Abstract
Dental caries and periodontal disease represent a health problem and a social cost for the entire population, and in particular for socio-economically disadvantaged individuals who are less resistant to disease. The aim of this review is to estimate the prevalence and severity of the two dental pathologies, caries and periodontal disease, in the different classes of socio-economically disadvantaged subjects and to understand which of them are most affected. A systematic search of the literature was performed in MEDLINE (via PubMed), EMBASE and Web of Science after establishing a suitable search strategy for each database, using keywords related to socio-economically vulnerable classes and health outcomes. Socio-economically disadvantaged individuals are more susceptible to tooth decay and periodontal disease (with relative tooth loss) than non-vulnerable people. Additionally, when multiple vulnerabilities are combined in the same subject, these oral diseases worsen. There is no type of vulnerability more affected by caries and periodontitis than others, since overall they all have severe disease indices. The data from this systematic literature review might be useful for health policy makers looking to allocate more resources and services to socially disadvantaged individuals, resulting in making them more resilient to oral disease due to their social marginalization.
1. Introduction
The lack of equality in economic development and social progress between countries, political instability, wars and consequent migratory phenomena, ecological calamities and pandemic diseases affect the socio-economic status of populations worldwide, with ever newer and wider categories of disadvantaged groups [1]. However, socio-economically disadvantaged individuals are found in every social context, in both industrialized and developing countries [2].
One of the most common aspects of socio-economically disadvantaged people is poverty, with shared features such as low education [3], unemployment, strenuous and precarious jobs [4], uncertain housing [5], lack of health insurance [6], immigration [7] and incarceration [8]. Other conditions that cause social vulnerability are related to the ebb and flow of life itself, such as childhood, adolescence [9], old age [10] and pregnancy [11]. Finally, there are less easily classifiable but socio-economically important categories of vulnerability such as minorities due to ethnic origin [12], sexual orientation [13] or family status (e.g., single-parent families or families with separated parents) [13]. All of these types of disadvantaged individuals experience isolation and social exclusion as well as poor health and disparate healthcare access [12]. Moreover, it has been highlighted in the literature that individuals living with a low socio-economic status are more likely to have an unhealthy lifestyle through adopting bad habits such as alcohol, tobacco and drug abuse, use of illegal drugs and poor diet and personal hygiene, all of which affect one’s general and oral health [14,15,16].
Dental caries and periodontal disease are classified among the most common non-communicable diseases in the world and, in addition, the most prevalent diseases of the mouth [17]. These diseases result in reduced masticatory, swallowing and speech functions as well as pain and oral infections, leading to an increased risk of systemic diseases (e.g., heart attack, stroke) and psychological and relational disorders [18,19]. Similarly to all non-communicable systemic diseases, caries and periodontal disease are also expected to be more prevalent and severe among socio-economically disadvantaged subjects [19].
This study attempts to offer a comprehensive view of the dental health situation of socially vulnerable classes, considering them in their complexity and variety, since there is a lack of information in the literature.
The aim of this systematic review is to provide updated and exhaustive data (through the analysis of the publications of the last five years, considering that in the literature articles only focus on a single type of vulnerability) of the prevalence and severity of dental and periodontal health of socio-economically disadvantaged subjects, making a comparison with the entire population and between the different classes of vulnerable individuals.
Null hypotheses:
- There are no differences regarding carious pathology and periodontal disease between socio-economically disadvantaged subjects and the normal population.
- There are no differences concerning caries and periodontal disease between different categories of socio-economically disadvantaged and vulnerable individuals.
- There are no differences in terms of caries and periodontal disease in socio-economically disadvantaged individuals who combine different types of socio-economic vulnerability.
2. Materials and Methods
This review is in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) 2020 Statement in order to maintain a codified organization of the study [20]. In addition, the protocol of this review has been registered in the International Prospective Register of Systematic Reviews database (PROSPERO) (registration number: CRD42021251487).
The outcomes of interest were divided into primary and secondary based on the degree of relevance for this review. Primary outcomes were dental caries, periodontal disease and tooth loss (total or partial edentulism), while secondary ones were dental service attendance, oral health-related quality of life, perceived oral health and emergency treatment. Secondary outcomes will be considered only when their relationship to caries and periodontitis is clear from reading the text (e.g., not when referring to oral cancer or other oral diseases).
Considering the eligibility criteria, any type of observational study design was evaluated as suitable for inclusion in this review such as cross-sectional, case–control, prospective and retrospective cohort studies. Clinical trials were also suitable for inclusion when reporting epidemiological baseline data (useful for this review) before the start of the intervention(s). Only studies published within the last 5 years (30 November 2015 to 30 November 2020) and those investigating the prevalence and severity of dental caries and periodontal disease in adult socio-economically disadvantaged subjects (socio-economically vulnerable people) were considered. Studies written in a language other than English were excluded. Additionally, studies that did not address any of the afore mentioned outcomes or socially vulnerable people were also excluded.
A systematic search of electronic databases was performed using a combination of MeSH terms and free-text words adapted to each database to maximize database specificity. The complete search strategies are reported in Supplementary Table S1. The searched databases included MEDLINE (via PubMed), EMBASE and Web of Science. Further searches were performed in the reference lists of relevant studies, and in book chapters and literature reviews dealing with the topic of interest.
All the studies resulting from the search strategies were imported into an Endnote library and duplicates were removed. Two reviewers (GL and CV) independently assessed the records (title and abstract), selecting the studies that met the eligibility criteria. Any type of disagreement was resolved by consulting a third independent reviewer (SC). After this screening, the records selected were analyzed in their full-text version, and two other reviewers (GL and SP) independently assessed whether they should be included in the review. In case of disagreement, a third author was consulted (SC). The same two reviewers carried out the extraction of the data in a standardized data form, including authors, year of publication, study design, country, setting, characteristics of participants (vulnerability category, number, percentage of women and age), primary and/or secondary outcomes, disease index, study results and notes.
The PRISMA flow diagram (Figure 1) was used to report the included studies according to the eligibility criteria and those excluded during the study selection process.
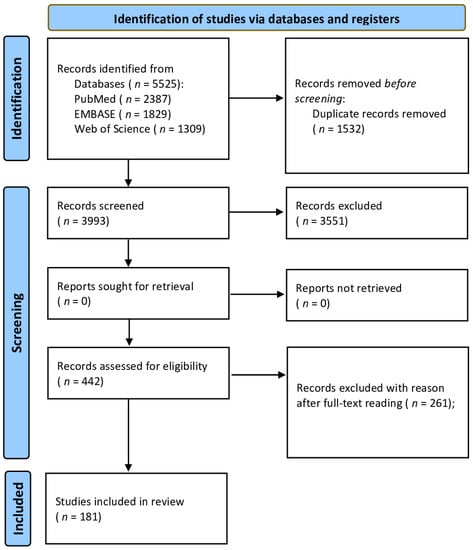
Figure 1.
PRISMA flow diagram for systematic review.
Quality assessment was performed independently by two reviewers (CV and GL) for each included study using the JBI’s Critical Appraisal Tool Checklist for Analytical Cross Sectional Studies, for Case-Control Studies and for Cohort Studies [21]. Any type of disagreement was resolved by consulting a third independent reviewer (SC). With this evaluation tool, the methodological quality of the included studies was evaluated, and the extent to which a study has addressed the possibility of bias in its design, conduct and analysis was determined. JBI’s Tool comprises various check-lists, each referring to a different type of study, of which we utilized three. For the cross-sectional studies, we used the 8-item checklist, considering the following: inclusion criteria definition, subjects and setting description, exposure measurements, standard criteria for measurements, confounding factor identification, strategies to deal with confounding factors, outcome measurements and statistical analysis. For cohort studies, we used the 11-item checklist, which takes into consideration the following: recruitment of population and groups, exposure similarity measures (exposed/unexposed groups), exposure measurements, confounding factor identification, strategies to deal with confounding factors, no outcome at the moment of exposure, outcome measurements, appropriate follow-up, follow-up completeness, strategies to address incomplete follow-up and statistical analysis. For case–control studies, the 10-item checklist was employed: group comparability other than presence/absence of disease, cases and controls matching, cases/controls criteria identification, exposure measurements, procedure similarity for cases and controls, confounding factor identification, strategies to deal with confounding factors, outcome assessment, appropriate exposure period and statistical analysis. The studies could then be rated as good, moderate or poor quality by answering the questions in the categories mentioned with “Yes”, “No”, “Unclear” or “Not/Applicable”.
We assessed whether the homogeneity of the studies considered was sufficient in terms of design, population characteristics and type of oral disease to allow meta-analyses. Furthermore, the results were described narratively in the main text and in the tables. Meta-analysis of the prevalence of caries and periodontal disease in disadvantaged subjects was performed using random effects models, assuming a high heterogeneity between studies, by using the Freeman–Tukey double arcsine transformation for stabilizing the variance. We also pooled the odds ratios reported in studies that compared the occurrence of caries and periodontal disease between disadvantaged subjects and a control group. Additionally, in this case, we used random effects models (inverse variance method) due to a high expected heterogeneity between the included studies. We also calculated weighted means for studies having a single group of participants, and weighted mean difference for studies also having a control group. Secondary analyses were carried out with fixed effects. For all the meta-analyses, summary estimates along with 95% confidence intervals (95% CIs) were reported. Heterogeneity among studies was assessed using I² statistics. We investigated possible causes of heterogeneity through subgroup analyses, comparing participants in institutional vs. non-institutional settings. The risk of publication bias in studies reporting odds ratios was not assessed due to an insufficient number of studies (i.e., <10) included in each meta-analysis. For all the statistical analyses (see Supplementary Figure S1), the software STATA 13/SE was used.
3. Results
Of the 3993 records obtained from the analysis of the databases, adopting the search strategy described in the Materials and Methods section, 442 were selected for reading the full text, 181 of which were included as they met the inclusion criteria and satisfied the quality assessment (see Figure 1 and Supplementary Table S2). A total of 168 studies were cross-sectional, four were case–control studies and nine were cohort studies.
3.1. Prevalence of Caries
The prevalence of caries was expressed in the six types of disadvantaged subjects, starting in the description with those most affected, such as prisoners with 77% ([95% CI 66–85%]; 803 participants, three studies, I2 = 90%) [22,23,24], elderly people with 62% ([95% CI 50–73%]; 38,133 participants, 24 studies, I2 = 99.7%) [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] (Figure 2), alcohol and drug abusers with 60% ([95% CI 56–64]; 592 participants, two studies, I2 = not assessable) [49,50], immigrants with 65% ([95% CI 18–99%]; 878 participants, three studies, I2 = 99.1%) [39,51,52], followed by pregnant women with 29% ([95% CI 8–56%]; 506 participants, three studies, I2 = 97.4%) [53,54,55]. All groups showed high scores of prevalence.
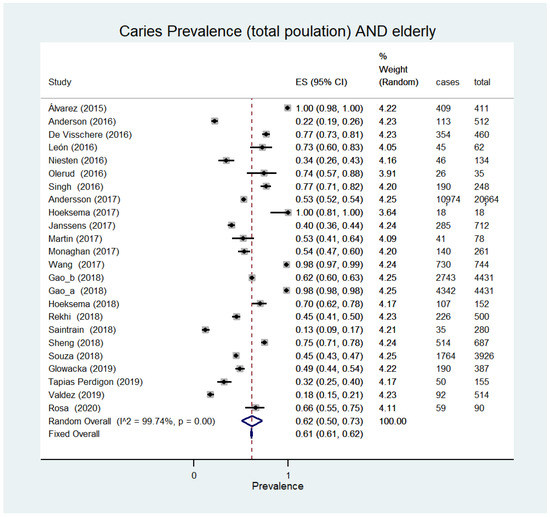
Figure 2.
Caries prevalence (total population) AND elderly.
When disadvantaged subjects were compared with the general population, they had a higher level of caries. Low-income subjects, indeed, have a double probability of suffering from caries (OR 2.2 [95% CI 1.7–2.7], p < 0.05; 6524 participants, two studies) [56,57], while subjects with a low level of education showed a greater than one and a half times probability (OR 1.6 [95% CI 1.42–1.9], p < 0.05; 5653 participants) [57], with a similar odds ratio to immigrants (OR 1.66 [95% CI 1.29–2.13], p < 0.05; 3738 participants) [58] and individuals living in rural areas (OR 1.6 [95% CI 1.2–4.3], p = 0.01; 280 participants) [59].
3.2. Caries Experience (DMFT)
Caries experience (DMFT) was calculated in six types of disadvantaged individuals, of which the elderly were those with the highest DMFT 18.7 SD 2.4 ([95% CI 13.5–24]; 1160 participants, 17 studies) [25,28,30,31,34,40,41,44,48,60,61,62,63,64,65,66], followed by homeless subjects with DMFT 17.3 SD 0.4 ([95% CI 12.6–22.1]; 100 participants, two studies) [67,68], immigrants with 14.9 SD 0.9 ([95% CI 9.6–18.7]; 843 participants, two studies) [51,52], alcohol and drug abusers with 12.9 SD 0.8 ([95% CI 11.2–14.6]; 1891 participants, nine studies) [49,50,69,70,71,72,73,74,75], low-income people with9.9 SD 0.5 ([95% CI 3–16.7];3043 participants, two studies) [60,76], low-education people with 9.8 SD0.03 ([95% CI 9.4–10.2]; 3043 participants, two studies) [60,76] and prisoners with 8.9 SD 0.8 ([95% CI 6.3–10.4]; 802 participants, three studies) [22,23,24]. Lower DMFT was found in sex workers with 2.3 (249 participants) [77] and in subjects who work without any specific qualification with 2.9 (510 participants) [78].
