
Knowledge into the Practice against COVID-19: A Cross-Sectional Study from Ghana

 ,
,  ,
,  ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of the Questionnaire
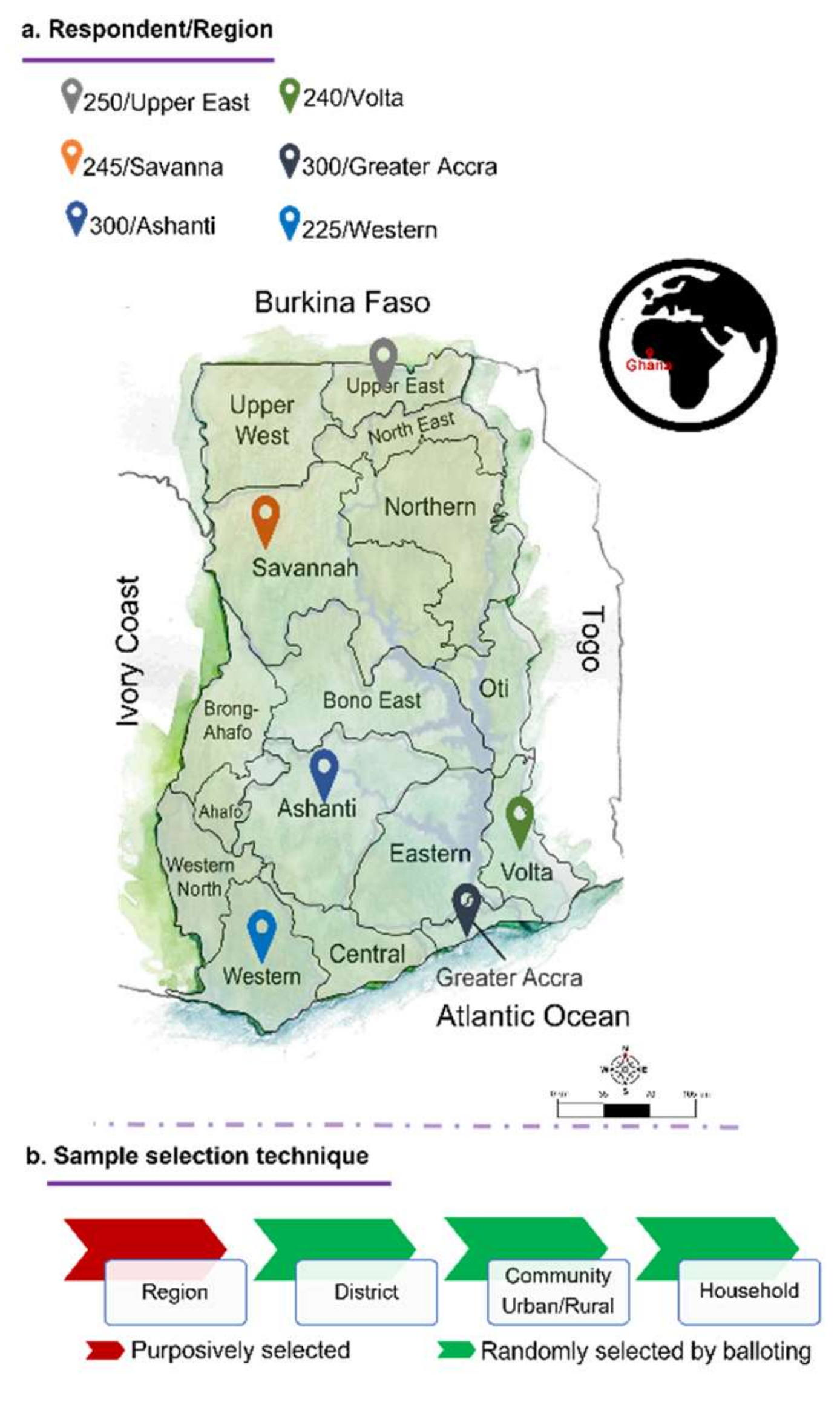
2.2. Study Design and Data Collection
2.3. Statistical Procedure
3. Results
3.1. Descriptive Statistics
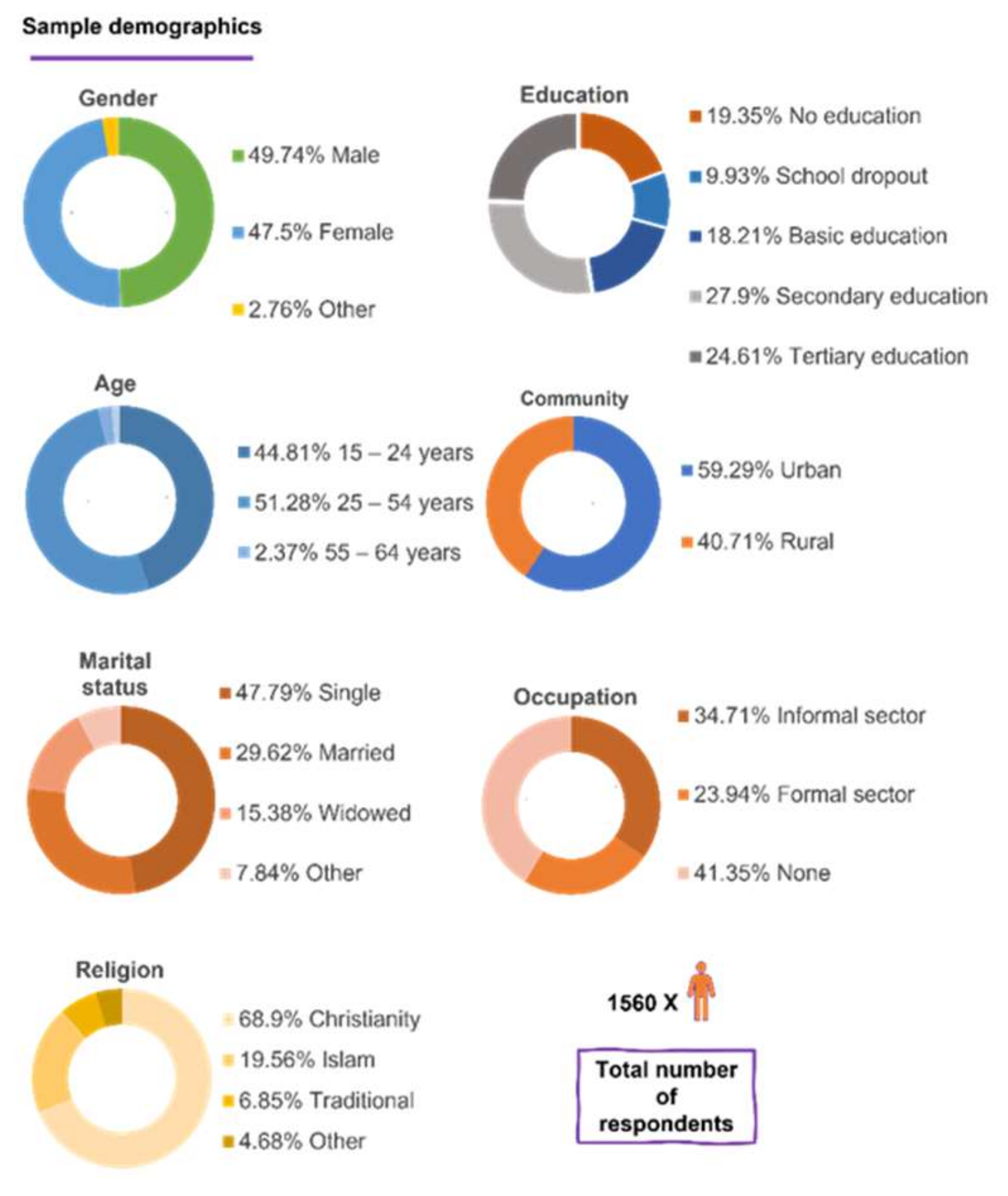
3.1.1. Socio-Demographic Indicators
3.1.2. Data Obtained from the Knowledge Section
3.1.3. Data Obtained from the Practice Section
3.2. Linear Multiple Regression Analysis
3.2.1. Influences on the Knowledge of COVID-19
3.2.2. Knowledge onto Practice
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mbow, M.; Lell, B.; Jochems, S.P.; Cisse, B.; Mboup, S.; Dewals, B.G.; Jaye, A.; Dieye, A.; Yazdanbakhsh, M. COVID-19 in Africa: Dampening the storm? Science 2020, 369, 624–626. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.; Pullano, G.; Pinotti, F.; Valdano, E.; Poletto, C.; Boëlle, P.-Y.; D’Ortenzio, E.; Yazdanpanah, Y.; Eholie, S.P.; Altmann, M.; et al. Preparedness and vulnerability of African countries against importations of COVID-19: A modelling study. Lancet 2020, 395, 871–877. [Google Scholar] [CrossRef] [Green Version]
- Kapata, N.; Ihekweazu, C.; Ntoumi, F.; Raji, T.; Chanda-Kapata, P.; Mwaba, P.; Mukonka, V.; Bates, M.; Tembo, J.; Corman, V.; et al. Is Africa prepared for tackling the COVID-19 (SARS-CoV-2) epidemic. Lessons from past outbreaks, ongoing pan-African public health efforts, and implications for the future. Int. J. Infect. Dis. 2020, 93, 233–236. [Google Scholar] [CrossRef]
