Abstract
Context: Fever is a common symptom in children that nurses and pediatricians treat. Although it is a common sign in clinical practice, fever instills irrational fears in parents that health professionals share. Objective: To investigate whether doctors’ and nurses’ knowledge, perceptions, and attitudes toward fever influence how this sign is managed. Furthermore, it intends to evaluate whether educational programs increase knowledge and change attitudes and/or perceptions of nurses about children’s fever. Data Sources: A systematic review with meta-analysis was conducted with PRISMA international standards and the Cochrane recommendations. Study selection: Articles examining health professionals’ (doctors and/or nurses) knowledge, perceptions, and/or attitudes toward fever in children and the use of antipyretics were selected for the study. Data extraction: The qualitative analysis was carried out by classifying the articles according to the applied educational programs for nurses related to fever care for children that evaluated different outcomes to determine their efficacies. Results: For the qualitative synthesis, 41 articles were included, and 5 of these were taken in meta-analysis, which measured the effectiveness of educational programs for fever management in nurses. Limitations: All of the included studies generally had a high risk of bias. Conclusion: According to the evidence reviewed, nurses’ and physicians’ perceptions and attitudes regarding fever management in children indicate an overtreatment of this sign. We can give a recommendation grade of D on the use of educational programs to modify attitudes, perceptions, and knowledge about fever in children and improve clinical practice in nurses.
1. Introduction
Fever in children is associated with acute childhood illnesses and is a sign that nurses and pediatricians routinely treat [1,2,3,4,5,6,7,8]. According to the authors, although it is a common sign in clinical practice, health professionals share the most common observations with parents, such as brain damage, seizures, and death [1,2,3,4,5,6,7,8].
Fever reduction has shown no effect on morbidity or mortality in children with acute febrile illness. In addition, fever does not lead to tissue injury because it is regulated and self-limited by the hypothalamus [1,2,8,9,10,11,12,13,14,15].
Fever serves several beneficial physiological functions in the host’s defense against infection, including alerting the pathological situation and delaying the growth and reproduction of bacteria and viruses [1,2,3,4,5,7,8,9,10,11,13,14,15,16]. As a result, if fever is not harmful in and of itself, treatment should focus on comfort, with rational use of antipyretic therapies. Moreover, febrile seizures have not been associated with brain damage, and antipyretic treatment has not been reported for their prevention [1,2,3,4,5,7,8,9,10,11,13,14,15,16].
Navarro and de Carlos demonstrated that professionals’ incorrect attitudes toward the febrile child are cultural errors passed down from generation to generation, mainly from fear of febrile seizures and neurological sequelae [17]. The irrationality of these fears is evident when the evidence shows that febrile convulsions do not cause neurological damage and antipyretics do not prevent them, although they are sometimes used for that purpose [3,9,10,13,15,18].
Separating the sign from the underlying condition and understanding the febrile process, according to the authors, allows them to provide the essential care to the child, alerting for signs of serious illness, avoiding dehydration, and ensuring nutrient intake [6,7,11].
In this regard, Razón stated that there is little information about fever in which doctors and nurses are trained and that it causes anxiety in managing the febrile child [1]. In another study, Demir and Sekreter found that 65% of physicians consider this sign harmful, and 85% of pediatricians believe that fever can develop brain damage [19].
A temperature limit for antipyretics administration is a fundamental aspect in reaching a consensus on their usage. According to a study conducted with Australian nurses, using drugs on other aspects such as the child’s discomfort can lead to conflicts with parents and/or peers [20]. Parental influence on antipyretic measures, nursing colleagues, medical professionals, and workload, among other factors, was expressed by Australian nurses [20].
Educational programs have been considered a resource for changing the activities that professionals perform daily in clinical practice. Studies assessing educational programs that were included in this study were aimed to modify the ingrained knowledge, attitudes, and perceptions in nurses and evaluate their efficacy on increased knowledge [21,22], changing attitudes [23], knowledge and attitudes [24], perceptions and attitudes [25] or knowledge, attitudes, and perceptions [26].
The purpose of this systematic review and meta-analysis is to determine how doctors’ and nurses’ knowledge, perceptions, and attitudes toward fever management in children influence their practice. Furthermore, it intends to investigate whether educational programs increase knowledge and change nurses’ attitudes and/or perceptions about children’s fever.
2. Materials and Methods
2.1. Design
A systematic review with meta-analysis was carried out on doctors’ and nurses’ knowledge, attitudes, and perceptions about fever in children under the age of 14. PRISMA international standards and Cochrane recommendations were followed, and it was registered in PROSPERO on 31 August 2020 (No: CRD42020201362).
2.2. Search Strategy
From 15 November 2020 to 15 January 2021, the following databases were used for the bibliographic search: Virtual Health Library, Pubmed, Web of Science, and Cochrane. In addition, EBSCOhost meta-search was conducted with the following selected databases: Psychology and Behavioral Sciences Collection, APA PsycInfo, CINAHL with Full Text, Educational Administration Abstracts, MLA Directory of Periodicals, MLA International Bibliography, APA PsycArticles, E-Journals, eBook Collection (EBSCOhost), Social Work Abstracts, and SocINDEX with Full Text.
The search strategy was developed by truncating the DeCS/MeSH descriptors and a free term with Boolean operators. To avoid losing results, the search formula was: (pediatricians OR nurses, pediatric) and (fever OR Fever Phobia) in addition to a subsequent search with the only free term “fever phobia”.
Subsequently, a directed or snowball search was conducted, which included reviewing the references in the articles as well as those relevant to the study phenomenon that had not appeared due to the included limits. The article selection process was performed in two phases. The titles and abstracts were reviewed first, followed by a full-text reading to determine if they met the inclusion criteria and were of sufficient quality.
2.3. Inclusion Criteria
- (a)
- Articles examining health professionals’ (doctors and/or nurses) knowledge, perceptions, and/or attitudes toward fever in children under the age of 14 in hospital and community settings, as well as the use of antipyretics.
- (b)
- Written in English or Spanish.
2.4. Exclusion Criteria
- (a)
- Articles that only evaluate fever from a biological perspective.
- (b)
- Research articles on the pharmacological properties of antipyretics.
- (c)
- Articles about fever after vaccination.
- (d)
- Articles assessing the effectiveness of temperature measurement methods.
- (e)
- Articles focusing on parents’ knowledge, perceptions, and/or attitudes toward fever in children.
- (f)
- Articles on the assessment of discomfort in children.