In all three types of disadvantaged individuals in whom caries experience was compared with the general population, DMFT was higher in socially vulnerable people. Specifically, a greater probability of having a higher DMFT index was found in low-education people (OR 1.40 [95% CI 1.29–1.52], p < 0.05; 6051 participants) [57], in low-income people (OR 3.7 [95% CI 2.8–4.6], p < 0.05; 1695 participants, two studies, I2 = 78%) [56,76] and in professionals who sustain an excessive hourly workload (>40 h of overtime) (OR 2.56 [95% CI 1.23–5.33] p = 0.012 to OR 3.01 [95% CI 1.13–7.97] p = 0.027; 950 participants) [79,80]. Moreover, institutionalized elderly people (resident in care homes) showed a higher caries experience than non-institutionalized elderly people with a DMFT 25.4 SD 2.1 ([95% CI 19.9–30.9]; 2608 participants, six studies) versus 16.1 SD 2.1 ([95% CI 11.2–21]; 8276 participants, nine studies) [29,31,34,40,41,44,48,60,61,63,64,81,82]. This difference between the two was essentially due to an increased number of teeth lost because of caries, with MT 21.4 SD 2.9 ([95% CI 12.2–30.6]; 2123 participants, seven studies) in institutionalized elderly individuals versus 9.7 SD 0.5 ([95% CI 8.4–11]; 7641 participants, four studies) in non-institutionalized ones [29,31,34,40,41,48,62,63,64,66,81].
3.3. Gingivitis
Gingivitis was noted in six different types of disadvantaged individuals, two of which showed the highest prevalence, such as alcohol and drug abusers with 82% ([95% CI 43–100%]; 357 patients, three studies, I2 98.8%) [71,72,75] and prisoners with 63% ([95% CI 54–72%]; 802 patients, three studies) [22,23,24]. High prevalence values were also found in pregnant women with 41% ([95% CI 34–49%]; 2242 participants, nine studies) [53,54,55,83,84,85,86,87,88] (Figure 3) and the elderly with 41% ([95% CI 29–52%];11,048 participants, 15 studies) [26,28,35,39,43,47,65,66,81,89,90,91,92,93,94]. Lower prevalence values were found in subjects with low levels of education (19% [95% CI 18–19%]; 75,095 participants, two studies, I2 = not assessable) [95,96] and low income (19% [95% CI 18–19]; 54,593 participants, two studies, I2 = 0.00) [93,94] and in immigrants (15% [95% CI 12–18%]; 746 participants, two studies, I2 = 0.00) [39,51].
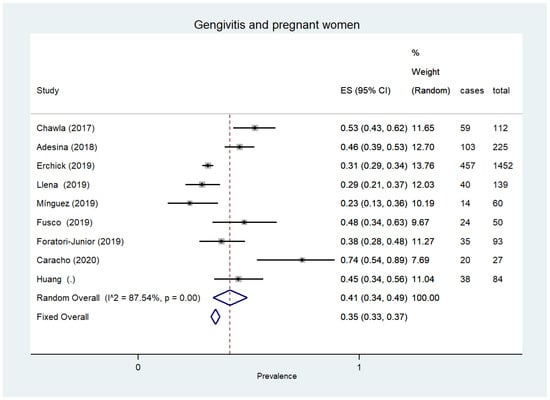
Figure 3.
Gingivitis and pregnant women.
When a comparison was made, disadvantaged people showed a higher prevalence of gingivitis than non-disadvantaged people. In particular, gingivitis was more prevalent in people with low education than in individuals with higher education (OR 2.6 [95% CI 2.5–2.7%], p < 0.05; 75,095 participants, two studies, I2 = 99.1%) [95,96], in low-income people (18.8% [n. = 5615/75,095]) versus higher-income people (7, 5% [n. = 5615/75,095]) [93,94] and in drug addicts versus the general population (39.6% vs. 28.4%, p < 0.001; 200 participants) [75].
3.4. Periodontitis
In the included studies, the presence of periodontitis was expressed by the Community Periodontal Index (CPI 3 or 4) or with at least one gingival site with ≥4 mm of periodontal pocket depth (PPD) or with ≥4 mm loss of clinical attachment (CAL). The prevalence of periodontitis has been reported in seven types of vulnerable individuals. Considering the number of published studies, most of them (12 studies) were focused on the elderly, who showed a prevalence value of 53% ([95% CI 42–63]; 6832 participants, 12 studies, I2 = 98.5%) [28,43,47,66,81,89,90,91,92,94,97,98] (Figure 4). Five studies described the prevalence of this disease in pregnant women with a value of 34% ([95% CI 13–58%]; 1757 participants, five studies, I2 = 97.6%) [54,83,84,87,88]. Moreover, three studies evaluated immigrants with a prevalence score of 40% ([95% CI 25–56%]; 1625 participants, three studies, I2 = 91.4) [39,52,99] and two studies involved subjects having a low level of education with a score of 56% ([95% CI 54–59%]; 1496 participants, two studies, I2 = not assessable) [95,100]. In the remaining groups with vulnerabilities, the prevalence data were described through single studies evaluating unskilled workers (51.3% [n. = 261/510]) [78], drug abusers (43% [n. = 46/106]) [101] and low-income subjects (31.0% [n. = 690/2149]) [102].
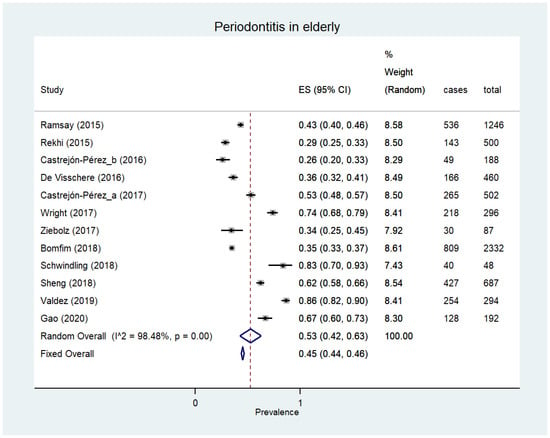
Figure 4.
Periodontitis in the elderly.
In the comparative studies, periodontitis was more prevalent and/or severe in socially disadvantaged subjects than in the general population. This comparison described five different types of vulnerable individuals, as follows. In elderly subjects (≥75 years) compared to young ones (25–44 years), there was a higher probability of suffering from periodontal disease (OR 1.68 [1.30–2.17], p < 0.001; 1693 participants) [95]. Likewise, low level education individuals showed an increased probability of having this oral disease than more educated people (OR 2.5 [95% CI 2.2–2.8]; 6036 participants, two studies, I2 = 91.6) [103]. Conversely, greater education was a protective element, reducing the probability of suffering from moderate–severe (OR 0.25 [0.17–0.38] p < 0.01) or severe (OR 0.29 [95% CI 0.17–0.50], p < 0.01) periodontitis, as shown in a study of 8886 participants [104]. Low-income individuals, when compared to those with a more stable or higher income, showed a greater prevalence of periodontitis (31.0% [n. = 690/2149] vs. 23.2% [n. = 516/2216] p < 0.001) [100] or a greater probability of being affected by this oral disease (OR 1.35 [1.15–1.58], p < 0.05; 17,583 participants) [102]. In immigrants without citizenship of their host country, compared to those who obtained it, an increased probability of suffering from periodontitis was demonstrated (OR 1.95 [1.42–2.67], p < 0.05; 3738 participants) [58]. Subjects who were addicted to substances such as crack and/or cocaine were found to have a triple probability of suffering from periodontitis (OR 3.44 [1.51–7.86], p < 0.01; 106 participants) and an increased mean periodontal pocket value (PPD 2.84 SD 0.76 vs. 2.55 SD 0.73 mm, p = 0.04; 106 participants) [101].
3.5. Complete Edentulism
The prevalence of edentulism was reported in four types of vulnerable individuals. In the elderly, edentulism was found to affect almost a third of the population of participants (32% [95% CI 28–37]; 116,284 participants, 56 studies, I2 = 99.6%) [26,27,28,31,32,33,34,35,36,37,38,39,42,44,46,47,60,63,66,81,90,91,92,95,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136], while in subjects with a low education level the prevalence was 17% ([95%CI17–31]; 2519 participants, three studies, I2 = 97.9%) [56,137,138] and 3% in drug abusers ([95% CI 2–5%]; 666 participants, three studies, I2 = 0.00) [50,72]. Finally, in low-income people, although based on the data expressed in a single study, the edentulous showed a prevalence of 22.6% (n. = 152/672) [137].
When a comparison was made, socially vulnerable individuals in all studies were more affected by edentulism than non-vulnerable ones, as described in low-income subjects (22.6% [n. = 152/672] vs. 3.5 [68/1934], p < 0.001) [137], low-education subjects (OR 6 [95% 3.3–10.7], p = 0.005; 6078 participants, three studies, I2 = 80.8%) [56,137,138], drug abusers (4.58% vs. 1.96%, p < 0.001; 517 participants) [50] and in black subjects (ethnic minority) (9.7% [n. = 228/2352] vs. 4.3% [n. = 335/7630], p < 0.001) [137].Similarly, the elderly (≥65 years), when compared to younger individuals (50–64 years), were more than twice as likely to be edentulous ((OR 2.15), p < 0.001; 15,473 participants) [139]. Moreover, institutionalized elders were found to have a higher edentulous prevalence (36% [95% CI 29–44]; 10,998 participants, 17 studies) [28,34,37,38,60,63,81,111,113,118,120,123,125,130,132,135] than non-institutionalized ones (25% [95% CI 21–30]; 89,115 participants, 31 studies), with a statistically significative difference (p < 0.05) [26,27,31,35,36,42,44,46,47,90,91,92,97,105,106,107,108,109,112,113,116,119,121,122,124,127,128,129,131,133].
3.6. Partial Tooth Loss (Partial Edentulism)
In nine categories of socially disadvantaged subjects, data on tooth loss outcome were expressed. All the studies agree on a greater tooth loss among socially disadvantaged subjects compared to the general population. The results of this outcome have been described for single types of vulnerable populations.
3.6.1. The Elderly
More than half of the elderly showed a non-functional dentition for chewing (≤20 remaining teeth) (56% [95% CI 50–62]; 103,770 participants, 26 studies, I2 = 99.7%) [28,35,42,46,60,66,92,96,105,106,111,112,117,118,119,130,131,132,135,140,141,142,143,144,145,146] and more than a third of them a dentition with severe functional impairment (<10 remaining teeth) (36% [95% CI 29–43]; 42,964 participants, eight studies, I2 = 99.5) [96,105,117,118,142,143,145,146].
3.6.2. Low-Education People
In terms of prevalence, low-education individuals, when compared to the reference group, showed an increased risk of tooth loss (OR 4.9 [95% CI 0.7–33.9], p = 0.083; 11,565 participants, two studies, I2 = 61.2%) [147,148] or had non-functional dentition (≤20 remaining teeth) (OR 2 [95% CI 0.97–4.1], p = 0.076; 5814 participants, two studies, I2 = 61.2%) [57,149]. Furthermore, they are more likely to have fewer teeth than the population median number (59.2%, n. = 734/1289 vs. 42.7%, n. = 216/538, p < 0.001) [102]. On the contrary, a high degree of education increases the prevalence of subjects without tooth loss (51.9% [n. = 809/1559] vs. 60.6% [n. = 1064/1753] p < 0.001; 6710 participants) [150]. Considering the number of residual teeth as an outcome, low income was found to be a risk factor of tooth loss. This concept was expressed as the average number of teeth per capita (23.4 SD2.6 vs. 26.7 SD 1.1, p < 0.01; 36,506 participants) [151,152], as the average difference in number of teeth (MD −0.279 [−3.48 to −2.10] p < 0.05; 5084 participants) [153] and, in addiction, as the probability of having a reduced number of teeth in terms of mean ratio (MR 0.93 [0.93–0.94], p < 0.001; 9564 participants) [154] or risk ratio (RR0.79 [95% CI 0.75–0.83], p < 0.05) [155]. The prevalence of severe tooth loss (<10 remaining teeth) also appeared to be conditioned by a low level of education, with similar scores in both men (OR 2.71 [95% CI 2.27–3.24], p < 0.001) and women (OR 3.00 [95% CI 2.31–3.90], p < 0.001) as reported in a study involving 34,975 participants [156].