- Adams, J.; MacKenzie, M.J.; Amegah, A.K.; Ezeh, A.; Gadanya, M.A.; Omigbodun, A.; Sarki, A.M.; Thistle, P.; Ziraba, A.K.; Stranges, S.; et al. The conundrum of Low COVID-19 mortality burden in sub-Saharan Africa: Myth or reality? Glob. Health Sci. Pract. 2021, 9, 433–443. [Google Scholar] [CrossRef]
- Sagar, M.; Reifler, K.; Rossi, M.; Miller, N.S.; Sinha, P.; White, L.F.; Mizgerd, J.P. Recent endemic coronavirus infection is associated with less-severe COVID-19. J. Clin. Investig. 2021, 131, e143380. [Google Scholar] [CrossRef]
- Schröder, M.; Bossert, A.; Kersting, M.; Aeffner, S.; Coetzee, J.; Timme, M.; Schlüter, J. COVID-19 in South Africa: Outbreak despite interventions. Sci. Rep. 2021, 11, 4956. [Google Scholar] [CrossRef] [PubMed]
- Senghore, M.; Savi, M.K.; Gnangnon, B.; Hanage, W.P.; Okeke, I.N. Leveraging Africa’s preparedness towards the next phase of the COVID-19 pandemic. Lancet Glob. Health 2020, 8, e884–e885. [Google Scholar] [CrossRef]
- Bonful, H.A.; Addo-Lartey, A.; Aheto, J.M.K.; Ganle, J.K.; Sarfo, B.; Aryeetey, R. Limiting spread of COVID-19 in Ghana: Compliance audit of selected transportation stations in the Greater Accra region of Ghana. PLoS ONE 2020, 15, e0238971. [Google Scholar] [CrossRef]
- Gaye, B.; Khoury, S.; Cene, C.W.; Kingue, S.; N’Guetta, R.; Lassale, C.; Baldé, D.; Diop, I.B.; Dowd, J.B.; Mills, M.C.; et al. Socio-demographic and epidemiological consideration of Africa’s COVID-19 response: What is the possible pandemic course? Nat. Med. 2020, 26, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Press Releases|COVID-19|Ghana. Available online: https://www.ghanahealthservice.org/covid19/press-releases.php (accessed on 24 September 2021).