- (g)
- Letters to the editor, comments from experts, and translations of original articles.
2.5. Data Collection
The articles were selected in pairs, and any disagreements were resolved by consulting a third researcher. Identification, screening, selection, and inclusion were the four stages of the paper’s selection procedure. All the articles’ titles were scrutinized using the inclusion criteria to eliminate those that were irrelevant. Papers with dubious titles were included in the following phase for in-depth analysis. A summary of each chosen study was reviewed in the third phase of selection to determine doctors’ and nurses’ knowledge, perceptions, and attitudes about fever in children.
An Excel coding sheet was then created for each article: literature reviews, surveys, common practice descriptions, and educational programs. Finally, the meta-analysis included the selected articles containing the evaluation of an educational program for nurses.
The studies’ quality was investigated using the “Critical Appraisal Skills Program (CASPe)” via the online critical reading card tool “FLC 3.0”. According to the criteria applied by this tool, the studies were classified as low, medium, or high quality.
2.6. Assessment of the Bias Risk
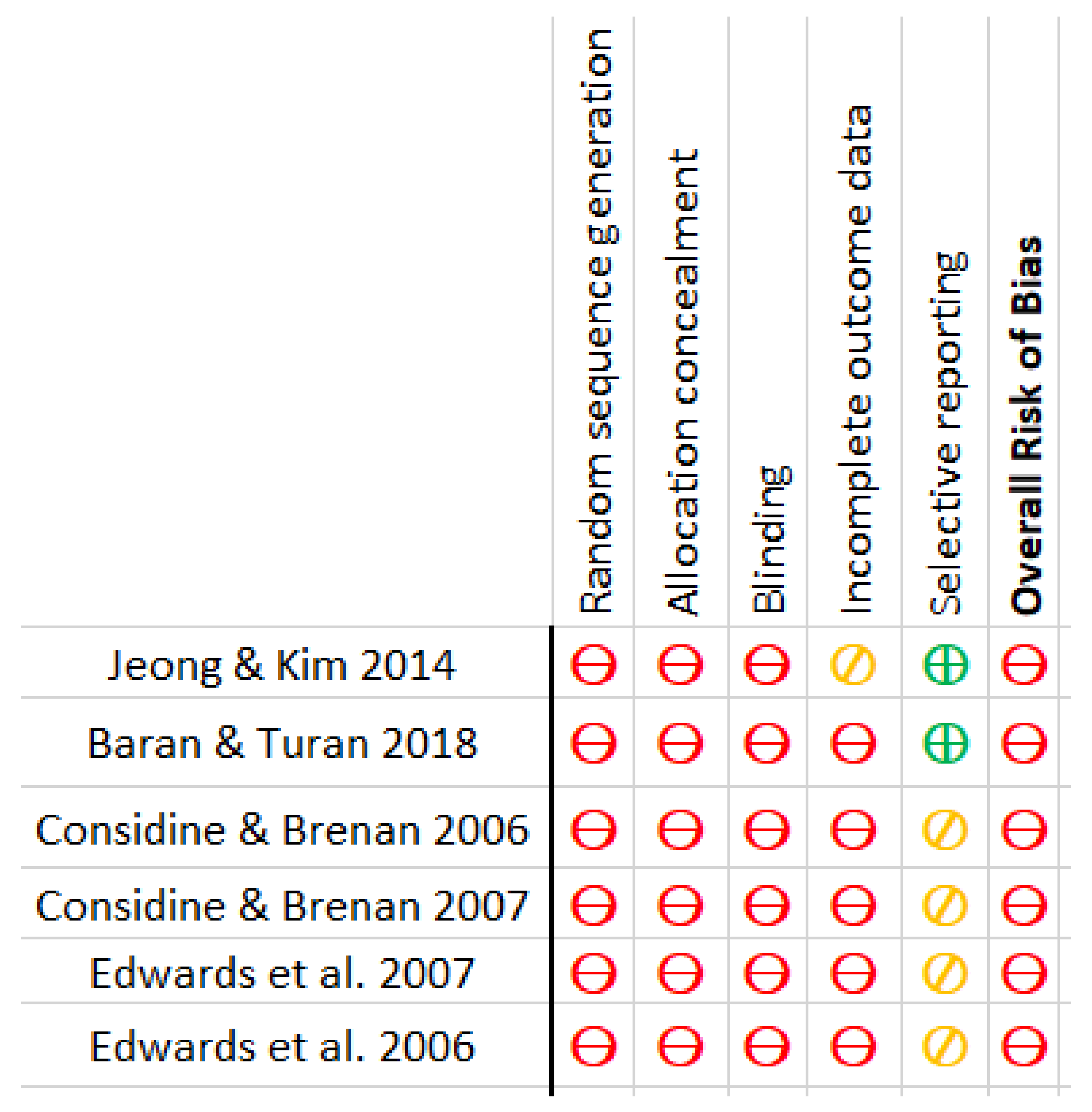
The bias risk of the articles included in the meta-analysis was evaluated. The authors agreed on the biases of the included research. The risk of bias was assessed using seven domains of the Cochrane Collaboration Tool version 5.1.0 [27], including appropriate sequence generation, allocation concealment, blinding, incomplete outcome measures, selective reporting, and other biases. First, the aspects of the studies related to the aforementioned domains were examined, and then the bias risk was determined. The risk levels were labeled as “low risk”, “high risk”, or “moderate/uncertain risk”. The overall risk of bias for each study was calculated based on the analysis of each domain separately. The rating was identified via the most prevalent risk of bias value in various items of each study.
2.7. Analysis and Synthesis
2.7.1. Qualitative Synthesis
The qualitative analysis was carried out to gain a better understanding of the phenomenon under investigation. The variables that influence the care and/or treatment of febrile children by health professionals were investigated. Non-analytical articles, or those that did not establish relationships between variables, were listed in this category of analysis. All of the articles could not be included in the meta-analysis due to their heterogeneity and non-analytical conditions.
2.7.2. Quantitative Synthesis
After that, studies with an analytical nature were considered for the meta-analysis. The articles evaluating educational programs for nurses that had at least two statistical measures of the variables were extracted. The Meta-Essentials Excel tool was used to create the meta-analysis. The articles’ analyses were divided into three groups based on the variables: those that evaluated knowledge, and those that investigated the attitudes and/or perceptions. If an article examined more than one variable, it might be classified as belonging to more than one category.
