
Healthy Moms and Babies Preventive Psychological Intervention Application: A Study Protocol


 and
and
Abstract
:1. Introduction
2. Methods
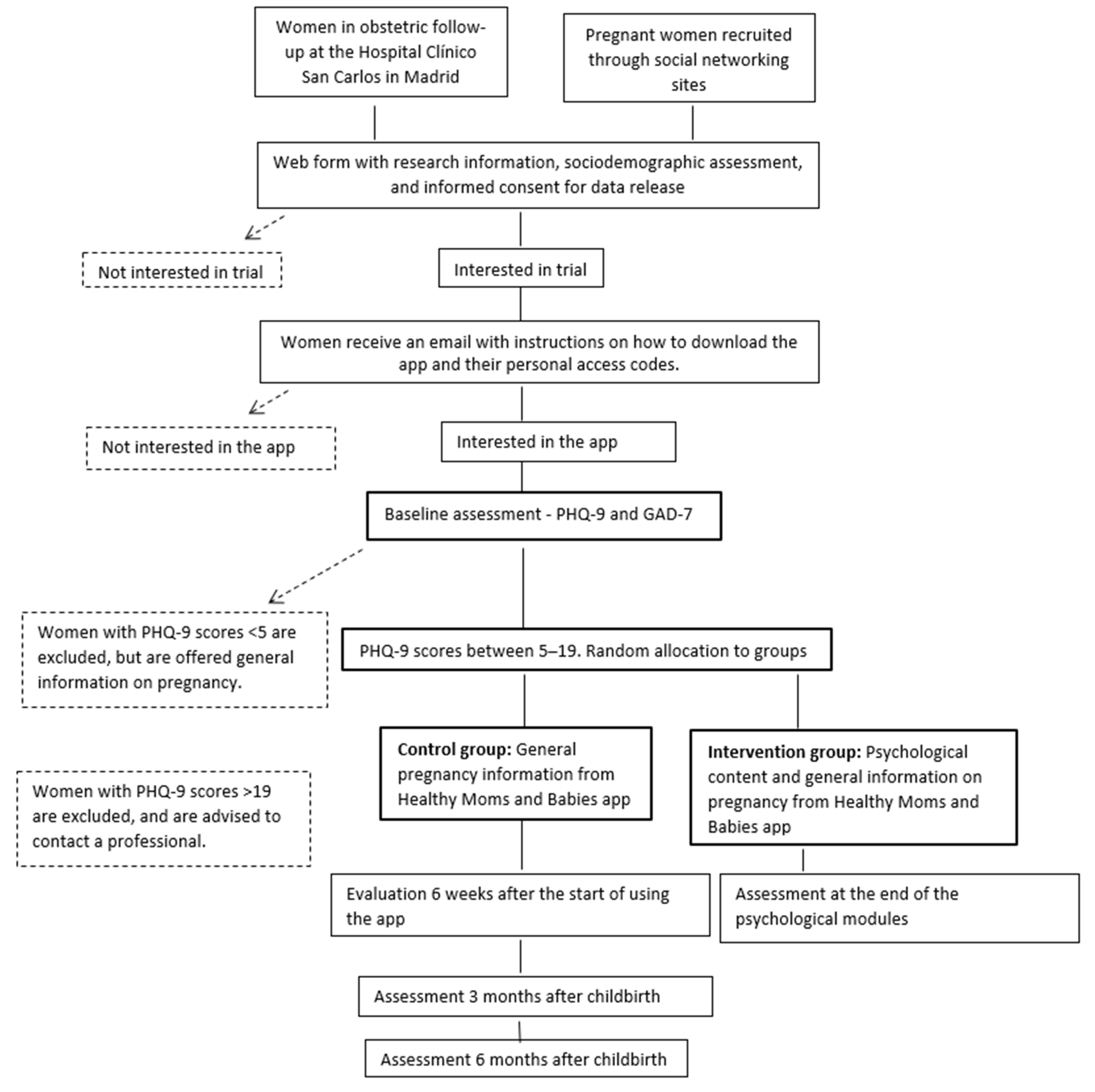
2.1. Design and Population
2.2. Recruitment of Women
2.2.1. Identification and Recruitment in the Obstetrics and Gynecology Department
2.2.2. Mass Recruitment on Social Media
2.2.3. Evaluation, Downloading Instructions and Accessing Passwords
2.3. Outcomes and the Allocation of Participants to Trial Groups
2.3.1. Primary Outcome
2.3.2. Secondary Outcome
2.4. Inclusion and Exclusion Criteria
2.5. Randomization
2.6. Adherence
2.7. Ethical Standards
2.8. Sample Size
2.9. Analysis Plan
3. Intervention
3.1. Rationale
3.2. Goals of the Intervention
3.3. Overview of the Intervention
3.4. Email Reminders to Increase App Utilization
3.5. Intervention Quality Control Procedures
3.6. Usual Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal depression: A systematic review of prevalence and incidence. Obstet. Gynecol. 2015, 106, 1071–1083. [Google Scholar] [CrossRef]
- Rodríguez-Muñoz, M.F.; Castelao-Legazapi, P.C.; Olivares-Crespo, M.E.; Soto-Balbuena, C.; Izquierdo-Méndez, N.; Ferrer-Barrientos, F.J.; Huynh-Nhu, L. PHQ-2 como primer instrumento de cribado de la depresión prenatal. Rev. Esp. Salud. Pública 2017, 91, 1–8.e201701010. [Google Scholar]
- Muñoz, R.F. Prevent depression in pregnancy to boost all mental health. Nature 2019, 574, 631–633. [Google Scholar] [CrossRef]
- Fonseca, A.; Ganho-Ávila, A.; Lambregtse-van den Berg, M.; Lupatteli, A.; Rodríguez-Muñoz, M.F.; Ferrerira, P.; Nakié Rados, S.; Bina, R. Emerging issues and questions on peripartum depression prevention, diagnosis and treatment: A consensus report from the cost action riseup-PPD. J. Affect. Disord. 2020, 274, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Roshaidai, S.; Arifin, M.; Cheyne, H.; Maxwell, M. Review of the prevalence of postnatal depression across cultures. AIMS Public Health 2018, 5, 260–295. