Environmental Microbial Contamination during Cystic Fibrosis Group-Based Psychotherapy

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
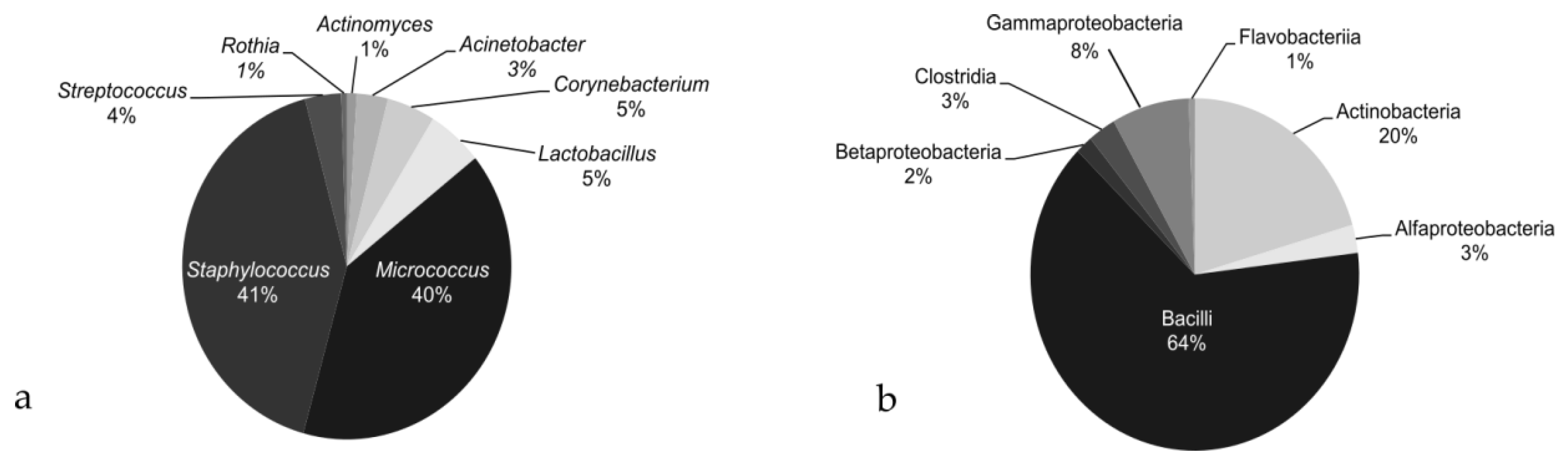
MEM Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Castellani, C.; Duff, A.J.A.; Bell, S.C.; Heijerman, H.G.M.; Munck, A.; Ratjen, F.; Sermet-Gaudelus, I.; Southern, K.W.; Barben, J.; Flume, P.A.; et al. ECFS best practice guidelines: The 2018 revision. J. Cyst. Fibros. 2018, 17, 153–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, S.C.; Mall, M.A.; Gutierrez, H.; Macek, M.; Madge, S.; Davies, J.C.; Burgel, P.R.; Tullis, E.; Castaños, C.; Castellani, C.; et al. The future of cystic fibrosis care: A global perspective. Lancet Respir. Med. 2020, 8, 65–124. [Google Scholar] [CrossRef] [Green Version]
- Helms, S.W.; Dellon, E.P.; Prinstein, M.J. Friendship quality and health-related outcomes among adolescents with cystic fibrosis. J. Pediatr. Psychol. 2015, 40, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Goldbeck, L.; Fidika, A.; Herle, M.; Quittner, A.L. Cochrane corner: Psychological interventions for individuals with cystic fibrosis and their families. Thorax 2015, 70, 1089–1091. [Google Scholar] [CrossRef] [Green Version]
- Saez-Flores, E.; Tonarely, N.A.; Barker, D.H.; Quittner, A.L. Examining the stability of the hospital anxiety and depression scale factor structure in adolescents and young adults with cystic fibrosis: A confirmatory factor analysis. J. Pediatr. Psychol. 2018, 43, 625–635. [Google Scholar] [CrossRef]
- Quittner, A.L.; Goldbeck, L.; Abbott, J.; Duff, A.; Lambrecht, P.; Solé, A.; Tibosch, M.M.; Brucefors, A.B.; Yüksel, H.; Catastini, P.; et al. Prevalence of depression and anxiety in patients with cystic fibrosis and parent caregivers: Results of the International Depression Epidemiological Study across nine countries. Thorax 2014, 69, 1090–1097. [Google Scholar] [CrossRef] [Green Version]
- Quittner, A.L.; Barker, D.H.; Snell, C.; Grimley, M.E.; Marciel, K.; Cruz, I. Prevalence and impact of depression in cystic fibrosis. Curr. Opin. Pulm. Med. 2008, 14, 582–588. [Google Scholar] [CrossRef]
- Lorentzen, S.; Bakali, J.V.; Hersoug, A.G.; Hagtvet, K.A.; Ruud, T.; Høglend, P. Psychodynamic group psychotherapy: Impact of group length and therapist professional characteristics on development of therapeutic alliance. Clin. Psychol. Psychother. 2012, 19, 420–433. [Google Scholar] [CrossRef]
- Saiman, L.; Siegel, J.D.; LiPuma, J.J.; Brown, R.F.; Bryson, E.A.; Chambers, M.J.; Downer, V.S.; Fliege, J.; Hazle, L.A.; Jain, M.; et al. Infection prevention and control guideline for cystic fibrosis: 2013 update. Infect. Control Hosp. Epidemiol. 2014, 35, s1–s67. [Google Scholar] [CrossRef]