3.6.3. Low-Income People
In terms of prevalence, the low income compared to the reference population was more likely to have both non-functional dentition (≤20 remaining teeth) (OR 3.9 [95% CI 3.2–4.8], p < 0.05; 5440 participants, two studies, I2 = not assessable) [148,157] and a higher percentage of subjects with a lower than average number of teeth (60.2% [n. = 516/906] vs. 47.2% [n. = 326/714 ], p < 0.001) [102]. Conversely, higher income increased the likelihood of a functional dentition (≥20 remaining teeth) (OR 1.39 [1.24–1.56], p < 0.05; 9564 participants) [158]. In terms of the number of residual teeth, low-income people were more likely to show fewer teeth than control group individuals (24.48 SD 0.05 vs. 21.81 SD 0.13, p < 0.001; 36,026 participants) [152]. This increased tooth loss was also expressed in terms of mean difference (MD −0.69 [–1.22 to –0.15], p < 0.05) [153] and of higher probability (mean ratio 1.97, [CI 1.76–2.20], p < 0.001; 9564 participants) [154].
3.6.4. Ethnic/Race Minorities
White people compared to black people (ethnic minority) showed a lower prevalence of loss of functional dentition with ≤20 residual teeth (17.8% [n. = 529/2959] vs. 50.3% [n. = 255/507], p < 0.001) [159], as well as an increased probability of maintaining a functional dentition (OR 1.10 [1.01–1.20], p < 0.05; 9564 participants) [158]. Additionally, in a study conducted on 6366 Brazilians, ethnic minorities were more likely to lose functional dentition in adulthood (40 years) than non-Hispanic whites, who represented the reference group, with an odds ratio that ranged from 1.41 (0.88–2.25) to 2.55 (1.39–4.66) [157].
3.6.5. Populations Living in Rural Areas
Living in a rural area was a risk factor for tooth loss (OR 0.68 (0.56–0.82), p < 0.05; 3255 participants) [102], while residing in an urban area was a protective factor (OR 1.22 (1.02–1.46), p = 0.021; 3767 participants) [160]. Even in the most severe cases of tooth loss (more than half of teeth being missing), the rural population was more affected than the urban population (70% [n. = 1576/2796] vs. 52.8% [1220/2796], p < 0.01) [161].
3.6.6. Subjects with Precarious/Unhealthy Working Conditions
Two studies have dealt with tooth loss in this type of vulnerability. In one study, unskilled workers, when compared with professionals, showed a higher probability of not functional dentition with <20 remaining teeth (OR 1.74 [1.15–2.62], p = 0.009; 592 participants) [162]. In the second study, lack of job stability was described as related to greater tooth loss in both males (OR 1.55 [1.18, 2.04], p < 0.05) and females (OR 1.44 [1.16, −1.79], p < 0.05), evaluating2652 participants [163].
3.6.7. Subjects with Negative Experiences in Childhood
In a study of 6427 participants, the likelihood of partial or total tooth loss by the age of 50 was increased in those individuals who during their childhood experienced the loss of at least one parent or their divorce (OR 1.93 [1.52–2.46], p < 0.001), physical abuse (OR 1.33 [1.03–2.06], p < 0.05), cigarette smoking (OR 1.76 [1.29–2.39], p < 0.01) or poverty (OR 1.81 [1.37–2.38], p < 0.001) [102].
3.7. Dental Service Attendance
All four types of socially vulnerable individuals where this outcome was noted showed a high degree of irregular dentist attendance, involving more than half of the participants evaluated. Specifically, this bad habit affected 75%of the homeless ([95% CI 73–76%]; 2530 participants, two studies) [67,68], 66% of pregnant women ([95%CI48–82]; 5103 participants, eight studies, I2 = 99%) [54,83,84,164,165,166,167,168], 55% of immigrants ([95% CI 21–87%]; 1351 participants, five studies) [51,169,170,171,172] (Figure 5) and 54% of the elderly ([95% CI 43–65%]; 33,430 participants, 19 studies, I2 = 99.7%) [33,36,41,46,47,90,91,96,97,106,110,116,126,132,139,142,173,174,175].
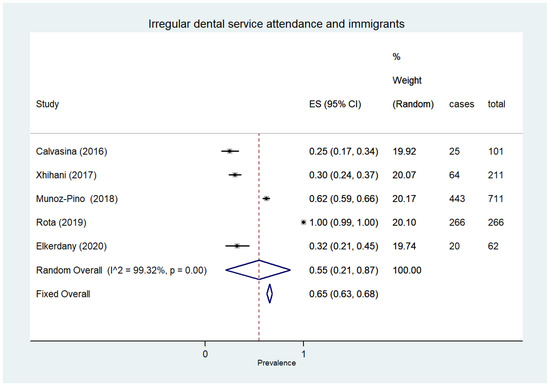
Figure 5.
Irregular dental service attendance and immigrants.
Furthermore, socially vulnerable people showed a greater tendency to visit the dentist more irregularly than the general population. A low level of education, for example, was identified as a factor that hindered a regular patient–dentist relationship (OR 0.68, 95% CI 0.48–0.95, p = 0.004) [176], favoring habits of irregular attendance of the dental service (OR 1.33 [1.26–1.40], p≤ 0.01; 90,845 participants) [177]. On the contrary, a high cultural level facilitated a regular relationship with the dentist (OR 2.07 [1.85–2.31], p = 0.001; 12,532 participants) [178]. Similarly, low income seemed to increase an irregular dental service attendance, with the data expressed in terms of odds ratio (OR 2.8 [95% CI 0.8–4.2], p < 0.07; 100,709 participants, four studies, I2 = 99.3%) [142,169,177,179] or risk ratio (RR 2.44 [2.17–2.73], p < 0.05; 3323 participants) [179], while high income was a preventive factor favoring a regular dental service attendance (OR 0.855 [0.803–0.911] p < 0.001; 12,532 participants) [177]. Considering the phenomenon of immigration, people living in countries hosting immigrants are more likely to visit the dentist regularly than immigrants (OR 1.24 [1.14–1.35], p < 0.05; 2648 participants) [180]. Finally, the lack of insurance coverage contributed to an increase in the irregular frequency of dental services (OR 6.54 [3.0, 14.33], p < 0.05; 154 participants) [179]. On the contrary, insurance coverage was a factor favoring regular visits to the dentist, with this outcome being described in terms of increased prevalence (72.3% vs. 53.3%, p < 0.001) [181] and probability of visiting the dentist (RR 1.8 [95% CI 1.4–2.3], p < 0.05; 2702 participants, two studies, I2 = not assessable) [175,182]. The type of insurance also affected the degree of attendance, and in fact, individuals with private insurance showed a greater aptitude to visit the dentist regularly than those covered by public insurance such as Medicare (OR 1.25–1.95), p < 0.001) or Medicaid (OR 1.29 (1.10–1.51), p = 0.001), as reported in a study conducted in the USA on a population sample of 402,077 participants [183].
3.8. Oral Health-Related Quality of Life (OHRQoL)
This outcome was described in three types of vulnerable individuals. In the elderly, one third of the subjects examined showed a reduced quality of life due to oral health problems such as pain, difficulty chewing or swallowing and psychological and/or relational discomfort due to the condition of their teeth (28% [95% CI 19–38]; 16,672 participants, 11 studies, I2 = 99.3%) [45,111,116,125,132,140,184,185,186,187,188], while the prevalence of this outcome in immigrants was 55% ([95% CI 21–87%]; 709 participants, three studies, I2 = 99.3%) [52,189,190]. Finally, in the only comparative study carried out, subjects living in rural areas compared to those in urban areas presented a worse quality of life related to dental or periodontal disorders measured with a specific scale called the Oral Health Impact Profile—14-item questionnaire (11.49 SD 9.733 vs. 5.88 SD 5.588, p < 0.001; 100 participants) [191].
3.9. Oral Health Perception
The most relevant data were reported in pregnant women, where about half of them showed a worse perception of their oral health (45% ([95% CI 25–66%]; 515 participants, four studies, I2 = 95.7%) [54,55,167,168], while this negative perception was less prevalent among the elderly (28% [95% CI 19–38%]; 67,049 participants, 20 studies, I2 = 99.3%) [28,36,38,41,45,46,92,96,111,113,123,125,139,140,143,173,174,192,193,194].
When compared, socially vulnerable individuals presented a worse perception of their oral health status than the general population. This increased degree of negative perception was expressed in terms of prevalence (77.5% n. = 224/631 vs. 22.5% n. = 65/342, p < 0.001) [195], absolute difference (AD 20.49% [4.95–36.4]; 14,960 participants) [196] and probability, as published in two cross sectional studies (OR 2.8 [95% CI 0.5–14.7], p = 0.073; 65,363 participants, I2 = 99.0%) [180,197] and in a prospective study (RR1.61 [1.28–2.03] p < 0.05; 2812 participants) [155].This perception of poor oral health was also found to be more likely in low-income subjects when compared with the reference population, with this outcome being expressed in terms of odds ratio (2.2 [95% CI 1.7–2.6], p < 0.05; 68,966 participants, four studies, I2 = 61.2%) [180,197,198,199], risk ratio (3.18 [2.13–4.74], p < 0.05; 2812 participants) [155] and absolute difference (AD 15.77% [12.77–18.77]; 14,960 participants) [196]. Even among skilled workers subjected to stress due to excessive working hours (>40 h of overtime), an increased negative perception of their oral health was found compared to subjects working in less stressful conditions (OR 3.25 (1.66–6.35), p < 0.001; 950 participants) [79,80].
3.10. Emergency Room Treatments Due to Non-Traumatic Injuries
In two groups of socially vulnerable individuals, a greater use of emergency room treatment for non-traumatic dental injuries was demonstrated than with the non-vulnerable population, specifically black individuals (ethnic minority), who had nearly five times more visits (1118 participants) [200], and those without any health insurance, as expressed in the studies of Franciscatto and co-workers (OR 1.36 [1.24–1.49], p < 0.001; 6282participants) and of DeLia (2015) (p < 0.001; 96,787 participants) [201,202].
3.11. People with Multiple Social Vulnerabilities
Where subjects with two (or more) social vulnerabilities were compared with those with a single vulnerability, the former showed a worse dental and/or periodontal health status. For example, when older people with a low level of education were compared with those who were more educated, a higher prevalence of caries was found. (30.8% [n. 961/3119] vs. 11.7% [n. = 365/3119], p < 0.05) [118], while a high level of education was found as a preventive factor against caries for elderly people (OR 0.81 [0.74–0.89], p = 0.001; 4431 participants) [29]. Similarly, low income, when added to old age, increased the prevalence of caries (28.6% [n. = 892/3119) vs. 9.9% [n. = 365/3119], p < 0.05) [118]. In a study conducted by Martin and co-workers, older non-Hispanic whites residing in urban areas appeared less affected by tooth decay than Mexican-American or black (race minorities) elderly people residing in rural areas (p < 0.05) [36]. Education was also noted as a preventive factor against severe periodontal disease in the elderly (p = 0.004; 30,427 participants) [203], decreasing the likelihood of suffering from this oral disease (RR 0.96 [0.95–0, 97], p < 0.05; 2332 participants) [89]. Low income also seemed to increase the prevalence of periodontitis in the elderly (p < 0.001; 687 participants) [43] as well as the likelihood of suffering from this disease (OR 1.39 [1.01–1.91], p < 0.05; 2147 participants) [204], while high income was a prevention factor against periodontitis (RR 0.91 [0.86 0.96], p < 0.05; 2332) [89]. Finally, a rural environment seemed to make the elderly more susceptible to periodontitis than an urban environment (p = 0.007; 30,427 participants) [205].
Furthermore, low income in pregnant women was a risk factor for periodontitis (OR 0.61 [0.46–0.81], p = 0.001, 160 participants) [88]. Similarly, poor quality of life related to oral health in pregnant women appeared to be linked to unemployment status, low levels of education and immigration status (p < 0.05) [167].
3.12. Quality Assessment of Included Studies
Using JBI’s Critical Appraisal Tool Checklist, the following considerations were performed on the study methodology of included papers (see Supplementary Table S2). Of the 168 included cross-sectional studies, 126 studies met 6/8 criteria and 42 studies met 8/8 criteria. Of the nine included cohort studies, seven studies met 9/11 criteria and two studies met 11/11 criteria. Of the four included case–control studies, all the studies met 8/10 criteria. Of the 181 selected articles, in 137 studies confounding factors were not clearly investigated.
4. Discussion
The socially vulnerable who live on the margins of society with reduced resilience to adverse events constitute a very heterogeneous typology of individuals with different traits and habits regarding age, sex, living environment, origin, socio-economic status and beliefs. Despite these differences, in this systematic review of the literature, it was found that socially vulnerable subjects showed shared traits in terms of their oral health. The first common trait was a higher prevalence and/or severity of caries and periodontal disease (and related tooth loss) compared to the general population. Specifically, our study showed that caries in vulnerable individuals, with a prevalence ranging between 39% and 77.4%, was greater than 29.4% of the general population, indicating the global burden of this disease in 2017 [206]. This increased prevalence was also confirmed by studies included in this review, which made a direct comparison between socially disadvantaged and non-disadvantaged individuals. Additionally, in relation to the severity of the caries (measured by the DMFT index), socially disadvantaged individuals showed higher scores than non-vulnerable people, with values that in most of the different types of vulnerable subjects ranged between 11.8 and 18.7.