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.K.; Marcos, G.; Abelha, L.; Fortes, L.; Ferdandes de Cintra Santos, J.; Agadir, S.; Lima, D.; Valencia, E. Depression during Pregnancy: Review of Epidemiological and Clinical Aspects in Developed and Developing Countries [Internet]. Intechopen-Brazil, 2011. Available online: https://www.intechopen.com/books/psychiatric-disorders-trends-and-developments/depression-during-pregnancy-review-of-epidemiological-and-clinical-aspects-in-developed-and-developi (accessed on 15 June 2020).
- Rodríguez-Muñoz, M.F.; Huynh-Nhu, L.; Vargas de la Cruz, I.; Olivares Crespo, M.E.; Izquierdo Méndez, N. Feasibility of screening and prevalence of prenatal depression in an obstetric setting in Spain. Eur. J. Obstet. Gynecol. Reprod Biol. 2017, 215, 101–105. [Google Scholar] [CrossRef]
- Marcos-Nájera, R.; Rodríguez-Muñoz, M.F.; Soto Balbuena, C.; Olivares Crespo, M.E.; Izquierdo Méndez, N.; Huynh-Nhu, L.; Escudero Gomis, A. The prevalence and risk factors for antenatal depression among pregnant immigrant and native women in Spain. J. Transcult. Nurs. 2019, 31, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Sanjuan, J.; Martín-Santos, R.; García-Esteve, L.; Carot, M.; Guillamat, R.; Gutierrez-Zotes, A.; Gornemann, I.; Canellas, F.; Baca-Garcia, E.; Jover, M.; et al. Mood changes after delivery: Role of the serotonin transporter gene. Br. J. Psychiatry 2008, 193, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Sanidad y Políticas Sociales. Sistema Nacional de Salud; Ministerio de Sanidad y Políticas Sociales: Madrid, Spain, 2010. [Google Scholar]
- Falah-Hassani, K.; Shiri, R.; Dennis, C.L. Prevalence and risk factors for comorbid postpartum depressive symptomatology and anxiety. J. Affect. Disord 2016, 198, 142–147. [Google Scholar] [CrossRef]
- Soto-Balbuena, C.; Rodríguez-Muñoz, M.F.; Escudero Gomis, A.I.; Ferrer Barriendos, F.J.; Huynh-Nhu, L.; Grupo PMB-HUCA. Incidence, prevalence, and risk factors related to anxiety symptoms during pregnancy. Psicothema 2018, 30, 257–263. [Google Scholar] [CrossRef]
