
A Comparative Prevalence of Birth Defects between Newborns of Immigrant and Native-Born Mothers in Taiwan: Ten Years of Population-Based Data

 ,
,
Abstract
:1. Introduction
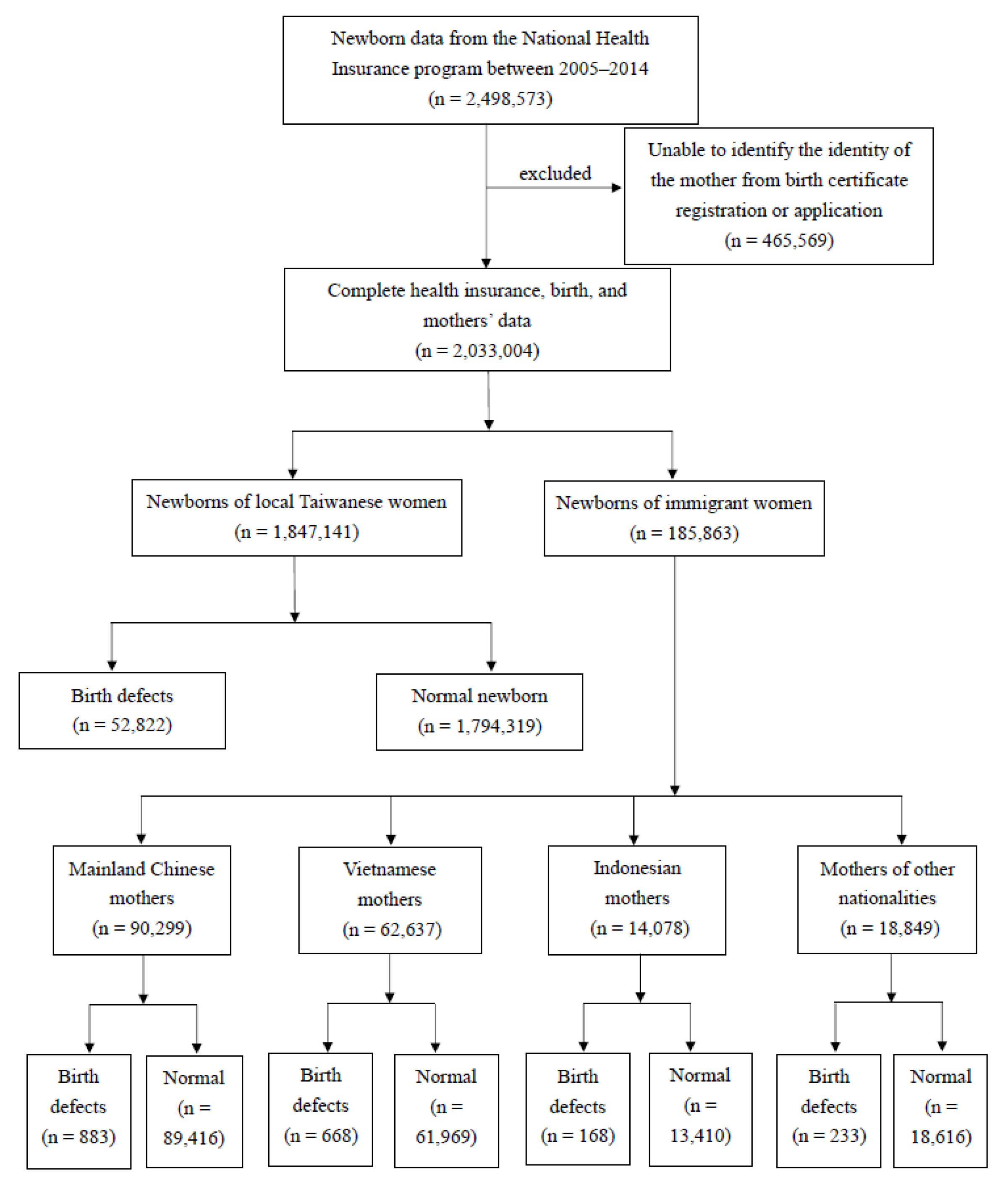
2. Methods
2.1. Data Collection
2.2. Categories of Birth Defect Diagnoses in Newborns
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lie, R.T.; Wilcox, A.J.; Skjaerven, R. Survival and reproduction among males with birth defects and risk of recurrence in their children. Obstet. Gynecol. Surv. 2001, 56, 397–398. [Google Scholar] [CrossRef]
- Grover, S.; Garg, B.; Sood, N.; Arora, K. Lethal congenital malformations in fetuses—Antenatal ultrasound or perinatal autopsy. Fetal Pediatr. Pathol. 2017, 36, 220–231. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Congenital Anomalies; WHO: Geneva, Switzerland, 2015; Available online: https://www.who.int/news-room/fact-sheets/detail/congenital-anomalies (accessed on 21 January 2021).