- Clifton, I.J.; Peckham, D.G. Defining routes of airborne transmission of Pseudomonas aeruginosa in people with cystic fibrosis. Expert Rev. Respir. Med. 2010, 4, 519–529. [Google Scholar] [CrossRef]
- Knibbs, L.D.; Johnson, G.R.; Kidd, T.J.; Cheney, J.; Grimwood, K.; Kattenbelt, J.A.; O’Rourke, P.K.; Ramsay, K.A.; Sly, P.D.; Wainwright, C.E.; et al. Viability of Pseudomonas aeruginosa in cough aerosols generated by persons with cystic fibrosis. Thorax 2014, 69, 740–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, M.E.; Stockwell, R.E.; Johnson, G.R.; Ramsay, K.A.; Sherrard, L.J.; Jabbour, N.; Ballard, E.; O’Rourke, P.; Kidd, T.J.; Wainwright, C.E.; et al. Face masks and cough etiquette reduce the cough aerosol concentration of Pseudomonas aeruginosa in people with cystic fibrosis. Am. J. Respir. Crit. Care Med. 2018, 197, 348–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, M.E.; Stockwell, R.E.; Johnson, G.R.; Ramsay, K.A.; Sherrard, L.J.; Kidd, T.J.; Cheney, J.; Ballard, E.L.; O’Rourke, P.; Jabbour, N.; et al. Cystic fibrosis pathogens survive for extended periods within cough-generated droplet nuclei. Thorax 2019, 74, 87–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pegues, D.A.; Carson, L.A.; Tablan, O.C.; FitzSimmons, S.C.; Roman, S.B.; Miller, J.M.; Jarvis, W.R. Acquisition of Pseudomonas cepacia at summer camps for patients with cystic fibrosis. J. Pediatr. 1994, 124, 694–702. [Google Scholar] [CrossRef] [Green Version]
- Saiman, L.; Siegel, J. Infection control recommendations for patients with cystic fibrosis: Microbiology, important pathogens, and infection control practices to prevent patient-to-patient transmission. Am. J. Infect. Control 2003, 31, 1–62. [Google Scholar] [CrossRef] [Green Version]
- Ridderberg, W.; Andersen, C.; Væth, M.; Bregnballe, V.; Nørskov-Lauritsen, N.; Schiøtz, P.O. Lack of evidence of increased risk of bacterial transmission during cystic fibrosis educational programmes. J. Cyst. Fibros. 2016, 15, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Döring, G.; Conway, S.P.; Heijerman, H.G.M.; Hodson, M.E.; Hùiby, N.; Smyth, A.; Touw, D.J. Antibiotic therapy against Pseudomonas aeruginosa in cystic fibrosis. Eur. Respir. J. 2000, 16, 749–767. [Google Scholar] [CrossRef]
- Napoli, C.; Marcotrigiano, V.; Montagna, M.T. Air sampling procedures to evaluate microbial contamination: A comparison between active and passive methods in operating theatres. BMC Public Health 2012, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- Pasquarella, C.; Pitzurra, O.; Savino, A. The index of microbial air contamination. J. Hosp. Infect. 2000, 46, 241–256. [Google Scholar] [CrossRef] [Green Version]
