | 0.2 | 1.34 (0.58–3.12) | 0.5 |
| Inherited thrombophilia | 0.99 (0.19–5.06) | 0.9 | 1.73 (0.48–6.22) | 0.4 |
| MTHFR polymorphisms | 1.52 (0.50–4.55) | 0.5 | 1.09 (0.48–2.49) | 0.8 |
| Antithrombotic therapy | 1.29 (0.39–4.19) | 0.7 | 1.95 (0.81–4.67) | 0.1 |
| Group A (n = 111) | Group B (n = 158) | |||||
|---|---|---|---|---|---|---|
| Live Birth (n = 54) | Pregnancy Loss (n = 13) | No Pregnancy (n = 44) | Live Birth (n = 57) | Pregnancy Loss (n = 14) | No Pregnancy (n = 87) | |
| Homocysteine Concentrations | ||||||
| MTHFR C677T | MTHFR C677T | |||||
| CC | 11.6 (±6.2) | 9.4 (±2.7) | 12.5 (±8.8) | 9 (±3.4) | 14.8 (±13.3) | 8.2(±3.2) |
| CT | 8.8 (±4.2) | 8 (±1.4) | 8.2 (±2.3) | 8.4 (±3.5) | 7.6 (±2.0) | 8.1 (±2.3) |
| TT | 12.7 (±5.9) | - | 8.4 (±5) | 8.3 (±4.2) | 8.6 (±4.2) | 9.3 (±2.5) |
| MTHFR A1298C | MTHFR A1298C | |||||
| AA | 11.6 (±6.3) | 7.9 (±1.4) | 10 (±6.7) | 8.6 (±3.6) | 13.1 (±8.5) | 8.4 (±2.9) |
| AC | 8.1 (±0.9) | 12.2 (±0.3) | 9 (±3.7) | 9.3 (±4.4) | 6.3 (±1.2) | 8.7 (±2.1) |
| CC | 9.7 (±1.0) | - | - | 7.7 (±1.8) | - | 7.9 (±3.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirillo, M.; Fucci, R.; Rubini, S.; Coccia, M.E.; Fatini, C. 5-Methyltetrahydrofolate and Vitamin B12 Supplementation Is Associated with Clinical Pregnancy and Live Birth in Women Undergoing Assisted Reproductive Technology. Int. J. Environ. Res. Public Health 2021, 18, 12280. https://doi.org/10.3390/ijerph182312280
Cirillo M, Fucci R, Rubini S, Coccia ME, Fatini C. 5-Methyltetrahydrofolate and Vitamin B12 Supplementation Is Associated with Clinical Pregnancy and Live Birth in Women Undergoing Assisted Reproductive Technology. International Journal of Environmental Research and Public Health. 2021; 18(23):12280. https://doi.org/10.3390/ijerph182312280
Chicago/Turabian StyleCirillo, Michela, Rossella Fucci, Sara Rubini, Maria Elisabetta Coccia, and Cinzia Fatini. 2021. "5-Methyltetrahydrofolate and Vitamin B12 Supplementation Is Associated with Clinical Pregnancy and Live Birth in Women Undergoing Assisted Reproductive Technology" International Journal of Environmental Research and Public Health 18, no. 23: 12280. https://doi.org/10.3390/ijerph182312280