- Health Promotion Administration, Ministry of Health and Welfare, R.O.C. (Taiwan). 2017. Available online: https://dep.mohw.gov.tw/dos/np-1776-113.html (accessed on 21 January 2021).
- Health Promotion Administration, Ministry of Health and Welfare, R.O.C. (Taiwan). 2021. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=649&pid=13646 (accessed on 15 May 2021).
- Steinlin, M. Cerebellar disorders in childhood: Cognitive problems. Cerebellum 2008, 7, 607–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Namankany, A.; Alhubaishi, A. Effects of cleft lip and palate on childrens psychological health: A systematic review. J. Taibah Univ. Medical Sci. 2018, 13, 311–318. [Google Scholar]
- Borge, A.I.; Wefring, K.; Lie, K.; Nordhagen, R. Chronic illness and aggressive behaviour: A population-based study of 4-year-olds. Eur. J. Dev. Psychol. 2004, 1, 19–29. [Google Scholar] [CrossRef]
- Department of Household Registration, Ministry of the Interior, R.O.C. 2015. Available online: https://www.ris.gov.tw/app/portal/346 (accessed on 21 January 2021).
- Canfield, M.A.; Mai, C.T.; Wang, Y.; O’Halloran, A.; Marengo, L.K.; Olney, R.S.; Borger, C.L.; Rutkowski, R.; Fornoff, J.; Irwin, N.; et al. The association between race/ethnicity and major birth defects in the United States, 1999–2007. Am. J. Public Health. 2014, 104, e14–e23. [Google Scholar] [CrossRef]
- Hsia, H. The subjectivation of marriage migrants in Taiwan: The insider’s perspectives. Learning from the Ground Up; Palgrave Macmillan: New York, NY, USA, 2010; pp. 101–118. [Google Scholar]
- Yang, H.J.; Kuo, Y.J.; Wang, L.; Yang, C.Y. Culture, parenting, and child behavioral problems: A comparative study of cross-cultural immigrant families and native-born families in Taiwan. Transcult. Psychiatry 2014, 51, 526–544. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Huang, X.; Wang, B.; Zhang, Y.; Rongkavilit, C.; Zeng, D.; Jiang, Y.; Wei, B.; Sanjay, C.; McGrath, E. Epidemiology of birth defects based on surveillance data from 2011–2015 in Guangxi, China: Comparison across five major ethnic groups. BMC Public Health 2018, 18, 1008. [Google Scholar] [CrossRef]
- Egede, L.E. Race, ethnicity, culture, and disparities in health care. J. Gen. Intern. Med. 2006, 21, 667–669. [Google Scholar] [CrossRef]
- Schumann, B.; Lundevaller, E.H.; Karlsson, L. Weather extremes and perinatal mortality—Seasonal and ethnic differences in northern Sweden, 1800–1895. PLoS ONE 2019, 14, e0223538. [Google Scholar] [CrossRef]
- Agha, M.M.; Glazier, R.H.; Moineddin, R. Birth defects among immigrants: Impact of exposure to a new environment, a 20 year population-based study. J. Public Health Epidemiol. 2020, 12, 238–245. [Google Scholar]
- Anthony, S.; Kateman, H.; Brand, R.; Ouden, A.L.; Dorrepaal, C.A.; Van Der Pal-De Bruin, K.M.; Buitendijk, S.E. Ethnic differences in congenital malformations in the Netherlands: Analyses of a 5-year birth cohort. Paediatr. Perinat. Epidemiol. 2005, 19, 135–144. [Google Scholar] [CrossRef]
- Huang, S.; Yang, H. Is there a healthy immigrant effect among women through transnational marriage? Results from immigrant women from Southeast Asian countries in Taiwan. J. Immigr. Minor. Health. 2018, 20, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Hashmi, S.S.; Waller, D.K.; Langlois, P.; Canfield, M.; Hecht, J.T. Prevalence of nonsyndromic oral clefts in Texas: 1995–1999. Am. J. Med. Genet. A 2005, 134A, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Druschel, C.; Lin, S. Maternal birthplace and major congenital malformations among New York Hispanics. Birth Defects Res. Part A Clin. Mol. Teratol. 2006, 76, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.L.; Huang, I.C.; Tsai, H.J.; Wang, H.P. Comparisons of fertility rate and birth quality between native and foreign-born women in Taiwan. J. Soc. Sci. Phil. 2001, 24, 83–120. (In Chinese) [Google Scholar]