- Why Is Europe Returning to the Dark Days of COVID? The ASEAN Post. Available online: https://theaseanpost.com/article/why-europe-returning-dark-days-covid (accessed on 23 November 2021).
- Lund-Thomsen, P.; Ramirez, J. Beyond Compliance and Cooperation? CBS: New York, NY, USA, 2020. [Google Scholar]
- Rahman, A.; Zaman, N.; Asyhari, A.T.; Al-Turjman, F.; Alam Bhuiyan, Z.; Zolkipli, M. Data-driven dynamic clustering framework for mitigating the adverse economic impact of Covid-19 lockdown practices. Sustain. Cities Soc. 2020, 62, 102372. [Google Scholar] [CrossRef]
- Barrett, G. The Future of Legal Europe: Will We Trust in It? Springer Nature: Basingstoke, UK, 2021. [Google Scholar]
- Bonell, C.; Michie, S.; Reicher, S.; West, R.; Bear, L.; Yardley, L.; Curtis, V.; Amlôt, R.; Rubin, G.J. Harnessing behavioural science in public health campaigns to maintain ‘social distancing’ in response to the COVID-19 pandemic: Key principles. J. Epidemiol. Community Health 2020, 74, 617–619. [Google Scholar] [PubMed]
- Fox, J.; Weisberg, S. An R Companion to Applied Regression; Sage Publications: New York, NY, USA, 2018. [Google Scholar]
- Canty, A.; Ripley, B.D. boot: Bootstrap R (S-Plus) Functions. R Package Version 1.3-28. 2021. Available online: https://cran.r-project.org/web/packages/boot/citation.html (accessed on 6 December 2021).