- Human Microbiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature 2012, 486, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Grice, E.A.; Segre, J.A. The skin microbiome. Nat. Rev. Microbiol. 2011, 9, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Erdem, G.; Leber, A. Acinetobacter species. In Principles and Practice of Pediatric Infectious Diseases; Long, S.S., Prober, C.G., Fischer, M., Eds.; Elsevier Inc.: Amsterdam, The Netherlands, 2018; pp. 851–853. ISBN 9780323401814. [Google Scholar]
- Kashem, S.W.; Kaplan, D.H. Skin immunity to Candida albicans. Trends Immunol. 2016, 37, 440–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miroballi, Y.; Garber, E.; Jia, H.; Zhou, J.J.; Alba, L.; Quittell, L.M.; Angst, D.; Cabana, M.; Saiman, L. Infection control knowledge, attitudes, and practices among cystic fibrosis patients and their families. Pediatr. Pulmonol. 2012, 47, 144–152. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patient | Gender | FEV1 1 | Colonization Year 2013 | Colonization Year 2014 | Colonization Year 2015 | |||
|---|---|---|---|---|---|---|---|---|
| Range (%) | Chronic 2 | Intermittent 2 | Chronic | Intermittent | Chronic | Intermittent | ||
| Pt1 | M | 71–63 | PA 3, PAM | CA, CI, KO, MSSA | PA, PAM | CA | PA, PAM | MSSA |
| Pt2 | F | 48–45 | PA, PAM | CA, GC, KO | PA, PAM | CA, EC | Not available * | Not available * |
| Pt3 | M | 42–41 | PA | CA, PAM, STM | PA, PAM | CA, MSSA | PA, PAM | AF, CA |
| Pt4 | F | 49–42 | PA, PAM | AC, AF | PA, PAM | AF, STM | PA, PAM | none |
| Pt5 | F | 99–76 | PA | CA, EF, PAM, MSSA | PA, PAM | AF, CA, MSSA, STM | PA, STM | none |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossitto, M.; Tabarini, P.; Tuccio Guarna Assanti, V.; Montemitro, E.; Pompilio, A.; Fiscarelli, E.V. Environmental Microbial Contamination during Cystic Fibrosis Group-Based Psychotherapy. Int. J. Environ. Res. Public Health 2021, 18, 1142. https://doi.org/10.3390/ijerph18031142
Rossitto M, Tabarini P, Tuccio Guarna Assanti V, Montemitro E, Pompilio A, Fiscarelli EV. Environmental Microbial Contamination during Cystic Fibrosis Group-Based Psychotherapy. International Journal of Environmental Research and Public Health. 2021; 18(3):1142. https://doi.org/10.3390/ijerph18031142
Chicago/Turabian StyleRossitto, Martina, Paola Tabarini, Vanessa Tuccio Guarna Assanti, Enza Montemitro, Arianna Pompilio, and Ersilia Vita Fiscarelli. 2021. "Environmental Microbial Contamination during Cystic Fibrosis Group-Based Psychotherapy" International Journal of Environmental Research and Public Health 18, no. 3: 1142. https://doi.org/10.3390/ijerph18031142