A similar epidemiological pattern was found in periodontitis, with higher prevalence scores for socially disadvantaged subjects showing percentages between 43% and 60%, with the exception of pregnant women and low-income subjects where the percentages were less. As with caries and periodontitis, complete edentulism among the vulnerable (where prevalence ranged from 16 to 27% in our study) showed significantly higher scores than the 3.3% of the general population, as reported in 2017 [206]. Additionally, taking into account the partial edentulism in its two clinical variants (<21 or <9 residual teeth in the oral cavity), socially vulnerable people were more affected than individuals with better social conditions.
Other common traits found in different types of vulnerable people were the perception of an unhealthy oral state and a poor oral health-related quality of life (OHRQoL). Moreover, socially vulnerable people were less likely to visit the dentist regularly than non-vulnerable ones. This bad habit makes it more difficult for dental professionals to protect their compromised oral health. Probably a new model of health policy should be developed (in addition to the existing one) with solutions able to meet socially vulnerable subjects in their environment without waiting for the patient to visit the dental office. In other words, this health policy should be based more on education, prophylaxis and minimally invasive treatment of oral diseases, also using innovative transportable devices and instruments in order to reach people living on the margins of the social network. Atraumatic restorative treatment (ART) is the best known of these types of easy intervention, which can be performed outside the dental office [207].
Another shared trait noted among socially disadvantaged subjects was the presence of a worsening of dental–periodontal health when more social vulnerabilities are pooled in the same individuals. This particular worsening is not unlike that described in the literature where multiple health vulnerabilities (with chronic illnesses) occur in a single subject [208].
In this study, we did not include disabled people among the categories of social vulnerability, as they may be affected by a double vulnerability, social and sanitary, at the same time. However, it must be taken into account that social and medical vulnerability combined increase the risk factors for caries and periodontal disease [209].
In recent years, the literature has shown that caries and periodontal disease cause, as a complication, an increased risk of onset of multiple systemic diseases such as cardio-vascular disease, dysmetabolic syndrome, respiratory tract infection and preterm birth in the general population [210,211,212,213]. Based on data described in this review, the risk of these complications should be considered increased for socially disadvantaged subjects due to their more compromised oral health status. A further complication for the vulnerable could be the psychological impact of a bad dental condition (bad smile) on self-esteem, which could worsen their social exclusion situation [214].
No reviews have been found in the literature that dealt with dental–periodontal health in socially vulnerable individuals as a whole. However, some reviews were found that reported scientific evidence of oral health for single individual types of socially disadvantaged individuals. These reviews provided overall results in agreement with the present study in highlighting a health disparity between socially vulnerable and non-vulnerable individuals. The concordance of the results between this review (consisting of studies published in the last five years) and the others found in the literature (including most studies prior to the last five years) showed that the problem of oral health in socially disadvantaged subjects did not improve over time. On the contrary, there is a growing social polarization of dental–periodontal diseases (as demonstrated in this review), even in the context of global improvement concerning caries and periodontitis [215].
Limitations
- Considering the scope of providing an overall view of dental–periodontal health involving all types of socially vulnerable subjects, this review does not present a complete picture for two reasons. The first reason is that in the literature (consequently in our review), not all types of vulnerable subjects are mentioned in relation to their dental–periodontal health. The second reason is that in many groups of vulnerable subjects, not all the dental–periodontal health outcomes (those indicated in the “Materials and Methods” section of this review) were described, and in some cases even the primary ones were missing.
- The high level of heterogeneity (I2 > 90%) of results relative to the majority of the outcomes in this review reduces the reliability of conclusions on the dental–periodontal health of vulnerable subjects, who were the focus of our research
- This systematic review did not take into account the differences between developing and underdeveloped countries in the assessment of socially vulnerable people. This was to limit any subgroup analysis (especially in some groups of vulnerable subjects described by only a few studies with a reduced number of participants) in order to avoid the risk of compromising the accuracy of the results by reducing the sample size of enrolled individuals.
5. Conclusions
Despite a certain degree of incompleteness of the data due to the complexity of this topic, the results of our review supported the hypothesis of a more compromised dental–periodontal status in socially disadvantaged subjects than in the non-vulnerable population. The increased risk of dental–periodontal diseases was a finding found in every type of social vulnerability and seemed to worsen in the presence of pooled vulnerabilities. Furthermore, according to the results of this review, to date the health policies adopted by the National Health Systems in most countries seem inadequate to reduce the inequalities in oral health between socially vulnerable and non-vulnerable people. Therefore, the results of this review will hopefully stimulate health policy makers to adopt measures, both legislative and economic, which are more protective of socially vulnerable subjects. In fact, the loss of oral health inevitably creates a negative impact on the overall health of the vulnerable worldwide, with significant financial consequences for National Health Systems and for the global general population.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/ijerph182312360/s1, Table S1: Strategy search, Table S2: Quality assessment, Figure S1: Statistical analysis not included in the main text, Table S3: PRISMA checklist.
Author Contributions
Conceptualization, S.C. and G.L. (Giuseppe Lomurno); methodology, C.V. and G.L. (Guido Lombardo); software, M.O. and C.V.; validation, G.L. (Guido Lombardo), M.O. and S.C.; formal analysis, S.C. and M.O.; investigation, C.V., G.L. (Guido Lombardo), S.P. and S.C.; resources, G.L. (Giuseppe Lomurno); data curation, M.N. and A.P.L.; writing—original draft preparation, C.V. and G.L. (Guido Lombardo); writing—review and editing, G.L. (Guido Lombardo) and S.P.; visualization, S.P. and A.P.L.; supervision, S.C. and G.L. (Giuseppe Lomurno); project administration, S.C. and M.N.; funding acquisition, G.L. (Guido Lombardo) and S.P. All authors have read and agreed to the published version of the manuscript.
Funding
This study is a multicenter implementation project promoted and funded by the National Center for Disease Prevention and Control—Ministry of Health (CCM 2019).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
The authors acknowledge the contributions of Simona Lanari for sharing prior knowledge on the topic of socio-economic vulnerability and Sheila Tabakoff for editing the English text.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- Kåks, P.; Målqvist, M. Peer support for disadvantaged parents: A narrative review of strategies used in home visiting health interventions in high-income countries. BMC Health Serv. Res. 2020, 20, 682. [Google Scholar] [CrossRef]
- Stormacq, C.; Van den Broucke, S.; Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot. Int. 2019, 34, e1–e17. [Google Scholar] [CrossRef] [PubMed]
- Rune, H.C.; Nielsen, H.O. Disparities in Quality of Work Linked to Education and Socioeconomic Status; European Foundation for the Improvement of Living and Working Conditions: Dublin, Ireland, 2009. [Google Scholar]
- Mabhala, M.A.; Yohannes, A.; Griffith, M. Social conditions of becoming homelessness: Qualitative analysis of life stories of homeless peoples. Int. J. Equity Health 2017, 16, 150. [Google Scholar] [CrossRef] [PubMed]
- Frick, K.; Bopp, A. Poverty: Insurance Theory and the Medically Uninsured. Atl. Econ. J. 2005, 33, 451–459. [Google Scholar] [CrossRef]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Aldridge, R.W.; Story, A.; Hwang, S.W.; Nordentoft, M.; Luchenski, S.A.; Hartwell, G.; Tweed, E.J.; Lewer, D.; VittalKatikireddi, S.; Hayward, A.C. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: A systematic review and meta-analysis. Lancet 2018, 391, 241–250. [Google Scholar] [CrossRef]
- Moghaddam, L.F.; Vettore, M.V.; Bayani, A.; Bayat, A.H.; Ahounbar, E.; Hemmat, M.; Armoon, B.; Fakhri, Y. The Association of Oral Health Status, demographic characteristics and socioeconomic determinants with Oral health-related quality of life among children: A systematic review and Meta-analysis. BMC Pediatr. 2020, 20, 489. [Google Scholar] [CrossRef]
- Valtorta, N.K.; Moore, D.C.; Barron, L.; Stow, D.; Hanratty, B. Older Adults’ Social Relationships and Health Care Utilization: A Systematic Review. Am. J. Public Health 2018, 108, e1–e10. [Google Scholar] [CrossRef]
- Van der Zande, I.S.E.; van der Graaf, R.; Oudijk, M.A.; van Delden, J.J.M. Vulnerability of pregnant women in clinical research. J Med. Ethics 2017, 43, 657–663. [Google Scholar] [CrossRef]
- Waisel, D.B. Vulnerable populations in healthcare. Curr. Opin. Anaesthesiol. 2013, 26, 186–192. [Google Scholar] [CrossRef]
- Brooks, H.; Llewellyn, C.D.; Nadarzynski, T.; Pelloso, F.C.; De Souza Guilherme, F.; Pollard, A.; Jones, C.J. Sexual orientation disclosure in health care: A systematic review. Br. J. Gen.Pract. 2018, 68, e187–e196. [Google Scholar] [CrossRef]
- Allen, L.; Williams, J.; Townsend, N.; Mikkelsen, B.; Roberts, N.; Foster, C.; Wickramasinghe, K. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: A systematic review. Lancet Glob. Health 2017, 5, e277–e289. [Google Scholar] [CrossRef]
- Probst, L.F.; Pucca Junior, G.A.; Pereira, A.C.; Carli, A.D. Impact of financial crises on oral health indicators: An integrative review of the literature. Cien. Saude Colet. 2019, 24, 4437–4448. [Google Scholar] [CrossRef] [PubMed]
- Hurley, R. Legalise and regulate illicit drugs to reduce poverty, say campaigners. BMJ 2019, 364, l317. [Google Scholar] [CrossRef]
- Jepsen, S.; Blanco, J.; Buchalla, W.; Carvalho, J.C.; Dietrich, T.; Dörfer, C.; Eaton, K.A.; Figuero, E.; Frencken, J.E.; Graziani, F.; et al. Prevention and control of dental caries and periodontal diseases at individual and population level: Consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44 (Suppl.18), S85–S93. [Google Scholar] [CrossRef]
- González Navarro, B.; Pintó Sala, X.; Jané Salas, E. Relationship between cardiovascular disease and dental pathology. Systematic review. Med. Clin. 2017, 149, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Philadelphia, PA, USA, 2020. [Google Scholar]
- Priwe, C.; Carlsson, P. Oral Health Status of Male Swedish Citizens at Admission to Prison. J. Correct Health Care 2018, 24, 382–394. [Google Scholar] [CrossRef]
