Prevalence of Diabetes and Hypertension among Hajj Pilgrims: A Systematic Review


 ,
,  and
and
Abstract
:1. Introduction
2. Method
2.1. Study Design
2.2. Data Sources and Search Strategy
2.3. Study Selection
2.4. Data Extraction and Quality Management
2.5. Data Synthesis and Statistical Analysis
3. Results
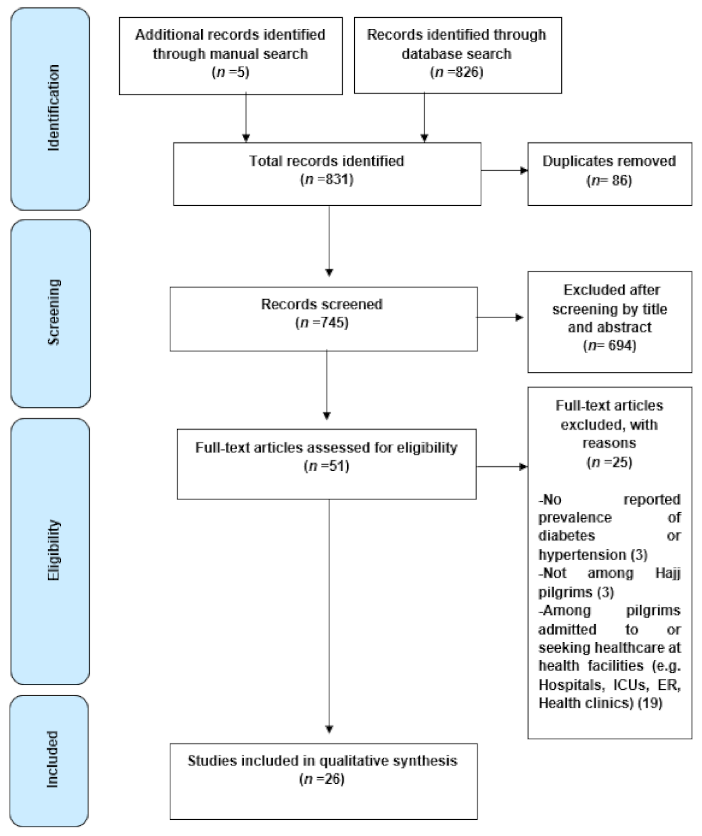
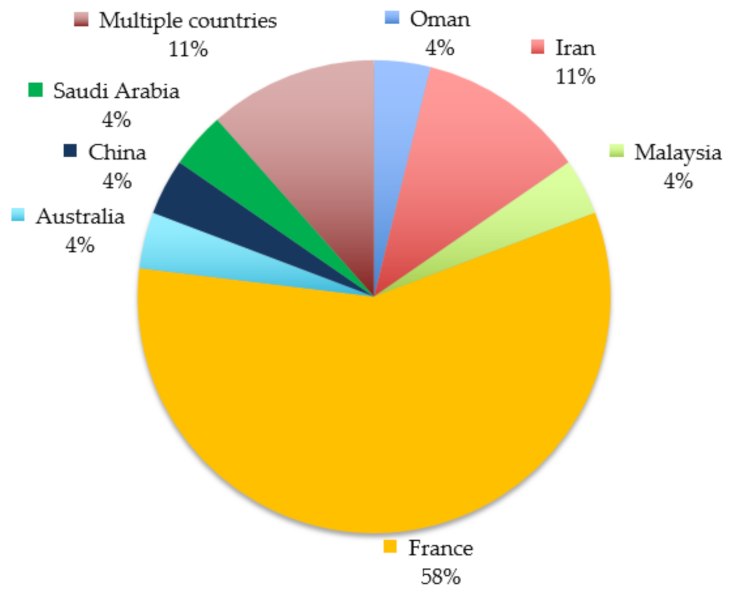
3.1. Included Studies
3.2. Prevalence of Diabetes and Hypertension among Hajj Pilgrims
3.3. Prevalence of Other Health Conditions among Hajj Pilgrims
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Global Burden of Diseases (G. B. D.)-Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Diseases (G. B. D.)-Disease Injury Incidence Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014. Attaining the Nine Global Noncommunicable Diseases Targets; A Shared Responsibility; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Hypertension- Fact. sheet; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Bommer, C.; Heesemann, E.; Sagalova, V.; Manne-Goehler, J.; Atun, R.; Barnighausen, T.; Vollmer, S. The global economic burden of diabetes in adults aged 20–79 years: A cost-of-illness study. Lancet Diabetes Endocrinol. 2017, 5, 423–430. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P. Global burden of disease--where does diabetes mellitus fit in? Nat. Rev. Endocrinol. 2013, 9, 258–260. [Google Scholar] [CrossRef]
- Yezli, S.; Yassin, Y.; Awam, A.; Attar, A.; Al-Jahdali, E.; Alotaibi, B. Umrah. An opportunity for mass gatherings health research. Saudi Med. J. 2017, 38, 868–871. [Google Scholar] [CrossRef]
- Ebrahim, S.H.; Memish, Z.A.; Uyeki, T.M.; Khoja, T.A.; Marano, N.; McNabb, S.J. Public health. Pandemic H1N1 and the 2009 Hajj. Science 2009, 326, 938–940. [Google Scholar] [CrossRef]
- Ahmed, Q.A.; Arabi, Y.M.; Memish, Z.A. Health risks at the Hajj. Lancet 2006, 367, 1008–1015. [Google Scholar] [CrossRef]
- Shafi, S.; Dar, O.; Khan, M.; Khan, M.; Azhar, E.I.; McCloskey, B.; Zumla, A.; Petersen, E. The annual Hajj pilgrimage-minimizing the risk of ill health in pilgrims from Europe and opportunity for driving the best prevention and health promotion guidelines. Int. J. Infect. Dis. 2016, 47, 79–82. [Google Scholar] [CrossRef] [Green Version]
- Algeffari, M. Diabetes and Hajj pilgrims: A Narrative review of literature. J. Pak. Med. Assoc. 2019, 69, 879–884. [Google Scholar]
- Khogeer, Z.; Alnifaee, R.; Alyamani, S.; Alharbi, K.; Hanbzaza, S.; Mashhor, A.; Alfelali, M.; Barasheed, O. Acute Complications of Diabetes Among Pilgrims During Hajj 2017: A Brief Report. Diabetes 2020, 741–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Shimemeri, A. Cardiovascular disease in Hajj pilgrims. J. Saudi Heart Assoc. 2012, 24, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Shujaa, A.; Alhamid, S. Health response to Hajj mass gathering from emergency perspective, narrative review. Turk. J. Emerg. Med. 2015, 15, 172–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sindy, A.I.; Baljoon, M.J.; Zubairi, N.A.; Dhafar, K.O.; Gazzaz, Z.J.; Deiab, B.A.; Hothali, F.A. Pattern of patients and diseases during mass transit: The day of Arafat experience. Pak. J. Med. Sci. 2015, 31, 1099–1103. [Google Scholar] [CrossRef]