- European Surveillance of Congenital Anomalies (EUROCAT): Prevalence Tables 2008–2012. Available online: http://www.eurocat-network.eu/accessprevalencedata/prevalencetables (accessed on 21 January 2021).
- Bellizzi, S.; Ali, M.M.; Abalos, E.; Betran, A.P.; Kapila, J.; Pileggi-Castro, C.; Vogel, J.P.; Merialdi, M. Are hypertensive disorders in pregnancy associated with congenital malformations in offspring? Evidence from the WHO Multicountry cross sectional survey on maternal and newborn health. BMC Pregnancy Childbirth 2016, 16, 198. [Google Scholar] [CrossRef] [Green Version]
- Karimi, P.; Kamali, E.; Mousavi, S.M.; Karahmadi, M. Environmental factors influencing the risk of autism. J. Res. Med. Sci. Off. J. Isfahan Univ Med. Sci. 2017, 22, 27. [Google Scholar]
- Lupo, P.J.; Mitchell, L.E.; Jenkins, M.M. Genome-wide association studies of structural birth defects: A review and commentary. Birth Defects Res. 2019, 111, 1329–1342. [Google Scholar] [CrossRef]
- Padula, A.M.; Yang, W.; Schultz, K.; Lee, C.; Lurmann, F.; Hammond, S.K.; Shaw, G.M. Gene–environment interactions between air pollution and biotransformation enzymes and risk of birth defects. Birth Defects Res. 2021, 113, 676–686. [Google Scholar] [CrossRef]
- Mekonnen, D.; MollaTaye; Worku, W. Congenital anomalies among newborn babies in Felege-Hiwot Comprehensive specialized referral hospital, Bahir Dar, Ethiopia. Sci. Rep. 2021, 11, 11027. [Google Scholar] [CrossRef]
- Liu, X.; Nie, Z.; Chen, J.; Guo, X.; Ou, Y.; Chen, G.; Mai, J.; Gong, W.; Wu, Y.; Gao, X.; et al. Does maternal environmental tobacco smoke interact with social-demographics and environmental factors on congenital heart defects? Environ. Pollut. 2018, 234, 214–222. [Google Scholar] [CrossRef]
- Yao, C.A.; Swanson, J.; Chanson, D.; Taro, T.B.; Gura, B.; Figueiredo, J.C.; Wipfli, H.; Hatcher, K.; Vanderburg, R.; Magee, W.P., III. Barriers to reconstructive surgery in low-and middle-income countries: A cross-sectional study of 453 cleft lip and cleft palate patients in Vietnam. Plast. Reconstr. Surg. 2016, 138, 887e–895e. [Google Scholar] [CrossRef] [PubMed]
- Agot, G.N.; Mweu, M.M.; Wang’ombe, J.K. Risk factors for major external structural birth defects among children in Kiambu County, Kenya: A case-control study. F1000Research 2021, 10, 59. [Google Scholar] [CrossRef] [PubMed]
- Souza, S.D.; Nampo, F.K.; Pestana, C.R. Major birth defects in the Brazilian side of the triple border: A population-based cross-sectional study. Arch. Public Health 2020, 78, 61. [Google Scholar] [CrossRef]
- Li, Z.; Chen, Y.; Qiu, L.; Chen, D.; Hu, C.; Xu, J.; Zhang, X. Prevalence, types, and malformations in congenital anomalies of the kidney and urinary tract in newborns: A retrospective hospital-based study. Ital. J. Pediatr. 2019, 45, 50. [Google Scholar] [CrossRef]
- Health Promotion Administration, Ministry of Health and Welfare, R.O.C (Taiwan). 2020. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=4141&pid=12969 (accessed on 21 January 2021).