- Fotedar, S.; Chauhan, A.; Bhardwaj, V.; Manchanda, K.; Fotedar, V. Association between oral health status and oral health-related quality of life among the prison inmate population of kanda model jail, Shimla, Himachal Pradesh, India. Indian J. Public Health 2016, 60, 150–153. [Google Scholar] [CrossRef]
- Soares, G.H.; Mendonça, I.; Michel-Crosato, E.; Moysés, S.J.; Moysés, S.T.; Werneck, R.I. Impact of oral conditions on the quality of life of incarcerated women in Brazil. Health Care Women Int. 2019, 40, 776–787. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, L.; Liberman, J.; Abreu, S.; Mangarelli, C.; Correa, M.B.; Demarco, F.F.; Lorenzo, S.; Nascimento, G.G. Dental caries in Uruguayan adults and elders: Findings from the first Uruguayan National Oral Health Survey. Cad. Saude Publica 2015, 31, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Martin, N.R.; Kelly, S.M.; Brown, H.A. Oral Health Status of Older Adults Attending Senior Centers and Congregate Meal Sites in New Hampshire. J. Dent. Hyg. 2016, 90, 128–134. [Google Scholar] [PubMed]
- Andersson, P.; Renvert, S.; Sjogren, P.; Zimmerman, M. Dental status in nursing home residents with domiciliary dental care in Sweden. Community Dent. Health 2017, 34, 203–207. [Google Scholar]
- De Visschere, L.; Janssens, B.; De Reu, G.; Duyck, J.; Vanobbergen, J. An oral health survey of vulnerable older people in Belgium. Clin. Oral Investig. 2016, 20, 1903–1912. [Google Scholar] [CrossRef]
- Gao, Y.B.; Hu, T.; Zhou, X.D.; Shao, R.; Cheng, R.; Wang, G.S.; Yang, Y.M.; Li, X.; Yuan, B.; Xu, T.; et al. How Root Caries Differs between Middle-aged People and the Elderly: Findings from the 4th National Oral Health Survey of China. Chin. J. Dent. Res. 2018, 21, 221–229. [Google Scholar]
- Gao, Y.B.; Hu, T.; Zhou, X.D.; Shao, R.; Cheng, R.; Wang, G.S.; Yang, Y.M.; Li, X.; Yuan, B.; Xu, T.; et al. Dental Caries in Chinese Elderly People: Findings from the 4th National Oral Health Survey. Chin. J. Dent. Res. 2018, 21, 213–220. [Google Scholar]
- Głowacka, B.; Konopka, T. Needs for gerodontological treatment in the elderly living in Lower Silesia. Dent. Med. Probl. 2019, 56, 89–96. [Google Scholar] [CrossRef]
- Hoeksema, A.R.; Peters, L.L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A.; Visser, A. Health and quality of life differ between community living older people with and without remaining teeth who recently received formal home care: A cross sectional study. Clin. Oral Investig. 2018, 22, 2615–2622. [Google Scholar] [CrossRef]
- Hoeksema, A.R.; Spoorenberg, S.; Peters, L.L.; Meijer, H.; Raghoebar, G.M.; Vissink, A.; Wynia, K.; Visser, A. Elderly with remaining teeth report less frailty and better quality of life than edentulous elderly: A cross-sectional study. Oral. Dis. 2017, 23, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Janssens, B.; Vanobbergen, J.; Petrovic, M.; Jacquet, W.; Schols, J.M.G.A.; De Visschere, L. The oral health condition and treatment needs assessment of nursing home residents in Flanders (Belgium). Community Dent. Health 2017, 34, 143–151. [Google Scholar]
- León, S.; Bravo-Cavicchioli, D.; Giacaman, R.A.; Correa-Beltrán, G.; Albala, C. Validation of the Spanish version of the oral health impact profile to assess an association between quality of life and oral health of elderly Chileans. Gerodontology 2016, 33, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.L.; Boyd, L.D.; Tapias-Perdigón, H.; LaSpina, L.M. Oral Health Status of Independent Older Adults in Texas: An observational study comparing urban and rural areas. J. Dent. Hyg. 2017, 91, 40–47. [Google Scholar]
- Monaghan, N.; Karki, A.; Playle, R.; Johnson, I.; Morgan, M. Measuring oral health impact among care home residents in Wales. Community Dent. Health 2017, 34, 14–18. [Google Scholar] [PubMed]
- Niesten, D.; Witter, D.; Bronkhorst, E.; Creugers, N. Oral health-related quality of life and associated factors in a care-dependent and a care-independent older population. J. Dent. 2016, 55, 33–39. [Google Scholar] [CrossRef]
- Olerud, E.; Hagman-Gustavsson, M.L.; Gabre, P. Oral health status in older immigrants in a medium-sized Swedish city. Spec Care Dentist. 2016, 36, 328–334. [Google Scholar] [CrossRef]
- Rekhi, A.; Marya, C.M.; Nagpal, R.; Oberoi, S.S. Assessment of Oral Health Related Quality of Life Among the Institutionalised Elderly in Delhi, India. Oral Health Prev Dent. 2018, 16, 59–66. [Google Scholar]
- Rosa, R.W.; Samot, J.; Helmer, C.; Pourtau, G.; Dupuis, V.; Fricain, J.C.; Georget, A.; Dartigues, J.F.; Arrivé, E. Important oral care needs of older French people: A cross-sectional study. Rev. Epidemiol. SantePublique 2020, 68, 83–90. [Google Scholar] [CrossRef]
- Saintrain, M.V.L.; Saintrain, S.V.; Sampaio, E.G.M.; Ferreira, B.S.P.; Nepomuceno, T.C.; Frota, M.A.; Vieira-Meyer, A.P. Older adults’ dependence in activities of daily living: Implications for oral health. Public Health Nurs. 2018, 35, 473–481. [Google Scholar] [CrossRef]
- Sheng, X.; Xiao, X.; Song, X.; Qiao, L.; Zhang, X.; Zhong, H. Correlation between oral health and quality of life among the elderly in Southwest China from 2013 to 2015. Medicine 2018, 97, e10777. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Purohit, B.M.; Masih, N. Geriatric oral health predicaments in New Delhi, India. Geriatr. Gerontol. Int. 2016, 16, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.G.S.; Costa Oliveira, B.E.; Sampaio, A.A.; Lages, V.A.; Romão, D.A.; Martins, A.M.E.B.L. Contextual and Individual Determinants of Root Caries in Older People. Caries Res. 2018, 52, 253–261. [Google Scholar] [CrossRef]
- Tapias Perdigon, H.; Schneiderman, E.; Opperman, L.A. Oral health assessment of independent elders in Texas. Spec. Care Dentist. 2019, 39, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Valdez, E.; Wright, F.A.C.; Naganathan, V.; Milledge, K.; Blyth, F.M.; Hirani, V.; Le Couteur, D.G.; Handelsman, D.J.; Waite, L.M.; Cumming, R.G. Frailty and oral health: Findings from the Concord Health and Ageing in Men Project. Gerodontology 2020, 37, 28–37. [Google Scholar] [CrossRef]
- Wang, L.; Cheng, L.; Yuan, B.; Hong, X.; Hu, T. Association between socio-economic status and dental caries in elderly people in Sichuan Province, China: A cross-sectional study. BMJ Open 2017, 7, e016557. [Google Scholar] [CrossRef]
- Sordi, M.B.; Massochin, R.C.; Camargo, A.R.; Lemos, T.; Munhoz, E.A. Oral health assessment for users of marijuana and cocaine/crack substances. Braz. Oral Res. 2017, 31, e102. [Google Scholar] [CrossRef]
- Shetty, V.; Harrell, L.; Murphy, D.A.; Vitero, S.; Gutierrez, A.; Belin, T.R.; Dye, B.A.; Spolsky, V.W. Dental disease patterns in methamphetamine users: Findings in a large urban sample. J. Am. Dent. Assoc. 2015, 146, 875–885. [Google Scholar] [CrossRef]
- Muñoz-Pino, N.; Vives-Cases, C.; Agudelo-Suárez, A.A.; Ronda-Pérez, E. Comparing Oral Health Services Use in the Spanish and Immigrant Working Population. J. Immigr. Minor. Health 2018, 20, 809–815. [Google Scholar] [CrossRef]
- Høyvik, A.C.; Lie, B.; Grjibovski, A.M.; Willumsen, T. Oral Health Challenges in Refugees from the Middle East and Africa: A Comparative Study. J. Immigr. Minor Health 2019, 21, 443–450. [Google Scholar] [CrossRef]
- Adesina, K.T.; Ernest, M.A.; Tobin, A.O.; Isiaka-Lawal, S.A.; Adeyemi, M.F.; Olarinoye, A.O.; Ezeoke, G.G. Oral health status of pregnant women in Ilorin, Nigeria. J. Obstet. Gynaecol. 2018, 38, 1093–1098. [Google Scholar] [CrossRef]
- Chawla, R.M.; Shetiya, S.H.; Agarwal, D.R.; Mitra, P.; Bomble, N.A.; Narayana, D.S. Knowledge, Attitude, and Practice of Pregnant Women regarding Oral Health Status and Treatment Needs following Oral Health Education in Pune District of Maharashtra: A Longitudinal Hospital-based Study. J. Contemp. Dent. Pract. 2017, 18, 371–377. [Google Scholar] [CrossRef]
- Llena, C.; Nakdali, T.; Sanz, J.L.; Forner, L. Oral Health Knowledge and Related Factors among Pregnant Women Attending to a Primary Care Center in Spain. Int. J. Environ Res. Public Health 2019, 16, 5049. [Google Scholar] [CrossRef]
- Lambert, M.; De Reu, G.; De Visschere, L.; Declerck, D.; Bottenberg, P.; Vanobbergen, J. Social gradient in caries experience of Belgian adults 2010. Community Dent. Health 2018, 35, 160–166. [Google Scholar] [PubMed]
- Nogueira, J.S.; Pereira, A.C.; Frias, A.C.; Ambrosano, G.M.B.; Cortellazzi, K.L.; Guerra, L.M.; Cavalcante, D.F.B.; Bulgareli, J.V. Social capital and factors associated with the caries experience in adults—A population-based study in Brazil. Braz. Oral Res. 2019, 33, e118. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F.A.; Wang, Y.; Borrell, L.N.; Bae, S.; Stimpson, J.P. Disparities in oral health by immigration status in the United States. J. Am. Dent. Assoc. 2018, 149, 414–421.e3. [Google Scholar] [CrossRef]
- Tafere, Y.; Chanie, S.; Dessie, T.; Gedamu, H. Assessment of prevalence of dental caries and the associated factors among patients attending dental clinic in Debre Tabor general hospital: A hospital-based cross-sectional study. BMC Oral Health 2018, 18, 119. [Google Scholar] [CrossRef]
- Janssens, B.; Vanobbergen, J.; Petrovic, M.; Jacquet, W.; Schols, J.M.; De Visschere, L. The impact of a preventive and curative oral healthcare program on the prevalence and incidence of oral health problems in nursing home residents. PLoS ONE 2018, 13, e0198910. [Google Scholar] [CrossRef]
- Klotz, A.L.; Zajac, M.; Ehret, J.; Kilian, S.; Rammelsberg, P.; Zenthöfer, A. Short-Term Effects of a Deterioration of General Health on the Oral Health of Nursing-Home Residents. Clin. Interv. Aging 2020, 15, 29–38. [Google Scholar] [CrossRef]
- Mulic, A.; Tveit, A.B.; Stenhagen, K.R.; Oscarson, N.; Staxrud, F.; Jönsson, B. The frequency of enamel and dentin caries lesions among elderly Norwegians. Acta Odontol. Scand. 2020, 78, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Puturidze, S.; Margvelashvili, M.; Bilder, L.; Kalandadze, M.; Margvelashvili, V. Correlation of oral health status with general health in elderly living at residential homes in georgia. Georgian Med. News 2019, 292–293, 21–25. [Google Scholar]
- Sáez-Prado, B.; Haya-Fernández, M.C.; Sanz-García, M.T. Oral health and quality of life in the municipal senior citizen’s social clubs for people over 65 of Valencia, Spain. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e672–e678. [Google Scholar]
- Skośkiewicz-Malinowska, K.; Noack, B.; Kaderali, L.; Malicka, B.; Lorenz, K.; Walczak, K.; Weber, M.T.; Mendak-Ziółko, M.; Hoffmann, T.; Ziętek, M.; et al. Oral Health and Quality of Life in Old Age: A Cross-Sectional Pilot Project in Germany and Poland. Adv. Clin. Exp. Med. 2016, 25, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.A.C.; Law, G.; Chu, S.K.; Cullen, J.S.; Le Couteur, D.G. Residential age care and domiciliary oral health services: Reach-OHT-The development of a metropolitan oral health programme in Sydney, Australia. Gerodontology 2017, 34, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Stormon, N.; Pradhan, A.; McAuliffe, A.; Ford, P.J. Does a facilitated pathway improve access to dental services for homeless and disadvantaged adults? Eval. Program Plann. 2018, 71, 46–50. [Google Scholar] [CrossRef]
- Doughty, J.; Stagnell, S.; Shah, N.; Vasey, A.; Gillard, C. The Crisis at Christmas Dental Service: A review of an annual volunteer-led dental service for homeless and vulnerably housed people in London. Br. Dent. J. 2018, 224, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Aukštakalnis, R.; Jurgelevičius, T. The oral health status and behaviour of methadone users in Lithuania. Stomatologija 2018, 20, 27–31. [Google Scholar]
- Clague, J.; Belin, T.R.; Shetty, V. Mechanisms underlying methamphetamine-related dental disease. J. Am. Dent. Assoc. 2017, 148, 377–386. [Google Scholar] [CrossRef]