All the articles included in the meta-analysis shared the relationship of the variables through the mean and standard deviation (SD). Therefore, these two measures were chosen to compare the results of the various articles and draw conclusions.
The mean and SD of each variable were extracted from the pre-test and post-test results of the selected studies, depending on whether their intervention included an experimental and control group or only an experimental group. The standardized mean difference (SMD) at 95% confidence intervals (CI) was calculated by dividing the mean difference between the experimental and control groups by the SD of both groups. In each of Cohen’s studies, SMDs in the means were weighted by the inverse of their variance to obtain the pooled index of the magnitude of the effect. A random-effects model was selected due to the high heterogeneity of the studies.
The differences between the averages of the pre-test and post-test of experimental and control groups were calculated to determine the size effect of variables. Subsequently, the difference between the mean of the experimental and control group’s pre-tests was assessed. Accordingly, the size effect could be obtained by adding this difference to the experimental group mean difference based on the relation proposed by Cohen.
The magnitude effect of the involved variables was calculated for one of the studies that did not have a control group but had a pre-test and post-test of a single group. This was obtained by dividing the difference in the standardized means of the pre-test and post-test proposed by Cohen via the post-test SD. The magnitude effect was calculated using Rosenthal’s r because in a study lacking the mean and SD data (Considine & Brennan, 2007). The Z value was extracted by taking the square root of U Mann Whitney’s with N, which has the same properties as Cohen’s d.
Heterogeneity was assessed using the inferential Q test proposed by Cochrane and the I2 index of heterogeneity with its 95% CI. When I2 was more than 50%, heterogeneity was considered as high. The size effect was interpreted using the following thresholds: 0.2-small, 0.5-medium, and 0.8-large. The p-value of 0.05 was also used to determine statistical significance.
3. Results
3.1. Search Results
The search was completed in January 2021, with 1298 articles discovered in databases and 42 articles found using the “snowball” technique. After removing duplicates, there were 1046 articles left. 88 of the aforementioned cases were evaluated in full text for inclusion in the study. In addition, 47 papers were excluded for the following reasons: Concentration on parental knowledge, perceptions, and attitudes toward fever in children, focus on fever after vaccination, studying fever solely from a biological or pharmacological standpoint, defining malaise, and stating expert opinions as well as translations. Finally, 46 articles were derived. Forty-one were included in the qualitative synthesis, while the quantitative synthesis comprised 5 cases. This information is represented in Figure 1: PRISMA flowchart.

Figure 1.
PRISMA flowchart. From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097.
The included articles were then used to create two tables. Table 1 lists the articles included in the qualitative synthesis. This table provides the following information for each paper: design, data collection method, objectives, location and date, population and sample, results, conclusions, quality, and level of evidence. The second table (Table 2) summarizes articles that evaluated educational programs and could be used in the quantitative analysis. Therefore, the following sections were added to Table 2: Intervention and comparison, the number of participants in intervention and control groups, the measurement instrument applied, and the variables analyzed.

Table 1.
Quality of studies measured by “Critical Appraisal Skills Programme España” (CASPe) *. Levels of evidence used: “Scottish Intercollegiate Guidelines Network” SIGN (for studies with quantitative methodology) **; Gálvez Toro method (for studies with qualitative methodology) ***.
Table 2.
Quality of studies measured by “Critical Appraisal Skills Programme España” (CASPe) *. Levels of evidence used: “Scottish Intercollegiate Guidelines Network” SIGN (for studies with quantitative methodology) **; Gálvez Toro method (for studies with qualitative methodology) ***.
3.2. Description of the Included Studies
There are 18 bibliographic reviews (44%), 1 systematic review (2.4%), 21 studies with quantitative methodology (51.3%), and 1 qualitative research (2.4%) among the 41 articles included.
Among the qualitatively analyzed articles that used quantitative methods, descriptive ones using self-administered questionnaires were included (n = 12) [19,28,29,30,31,32,33,34,35,36,37,38], one of which was an audit of antipyretics administration records in hospitalized children [39].
Studies collected data on doctors’ practices (n = 9) [19,28,31,32,33,34,37,38,40], nurses’ practices (n = 4) [29,30,36,39], or both (n = 2) [35,41].
The descriptive studies included 472 nurses; 83 stated that they had training in pediatrics, but the majority referred to pediatric nurses; however, it was not specified whether the training was a regulated or official postgraduate course. The total number of doctors considered was 4651, with 4343 being pediatricians and 20 being resident doctors. Within the quantitative studies, quasi-experimental evaluating educational program effectiveness stood out (n = 6) [21,22,23,24,25,26]. There were 293 pediatric hospital nurses in total. The meta-analysis included five studies, one of which was excluded due to a lack of statistical data.
The meta-analysis was conducted with five studies that included samples from 59 Korean nurses [26], 126 Turkish nurses [21], 31 Australian nurses [22], and two other studies that did not specify the sample of Australian nurses used [20,24,25]. According to the bias analysis, none of the studies used adequate randomization for sample selection. Gender was only specified in two of the quantitative studies included in the investigation.
The average age of the participants was 31.51 years, with a standard deviation of 7.5 years [21,22,24,25,26]. In terms of participant distribution and design, 3 presented an experimental and control group, administrating pre-tests and post-tests in both groups [26], or including a “latency test” carried out 4 months after the educational intervention [24,25]. There were no procedures for group randomization used. The other three studies only presented an intervention category with the evaluation of a pre-test and a post-test in the same group [21,22]. Finally, a qualitative methodology based on focus groups in an Australian hospital with 15 nurses was included [20].
3.3. Variables Measured in the Educational Programs
3.3.1. Qualitative Analysis
The qualitative analysis was carried out by classifying the articles by educational programs for nurses that evaluated different outcomes to measure the efficacy of the studied program related to fever care for children, which would later be included in the quantitative meta-analysis. These classes were attitudes, knowledge, and perceptions.
As a result, the research was classified according to the variable they measured. When the evaluation of the education programs probed nurses’ understanding of fever physiology, fever management, and antipyretic drugs or measures, the results were categorized as knowledge. The attitude class contained tests that assessed changes in the professionals’ clinical practice regarding the management of a febrile child, performance against febrile convulsions, and the health education they would provide to parents following the training. The perceptions category included results relating to how parents, other nursing colleagues, and physicians influence the care of a febrile child, and how much control they have over the management of the febrile child.