- Chen, L.; Chiou, J.; Huang, J.; Su, P.; Chen, J. Birth defects in Taiwan: A 10-year nationwide population-based, cohort study. J. Formos. Med. Assoc. 2020, 119, 553–559. [Google Scholar] [CrossRef]
- Basu, M.; Zhu, J.Y.; LaHaye, S.; Majumdar, U.; Jiao, K.; Han, Z.; Garg, V. Epigenetic mechanisms underlying maternal diabetes-associated risk of congenital heart disease. JCI Insight 2017, 2, e95085. [Google Scholar] [CrossRef] [Green Version]
- Øyen, N.; Diaz, L.J.; Leirgul, E.; Boyd, H.A.; Priest, J.; Mathiesen, E.R.; Quertermous, T.; Wohlfahrt, J.; Melbye, M. Prepregnancy diabetes and offspring risk of congenital heart disease: A nationwide cohort study. Circulation 2016, 133, 2243–2253. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.B.; Florez, J.C. Genetics of diabetes mellitus and diabetes complications. Nat. Rev. Nephrol. 2020, 16, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Dye, T.D.; Li, D. Effects of pre-gestational diabetes mellitus and gestational diabetes mellitus on macrosomia and birth defects in upstate New York. Diabetes Res. Clin. Pract. 2019, 155, 107811. [Google Scholar] [CrossRef]
- Lopez, K.N.; Nembhard, W.N.; Wang, Y.; Liu, G.; Kucik, J.E.; Copeland, G.; Gilboa, S.M.; Kirby, R.S.; Canfield, M. Birth defect survival for Hispanic subgroups. Birth Defects Res. 2018, 110, 352–363. [Google Scholar] [CrossRef]
- Su, F.; Lu, M.; Yu, S.; Yang, C.; Yang, C.; Tseng, S.; Yan, Y. Increasing trend in the prevalence of gestational diabetes mellitus in Taiwan. J. Diabetes Investig. 2021, 12, 2080–2088. [Google Scholar] [CrossRef] [PubMed]
- Tain, Y.L.; Luh, H.; Lin, C.Y.; Hsu, C.N. Incidence and risks of congenital anomalies of kidney and urinary tract in newborns: A population-based case-control study in Taiwan. Medicine 2016, 95, e2659. [Google Scholar] [CrossRef] [PubMed]
- Parnell, A.S.; Correa, A.; Reece, E.A. Pre-pregnancy obesity as a modifier of gestational diabetes and birth defects associations: A systematic review. Matern Child Health J. 2017, 21, 1105–1120. [Google Scholar] [CrossRef] [PubMed]
- Miao, Q.; Dunn, S.; Wen, S.W.; Lougheed, J.; Reszel, J.; Venegas, C.L.; Walker, M. Neighbourhood maternal socioeconomic status indicators and risk of congenital heart disease. BMC Pregnancy Childbirth 2021, 21, 72. [Google Scholar] [CrossRef]
- Wu, M.; Chen, H.; Lu, C.; Wang, J.; Huang, S.; Huang, S. Prevalence of congenital heart disease at live birth in Taiwan. J. Pediatr. 2010, 156, 782–785. [Google Scholar] [CrossRef]
- Department of Household Registration, Ministry of the Interior, R.O.C. 2018. Available online: https://ws.moi.gov.tw/001/Upload/OldFile/news_file/107%E5%B9%B4%E6%96%B0%E4%BD%8F%E6%B0%91%E7%94%9F%E6%B4%BB%E9%9C%80%E6%B1%82%E8%AA%BF%E6%9F%A5%E6%91%98%E8%A6%81.pdf (accessed on 21 January 2021). (In Chinese)
- Kim, Y.Y. Cross-Cultural Adaptation. Oxford Research Encyclopedia of Communication. 2017. Available online: https://oxfordre.com/communication/view/10.1093/acrefore/9780190228613.001.0001/acrefore-9780190228613-e-21 (accessed on 21 January 2021).