- Yapi, R.; Houngbedji, C.; N’Guessan, D.; Dindé, A.; Sanhoun, A.; Amin, A.; Gboko, K.; Heitz-Tokpa, K.; Fokou, G.; Bonfoh, B. Knowledge, attitudes, and practices (KAP) regarding the COVID-19 outbreak in Côte d’Ivoire: Understanding the Non-compliance of populations with Non-pharmaceutical interventions. Int. J. Environ. Res. Public Health 2021, 18, 4757. [Google Scholar] [CrossRef]
- Mendy, P.A.; Jawo, E.; Jallow, B.J.; Ceesay, B.; Mendy, S.A.; Camara, B.; Ndaw, M. Knowledge, Attitude and Practice of Gambians towards the Novel Coronavirus (COVID-19) Pandemic in The Gambia: A cross-sectional study. Afr. J. Health Sci. 2021, 34, 134–147. [Google Scholar]
- Ssebuufu, R.; Sikakulya, F.K.; Mambo, S.B.; Wasingya, L.; Nganza, S.K.; Ibrahim, B.; Kyamanywa, P. Knowledge, attitude, and Self-Reported practice toward measures for prevention of the spread of COVID-19 among ugandans: A nationwide online Cross-Sectional survey. Front. Public Health 2020, 8, 618731. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Nelson, A.; Lopez, A.L.; Sack, D.A. Updated Global Burden of Cholera in Endemic Countries. PLoS Negl. Trop. Dis. 2015, 9, e0003832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besser, A.; Flett, G.L.; Nepon, T.; Zeigler-Hill, V. Personality, cognition, and adaptability to the COVID-19 pandemic: Associations with loneliness, distress, and positive and negative mood states. Int. J. Ment. Health Addict. 2020, 1–25. [Google Scholar] [CrossRef]
- Nettleton, S. The Sociology of Health and Illness; John Wiley & Sons: Hoboken, NJ, USA, 2020. [Google Scholar]
- Al Ahdab, S. A cross-sectional survey of knowledge, attitude and practice (KAP) towards COVID-19 pandemic among the Syrian residents. BMC Public Health 2021, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Moon, S.J.; Ndombi, G.O.; Kim, K.-N.; Berhe, H.; Nam, E.W. COVID-19 Perception, knowledge, and preventive practice: Comparison between South Korea, Ethiopia, and democratic republic of Congo. Afr. J. Reprod. Health 2020, 24, 66–77. [Google Scholar]
- Abdelhafiz, A.S.; Mohammed, Z.; Ibrahim, M.E.; Ziady, H.H.; Alorabi, M.; Ayyad, M.; Sultan, E.A. Knowledge, Perceptions, and Attitude of Egyptians Towards the Novel Coronavirus Disease (COVID-19). J Community Health 2020, 45, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Ghana Living Wage Individual|2021 Data|2022 Forecast|2015–2020 Historical. Available online: https://tradingeconomics.com/ghana/living-wage-individual (accessed on 21 November 2021).
- Dzisi, E.K.J.; Dei, O.A. Adherence to social distancing and wearing of masks within public transportation during the COVID 19 pandemic. Transp. Res. Interdiscip. Perspect. 2020, 7, 100191. [Google Scholar] [CrossRef]
- Zhang, J.; Nonvignon, J.; Mao, W. How Well is Ghana—With One of the Best Testing Capacities in Africa—Responding to COVID-19? Brook Institution. 2020. Available online: https://www.brookings.edu/blog/future-development/2020/07/28/how-well-is-ghana-with-one-of-the-best-testing-capacities-in-africa-responding-to-covid-19/ (accessed on 6 December 2021).
- Saba, C.K.S. COVID-19: Implications for Food, Water, Hygiene, Sanitation, and Environmental Safety in Africa: A Case Study in Ghana. 2020. Available online: https://www.preprints.org/manuscript/202005.0369/v1 (accessed on 21 November 2021).