The analyzed studies employed various educational methods and attempted to adjust these variables as well as different evaluation methods to determine whether these programs are effective. A Korean study compared a “blended learning program” (which combines traditional classes with online learning) to “face-to-face lessons” (Traditional classes). Based on the findings, there was no difference in effectiveness between the two methods, but the intervention group had higher satisfaction in both methodologies through pre-test and post-test [26]. Another study measured the increase in knowledge between the pre-test and the post-test for those who were given a “training booklet”. The authors specified that those who were provided the “training booklet,” had a slight increase in knowledge, but when each professional read this information on their own, it was impossible to control whether this reading was done correctly [21]. Two Australian studies compared the prior and subsequent knowledge of a group of nurses after receiving two tutorials. Only 45.2% of the participants completed the tutorials, and the rest of the professionals were given the information in writing prior to the evaluation [22,23]. Two other studies with the same sample compared the pre-test, post-test, and latency test of nurses who had participated in a peer education program to those who continued with their usual practice but did not specify which sample was the control group [24,25].
The studies were all performed in hospitals. Because of staff mobility, which resulted in the loss of professionals who changed units or terminated their contracts [24,25], the sampling method used was convenience [21,22,23], selecting nurses from two children’s hospitals [26], or choosing entire units. Although there were differences in nurse specialization, work experience, and unit category, no prior selection criteria were established. It should be noted that the majority of the sample’s losses occurred during the follow-up and evaluation of the educational program. Therefore, the studies included had a high risk of bias in participant selection.