- Sutter-Dallay, A.; Giaconne-Marcesche, V.; Glatigny-Dallay, E.; Verdoux, H. Women with anxiety disorders during pregnancy are at increased risk of intense postnatal depressive symptoms: A prospective survey of the MATQUID cohort. Eur. Psychiatry 2004, 19, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Field, T. Prenatal depression effectcs on early development: A review. Infant. Behav. Dev. 2011, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Śliwerski, A.; Kossakowska, K.; Jarecka, K.; Świtalska, J.; Bielawska-Batorowicz, E. The effect of maternal depression on infant attachment: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 2675. [Google Scholar] [CrossRef] [Green Version]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, P.; Brouyere, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Women Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef] [Green Version]
- Fonagy, P.; Target, M.; Cottrell, D.; Phillips, J.; Kurtz, Z. What Works for Whom? A Critical Review of Treatments for Children and Adolescents; Guilford: New York, NY, USA, 2002. [Google Scholar]
- Cox, E.Q.; Sowa, N.A.; Meltzer-Brody, S.E.; Gaynes, B.N. The Perinatal Depression Treatment Cascade: Baby Steps toward Improving Outcomes. J. Clin. Psychiatry. 2016, 77, 1189–1200. [Google Scholar] [CrossRef] [PubMed]
- US Preventive Services Task Force. Interventions to Prevent Perinatal Depression. US Preventive ServicesTask Force Recommendation Statement. J. Am. Med. Assoc. 2019, 321, 580–587. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; Weitz, E.; Karyotaki, E.; Garber, J.; Anderson, G. The effects of psychological treatment of maternal depression on children and parental functioning: A meta-analysis. Eur. Child. Adolesc. Psychiatry 2015, 24, 237–245. [Google Scholar] [CrossRef]
- Camacho, E.M.; Shields, G.E. Cost-effectiveness of interventions for perinatal anxiety and/or depression: A systematic review. BMJ Open 2018, 8, e022022. [Google Scholar] [CrossRef]
- Luca, D.L.; Margiotta, C.; Staatz, C.; Garlow, E.; Christensen, A.; Zivin, K. Financial Toll of Untreated Perinatal Mood and Anxiety Disorders Among 2017 Births in the United States. Am. J. Public Health 2020, 110, 888–896. [Google Scholar] [CrossRef]
- Centre of Perinatal Excelence. Mental Health the Consequences of Not Treating Perinatal Depression and Anxiety 2014. Available online: https://cope.org.au/wp-content/uploads/2013/12/PWC-2013_Final3.pdf (accessed on 15 July 2021).