- Okyere, I.; Chuku, E.O.; Ekumah, B.; Angnuureng, D.B.; Boakye-Appiah, J.K.; Mills, D.J.; Babanawo, R.; Asare, N.K.; Aheto, D.W.; Crawford, B. Physical distancing and risk of COVID-19 in small-scale fisheries: A remote sensing assessment in coastal Ghana. Sci. Rep. 2020, 10, 22407. [Google Scholar] [CrossRef]
- Van der Bijl, J.; van Poelgeest-Eeltink, A.; Shortridge-Baggett, L. The psychometric properties of the diabetes management self-efficacy scale for patients with type 2 diabetes mellitus. J. Adv. Nurs. 1999, 30, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Asingizwe, D.; Poortvliet, P.M.; Koenraadt, C.J.M.; van Vliet, A.; Ingabire, C.M.; Mutesa, L.; Leeuwis, C. Role of individual perceptions in the consistent use of malaria preventive measures: Mixed methods evidence from rural Rwanda. Malar. J. 2019, 18, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.O.; Neilands, T.B.; Dilworth, S.E.; Morin, S.F.; Remien, R.H.; Chesney, M.A. The Role of Self-Efficacy in HIV treatment adherence: Validation of the HIV treatment adherence Self-Efficacy Scale (HIV-ASES). J. Behav. Med. 2007, 30, 359–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mondal, P.; Sinharoy, A.; Sankoorikal, B.-J.; Siddaiah, R.; Mazur, L.; Graff, G. The influence of sociodemographic heterogeneity on the perceptions of COVID-19: A countrywide survey study in the USA. Int. J. Environ. Res. Public Health 2021, 18, 8922. [Google Scholar] [CrossRef]
- Chen, D.; Wang, Y.-J. Inequality-Related Health and Social Factors and Their Impact on Well-Being during the COVID-19 Pandemic: Findings from a National Survey in the UK. Int. J. Environ. Res. Public Health 2021, 18, 1014. [Google Scholar] [CrossRef] [PubMed]
- Gamba, R.J.; Wood, L.M.; Ampil, A.; Engelman, A.; Lam, J.; Schmeltz, M.T.; Pritchard, M.M.; Santillan, J.K.A.; Rivera, E.S.; Ortiz, N.; et al. Investigating the Feasibility of a Restaurant Delivery Service to Improve Food Security among College Students Experiencing Marginal Food Security, a Head-to-Head Trial with Grocery Store Gift Cards. Int. J. Environ. Res. Public Health 2021, 18, 9680. [Google Scholar] [CrossRef]
- Kim, B.H.; Ranzenhofer, L.; Stadterman, J.; Karvay, Y.G.; Burke, N.L. Food insecurity and eating pathology in adolescents. Int. J. Environ. Res. Public Health 2021, 18, 9155. [Google Scholar] [CrossRef]
- Cohen, A.; Ozer, E.; Rehkopf, D.; Abrams, B. High school composition and health outcomes in adulthood: A cohort study. Int. J. Environ. Res. Public Health 2021, 18, 3799. [Google Scholar] [CrossRef] [PubMed]
- Seydou, A. Who Wants COVID-19 Vaccination? In 5 West African Countries, Hesitancy is High, Trust Low. 2021. Available online: https://afrobarometer.org/publications/ad432-who-wants-covid-19-vaccination-5-west-african-countries-hesitancy-high-trust-low (accessed on 6 December 2021).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Chiedozie, A.P.; Chukwuebuka, O.J.; Chidimma, C.F.; Onyinyechi, O.V.; Chijioke, A.K.; Chibuzor, O.S.; Gabriel, O.C.; Chioma, U.B. Willingness to accept a potential COVID-19 vaccine in Nigeria. Am. J. Med. Sci. Med. 2021, 9, 1–5. [Google Scholar]
- Acheampong, T.; Akorsikumah, E.; Osae-Kwapong, J.; Khalid, M.; Appiah, A.; Amuasi, J. Examining vaccine hesitancy in Sub-Saharan Africa: A survey of the knowledge and attitudes among adults to receive COVID-19 vaccines in Ghana. Vaccines 2021, 9, 814. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R.G.; Hagen, L.; Walker, K.; O’Leary, H.; Lengacher, C. The COVID-19 vaccine social media infodemic: Healthcare providers’ missed dose in addressing misinformation and vaccine hesitancy. Hum. Vaccines Immunother. 2021, 17, 2962–2964. [Google Scholar] [CrossRef] [PubMed]