In terms of questionnaires, all educational programs used a structured self-administered questionnaire in their tests. Four of them applied or adapted the “fever management survey” developed by Walsh et al. in 2005, which is divided into three other questionnaires: fever management knowledge (FMK), fever management attitudes (FMA), and fever management practices (FMP) [23,24,25,26]. The study authors created and validated one of them to assess knowledge [22] or used an unvalidated questionnaire to evaluate knowledge [21].
3.3.2. Quantitative Analysis and Meta-Analysis
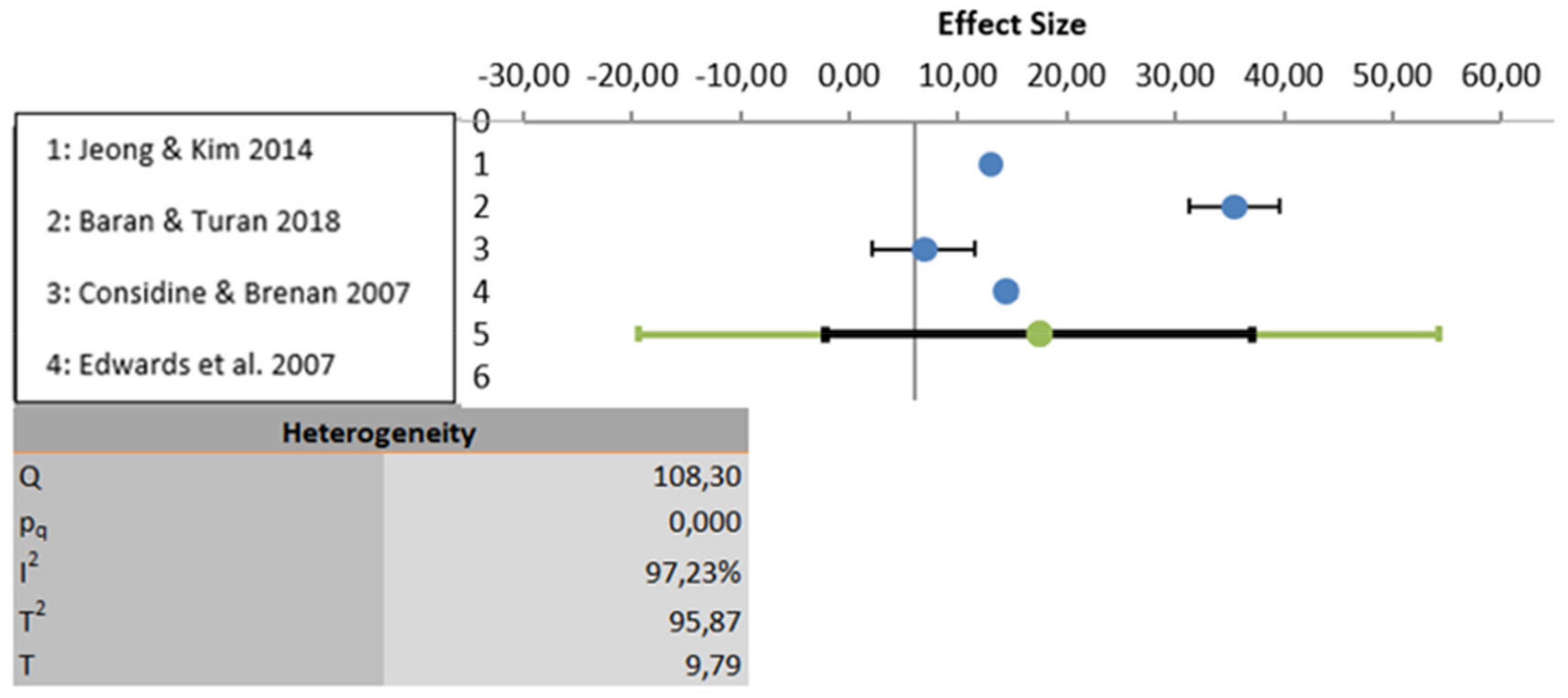
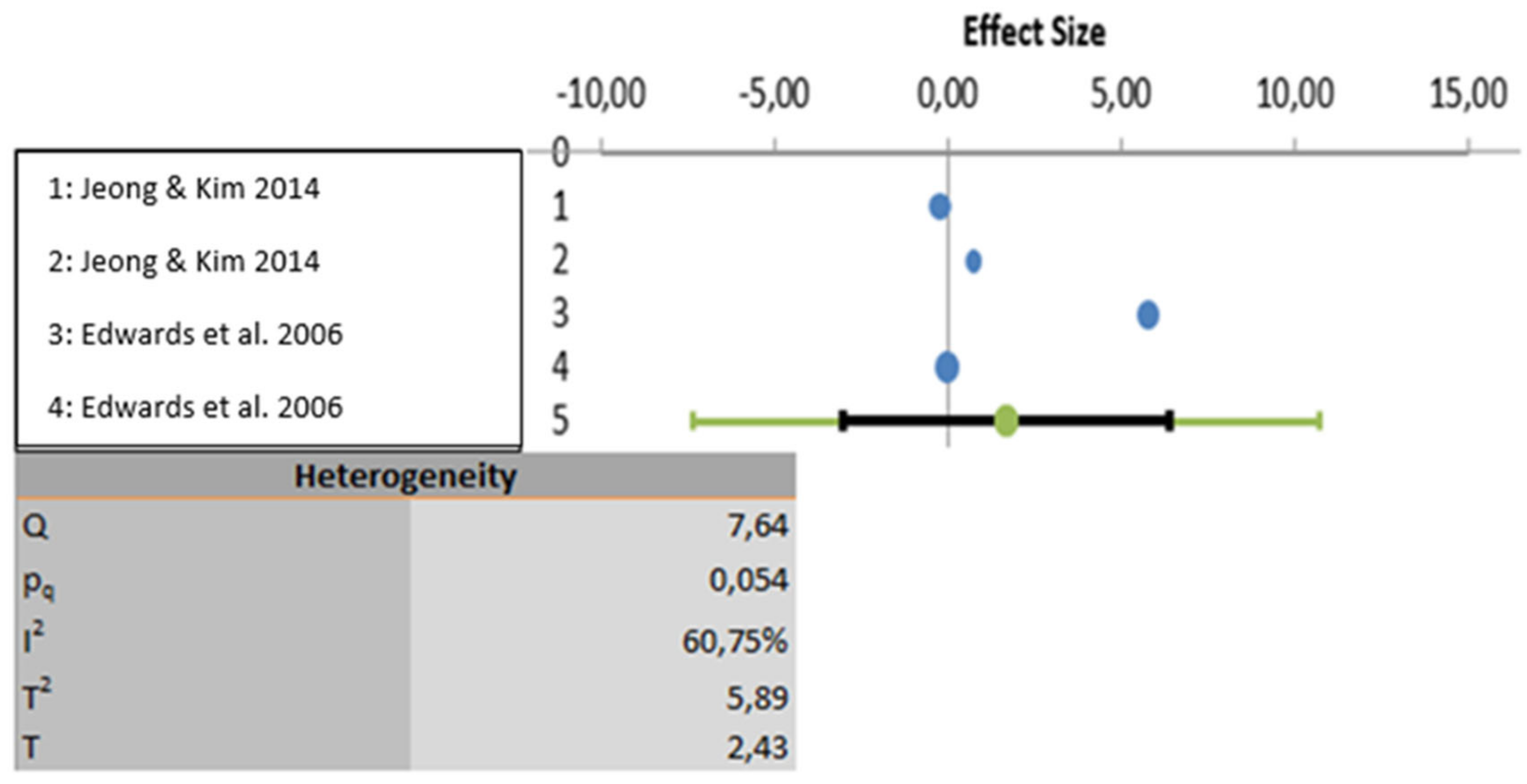
The meta-analysis was carried out based on five studies that evaluated educational programs [21,22,24,25,26]. One study was excluded because the results were not properly analyzed using statistical data [23]. All three variables show a high degree of heterogeneity. In the first-place knowledge is the variable with the highest heterogeneity (I2: 97.23%), followed by the variable attitudes (I2: 88.25%) and lastly the variable perceptions show the least heterogeneity (I2: 60.75%). Considering statistical significance, the knowledge and attitude variables show statistically significant results (p < 0.001) but the perceptions variable does not present statically significant result (p > 0.005). These analyses are depicted graphically in Figure 2, Figure 3 and Figure 4.

Figure 2.
Data analyzed for the variable knowledge.

Figure 3.
Data analyzed for the variable attitudes.

Figure 4.
Data analyzed for the variable perceptions.
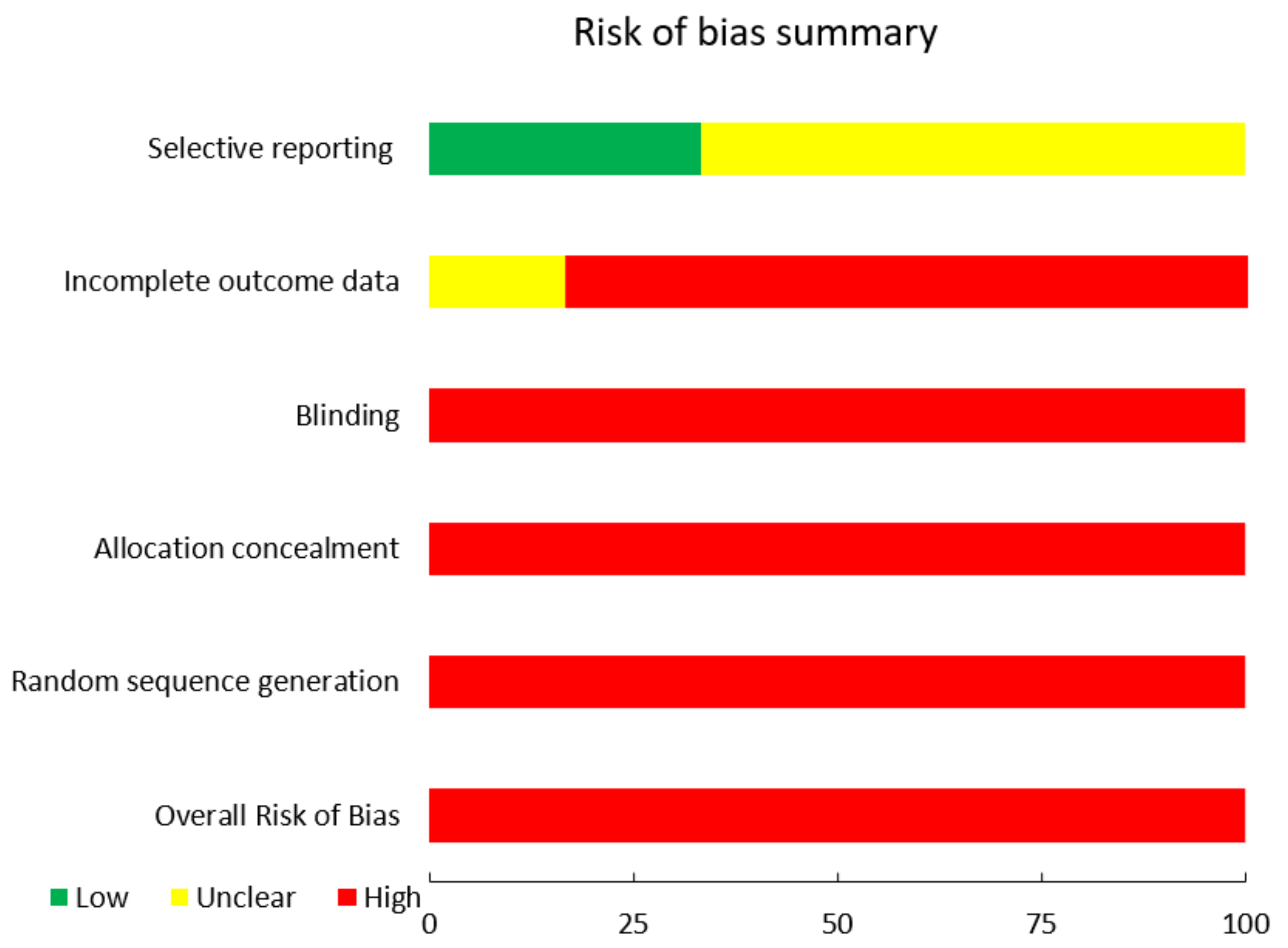
3.4. Risk of Bias
In general, all of the included studies had a high risk of bias. In addition, all were at high risk of insufficient sequence generation, allocation concealment, and blinding [21,22,23,24,25,26]. With the exception of one, all had a high risk of bias due to incomplete outcome measures [26]. Two of the reports chosen had a low risk of bias [21,26], while the others had a moderate risk level [22,23,24,25]. The risk of bias in the included articles is graphically depicted in Figure 5 and Figure 6.