- Ye, T.; Sun, D.; Dong, G.; Xu, G.; Wang, L.; Du, J.; Ren, P.; Yu, S. The effect of methamphetamine abuse on dental caries and periodontal diseases in an Eastern China city. BMC Oral Health 2018, 18, 8. [Google Scholar] [CrossRef]
- Rafat, S.; Tessma, M.; Klinge, B.; Borg, S.; De Palma, P. Oral Health Among Swedish Patients with Substance Use Disorders—A Comparative, Cross-Sectional Study. Oral Health Prev. Dent. 2020, 18, 229–237. [Google Scholar]
- Manicone, P.F.; Tarli, C.; Mirijello, A.; Raffaelli, L.; Vassallo, G.A.; Antonelli, M.; Rando, M.M.; Mosoni, C.; Cossari, A.; Lavorgna, L.; et al. Dental health in patients affected by alcohol use disorders: A cross-sectional study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5021–5027. [Google Scholar]
- Marques, T.C.; Sarracini, K.L.; Cortellazzi, K.L.; Mialhe, F.L.; de Castro Meneghim, M.; Pereira, A.C.; Ambrosano, G.M. The impact of oral health conditions, socioeconomic status and use of specific substances on quality of life of addicted persons. BMC Oral Health 2015, 15, 38. [Google Scholar] [CrossRef]
- Rommel, N.; Rohleder, N.H.; Koerdt, S.; Wagenpfeil, S.; Härtel-Petri, R.; Wolff, K.D.; Kesting, M.R. Sympathomimetic effects of chronic methamphetamine abuse on oral health: A cross-sectional study. BMC Oral Health 2016, 16, 59. [Google Scholar] [CrossRef]
- Arrica, M.; Carta, G.; Cocco, F.; Cagetti, M.G.; Campus, G.; Ierardo, G.; Ottolenghi, L.; Sale, S.; Strohmenger, L. Does a social/behavioural gradient in dental health exist among adults? A cross-sectional study. J. Int. Med. Res. 2017, 45, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Nouaman, M.N.; Meless, D.G.; Coffie, P.A.; Arrivé, E.; Tchounga, B.K.; Ekouévi, D.K.; Anoma, C.; Eholié, S.P.; Dabis, F.; Jaquet, A.; et al. Oral health and HIV infection among female sex workers in Abidjan, Côte d’Ivoire. BMC Oral Health 2015, 15, 154. [Google Scholar] [CrossRef] [PubMed]
- Rao, B.V.; Suresh Babu, A.M.; Kamalsha, S.K.; Rao, M.S.; Karthik, K. Oral Health Status and Treatment Needs of Gunj Marketing Yard Laborers of Raichur City, Karnataka. J. Pharm.Bioallied. Sci. 2017, 9, 195–200. [Google Scholar] [CrossRef]
- Yoshino, K.; Suzuki, S.; Ishizuka, Y.; Takayanagi, A.; Sugihara, N.; Kamijyo, H. Relationship between job stress and subjective oral health symptoms in male financial workers in Japan. Ind. Health 2017, 55, 119–126. [Google Scholar] [CrossRef]
- Yoshino, K.; Suzuki, S.; Ishizuka, Y.; Takayanagi, A.; Sugihara, N.; Kamijyo, H. Relationship between amount of overtime work and untreated decayed teeth in male financial workers in Japan. J. Occup Health 2017, 59, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Ziebolz, D.; Werner, C.; Schmalz, G.; Nitschke, I.; Haak, R.; Mausberg, R.F.; Chenot, J.F. Oral Health and nutritional status in nursing home residents-results of an explorative cross-sectional pilot study. BMC Geriatr. 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Wright, F.; Chu, S.Y.; Milledge, K.L.; Valdez, E.; Law, G.; Hsu, B.; Naganathan, V.; Hirani, V.; Blyth, F.M.; Le Couteur, D.G.; et al. Oral health of community-dwelling older Australian men: The Concord Health and Ageing in Men Project (CHAMP). Aust. Dent. J. 2018, 63, 55–65. [Google Scholar] [CrossRef]
- Caracho, R.A.; Foratori-Junior, G.A.; Fusco, N.D.S.; Jesuino, B.G.; Missio, A.L.T.; Sales-Peres, S.H.C. Systemic conditions and oral health-related quality of life of pregnant women of normal weight and who are overweight. Int. Dent. J. 2020, 70, 287–295. [Google Scholar] [CrossRef]
- Erchick, D.J.; Rai, B.; Agrawal, N.K.; Khatry, S.K.; Katz, J.; LeClerq, S.C.; Reynolds, M.A.; Mullany, L.C. Oral hygiene, prevalence of gingivitis, and associated risk factors among pregnant women in Sarlahi District, Nepal. BMC Oral Health 2019, 19, 2. [Google Scholar] [CrossRef]
- Huang, Z.; DerGarabedian, B.P.; He, L.; Sha, Y.; Chen, Z.; Kang, J.; Cai, Y.; Gao, P. Impact of Periodonto-pathogenic Microbiota and Sociodemographic Variables on Periodontal Status during Pregnancy and Postpartum Period. Oral Health Prev. Dent. 2020, 18, 855–864. [Google Scholar]
- Gil, L.; Mínguez, I.; Caffesse, R.; Llambés, F. Periodontal Disease in Pregnancy: The Influence of General Factors and Inflammatory Mediators. Oral Health Prev. Dent. 2019, 17, 69–73. [Google Scholar] [PubMed]
- Fusco, N.D.S.; Foratori-Junior, G.A.; Missio, A.L.T.; Jesuino, B.G.; Sales-Peres, S.H.C. Systemic and oral conditions of pregnant women with excessive weight assisted in a private health system. Int. Dent. J. 2019, 69, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Foratori-Junior, G.A.; da Silva, B.M.; da Silva Pinto, A.C.; Honório, H.M.; Groppo, F.C.; de Carvalho Sales-Peres, S.H. Systemic and periodontal conditions of overweight/obese patients during pregnancy and after delivery: A prospective cohort. Clin. Oral Investig. 2020, 24, 157–165. [Google Scholar] [CrossRef]
- Bomfim, R.A.; Frias, A.C.; Pannuti, C.M.; Zilbovicius, C.; Pereira, A.C. Socio-economic factors associated with periodontal conditions among Brazilian elderly people—Multilevel analysis of the SBSP-15 study. PLoS ONE 2018, 13, e0206730. [Google Scholar]
- Castrejón-Pérez, R.C.; Jiménez-Corona, A.; Bernabé, E.; Villa-Romero, A.R.; Arrivé, E.; Dartigues, J.F.; Gutiérrez-Robledo, L.M.; Borges-Yáñez, S.A. Oral Disease and 3-Year Incidence of Frailty in Mexican Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.S.; Chen, K.J.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. The Oral Health Status of Chinese Elderly People with and without Dementia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 1913. [Google Scholar] [CrossRef]
- Ramsay, S.E.; Whincup, P.H.; Watt, R.G.; Tsakos, G.; Papacosta, A.O.; Lennon, L.T.; Wannamethee, S.G. Burden of poor oral health in older age: Findings from a population-based study of older British men. BMJ Open 2015, 5, e009476. [Google Scholar] [CrossRef]
- Rantzow, V.; Andersson, P.; Lindmark, U. Occurrence of oral health problems and planned measures in dependent older people in nursing care. J. Clin. Nurs. 2018, 27, 4381–4389. [Google Scholar] [CrossRef]
- Rekhi, A.; Marya, C.M.; Oberoi, S.S.; Nagpal, R.; Dhingra, C.; Kataria, S. Periodontal status and oral health-related quality of life in elderly residents of aged care homes in Delhi. Geriatr. Gerontol. Int. 2016, 16, 474–480. [Google Scholar] [CrossRef]
- Hakeem, F.F.; Sabbah, W. Is there socioeconomic inequality in periodontal disease among adults with optimal behaviours. Acta Odontol. Scand. 2019, 77, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Han, K.; Vu, D.; Cho, K.H.; Lee, S.H. Number of remaining teeth and its association with socioeconomic status in South Korean adults: Data from the Korean National Health and Nutrition Examination Survey 2012–2013. PLoS ONE 2018, 13, e0196594. [Google Scholar]
- Castrejón-Pérez, R.C.; Borges-Yáñez, S.A.; Irigoyen-Camacho, M.E.; Cruz-Hervert, L.P. Negative impact of oral health conditions on oral health related quality of life of community dwelling elders in Mexico city, a population based study. Geriatr. Gerontol. Int. 2017, 17, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Schwindling, F.S.; Krisam, J.; Hassel, A.J.; Rammelsberg, P.; Zenthöfer, A. Long-term success of oral health intervention among care-dependent institutionalized seniors: Findings from a controlled clinical trial. Community Dent. Oral Epidemiol. 2018, 46, 109–117. [Google Scholar] [CrossRef]
- Luo, H.; Hybels, C.F.; Wu, B. Acculturation, depression and oral health of immigrants in the USA. Int. Dent. J. 2018, 68, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.H.; Han, D.H. Exposure to occupational noise and periodontitis in Korean workers. J. Periodontol. 2018, 89, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Antoniazzi, R.P.; Zanatta, F.B.; Rösing, C.K.; Feldens, C.A. Association Among Periodontitis and the Use of Crack Cocaine and Other Illicit Drugs. J. Periodontol. 2016, 87, 1396–1405. [Google Scholar] [CrossRef]
- Lee, J.H.; Yi, S.K.; Kim, S.Y.; Kim, J.S.; Kim, H.N.; Jeong, S.H.; Kim, J.B. Factors Related to the Number of Existing Teeth among Korean Adults Aged 55-79 Years. Int. J. Environ. Res. Public Health 2019, 16, 3927. [Google Scholar] [CrossRef]
- Bhat, M.; Do, L.G.; Roberts-Thomson, K. Risk indicators for prevalence, extent and severity of periodontitis among rural Indian population aged 35–54 years. Int. J. Dent. Hyg. 2018, 16, 492–502. [Google Scholar] [CrossRef]
- Celeste, R.K.; Oliveira, S.C.; Junges, R. Threshold-effect of income on periodontitis and interactions with race/ethnicity and education. Rev. Bras. Epidemiol. 2019, 22, e190001. [Google Scholar] [CrossRef]
- Aida, J.; Kondo, K.; Yamamoto, T.; Saito, M.; Ito, K.; Suzuki, K.; Osaka, K.; Kawachi, I. Is Social Network Diversity Associated with Tooth Loss among Older Japanese Adults? PLoS ONE 2016, 11, e0159970. [Google Scholar] [CrossRef]
- Andrade, F.B.; Teixeira, D.S.D.C.; Frazão, P.; Duarte, Y.A.O.; Lebrão, M.L.; Antunes, J.L.F. Oral health profile among community-dwelling elderly and its association with self-rated oral health. Rev. Bras. Epidemiol. 2019, 21 (Suppl. 2), e180012. [Google Scholar]
- Bachkati, K.H.; Mortensen, E.L.; Brønnum-Hansen, H.; Holm-Pedersen, P. Midlife Cognitive Ability, Education, and Tooth Loss in Older Danes. J. Am. Geriatr. Soc. 2017, 65, 194–199. [Google Scholar] [CrossRef]
- Bakker, M.H.; Vissink, A.; Spoorenberg, S.L.W.; Jager-Wittenaar, H.; Wynia, K.; Visser, A. Are Edentulousness, Oral Health Problems and Poor Health-Related Quality of Life Associated with Malnutrition in Community-Dwelling Elderly (Aged 75 Years and Over)? A Cross-Sectional Study. Nutrients 2018, 10, 1965. [Google Scholar] [CrossRef] [PubMed]
- Bakker, M.H.; Vissink, A.; Spoorenberg, S.L.W.; Wynia, K.; Visser, A. Self-reported oral health problems and the ability to organize dental care of community-dwelling elderly aged ≥75 years. BMC Oral Health 2020, 20, 185. [Google Scholar] [CrossRef]
- Beker, N.; van der Maarel-Wierink, C.D.; de Baat, C.; Holstege, H. Self-reported oral health in the Dutch 100-plus Study of cognitively healthy centenarians: An observational cohort study. BMC Geriatr. 2019, 19, 355. [Google Scholar] [CrossRef] [PubMed]
- Chiesi, F.; Grazzini, M.; Innocenti, M.; Giammarco, B.; Simoncini, E.; Garamella, G.; Zanobini, P.; Perra, C.; Baggiani, L.; Lorini, C.; et al. Older People Living in Nursing Homes: An Oral Health Screening Survey in Florence, Italy. Int. J. Environ. Res. Public Health 2019, 16, 3492. [Google Scholar] [CrossRef]
- Chiu, C.T.; Malhotra, R.; Tan, S.M.; Lim, J.; Chan, A.; Teoh, K.H.; Gan, S.T.; Saito, Y. Dental health status of community-dwelling older Singaporeans: Findings from a nationally representative survey. Gerodontology 2017, 34, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Cocco, F.; Campus, G.; Strohmenger, L.; Ardizzone, V.C.; Cagetti, M.G. The burden of tooth loss in Italian elderly population living in nursing homes. BMC Geriatr. 2018, 18, 76. [Google Scholar] [CrossRef]
- da Veiga Pessoa, D.M.; Roncalli, A.G.; de Lima, K.C. Economic and sociodemographic inequalities in complete denture need among older Brazilian adults: A cross-sectional population-based study. BMC Oral Health 2016, 17, 5. [Google Scholar] [CrossRef]
- Delwel, S.; Scherder, E.J.A.; Perez, R.S.G.M.; Hertogh, C.M.P.M.; Maier, A.B.; Lobbezoo, F. Oral function of older people with mild cognitive impairment or dementia. J. Oral Rehabil. 2018, 45, 990–997. [Google Scholar] [CrossRef] [PubMed]
- El Osta, N.; El Osta, L.; Khabbaz, L.R.; Saad, R.; Abi-Ghosn, C.; Hennequin, M.; Tubert-Jeannin, S.; Fakhouri, J. Social inequalities in oral health in a group of older people in a Middle Eastern country: A cross-sectional survey. Aging Clin. Exp. Res. 2018, 30, 1513–1521. [Google Scholar] [CrossRef]