- Guendelman, S.; English, P.B. Effect of United States Residence on Birth Outcomes among Mexican Immigrants: An Exploratory Study. Am. J. Epidemiol. 1995, 142 (Suppl. 9), S30–S38. [Google Scholar] [CrossRef]
- Lien, M.H.; Huang, S.S.; Yang, H.J. A pathway to negative acculturation: Marital maladjustment mediates the relationship between the length of residency and depressive symptoms in immigrant women in Taiwan. BMC Women’s Health 2021, 21, 190. [Google Scholar] [CrossRef] [PubMed]
- Kwak, K. Age and gender variations in healthy immigrant effect: A population study of immigrant well-being in Canada. J. Int. Migr. Integr. 2018, 19, 413–437. [Google Scholar] [CrossRef]
- Urquia, M.; Frank, J.; Moineddin, R.; Glazier, R. Immigrants’ duration of residence and adverse birth outcomes: A population-based study. BJOG Int. J. Obstet. Gynaecol. 2010, 117, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Nationality | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Taiwan (n = 1,847,141) | Mainland China (n = 90,299) | Vietnam (n = 62,637) | Indonesia (n = 14,078) | Others (n = 18,849) | ||||||
| n | % | n | % | n | % | n | % | n | % | |
| Live births and fetal deaths | ||||||||||
| Live births | 1,826,327 | 98.88 | 89,655 | 99.29 | 62,164 | 99.22 | 13,944 | 99.01 | 18,632 | 98.83 |
| Stillbirths | 20,814 | 1.13 | 644 | 0.72 | 473 | 0.78 | 134 | 1.00 | 217 | 1.17 |
| Fetal gender | ||||||||||
| Male | 960,578 | 52.01 | 47,318 | 52.41 | 32,757 | 52.12 | 7397 | 52.57 | 9760 | 51.81 |
| Female | 885,907 | 47.96 | 42,956 | 47.57 | 29,867 | 47.87 | 6676 | 47.39 | 9086 | 48.18 |
| Unknown | 656 | 0.04 | 25 | 0.03 | 13 | 0.02 | 5 | 0.03 | 3 | 0.02 |
| Single or multiple births | ||||||||||
| Single | 1,789,370 | 96.88 | 87,215 | 96.54 | 61,467 | 98.07 | 13,827 | 98.24 | 18,279 | 96.94 |
| Multiple | 57,771 | 3.12 | 3084 | 3.46 | 1170 | 1.94 | 251 | 1.77 | 570 | 3.06 |
| Birth location | ||||||||||
| Hospital | 1,303,655 | 70.56 | 61,039 | 67.78 | 36,010 | 58.31 | 8140 | 58.44 | 13,093 | 69.76 |
| Clinic | 540,754 | 29.30 | 29,178 | 32.13 | 26,536 | 41.56 | 5843 | 40.83 | 5704 | 29.97 |
| Other | 2732 | 0.15 | 82 | 0.09 | 91 | 0.14 | 95 | 0.74 | 52 | 0.28 |
| Gestational age | ||||||||||
| <24 weeks | 13,477 | 0.73 | 346 | 0.39 | 245 | 0.42 | 62 | 0.49 | 115 | 0.63 |
| 24–36 weeks | 171,636 | 9.29 | 6,193 | 6.90 | 4599 | 7.57 | 1061 | 7.58 | 1615 | 8.57 |
| 37–40 weeks | 1,607,241 | 87.01 | 79,287 | 87.85 | 55,136 | 88.08 | 12,313 | 87.49 | 16,298 | 86.47 |
| ≥41 weeks | 54,787 | 2.98 | 4473 | 4.87 | 2657 | 3.95 | 642 | 4.46 | 821 | 4.33 |