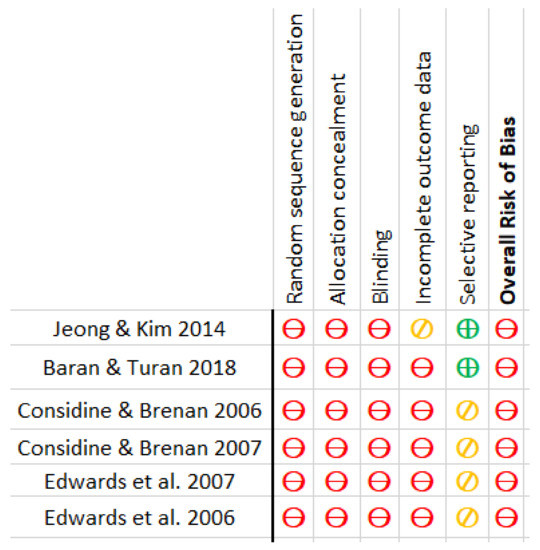
Figure 5.
Risk of Bias.

Figure 6.
Risk of Bias Summary.
4. Discussion
This systematic review included 41 studies to determine whether the knowledge, perceptions, and attitudes toward fever by doctors and nurses who work with children affect antipyretic measures. In addition, we aimed to assess if the educational programs included in the meta-analysis could lead to changes in the usual clinical practice of nursing care of the febrile child.
As Razón points out, lack of knowledge and understanding of this process leads to the use of aggressive treatments to achieve normothermia, such as combination antipyretic therapy [1]
Nurses and doctors agreed that fever might be beneficial, but they were concerned about the long-term consequences. For example, 50% of nurses in Ireland supposed that fever has beneficial effects on the immune system, and 84.9% reflected that regular paracetamol usage could disguise symptoms, but that fever should be treated rapidly to avoid febrile seizures [29].
The research demonstrated that a temperature limit, rather than discomfort, was the most important criterion for providing antipyretics. According to Radhi’s study, most physicians believe that antipyretic medication is intended to reduce fever symptoms; therefore, doctors tend to prescribe antipyretics for every child with this sign. As a result, it could be given to a child who is depressed as well as a playing child [5,9].
In one study, parents were advised to use antipyretics whenever the temperature rose above 38.3 °C [28]. Another study reported the temperature limits used by Argentine doctors to administer antipyretics, when 49% managed it at 38 °C or lower [37]. In a Spanish study, only three doctors advocated the general condition as a criterion for delivering antipyretics. Meanwhile, 67.8% of primary care pediatricians and 66.7% of hospital pediatricians recommended antipyretics when the temperature reached 38 °C [38].
According to an audit conducted in a hospital of the same nationality, 45% of antipyretics were given at temperatures below 38.3 °C. Although the authors of a recent study clarified that these medications could also be used for purposes other than temperature control, such as pain relief or discomfort, the reasons for their use were not explicitly stated in the reviewed article [39].
According to the pediatricians who participated in the Martins & Abecasis study, fever is a healthy physiological process for the immune system, and the child’s health should be considered during treatment due to the discomfort it may cause. However, antipyretics are still recommended by 78.1% of family doctors and 81.4% of pediatricians [35].
A mixture of antipyretics was shown to be effective in lowering body temperature. However, its safety, efficacy in improving the child’s comfort, and other clinical outcomes are still questioned [2,3,4,8,11,15]. Even so, only 15% thought the child’s discomfort as the first symptom [41]. Similarly, 76.1% of a Spanish pediatrician sample maintained this practice, with the caveat that it should only be used in exceptional cases [38].
Physical treatments such as applying the cold compresses or removing the child’s clothing would counter fever treatment [2,4,5,8,11,16]. Other examples using these strategies in pediatricians could be found in the Lava et al. research, where only 7% of pediatricians prescribe antipyretic therapy as an alternative. Whereas 65% recommended physical temperature lowering strategies [31].
The usage or recommendation of various temperature reduction methods by doctors and nurses has also been examined through descriptive research, and the practice may have changed over time. As an example, studies attended by Chiappini et al. in 2009, 2012, and 2015 clarified that the percentage of pediatricians using alternative antipyretic therapy or suggesting it to reduce the incidence of febrile seizures has decreased from 27% to 12.2%. There has also been a reduction in the recommendation of physical measures from 65% to 52%. Although, the recommendation of thinking about the child’s discomfort rather than a temperature was declined from 45.3 to 38.2% [33,34,40].
Notably the present review has focused on the knowledge, attitudes, and perceptions of professionals about fever in children, however several studies have shown that how professionals treat fever influences parents.
In this regard, it is worth noting that most authors seem to agree that the aggressive fever management by professionals promotes parental fear of this sign and their desire to achieve normothermia in their children [2,3,10,14,17]. This results in a rebound effect in which the parents’ anxiety influences the professionals, who seek to quickly resolve fever to satisfy them and reduce their anxiety [1,5,7]. When asked about this, pediatricians denied reducing fever to calm parents (81% and 63%) [31,32]. Moreover, the nurses did mention that parents were pressuring them to provide their children antipyretics [20].