- Furuta, M.; Takeuchi, K.; Adachi, M.; Kinoshita, T.; Eshima, N.; Akifusa, S.; Kikutani, T.; Yamashita, Y. Tooth loss, swallowing dysfunction and mortality in Japanese older adults receiving home care services. Geriatr. Gerontol. Int. 2018, 18, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.O.; Griffin, P.M.; Li, C.H.; Bailey, W.D.; Brunson, D.; Jones, J.A. Changes in Older Adults’ Oral Health and Disparities: 1999 to 2004 and 2011 to 2016. J. Am. Geriatr. Soc. 2019, 67, 1152–1157. [Google Scholar] [CrossRef]
- Han, D.H.; Khang, Y.H.; Choi, H.J. Association of parental education with tooth loss among Korean Elders. Community Dent. Oral Epidemiol. 2015, 43, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Heredia-Ponce, E.; Irigoyen-Camacho, A.E.; Sánchez-García, S. Oral Health Status of Institutionalized Older Women from Different Socioeconomic Positions. J. Health Care Poor Underserved 2017, 28, 1462–1476. [Google Scholar] [CrossRef]
- Hoeksema, A.R.; Peters, L.L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A.; Visser, A. Oral health status and need for oral care of care-dependent indwelling elderly: From admission to death. Clin. Oral Investig. 2017, 21, 2189–2196. [Google Scholar] [CrossRef]
- Kim, H.N.; Jang, Y.E.; Kim, C.B.; Kim, N.H. Socioeconomic status and self-reported periodontal symptoms in community-dwelling individuals: Data from the Korea Community Health Surveys of 2011 and 2013. Int. Dent. J. 2018, 68, 411–419. [Google Scholar] [CrossRef]
- Koistinen, S.; Olai, L.; Ståhlnacke, K.; Fält, A.; Ehrenberg, A. Oral health-related quality of life and associated factors among older people in short-term care. Int. J. Dent. Hyg. 2020, 18, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Laguzzi, P.N.; Schuch, H.S.; Medina, L.D.; de Amores, A.R.; Demarco, F.F.; Lorenzo, S. Tooth loss and associated factors in elders: Results from a national survey in Uruguay. J. Public Health Dent. 2016, 76, 143–151. [Google Scholar] [CrossRef]
- Maille, G.; Saliba-Serre, B.; Ferrandez, A.M.; Ruquet, M. Objective and perceived oral health status of elderly nursing home residents: A local survey in southern France. Clin. Interv. Aging. 2019, 14, 1141–1151. [Google Scholar] [CrossRef] [PubMed]
- Maille, G.; Saliba-Serre, B.; Ferrandez, A.M.; Ruquet, M. Use of care and the oral health status of people aged 60 years and older in France: Results from the National Health and Disability Survey. Clin. Interv. Aging. 2017, 12, 1159–1166. [Google Scholar] [CrossRef]
- Matsuyama, Y.; Jürges, H.; Listl, S. The Causal Effect of Education on Tooth Loss: Evidence from United Kingdom Schooling Reforms. Am. J. Epidemiol. 2019, 188, 87–95. [Google Scholar] [CrossRef]
- Mehr, K.; Olszanecka-Glinianowicz, M.; Chudek, J.; Szybalska, A.; Mossakowska, M.; Zejda, J.; Wieczorowska-Tobis, K.; Grodzicki, T.; Piotrowski, P. Dental status in the Polish senior population and its correlates-Results of the national survey PolSenior. Gerodontology 2018, 35, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Nakahori, N.; Sekine, M.; Yamada, M.; Tatsuse, T.; Kido, H.; Suzuki, M. Socioeconomic status and remaining teeth in Japan: Results from the Toyama dementia survey. BMC Public Health 2019, 19, 691. [Google Scholar] [CrossRef]
- Nihtilä, A.; Tuuliainen, E.; Komulainen, K.; Autonen-Honkonen, K.; Nykänen, I.; Hartikainen, S.; Ahonen, R.; Tiihonen, M.; Suominen, A.L. Preventive oral health intervention among old home care clients. Age Ageing 2017, 46, 846–851. [Google Scholar] [CrossRef]
- Saito, M.; Shimazaki, Y.; Nonoyama, T.; Tadokoro, Y. Associations of number of teeth with medical costs and hospitalization duration in an older Japanese population. Geriatr. Gerontol. Int. 2019, 19, 335–341. [Google Scholar] [CrossRef]
- Silva, A.E.R.; Echeverria, M.S.; Custódio, N.B.; Cascaes, A.M.; Camargo, M.B.J.; Langlois, C.O. Regular use of dental services and dental loss among the elderly. Cien. Saude. Colet. 2018, 23, 4269–4276. [Google Scholar] [CrossRef]
- Tiwari, T.; Scarbro, S.; Bryant, L.L.; Puma, J. Factors Associated with Tooth Loss in Older Adults in Rural Colorado. J. Community Health 2016, 41, 476–481. [Google Scholar] [CrossRef]
- Yoon, M.N.; Ickert, C.; Slaughter, S.E.; Lengyel, C.; Carrier, N.; Keller, H. Oral health status of long-term care residents in Canada: Results of a national cross-sectional study. Gerodontology 2018, 35, 359–364. [Google Scholar] [CrossRef]
- Zhang, Q.; Jing, Q.; Gerritsen, A.E.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Dental status of an institutionalized elderly population of 60 years and over in Qingdao, China. Clin. Oral Investig. 2016, 20, 1021–1028. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zimmerman, S.; Austin, S.; Cohen, L.; Reed, D.; Poole, P.; Ward, K.; Sloane, P.D. Readily Identifiable Risk Factors of Nursing Home Residents’ Oral Hygiene: Dementia, Hospice, and Length of Stay. J. Am. Geriatr. Soc. 2017, 65, 2516–2521. [Google Scholar] [CrossRef] [PubMed]
- Rouxel, P.; Tsakos, G.; Demakakos, P.; Zaninotto, P.; Chandola, T.; Watt, R.G. Is Social Capital a Determinant of Oral Health among Older Adults? Findings from the English Longitudinal Study of Ageing. PLoS ONE 2015, 10, e0125557. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, J.A.; Orleans, B.; Fontana, M.; Phillips, C.; Jones, J.A. Factors Associated With Becoming Edentulous in the US Health and Retirement Study. J. Am. Geriatr. Soc. 2019, 67, 2318–2324. [Google Scholar] [CrossRef]
- Caldwell, J.T.; Lee, H.; Cagney, K.A. The Role of Primary Care for the Oral Health of Rural and Urban Older Adults. J. Rural Health 2017, 33, 409–418. [Google Scholar] [CrossRef]
- Dahl, K.E.; Calogiuri, G.; Jönsson, B. Perceived oral health and its association with symptoms of psychological distress, oral status and socio-demographic characteristics among elderly in Norway. BMC Oral Health 2018, 18, 93. [Google Scholar] [CrossRef] [PubMed]
- Koistinen, S.; Olai, L.; Ståhlnacke, K.; Fält, A.; Ehrenberg, A. Oral health and oral care in short-term care: Prevalence, related factors and coherence between older peoples’ and professionals’ assessments. Scand. J. Caring Sci. 2019, 33, 712–722. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Kim, H.G.; Hur, J.Y.; Yang, K. Oral Health in Low-Income Older Adults in Korea. J. Community Health Nurs. 2016, 33, 98–106. [Google Scholar] [CrossRef]
- Mochida, Y.; Yamamoto, T.; Fuchida, S.; Aida, J.; Kondo, K. Does poor oral health status increase the risk of falls? The JAGES Project Longitudinal Study. PLoS ONE 2018, 13, e0192251. [Google Scholar]
- Nilsson, H.; Berglund, J.S.; Renvert, S. Periodontitis, tooth loss and cognitive functions among older adults. Clin. Oral Investig. 2018, 22, 2103–2109. [Google Scholar] [CrossRef]
- Okamoto, N.; Amano, N.; Nakamura, T.; Yanagi, M. Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: A cross-sectional study. BMC Oral Health 2019, 19, 110. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.G.; Cascaes, A.M.; Silva, A.E.; Seerig, L.M.; Nascimento, G.G.; Demarco, F.F. Edentulism, Severe Tooth Loss and Lack of Functional Dentition in Elders: A Study in Southern Brazil. Braz. Dent. J. 2016, 27, 345–352. [Google Scholar] [CrossRef]
- Ishikawa, S.; Konta, T.; Susa, S.; Kitabatake, K.; Ishizawa, K.; Togashi, H.; Tsuya, A.; Ueno, Y.; Kubota, I.; Yamashita, H.; et al. Risk factors for tooth loss in community-dwelling Japanese aged 40 years and older: The Yamagata (Takahata) study. Clin. Oral Investig. 2019, 23, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Gomes Filho, V.V.; Gondinho, B.V.C.; Silva-Junior, M.F.; Cavalcante, D.F.B.; Bulgareli, J.V.; Sousa, M.D.L.R.; Frias, A.C.; Batista, M.J.; Pereira, A.C. Tooth loss in adults: Factors associated with the position and number of lost teeth. Rev. Saude Publica 2019, 53, 105. [Google Scholar]
- Rodriguez, F.R.; Paganoni, N.; Weiger, R.; Walter, C. Lower Educational Level is a Risk Factor for Tooth Loss—Analysis of aSwiss Population (KREBS Project). Oral Health Prev. Dent. 2017, 15, 139–145. [Google Scholar] [PubMed]
- Novrinda, H.; Han, D.H.; Jung-Choi, K.; Ryu, J.I. Neo-Marxian social class inequalities in oral health among the South Korean population. Community Dent. Oral Epidemiol. 2019, 47, 162–170. [Google Scholar] [CrossRef]
- Wennström, A.; Boman, U.W.; Ahlqwist, M.; Björkelund, C.; Hakeberg, M. Perceived mental stress in relation to oral health over time in middle-aged Swedish women. Community Dent Health 2015, 32, 241–246. [Google Scholar]
- Song, I.S.; Han, K.; Choi, Y.J.; Ryu, J.J.; Park, J.B. Influence of oral health behavior and sociodemographic factors on remaining teeth in Korean adults: 2010–2012 Korea national health and nutrition examination survey. Medicine 2016, 95, e5492. [Google Scholar] [CrossRef]
- Steele, J.; Shen, J.; Tsakos, G.; Fuller, E.; Morris, S.; Watt, R.; Guarnizo-Herreño, C.; Wildman, J. The Interplay between socioeconomic inequalities and clinical oral health. J. Dent. Res. 2015, 94, 19–26. [Google Scholar] [CrossRef]
- Roberto, L.L.; Silveira, M.F.; de Paula, A.M.B.; Ferreira, E.; Ferreira, E.; Martins, A.M.E.B.L.; Haikal, D.S. Contextual and individual determinants of tooth loss in adults: A multilevel study. BMC Oral Health 2020, 20, 73. [Google Scholar] [CrossRef]
- Duijster, D.; Oude Groeniger, J.; van der Heijden, G.J.M.G.; van Lenthe, F.J. Material, behavioural, cultural and psychosocial factors in the explanation of socioeconomic inequalities in oral health. Eur. J. Public Health 2018, 28, 590–597. [Google Scholar] [CrossRef]
- Hach, M.; Christensen, L.B.; Lange, T.; Hvidtfeldt, U.A.; Danielsen, B.; Diderichsen, F.; Osler, M.; Prescott, E.; Andersen, I. Social inequality in tooth loss, the mediating role of smoking and alcohol consumption. Community Dent. Oral Epidemiol. 2019, 47, 416–423. [Google Scholar] [CrossRef]
- Goulart Mde, A.; Vettore, M.V. Is the relative increase in income inequality related to tooth loss in middle-aged adults? J. Public Health Dent. 2016, 76, 65–75. [Google Scholar] [CrossRef]
- Chalub, L.L.; Martins, C.C.; Ferreira, R.C.; Vargas, A.M. Functional Dentition in Brazilian Adults: An Investigation of Social Determinants of Health (SDH) Using a Multilevel Approach. PLoS ONE 2016, 11, e0148859. [Google Scholar] [CrossRef] [PubMed]
- Naorungroj, S.; Slade, G.D.; Divaris, K.; Heiss, G.; Offenbacher, S.; Beck, J.D. Racial differences in periodontal disease and 10-year self-reported tooth loss among late middle-aged and older adults: The dental ARIC study. J. Public Health Dent. 2017, 77, 372–382. [Google Scholar] [CrossRef]
- Kim, H.N.; Ha, T.G.; Kim, M.J.; Jun, E.J.; Jeong, S.H.; Kim, J.B. Factors related to number of present teeth in Korean elderly adults aged 55-84 years. Int. J. Dent. Hyg. 2016, 14, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Fantin, R.; Delpierre, C.; Kelly-Irving, M.; Barboza Solís, C. Early socioeconomic conditions and severe tooth loss in middle-aged Costa Ricans. Community Dent. Oral Epidemiol. 2018, 46, 178–184. [Google Scholar] [CrossRef]
- Suzuki, S.; Yoshino, K.; Takayanagi, A.; Ishizuka, Y.; Satou, R.; Kamijo, H.; Sugihara, N. Comparison of risk factors for tooth loss between professional drivers and white-collar workers: An internet survey. Ind. Health 2016, 54, 246–253. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sato, Y.; Tsuboya, T.; Watt, R.G.; Aida, J.; Osaka, K. Temporary employment and tooth loss: A cross-sectional study from the J-SHINE study. BMC Oral Health 2018, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.M.; Azevedo, J.A.P.; Martins, R.F.M.; Alves, C.M.C.; Ribeiro, C.C.C.; Thomaz, E.B.A.F. Anemia and Dental Caries in Pregnant Women: A Prospective Cohort Study. Biol Trace Elem Res. 2017, 177, 241–250. [Google Scholar] [CrossRef]