- Rodriguez-Muñoz, M.F.; Huynh-Nhu, L.; Lara Cantú, M.A.; Jaffe, A. Depresión Perinatal. En Rodríguez-Muñoz Coord, Psicología Perinatal: Teoría y Práctica; Pirámide: Madrid, Spain, 2019; pp. 25–54. [Google Scholar]
- Bina, R.; Glasser, S. Factors associated with attitudes toward seeking mental health treatment postpartum. Women Health 2018, 59, 1–12. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.; McMahon, C. Acceptance and experience of treatment for postnatal depression in a community mental health setting. Health Care Women Int. 2008, 29, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.H. Women’s attitudes, preferences, and perceived barriers to treatment for perinatal depression. Birth 2009, 36, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.; Chung-Lee, L. Postpartum depression help-seeking barriers and maternal treatment preferences: A qualitative systematic review. Birth 2006, 33, 323–331. [Google Scholar] [CrossRef]
- Barrera, A.Z.; Rosales, M.; Ruiz-Segovia, N.; Rodríguez-Muñoz, M.F. Sistemas e-Health en el Periodo Perinatal. En Rodríguez-Muñoz Coord., Psicología Perinatal: Teoría y Práctica; Pirámide: Madrid, Spain, 2019; pp. 371–381. [Google Scholar]
- Lee, E.W.; Denison, F.C.; Kahyee, H.; Reynolds, R.M. Web-based interventions for prevention and treatment of perinatal mood disorders: A systematic review. BMC Pregnancy Childbirth 2016, 16, 38. [Google Scholar] [CrossRef] [Green Version]
- Ashford, M.T.; Olander, E.K.; Ayers, S. Computer- or web-based interventions for perinatal mental health: A systematic review. J. Affect. Disord 2016, 197, 134–146. [Google Scholar] [CrossRef]
- Danaher, B.G.; Milgrom, J.; Seeley, J.R.; Stuart, S.; Schembri, C.; Tyler, M.S.; Ericksen, J.; Lester, W.; Gemmill, A.W.; Kosty, D.B.; et al. MomMoodBooster Web-Based Intervention for Postpartum Depression: Feasibility Trial Results. J. Med. Internet Res. 2013, 15, e2876. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, A.; Pereira, M.; Araújo-Pedrosa, A. Be a Mom: Formative evaluation of a Web-Based Psychological Intervention to Prevent Postpartum Depression. Cogn. Behav. Pract. 2018, 25, 473–495. [Google Scholar] [CrossRef]
- Fonseca, A.; Monteiro, F.; Alves, S.; Gorayeb, R.; Canavarro, M.C. Be a Mom, a Web-Based Intervention to prevent postpartum depression: The enhancement of self-regulatory skills and its association with postpartum, depressive symptoms. Front. Psychol. 2019, 10, 265. [Google Scholar] [CrossRef]
- Barrera, A.Z.; Wickham, R.E.; Muñoz, R.F. Online prevention of postpartum depression for Spanish- and English-speaking pregnant women: A pilot randomized controlled trial. Int. Interv. 2015, 2, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Duffecy, J.; Grekin, R.; Hinkel, H.; Gallivan, N.; Nelson, G.; O’Hara, M.W. A Group-Based Online Intervention to Prevent Postpartum Depression (Sunnyside): Feasibility Randomized Controlled Trial. JMIR Ment. Health 2019, 6, e10778. [Google Scholar] [CrossRef] [Green Version]
- Osma, J.; Barrera, A.; Ramphos, E. Are pregnant and postpartum women interested in health-related apps? Implications for the prevention of perinatal depression. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 412–415. [Google Scholar] [CrossRef]
- O’Higgins, A.; Murphy, O.C.; Egan, A.; Mullaney, L.; Sheehan, S.; Turner, M.J. The use of digital media by women using the maternity services in a developed country. Ir. Med. J. 2014, 107, 313–315. [Google Scholar]
- Lupton, D.; Pedersen, S. An Australian survey of women’s use of pregnancy and parenting apps. Women Birth 2016, 29, 368–375. [Google Scholar] [CrossRef] [Green Version]
- Unión Internacional de Telecomunicaciones. Tendencias en las Reformas de Telecomunicaciones 2015; Unión Internacional de telecomunicaciones: Geneva, Switzerland, 2015. [Google Scholar]
- Thomas, G.M.; Lupton, D. Threats and thrills: Pregnancy apps, risk, and consumption. Health Risk Soc. 2015, 17, 495–509. [Google Scholar] [CrossRef]
- Peñate, W. About the effectiveness of telehealth procedures in psychological treatment. Int. J. Clin. Health Psychol. 2012, 12, 475–487. [Google Scholar]
- O’Mahen, H.A.; Woodford, J.; McGinley, J.; Warren, F.C.; Richards, D.A.; Lynch, T.R.; Taylor, R.S. Internet-based behavioral activation treatment for postnatal depression Netmums : A randomized controlled trial. J. Affect. Disord. 2013, 150, 814–822. [Google Scholar] [CrossRef]
- Linardon, J.; Cuijpers, P.; Carlbring, P.; Messer, M.; Fuller-Tyszkiewicz, M. The efficacy of app-supported smartphone interventions for mental health problems: A meta-analysis of randomized controlled trials. World Psychiatry 2019, 18, 325–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ledford, C.J.W.; Cazona, M.R.; Cafferty, L.A.; Hodge, J.A. Mobile application as a prenatal education and engagement tool: A randomized controlled pilot. Patient Educ. Couns 2016, 99, 578–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- INE. Anuario de Estadística 2019. Available online: https://www.ine.es/prodyser/pubweb/anuario19/anu19_completo.pdf (accessed on 15 May 2021).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Pfizer. Patient Health Questionnaire PHQ-9 2007. Available online: http://www.phqscreeners.com/ (accessed on 15 June 2021).