| Age of mother | ||||||||||
| <20 | 27,112 | 1.48 | 25 | 0.03 | 1,52 | 1.58 | 233 | 1.56 | 68 | 0.36 |
| 20–34 | 1,452,836 | 78.74 | 79,222 | 87.47 | 58,204 | 92.04 | 12,300 | 86.21 | 14,310 | 75.48 |
| ≥35 | 367,193 | 19.79 | 11,052 | 12.51 | 3181 | 6.39 | 1545 | 12.23 | 4471 | 24.17 |
| Maternal diseases (from health insurance data) | ||||||||||
| Hypertension | 41,379 | 2.23 | 1698 | 1.89 | 1101 | 1.74 | 272 | 1.97 | 354 | 1.88 |
| Cardiovascular disease | 4041 | 0.22 | 328 | 0.37 | 165 | 0.28 | 52 | 0.38 | 58 | 0.31 |
| Renal disease | 6515 | 0.36 | 308 | 0.35 | 205 | 0.33 | 45 | 0.33 | 88 | 0.47 |
| Genitourinary infection | 116,062 | 6.27 | 5936 | 6.59 | 4111 | 6.64 | 870 | 6.29 | 1212 | 6.48 |
| General infection | 23,145 | 1.26 | 1211 | 1.35 | 869 | 1.41 | 193 | 1.34 | 248 | 1.32 |
| Anemia | 104,624 | 5.64 | 4339 | 4.81 | 3068 | 4.99 | 723 | 5.25 | 872 | 4.68 |
| Drug abuse/dependence | 4407 | 0.24 | 446 | 0.49 | 265 | 0.40 | 64 | 0.45 | 69 | 0.37 |
| Mental disorder | 48,452 | 2.62 | 3770 | 4.19 | 2494 | 3.88 | 557 | 3.98 | 725 | 3.87 |
| Alcohol-related conditions | 871 | 0.05 | 103 | 0.12 | 46 | 0.06 | 14 | 0.10 | 18 | 0.10 |
| DM | ||||||||||
| GDM | 218,327 | 11.79 | 6153 | 6.90 | 3783 | 6.77 | 680 | 5.19 | 1434 | 7.73 |
| Type 2 DM (within 2 years) | 8764 | 0.47 | 203 | 0.23 | 127 | 0.22 | 29 | 0.22 | 68 | 0.37 |
| Type 2 DM (2–5 years) | 13,193 | 0.71 | 208 | 0.24 | 112 | 0.24 | 33 | 0.27 | 70 | 0.39 |
| Year | Nationality of Mother | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Taiwan | Mainland China | Vietnam | Indonesia | Others | |||||||||||
| Total Births | Number of Newborns with Birth Defects | % | Total Births | Number of Newborns with Birth Defects | % | Total Births | Number of Newborns with Birth Defects | % | Total Births | Number of Newborns with Birth Defects | % | Total Births | Number of Newborns with Birth Defects | % | |
| 2005 | 181,326 | 5298 | 2.92 | 10,169 | 124 | 1.22 | 12,985 | 148 | 1.14 | 2301 | 25 | 1.09 | 2299 | 26 | 1.13 |
| 2006 | 182,361 | 5449 | 2.99 | 10,426 | 99 | 0.95 | 10,211 | 105 | 1.03 | 1948 | 18 | 0.92 | 2296 | 31 | 1.35 |
| 2007 | 183,992 | 5453 | 2.96 | 10,032 | 89 | 0.89 | 7805 | 84 | 1.08 | 1732 | 27 | 1.56 | 2007 | 23 | 1.15 |
| 2008 | 179,013 | 5290 | 2.96 | 9607 | 94 | 0.98 | 6559 | 57 | 0.87 | 1488 | 13 | 0.87 | 1885 | 19 | 1.01 |
| 2009 | 177,425 | 5220 | 2.94 | 8754 | 65 | 0.74 | 5380 | 58 | 1.08 | 1281 | 16 | 1.25 | 1735 | 26 | 1.50 |
| 2010 | 153,795 | 4379 | 2.85 | 7921 | 78 | 0.98 | 4094 | 39 | 0.95 | 1122 | 17 | 1.52 | 1575 | 13 | 0.83 |