- Umer, A.; Haile, Z.T.; Ahmadi-Montecalvo, H.; Chertok, I.R. Factors Associated with Receipt of Pre-pregnancy Preventive Dental Care Among Women in West Virginia: Pregnancy Risk Assessment Monitoring System (PRAMS) Survey 2009–2010. Oral Health Prev. Dent. 2016, 14, 413–422. [Google Scholar] [PubMed]
- Rio, R.; Sampaio-Maia, B.; Pereira, M.L.; Silva, M.J.; Azevedo, Á. Pregnancy as a Period of Enhanced Risk for Non-Cavitated Caries Lesions. Oral Health Prev. Dent. 2020, 18, 387–393. [Google Scholar]
- Martínez-Beneyto, Y.; Montero-Martin, J.; Garcia-Navas, F.; Vicente-Hernandez, A.; Ortiz-Ruiz, A.J.; Camacho-Alonso, F. Influence of a preventive program on the oral health-related quality of life (OHRQoL) of European pregnant women: A cohort study. Odontology 2019, 107, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Kateeb, E.; Momany, E. Dental caries experience and associated risk indicators among Palestinian pregnant women in the Jerusalem area: A cross-sectional study. BMC Oral Health 2018, 18, 170. [Google Scholar] [CrossRef]
- Calvasina, P.; Lawrence, H.P.; Hoffman-Goetz, L.; Norman, C.D. Brazilian immigrants’ oral health literacy and participation in oral health care in Canada. BMC Oral Health 2016, 16, 18. [Google Scholar] [CrossRef]
- Xhihani, B.; Rainchuso, L.; Smallidge, D.; Dominick, C. Oral Health Beliefs, Attitudes, and Practices of Albanian Immigrants in the United States. J. Community Health 2017, 42, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Rota, K.; Spanbauer, C.; Szabo, A.; Okunseri, C.E. Oral Health Practices, Beliefs and Dental Service Utilization of Albanian Immigrants in Milwaukee, Wisconsin: A Pilot Study. J.Immigr. Minor. Health 2019, 21, 315–323. [Google Scholar] [CrossRef]
- Elkerdany, A.; Gurenlian, J.; Freudenthal, J. Measuring Oral Health Literacy of Refugees: Associations with Dental Care Utilization and Oral Health Self-Efficacy. J. Dent. Hyg. 2020, 94, 9–17. [Google Scholar]
- Chahar, P.; Mohanty, V.R.; Aswini, Y.B. Oral health-related quality of life among elderly patients visiting special clinics in public hospitals in Delhi, India: A cross-sectional study. Indian J. Public Health 2019, 63, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Chae, S.; Lee, Y.; Kim, J.; Chun, K.H.; Lee, J.K. Factors associated with perceived unmet dental care needs of older adults. Geriatr. Gerontol. Int. 2017, 17, 1936–1942. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.S.; Yi, Y.J.; Donnelly, L.R. Oral health of older residents in care and community dwellers: Nursing implications. Int. Nurs. Rev. 2017, 64, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Blasi, P.R.; Krakauer, C.; Anderson, M.L.; Nelson, J.; Bush, T.; Catz, S.L.; McClure, J.B. Factors associated with future dental care utilization among low-income smokers overdue for dental visits. BMC Oral Health 2018, 18, 183. [Google Scholar] [CrossRef]
- Berglund, E.; Westerling, R.; Lytsy, P. Social and health-related factors associated with refraining from seeking dental care: A cross-sectional population study. Community Dent. Oral Epidemiol. 2017, 45, 258–265. [Google Scholar] [CrossRef]
- Piotrowska, D.E.; Jankowska, D.; Huzarska, D.; Szpak, A.S.; Pędziński, B. Socioeconomic inequalities in use and non-use of dental services in Poland. Int. J. Public Health 2020, 65, 637–647. [Google Scholar] [CrossRef]
- Akintobi, T.H.; Hoffman, L.M.; McAllister, C.; Goodin, L.; Hernandez, N.D.; Rollins, L.; Miller, A. Assessing the Oral Health Needs of African American Men in Low-Income, Urban Communities. Am. J. Mens. Health 2018, 12, 326–337. [Google Scholar] [CrossRef]
- Kailembo, A.; Preet, R.; Stewart Williams, J. Socioeconomic inequality in self-reported unmet need for oral health services in adults aged 50 years and over in China, Ghana, and India. Int. J. Equity Health 2018, 17, 99. [Google Scholar] [CrossRef]
- Srivastava, P.; Chen, G.; Harris, A. Oral Health, Dental Insurance and Dental Service use in Australia. Health Econ. 2017, 26, 35–53. [Google Scholar] [CrossRef]
- Teusner, D.N.; Brennan, D.S.; Spencer, A.J. Associations between level of private dental insurance cover and favourable dental visiting by household income. Aust. Dent. J. 2015, 60, 479–489. [Google Scholar] [CrossRef]
- Rampa, S.; Wilson, F.A.; Allareddy, V. Trends in dental-related emergency department visits in the State of California from 2005 to 2011. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.; Manso, A.C.; Escoval, A.; Salvado, F.; Nunes, C. Self-perception of oral health in older adults from an urban population in Lisbon, Portugal. Rev. Saude Publica 2016, 50, 53. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, Y.W.; de Almeida, L.F.D.; de Lucena, E.H.G.; Probst, L.F.; Cavalcante, D.F.B.; Frias, A.C.; Bulgareli, J.V.; Pereira, A.C. Factors that influence the oral impact on daily performance of older people in Brazil: A cross-sectional population-based study. Gerodontology 2020, 37, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.J.F.; Lins, C.A.A.; Macedo, L.P.V.; Sousa, V.P.S.; Duque, J.A.; Souza, M.C. Clinical and self-perceived oral health assessment of elderly residents in urban, rural, and institutionalized communities. Clinics 2019, 74, e972. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Abrahamsson, I.; Wide, U.; Hakeberg, M. Periodontal disease among older people and its impact on oral health-related quality of life. Gerodontology 2018, 35, 382–390. [Google Scholar] [CrossRef]
- Zusman, S.P.; Kushnir, D.; Natapov, L.; Goldsmith, R.; Dichtiar, R. Oral Health-Related Quality of Life in the Elderly in Israel--Results from the National Health and Nutrition Survey of the Elderly 2005–2006. Oral Health Prev. Dent. 2016, 14, 117–123. [Google Scholar] [PubMed]
- Abu-Awwad, M.; Al-Omoush, S.; Shqaidef, A.; Hilal, N.; Hassona, Y. Oral health-related quality of life among Syrian refugees in Jordan: A cross-sectional study. Int. Dent. J. 2020, 70, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Freiberg, A.; Wienke, A.; Bauer, L.; Niedermaier, A.; Führer, A. Dental Care for Asylum-Seekers in Germany: A Retrospective Hospital-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 2672. [Google Scholar] [CrossRef]
- Grover, V.; Malhotra, R.; Dhawan, S.; Kaur, G. Comparative Assessment of Oral Health Related Quality of Life in Chronic Periodontitis Patients of Rural and Urban Populations in Punjab. Oral Health Prev. Dent. 2016, 14, 235–240. [Google Scholar]
- Zhang, J.; Sardana, D.; Wong, M.C.M.; Leung, K.C.M.; Lo, E.C.M. Factors Associated with Dental Root Caries: A Systematic Review. JDR Clin. Trans. Res. 2020, 5, 13–29. [Google Scholar] [CrossRef]
- Lee, D.R.; Santo, E.C.; Lo, J.C.; Ritterman Weintraub, M.L.; Patton, M.; Gordon, N.P. Understanding functional and social risk characteristics of frail older adults: A cross-sectional survey study. BMC Fam. Pract. 2018, 19, 170. [Google Scholar] [CrossRef]
- Niesten, D.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Oral health care behavior and frailty-related factors in a care-dependent older population. J. Dent. 2017, 61, 39–47. [Google Scholar] [CrossRef]
- Chen, M.Y. Misperception of Oral Health among Adults in Rural Areas: A Fundamental but Neglected Issue in Primary Healthcare. Int. J. Environ. Res. Public Health 2018, 15, 2187. [Google Scholar] [CrossRef] [PubMed]
- Mejia, G.C.; Elani, H.W.; Harper, S.; Murray Thomson, W.; Ju, X.; Kawachi, I.; Kaufman, J.S.; Jamieson, L.M. Socioeconomic status, oral health and dental disease in Australia, Canada, New Zealand and the United States. BMC Oral Health 2018, 18, 176. [Google Scholar] [CrossRef] [PubMed]
- Capurro, D.A.; Davidsen, M. Socioeconomic inequalities in dental health among middle-aged adults and the role of behavioral and psychosocial factors: Evidence from the Spanish National Health Survey. Int. J. Equity Health 2017, 16, 34. [Google Scholar] [CrossRef] [PubMed]
- Hicks, T.A.; Wilson, S.M.; Thomas, S.P.; Dennis, P.A.; Neal, J.M.; Calhoun, P.S. Low Income as a Multiplicative Risk Factor for Oral Pain and Dental Problems Among, U.S. Veteran Smokers. Int. J. Behav. Med. 2018, 25, 67–73. [Google Scholar] [CrossRef]
- Bassim, C.W.; MacEntee, M.I.; Nazmul, S.; Bedard, C.; Liu, S.; Ma, J.; Griffith, L.E.; Raina, P. Self-reported oral health at baseline of the Canadian Longitudinal Study on Aging. Community Dent. Oral Epidemiol. 2020, 48, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Laniado, N.; Brow, A.R.; Tranby, E.; Badner, V.M. Trends in non-traumatic dental emergency department use in New York and New Jersey: A look at Medicaid expansion from both sides of the Hudson River. J. Public Health Dent. 2020, 80, 9–13. [Google Scholar] [CrossRef] [PubMed]
- DeLia, D.; Lloyd, K.; Feldman, C.A.; Cantor, J.C. Patterns of emergency department use for dental and oral health care: Implications for dental and medical care coordination. J. Public Health Dent. 2016, 76, 1–8. [Google Scholar] [CrossRef]
- Franciscatto, G.J.; Brennan, D.S.; Gomes, M.S.; Rossi-Fedele, G. Association between pulp and periapical conditions and dental emergency visits involving pain relief: Epidemiological profile and risk indicators in private practice in Australia. Int. Endod. J. 2020, 53, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Srisilapanan, P.; Korwanich, N.; Lalloo, R. Associations between social inequality and tooth loss in a household sample of elderly Thai people aged ≥60 years old. Gerodontology 2016, 33, 201–208. [Google Scholar] [CrossRef]
- Ramsay, S.E.; Papachristou, E.; Watt, R.G.; Lennon, L.T.; Papacosta, A.O.; Whincup, P.H.; Wannamethee, S.G. Socioeconomic disadvantage across the life-course and oral health in older age: Findings from a longitudinal study of older British men. J. Public Health 2018, 40, e423–e430. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Bernabé, E.; Liu, X.; Gallagher, J.E.; Zheng, S. Do contextual factors have a role in periodontal disease? J. Clin. Periodontol. 2017, 44, 13–21. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Oral Disorders Collaborators; Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar]
- Cianetti, S.; Pagano, S.; Nardone, M.; Lombardo, G. Model for Taking Care of Patients with Early Childhood Caries during the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 3751. [Google Scholar] [CrossRef]
- Ostberg, A.L.; Andersson, P.; Hakeberg, M. Oral impacts on daily performances: Associations with self-reported general health and medication. Acta Odontol. Scand. 2009, 67, 370–376. [Google Scholar] [CrossRef]
- D’Addazio, G.; Santilli, M.; Sinjari, B.; Xhajanka, E.; Rexhepi, I.; Mangifesta, R.; Caputi, S. Access to Dental Care-A Survey from Dentists, People with Disabilities and Caregivers. Int. J. Environ. Res. Public Health 2021, 18, 1556. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S. From focal sepsis to periodontal medicine: A century of exploring the role of the oral microbiome in systemic disease. J. Physiol. 2017, 595, 465–476. [Google Scholar] [CrossRef]
- Leira, Y.; Seoane, J.; Blanco, M.; Rodríguez-Yáñez, M.; Takkouche, B.; Blanco, J.; Castillo, J. Association between periodontitis and ischemic stroke: A systematic review and meta-analysis. Eur. J. Epidemiol. 2017, 32, 43–53. [Google Scholar] [CrossRef]
- Puertas, A.; Magan-Fernandez, A.; Blanc, V.; Revelles, L.; O’Valle, F.; Pozo, E.; León, R.; Mesa, F. Association of periodontitis with preterm birth and low birth weight: A comprehensive review. J. Matern. Fetal Neonatal. Med. 2018, 31, 597–602. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Spanemberg, J.C.; Cardoso, J.A.; Slob, E.M.G.B.; López-López, J. Quality of life related to oral health and its impact in adults. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).