- Kroenke, K.; Spitzer, R. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Marcos-Nájera, R.; Huynh-Nhu, L.; Rodríguez-Muñoz, M.F.; Olivares Crespo, M.E.; Izquierdo Mendez, N. The structure of the Patient Health Questionnaire-9 in pregnant women in Spain. Midwifery 2018, 62, 36–41. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto-Balbuena, C.; Rodríguez-Muñoz, M.F.; Le, H.N. Validation of the Generalized Anxiety Disorder Screener (GAD-7) in Spanish Pregnant Women. Psicothema 2021, 33, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, R.; Huynh-Nhu, L.; Ghosh Ippen, C.; Diaz, M.A.; Urizar, G.G., Jr.; Soto, J.; Mendelson, T.; Delucchi, K.; Lieberman, A.F. Prevention of postpartum depression in Low-Income Women development of the Mamás y Bebés/Mothers and Babies Course. Cogn. Behav. Pract. 2007, 14, 70–83. [Google Scholar] [CrossRef]
- Branquinho, M.; Rodriguez-Muñoz, M.F.; Maia, B.R.; Marques, M.; Matos, M.; Osma, J.; Moreno-Peral, P.; Conejo-Cerón, S.; Fonseca, A.; Vousoura, E. Effectiveness of psychological interventions in the treatment of perinatal depression: A systematic review of systematic reviews and meta-analyses. J. Affect. Disord. 2021, 291, 294–306. [Google Scholar] [CrossRef]
- Huang, L.; Zhao, Y.; Qiang, C.; Fan, B. Is cognitive behavioral therapy a better choice for women with postnatal depression? A systematic review and meta-analysis. PLoS ONE 2018, 13, e0205243. [Google Scholar] [CrossRef] [Green Version]
- Morrell, C.J.; Sutcliffe, P.; Booth, A.; Stevens, J.; Scope, A.; Stevenson, M.; Harvey, R.; Bessey, A.; Cantrell, A.; Dennis, C.L.; et al. A systematic review, evidence synthesis and meta-analysis of quantitative and qualitative studies evaluating the clinical effectiveness, the cost-effectiveness, safety, and acceptability of interventions to prevent postnatal depression. Health Technol. Assess 2016, 20. 20, 1–414. [Google Scholar] [CrossRef] [Green Version]
- Merwin, E.; Hinton, I.; Dembling, B.; Stern, S. Shortages of rural mental health professionals. Arch. Psychiatr. Nurs. 2003, 17, 42–51. [Google Scholar] [CrossRef]
- Ng, B.; Bardwell, W.A.; Camacho, A. Depression treatment in rural California: Preliminary survey of nonpsychiatric physicians. J. Rural. Health 2002, 18, 556–562. [Google Scholar] [CrossRef]
- Danaher, B.G.; Milgrom, J.; Seeley, J.R.; Stuart, S.; Schembri CTyler, M.S.; Ericksen, J.; Lester, W.; Gemmill, A.W.; Kosty, D.B.; Lewinsohn, P. Web-Based Intervention for Postpartum Depression: Formative Research and Design of the MomMoodBooster Program. JMIR Res. Protoc. 2012, 1, e18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, R.F.; Pineda, B.S.; Barrera, A.Z.; Bunge, E.; Leykin, Y. Digital tools for prevention and treatment of depression: Lessons from the institute for international internet interventions for health. Clin. Salud. 2021, 32, 37–40. [Google Scholar] [CrossRef]
- Sawyer, M.G.; Reece, C.E.; Bowering, L.; Jeffs, D.; Sawyer, A.C.; Peters, J.D.; Mpundu-Kaambwa, C.; Clark, J.J.; McDonald, D.; Mittinty, M.N.; et al. Usage, adherence and attrition: How new mothers engage with nurse-moderated web-based intervention to support maternal and infantl health. A 9 month observational study. BMJ Open 2016, 6, e009967. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Welcome | Content Always Available | General Information |