| 2011 | 185,255 | 5174 | 2.79 | 8608 | 82 | 0.95 | 4134 | 42 | 1.02 | 1085 | 7 | 0.65 | 1626 | 23 | 1.41 |
| 2012 | 219,656 | 5616 | 2.56 | 9654 | 109 | 1.13 | 4618 | 46 | 1.00 | 1186 | 17 | 1.43 | 1929 | 24 | 1.24 |
| 2013 | 183,919 | 5340 | 2.90 | 7453 | 68 | 0.91 | 3456 | 48 | 1.39 | 992 | 17 | 1.71 | 1675 | 31 | 1.85 |
| 2014 | 200,399 | 5603 | 2.80 | 7675 | 75 | 0.98 | 3395 | 41 | 1.21 | 943 | 11 | 1.17 | 1822 | 17 | 0.93 |
| Total | 1,847,141 | 52,822 | 2.86 | 90,299 | 883 | 0.98 | 62,637 | 668 | 1.07 | 14,078 | 168 | 1.19 | 18,849 | 233 | 1.24 |
| Category | Taiwan | Mainland China | Vietnam | Indonesia | Others | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Newborns with Defects | Prevalence Rate (%) | Number of Newborns with Defects | Prevalence Rate (%) | Number of Newborns with Defects | Prevalence Rate (%) | Number of Newborns with Defects | Prevalence Rate (%) | Number of Newborns with Defects | Prevalence Rate (%) | |
| Nervous system | 2850 | 0.15 | 49 | 0.05 * | 49 | 0.08 * | 12 | 0.09 * | 20 | 0.11 |
| Eyes, ears, face, and neck | 1535 | 0.08 | 32 | 0.04 * | 22 | 0.04 * | 6 | 0.04 | 13 | 0.07 |
| Cleft lip and cleft palate | 3582 | 0.19 | 123 | 0.14 * | 113 | 0.18 | 22 | 0.16 | 26 | 0.14 |
| Circulatory system | 16,922 | 0.92 | 136 | 0.15 * | 125 | 0.20 * | 36 | 0.26 * | 50 | 0.27 * |
| Respiratory system | 5261 | 0.28 | 46 | 0.05 * | 38 | 0.03 * | 15 | 0.1 1* | 9 | 0.05 * |
| Digestive system | 5811 | 0.31 | 96 | 0.11 * | 69 | 0.11 * | 17 | 0.12 * | 30 | 0.16 * |
| Genital, urinary organs | 10,021 | 0.54 | 163 | 0.18 * | 103 | 0.16 * | 29 | 0.21 * | 33 | 0.18 * |
| Musculoskeletal system | 8758 | 0.47 | 214 | 0.24 * | 148 | 0.24 * | 59 | 0.42 | 46 | 0.24 * |
| Chromosomal abnormalities | 2769 | 0.15 | 80 | 0.09 * | 48 | 0.05 * | 13 | 0.09 | 29 | 0.15 |
| Age of Mother | Taiwan | Mainland China | Vietnam | Indonesia | Others | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Births | Number of Newborns with Defects | % | Total Birth | Number of Newborns with Defects | % | Total Birth | Number of Newborns with Defects | % | Total Birth | Number of Newborns with Defects | % | Total Birth | Number of Newborns with Defects | % | |
| ≤34 years old | 1,479,948 | 40,804 | 2.76 | 79,247 | 734 | 0.93 | 59,456 | 627 | 1.05 | 12,533 | 140 | 1.12 | 14,379 | 171 | 1.19 |
| ≥35 years old | 367,193 | 12,018 | 3.27 | 1052 | 149 | 1.35 | 3181 | 41 | 1.29 | 1545 | 28 | 1.81 | 4470 | 62 | 1.39 |
| Adjusted Odds Ratios § | |||||
|---|---|---|---|---|---|
| Taiwan | Mainland China | Vietnam | Indonesia | Others | |