- Yezli, S.; Elganainy, A.; Awam, A. Strengthening health security at the Hajj mass gatherings: A Harmonised Hajj Health Information System. J. Travel Med. 2018, 25. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef] [Green Version]
- Baomer, A.A.S.; El Bushra, H.E. Profile of diabetic Omani pilgrims to Mecca. East. Afr. Med. J. 1998, 75, 211–214. [Google Scholar]
- Afshin-Nia, F.; Dehkordi, H.M.; Fazel, M.R.; Ghanei, M. How to reduce cardiovascular mortality and morbidity among Hajj Pilgrims: A multiphasic screening, intervention and assessment. Ann. Saudi Med. 1999, 19, 55–57. [Google Scholar] [CrossRef]
- Choudhry, A.J.; Al-Mudaimegh, K.S.; Turkistani, A.M.; Al-Hamdan, N.A. Hajj-associated acute respiratory infection among hajjis from Riyadh. East. Mediterr. Health J. 2006, 12, 300–309. [Google Scholar]
- Azarpazhooh, M.R.; Rafi, S.; Etemadi, M.M.; Khadem, N.; Fazlinejad, A. The relation between short-term oral contraceptive consumption and cerebrovascular, cardiovascular disorders in Iranian women attending Hajj. Saudi Med. J. 2008, 29, 1024–1027. [Google Scholar] [PubMed]
- Gautret, P.; Soula, G.; Delmont, J.; Parola, P.; Brouqui, P. Common health hazards in french pilgrims during the hajj of 2007: A prospective cohort study. J. Travel Med. 2009, 16, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautret, P.; Yong, W.; Soula, G.; Gaudart, J.; Delmont, J.; Dia, A.; Parola, P.; Brouqui, P. Incidence of Hajj-associated febrile cough episodes among French pilgrims: A prospective cohort study on the influence of statin use and risk factors. Clin. Microbiol. Infect. 2009, 15, 335–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deris, Z.Z.; Hasan, H.; Wahab, M.S.A.; Sulaiman, S.A.; Naing, N.N.; Othman, N.H. The association between pre-morbid conditions and respiratory tract manifestations amongst Malaysian Hajj pilgrims. Trop. Biomed. 2010, 27, 294–300. [Google Scholar] [PubMed]
- Gautret, P.; Bauge, M.; Simon, F.; Benkouiten, S.; Valero, R.; Parola, P.; Brouqui, P. Overweight and obesity in French Hajj pilgrims. J. Immigr Minor. Health 2013, 15, 215–218. [Google Scholar] [CrossRef]
- Razavi, S.M.; Sabouri-Kashani, A.; Ziaee-Ardakani, H.; Tabatabaei, A.; Karbakhsh, M.; Sadeghipour, H.; Mortazavi-Tabatabaei, S.A.; Salamati, P. Trend of diseases among Iranian pilgrims during five consecutive years based on a Syndromic Surveillance System in Hajj. Med. J. Islam Repub. Iran. 2013, 27, 179–185. [Google Scholar]