Consequently, researchers have developed actions to change nurses’ attitudes, perceptions, and/or knowledge in pediatric practice by measuring the efficacy of various educational methods.
Edwards’s examination demonstrated that peer education could increase general knowledge about fever but did not significantly improve knowledge about antipyretics. In terms of attitudes, they reported a significant improvement [24]. There were no differences in attitudes toward the efficacy of antipyretics between groups. In contrast, in the experimental group, the perception of control increased, and the intention to use antipyretics decreased [25].
Jeong and Kim compared a hybrid online and face-to-face approach versus a traditional method. Based on the findings, both the control and intervention groups significantly improved their knowledge of fever, attitudes, and intentions to use antipyretics. Nevertheless, regulatory influences and the perception of control did not change significantly. As a result, while the type of education did not improve the traditional method, it resulted in a higher level of satisfaction [26]. In other cases, using a training book slightly increased their knowledge [21]. Another study measured face-to-face tutorials and concluded that they improve knowledge and clinical practice [22,23]. In general, meta-analysis revealed that educational methods cause a statistically significant change in knowledge and attitudes, as opposed to perceptions which did not show a statistically significant change.
There are some limitations to this review. Due to language limitations, relevant studies might have been left out. In addition, the use of unvalidated questionnaires in articles may restrict the validity of the results. Furthermore, the study phenomenon, i.e., attitudes, knowledge, and perceptions, are variables that are difficult to quantify.
5. Conclusions
The attitudes, knowledge, and perceptions of health professionals that lead to overtreatment and overestimation of fever in children have received little attention. According to the reviewed literature, the way professionals understand fever and how they respond to it may result in fever management in children based on overtreatment and overestimation of fever and its complications, reflecting a possible irrational fear of this sign. On the one hand, most studies are descriptive and do not investigate these issues analytically, making it difficult to draw conclusions with a high level of evidence. Existing studies that evaluate educational programs, on the other hand, are an intriguing approach to this phenomenon, as they attempt to change knowledge, perceptions, and attitudes to modify daily clinical practice. Meanwhile, they still present a high risk of bias, and their efficacy cannot be affirmed. A qualitative study could delve deeper into the phenomenon, determining the reasons and acting based on them. The majority of the included studies, according to the SIGN scale “Scottish Intercollegiate Guidelines Network”, have a descriptive evidence level of 3 or a quasi-experimental level of 2. As a result, we can give a grade of recommendation D on the use of educational programs for the modification of attitudes, perceptions, and knowledge about fever in children and the improvement of clinical practice in nurses. Hence, the interventions evaluated cannot be recommended or discouraged.
Author Contributions
Conceptualization, F.V.-B. and J.M.-M.; methodology, F.V.-B. and J.M.-M.; software, F.V.-B. and J.M.-M.; validation, F.V.-B. and J.M.-M. and R.M.-B.; formal analysis, F.V.-B. and J.M.-M.; investigation, F.V.-B. and J.M.-M. and R.M.-B.; data curation, F.V.-B.; writing—original draft preparation, F.V.-B.; writing—review and editing, F.V.-B. and J.M.-M. and R.M.-B.; supervision, J.M.-M. and R.M.-B. All authors have read and agreed to the published version of the manuscript.
Funding
This systematic review with meta-analysis has no sources of funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data of this study are the included tables, figures, and referenced articles.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Razón Behar, R. Fiebrefobia. Rev. Cuba. Pediatr. 2011, 83, 431–441. [Google Scholar]
- Sullivan, J.E.; Farrar, H.C. Section on Clinical Pharmacology, Committee on Drugs. Fever and antipyretic use in children. Pediatrics 2011, 127, 580–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzuillo, P.; Guarino, S.; Barbi, E. Paracetamol: A focus for the general pediatrician. Eur. J. Pediatr. 2014, 173, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.; Purssell, E. Who’s Afraid of fever. Arch. Dis. Child. 2015, 100, 818–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Radhi, A.S.M. Why is the evidence not affecting the practice of fever management? Arch. Dis. Child. 2008, 93, 918–920. [Google Scholar] [CrossRef] [PubMed]
- Purssell, E. Antipyretic use in children: More than just temperature. J. Pediatr. 2013, 89, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purssell, E. Fever in children—A concept analysis. J. Clin. Nurs. 2013, 23, 3575–3582. [Google Scholar] [CrossRef] [PubMed]
- Crocetti, M.T.; Serwint, J.R. Fever: Separating fact from fiction. Contemp. Pediatr. 2005, 22, 34–42. [Google Scholar]
- El-Radhi, A.S.M. Fever management: Evidence vs current practice. World J. Clin. Pediatr. 2012, 1, 29–33. [Google Scholar] [CrossRef]
- Clarke, P. Evidence-Based Management of Childhood Fever: What Pediatric Nurses Need to Know. J. Pediatr. Nurs. 2014, 29, 372–375. [Google Scholar]
- McDougall, P.; Harrison, M. Fever and feverish illness in children under five years. Nurs. Stand. R. Coll. Nurs. 2014, 28, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Niehues, T. The Febrile Child: Diagnosis and Treatment. Dtsch. Arztebl. Int. 2013, 110, 764–774. [Google Scholar] [PubMed] [Green Version]
- Warwick, C. Paracetamol and fever management. J. R. Soc. Promot. Health 2008, 128, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Sherman, J.M.; Sood, S.K. Current challenges in the diagnosis and management of fever. Curr. Opin. Pediatr. 2012, 24, 400–406. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22525720 (accessed on 6 January 2021). [CrossRef] [PubMed]
- Teuten, P.; Paul, S.P.; Heaton, P.A. Management of childhood febrile illness. J. Fam. Health 2015, 25, 26–29. [Google Scholar]