| All defects | Reference | 0.37 (0.35–0.39) | 0.41 (0.38–0.44) | 0.47 (0.40–0.54) | 0.43 (0.38–0.49) |
| Nervous system | Reference | 0.43 (0.32–0.57) | 0.58 (0.43–0.77) | 0.65 (0.37–1.15) | 0.71 (0.46–1.10) |
| Eyes, ears, face, neck system | Reference | 0.45 (0.30–0.69) | 0.54 (0.24–1.21) | 0.81 (0.47–1.41) | 0.45 (0.30–0.69) |
| Cleft lip and cleft palate | Reference | 1.00 (0.83–1.21) | 0.86 (0.56–1.31) | 0.74 (0.50–1.08) | 1.00 (0.83–1.21) |
| Circulatory system | Reference | 0.25 (0.21–0.30) | 0.32 (0.23–0.45) | 0.30 (0.23–0.40) | 0.25 (0.21–0.30) |
| Respiratory system | Reference | 0.23 (0.17–0.31) | 0.39 (0.23–0.65) | 0.17 (0.09–0.32) | 0.23 (0.17–0.31) |
| Digestive system | Reference | 0.37 (0.29–0.46) | 0.41 (0.25–0.66) | 0.53 (0.37–0.76) | 0.37 (0.29–0.46) |
| Genital, urinary organs | Reference | 0.33 (0.28–0.41) | 0.44 (0.30–0.63) | 0.33 (0.23–0.47) | 0.33 (0.28–0.41) |
| Musculoskeletal system | Reference | 0.55 (0.47–0.65) | 0.50 (0.34–0.72) | 0.53 (0.39–0.70) | 0.55 (0.47–0.65) |
| Chromosomal abnormalities | Reference | 0.90 (0.67–1.20) | 0.94 (0.54–1.65) | 0.95 (0.64–1.41) | 0.90 (0.67–1.20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-J.; Chiou, J.-Y.; Huang, J.-Y.; Su, P.-H.; Chen, J.-Y.; Yang, H.-J. A Comparative Prevalence of Birth Defects between Newborns of Immigrant and Native-Born Mothers in Taiwan: Ten Years of Population-Based Data. Int. J. Environ. Res. Public Health 2021, 18, 12530. https://doi.org/10.3390/ijerph182312530
Lin Y-J, Chiou J-Y, Huang J-Y, Su P-H, Chen J-Y, Yang H-J. A Comparative Prevalence of Birth Defects between Newborns of Immigrant and Native-Born Mothers in Taiwan: Ten Years of Population-Based Data. International Journal of Environmental Research and Public Health. 2021; 18(23):12530. https://doi.org/10.3390/ijerph182312530
Chicago/Turabian StyleLin, Yu-Jung, Jeng-Yuan Chiou, Jing-Yang Huang, Pen-Hua Su, Jia-Yuh Chen, and Hao-Jan Yang. 2021. "A Comparative Prevalence of Birth Defects between Newborns of Immigrant and Native-Born Mothers in Taiwan: Ten Years of Population-Based Data" International Journal of Environmental Research and Public Health 18, no. 23: 12530. https://doi.org/10.3390/ijerph182312530
APA StyleLin, Y.-J., Chiou, J.-Y., Huang, J.-Y., Su, P.-H., Chen, J.-Y., & Yang, H.-J. (2021). A Comparative Prevalence of Birth Defects between Newborns of Immigrant and Native-Born Mothers in Taiwan: Ten Years of Population-Based Data. International Journal of Environmental Research and Public Health, 18(23), 12530. https://doi.org/10.3390/ijerph182312530