- Benkouiten, S.; Charrel, R.; Belhouchat, K.; Drali, T.; Salez, N.; Nougairede, A.; Zandotti, C.; Memish, Z.A.; al Masri, M.; Gaillard, C.; et al. Circulation of respiratory viruses among pilgrims during the 2012 Hajj pilgrimage. Clin. Infect. Dis. 2013, 57, 992–1000. [Google Scholar] [CrossRef] [Green Version]
- Gautret, P.; Benkouiten, S.; Salaheddine, I.; Belhouchat, K.; Drali, T.; Parola, P.; Brouqui, P. Hajj pilgrims knowledge about Middle East respiratory syndrome coronavirus, August to September 2013. Euro Surveill 2013, 18, 20604. [Google Scholar] [CrossRef]
- Gautret, P.; Benkouiten, S.; Salaheddine, I.; Parola, P.; Brouqui, P. Preventive measures against MERS-CoV for Hajj pilgrims. Lancet Infect. Dis. 2013, 13, 829–831. [Google Scholar] [CrossRef] [Green Version]
- Memish, Z.A.; Assiri, A.; Almasri, M.; Alhakeem, R.F.; Turkestani, A.; Al Rabeeah, A.A.; Al-Tawfiq, J.A.; Alzahrani, A.; Azhar, E.; Makhdoom, H.Q.; et al. Prevalence of MERS-CoV nasal carriage and compliance with the Saudi health recommendations among pilgrims attending the 2013 Hajj. J. Infect. Dis. 2014, 210, 1067–1072. [Google Scholar] [CrossRef] [Green Version]
- Gautret, P.; Charrel, R.; Benkouiten, S.; Belhouchat, K.; Nougairede, A.; Drali, T.; Salez, N.; Memish, Z.A.; al Masri, M.; Lagier, J.C.; et al. Lack of MERS coronavirus but prevalence of influenza virus in French pilgrims after 2013 Hajj. Emerg. Infect. Dis. 2014, 20, 728–730. [Google Scholar] [CrossRef]
- Tashani, M.; Barasheed, O.; Azeem, M.; Alfelali, M.; Badahdah, A.M.; Bokhary, H.; Almasri, N.; Alshehri, J.; Matbouly, G.; Kalantan, N.; et al. Pneumococcal vaccine uptake among Australian hajj pilgrims in 2011-13. Infect. Disord. Drug Targets 2014, 14, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Gautret, P.; Benkouiten, S.; Griffiths, K.; Sridhar, S. The inevitable Hajj cough: Surveillance data in French pilgrims, 2012–2014. Travel Med. Infect. Dis. 2015, 13, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, S.; Benkouiten, S.; Belhouchat, K.; Drali, T.; Memish, Z.A.; Parola, P.; Brouqui, P.; Gautret, P. Foot ailments during Hajj: A short report. J. Epidemiol Glob. Health 2015, 5, 291–294. [Google Scholar] [CrossRef] [Green Version]
- Verhoeven, P.O.; Gautret, P.; Haddar, C.H.; Benkouiten, S.; Gagnaire, J.; Belhouchat, K.; Grattard, F.; Charrel, R.; Pozzetto, B.; Drali, T.; et al. Molecular dynamics of Staphylococcus aureus nasal carriage in Hajj pilgrims. Clin. Microbiol. Infect. 2015, 21, 650.e655–650.e658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagneux-Brunon, A.; Andrillat, C.; Fouilloux, P.; Daoud, F.; Defontaine, C.; Charles, R.; Lucht, F.; Botelho-Nevers, E. Pre-travel advice seeking from GPs by travellers with chronic illness seen at a travel clinic. J. Travel Med. 2016, 23. [Google Scholar] [CrossRef] [Green Version]