|---|---|---|
 | Info about the Healthy Moms and Babies app FAQs about pregnancy and childbirth Infant development Videos on childbirth Configuration of the app | Breastfeeding Feeding Physical activity |
| Psychological Content | ||
| Module 1 | Module 2 | Module 3 |
| You are a mum | Psychoeducation | Feel better |
 Collects and validates your emotions. Invites you to use the app. Collects and validates your emotions. Invites you to use the app. |  Info on PPD and its symptoms. Info on PPD and its symptoms. |  Well-being, enhancing decision-making. Well-being, enhancing decision-making. |
| Module 4 | Module 5 | Module 6 |
| Thoughts | Enjoy the day | Relax |
 Cognitive restructuring, adjusting to reality, defusion strategies. Cognitive restructuring, adjusting to reality, defusion strategies. |  Behavioral activation with enjoyable activities. Time management and planning. Behavioral activation with enjoyable activities. Time management and planning. |  Relaxation audio clips for deactivation in stressful situations. Relaxation audio clips for deactivation in stressful situations. |
| Module 7 | Module 8 | Module 9 |
| Your body | Find a solution | Social support |
 Info on body and physiological changes in pregnancy. Info on body and physiological changes in pregnancy. |  Coping and problem-solving strategies. Coping and problem-solving strategies. |  Info on social support, assertive communication guidelines and support-seeking. Info on social support, assertive communication guidelines and support-seeking. |
| Module 10 | Module 11 | |
| Goodbye myths | Your baby | |
 Myths about motherhood and their demystification. Myths about motherhood and their demystification. |  Addresses the woman’s expectations of the baby and guidelines for secure attachment development. Addresses the woman’s expectations of the baby and guidelines for secure attachment development. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Segovia, N.; Rodriguez-Muñoz, M.F.; Olivares, M.E.; Izquierdo, N.; Coronado, P.; Le, H.-N. Healthy Moms and Babies Preventive Psychological Intervention Application: A Study Protocol. Int. J. Environ. Res. Public Health 2021, 18, 12485. https://doi.org/10.3390/ijerph182312485
Ruiz-Segovia N, Rodriguez-Muñoz MF, Olivares ME, Izquierdo N, Coronado P, Le H-N. Healthy Moms and Babies Preventive Psychological Intervention Application: A Study Protocol. International Journal of Environmental Research and Public Health. 2021; 18(23):12485. https://doi.org/10.3390/ijerph182312485
Chicago/Turabian StyleRuiz-Segovia, Natalia, Maria Fe Rodriguez-Muñoz, Maria Eugenia Olivares, Nuria Izquierdo, Pluvio Coronado, and Huynh-Nhu Le. 2021. "Healthy Moms and Babies Preventive Psychological Intervention Application: A Study Protocol" International Journal of Environmental Research and Public Health 18, no. 23: 12485. https://doi.org/10.3390/ijerph182312485
APA StyleRuiz-Segovia, N., Rodriguez-Muñoz, M. F., Olivares, M. E., Izquierdo, N., Coronado, P., & Le, H.-N. (2021). Healthy Moms and Babies Preventive Psychological Intervention Application: A Study Protocol. International Journal of Environmental Research and Public Health, 18(23), 12485. https://doi.org/10.3390/ijerph182312485