- Glatstein, M.; Scolnik, D. Fever: To treat or not to treat? World J. Pediatr. 2008, 4, 245–247. [Google Scholar] [CrossRef]
- Navarro García, M.A.; De Carlos Alegre, V. La fiebre en los niños. Guía de cuidados. ROL Enfermería 2010, 33, 55–62. [Google Scholar]
- Clericetti, C.M.; Milani, G.P.; Bianchetti, M.G.; Simonetti, G.D.; Fossali, E.F.; Balestra, A.M.; Bozzini, M.A.; Agostoni, C.; Lava, S.A. Systematic review finds that fever phobia is a worldwide issue among caregivers and healthcare providers. Acta Paediatr. Int. J. Paediatr. 2019, 108, 1393–1397. [Google Scholar] [CrossRef] [PubMed]
- Demir, F.; Sekreter, O. Knowledge, attitudes and misconceptions of primary care physicians. Ital. J. Pediatr. 2012, 38, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, H.E.; Courtney, M.D.; Wilson, J.E.; Monaghan, S.J.; Walsh, A.M. Fever management practices: What pediatric nurses say. Nurs. Health Sci. 2001, 3, 119–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baran, G.; Turan, E. Investigation of the Effect of the Training on Fever and Febrile Convulsion Management Given to Pediatric Nurses on Their Knowledge Level. Int. J. Caring Sci. 2018, 11, 677–685. [Google Scholar]
- Considine, J.; Brennan, D. Effect of an evidence-based paediatric fever education program on emergency nurses’ knowledge. Accid. Emerg. Nurs. 2007, 15, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Considine, J.; Brennan, D. Emergency nurses’ opinions regarding paediatric fever: The effect of an evidence-based education program. Australas Emerg. Nurs. J. 2006, 9, 101–111. [Google Scholar] [CrossRef]
- Edwards, H.; Walsh, A.; Courtney, M.; Monaghan, S.; Wilson, J.; Young, J. Improving paediatric nurses’ knowledge and attitudes in childhood fever management. J. Adv. Nurs. 2007, 57, 257–269. [Google Scholar] [CrossRef] [Green Version]
- Edwards, H.; Walsh, A.; Courtney, M.; Monaghan, S.; Wilson, J.; Young, J. Promoting evidence-based childhood fever management through a peer education programme based on the theory of planned behaviour. J. Clin. Nurs. 2006, 16, 1966–1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, Y.S.; Kim, J.S. Childhood fever management program for Korean pediatric nurses: A comparison between blended and face-to-face learning method. Contemp. Nurse 2014, 49, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Centro Cochrane Iberoamericano. Manual Cochrane de Revisiones Sistemáticas de Intervenciones, Versión 5.1.0. In Centro Cochrane Iberoamericano: Barcelona; 2012. [Google Scholar]
- El Khoury, A.C.; Durden, E.; Larry, M.; Markson, L.E.; Lee, A.W.; Duan, Y.; Foley, K. Perception and management of fever in infants up to six months of age: A survey of US pediatricans. BMC Pediatr. 2010, 10, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Greensmith, L. Nurses’ knowledge of and attitudes towards fever and fever management in one Irish children’s hospital. J. Child Health Care 2012, 17, 305–316. [Google Scholar] [CrossRef]
- Walsh, A.M.; Edwards, H.E.; Courtney, M.D.; Wilson, J.E.; Monaghan, S.J. Paediatric fever management: Continuing education for clinical nurses. Nurse Educ. Today 2006, 26, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lava, S.A.G.; Simonetti, G.D.; Ramelli, G.P.; Tschumi, S.; Bianchetti, M.G. Symptomatic management of fever by Swiss board-certified pediatricians: Results from a cross-sectional, Web-based survey. Clin. Ther. 2012, 34, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Bettinelli, A.; Provero, M.C.; Cogliati, F.; Villella, A.; Marinoni, M.; Saettini, F.; Bianchetti, M.G.; Nespoli, L.; Galluzzo, C.; Lava, S.A.G. Symptomatic fever management among 3 different groups of pediatricians in Northern Lombardy (Italy): Results of an explorative cross-sectional survey. Ital. J. Pediatr. 2013, 39, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiappini, E.; Parretti, A.; Becherucci, P.; Pierattelli, M.; Bonsignori, F.; Galli, L.; de Martino, M. Parental and medical knowledge and management of fever in Italian pre-school children. BMC Pediatr. 2012, 12, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Chiappini, E.; D’Elios, S.; Mazzantini, R.; Becherucci, P.; Pierattelli, M.; Galli, L.; de Martino, M. Adherence among Italian pediatricians to the Italian guidelines for the management of fever in children: A cross sectional survey. BMC Pediatr. 2013, 13, 210–216. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24350822 (accessed on 2 January 2021). [CrossRef] [PubMed] [Green Version]
- Martins, M.; Abecasis, F. Healthcare professionals approach paediatric fever in significantly different ways and fever phobia is not just limited to parents. Acta Paediatr. Int. J. Paediatr. 2016, 105, 829–833. [Google Scholar] [CrossRef]
- Walsh, A.M.; Edwards, H.E.; Courtney, M.D.; Wilson, J.E.; Monaghan, S.J. Fever management: Paediatric nurses’ knowledge, attitudes and influencing factors. J. Adv. Nurs. 2005, 49, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Melamud, A.; Suwezda, A.; Matamoros, R.; Ringuelet, L. Indicación de antitérmicos por médicos pediatras. Internet como modalidad de recolección de datos. Arch. Argent. Pediatr. 2008, 106, 404–408. [Google Scholar] [PubMed]
- García Puga, J.M.; Garrido Torrecillas, F.J.; Hernández Morillas, D.; Castillo Díaz, L.; Santos Pérez, J.L.; Callejas Pozo, J.E.; Ortega Páez, E.; Jiménez Romero, T.; Expósito Ruiz, M.; Ruiz Extremera, Á. Análisis del conocimiento y manejo de la fiebre por parte de pediatras y residentes en relación a un proceso asistencial establecido. Rev. Pediatr. Aten. Primaria 2012, 14, 115–126. [Google Scholar] [CrossRef] [Green Version]
- Edwards, H.E.; Courtney, M.D.; Wilson, J.E.; Monaghan, S.J.; Walsh, A.M. Fever management audit: Australian nurses’ antipyretic usage. Pediatr. Nurs. 2003, 29, 31–37. [Google Scholar] [PubMed]
- Chiappini, E.; Cangelosi, A.M.; Becherucci, P.; Pierattelli, M.; Galli, L.; de Martino, M. Knowledge, attitudes and misconceptions of Italian healthcare professionals regarding fever management in children. BMC Pediatr. 2018, 18, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Mayoral, C.E.; Marino, R.V.; Rosenfeld, W.; Greensher, J. Alternating antipyretics: Is this an alternative? Pediatrics 2000, 105, 1009–1012. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).