- Yeboah, P.; Forkuo, A.D.; Amponsah, O.K.O.; Adomako, N.O.; Abdin, A.Y.; Nasim, M.J.; Werner, P.; Panyin, A.B.; Emrich, E.; Jacob, C. Antimalarial drugs in Ghana: A case study on personal preferences. Science 2020, 2, 49. [Google Scholar] [CrossRef]
- Ditekemena, J.; Nkamba, D.; Mavoko, A.; Fodjo, J.S.; Luhata, C.; Obimpeh, M.; Van Hees, S.; Nachega, J.; Colebunders, R. COVID-19 Vaccine acceptance in the democratic republic of congo: A cross-sectional survey. Vaccines 2021, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Scharff, D.P.; Mathews, K.J.; Jackson, P.; Hoffsuemmer, J.; Martin, E.; Edwards, D. More than Tuskegee: Understanding Mistrust about Research Participation. J. Health Care Poor Underserved 2010, 21, 879–897. [Google Scholar] [CrossRef]
- Duong, D. What’s important to know about the new COVID-19 variants? Can. Med. Assoc. J. 2021, 193, E141–E142. [Google Scholar] [CrossRef]
- Boehm, E.; Kronig, I.; Neher, R.A.; Eckerle, I.; Vetter, P.; Kaiser, L. Novel SARS-CoV-2 variants: The pandemics within the pandemic. Clin. Microbiol. Infect. 2021, 27, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Carcelen, A.C.; Prosperi, C.; Mutembo, S.; Chongwe, G.; Mwansa, F.D.; Ndubani, P.; Simulundu, E.; Chilumba, I.; Musukwa, G.; Thuma, P.; et al. COVID-19 vaccine hesitancy in Zambia: A glimpse at the possible challenges ahead for COVID-19 vaccination rollout in sub-Saharan Africa. Hum. Vaccines Immunother. 2021, 1–6. [Google Scholar] [CrossRef]
- Corona: Germany Measures of the Federal Government. Available online: https://www.deutschland.de/en/news/german-federal-government-informs-about-the-corona-crisis (accessed on 23 November 2021).
- Saner, E. The Psychology of Masks: Why Have so Many People Stopped Covering Their Faces? The Guardian, 26 October 2021. Available online: https://www.theguardian.com/world/2021/oct/26/the-great-cover-up-why-the-uk-stopped-wearing-face-masks(accessed on 23 November 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | SD | |
|---|---|---|
| General Knowledge of infectious diseases | 0.654 | 0.188 |
| Influenza | 0.579 | 0.240 |
| Cholera | 0.752 | 0.222 |
| COVID-19 | 0.699 | 0.190 |
| Summative score | 0.671 | 0.177 |
| Preventive Practice | Response (%) Yes |
|---|---|
| Wearing of face mask | 28.7 |
| Regular hand washing | 31.7 |
| Social distancing | 28.0 |
| Willingness to be vaccinated | 35.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeboah, P.; Daliri, D.B.; Abdin, A.Y.; Appiah-Brempong, E.; Pitsch, W.; Panyin, A.B.; Adusei, E.B.A.; Razouk, A.; Nasim, M.J.; Jacob, C. Knowledge into the Practice against COVID-19: A Cross-Sectional Study from Ghana. Int. J. Environ. Res. Public Health 2021, 18, 12902. https://doi.org/10.3390/ijerph182412902
Yeboah P, Daliri DB, Abdin AY, Appiah-Brempong E, Pitsch W, Panyin AB, Adusei EBA, Razouk A, Nasim MJ, Jacob C. Knowledge into the Practice against COVID-19: A Cross-Sectional Study from Ghana. International Journal of Environmental Research and Public Health. 2021; 18(24):12902. https://doi.org/10.3390/ijerph182412902
Chicago/Turabian StyleYeboah, Prince, Dennis Bomansang Daliri, Ahmad Yaman Abdin, Emmanuel Appiah-Brempong, Werner Pitsch, Anto Berko Panyin, Emmanuel Bentil Asare Adusei, Afraa Razouk, Muhammad Jawad Nasim, and Claus Jacob. 2021. "Knowledge into the Practice against COVID-19: A Cross-Sectional Study from Ghana" International Journal of Environmental Research and Public Health 18, no. 24: 12902. https://doi.org/10.3390/ijerph182412902
APA StyleYeboah, P., Daliri, D. B., Abdin, A. Y., Appiah-Brempong, E., Pitsch, W., Panyin, A. B., Adusei, E. B. A., Razouk, A., Nasim, M. J., & Jacob, C. (2021). Knowledge into the Practice against COVID-19: A Cross-Sectional Study from Ghana. International Journal of Environmental Research and Public Health, 18(24), 12902. https://doi.org/10.3390/ijerph182412902