- Yezli, S.; Zumla, A.; Yassin, Y.; Al-Shangiti, A.M.; Mohamed, G.; Turkistani, A.M.; Alotaibi, B. Undiagnosed Active Pulmonary Tuberculosis among Pilgrims during the 2015 Hajj Mass Gathering: A Prospective Cross-sectional Study. Am. J. Trop. Med. Hyg. 2017, 97, 1304–1309. [Google Scholar] [CrossRef]
- Sow, D.; Dogue, F.; Edouard, S.; Drali, T.; Prades, S.; Battery, E.; Yezli, S.; Alotaibi, B.; Sokhna, C.; Raoult, D.; et al. Acquisition of enteric pathogens by pilgrims during the 2016 Hajj pilgrimage: A prospective cohort study. Travel Med. Infect. Dis. 2018, 25, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Hoang, V.T.; Ali-Salem, S.; Belhouchat, K.; Meftah, M.; Sow, D.; Dao, T.L.; Ly, T.D.A.; Drali, T.; Ninove, L.; Yezli, S.; et al. Respiratory tract infections among French Hajj pilgrims from 2014 to 2017. Sci. Rep. 2019, 9, 17771. [Google Scholar] [CrossRef]
- Alzahrani, A.S.; Alhumaidi, F.; Altowairqi, A.; Al-Malki, W.; AlFadhli, I. Screening for cognitive impairment in Arabic-speaking Hajj pilgrims. Egypt. J. Neurol. Psychiatry Neurosurg. 2019, 55, 1–7. [Google Scholar] [CrossRef]
- Hoang, V.T.; Dao, T.L.; Ly, T.D.A.; Belhouchat, K.; Chaht, K.L.; Gaudart, J.; Mrenda, B.M.; Drali, T.; Yezli, S.; Alotaibi, B.; et al. The dynamics and interactions of respiratory pathogen carriage among French pilgrims during the 2018 Hajj. Emerg Microbes Infect. 2019, 8, 1701–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Shi, F.; Yu, Z.; Yang, A.; Zeng, M.; Wang, J.; Yin, H.; Zhang, B.; Ma, X. A cross-sectional study on factors associated with hypertension and genetic polymorphisms of renin-angiotensin-aldosterone system in Chinese hui pilgrims to hajj. BMC Public Health 2019, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoang, V.T.; Meftah, M.; Anh Ly, T.D.; Drali, T.; Yezli, S.; Alotaibi, B.; Raoult, D.; Parola, P.; Pommier de Santi, V.; Gautret, P. Bacterial respiratory carriage in French Hajj pilgrims and the effect of pneumococcal vaccine and other individual preventive measures: A prospective cohort survey. Travel Med. Infect. Dis. 2019, 31, 101343. [Google Scholar] [CrossRef] [PubMed]
- Hasan, G.; Moabber, H.; Alyamani, A.; Sayeed, A.; Altatar, F. Study on risk factors (Predisposing factors) for poor diabetes control during hajj (1436/2015) in people with diabetes. Pak. J. Med. Sci. 2016, 32, 1092–1096. [Google Scholar] [CrossRef]
- Dong, C.; Ge, P.; Ren, X.; Fan, H.; Yan, X. Prevalence, awareness, treatment and control of hypertension among adults in rural north-western China: A cross-sectional population survey. J. Int. Med. Res. 2013, 41, 1291–1300. [Google Scholar] [CrossRef] [Green Version]
- Esteghamati, A.; Gouya, M.M.; Abbasi, M.; Delavari, A.; Alikhani, S.; Alaedini, F.; Safaie, A.; Forouzanfar, M.; Gregg, E.W. Prevalence of diabetes and impaired fasting glucose in the adult population of Iran: National Survey of Risk Factors for Non-Communicable Diseases of Iran. Diabetes Care 2008, 31, 96–98. [Google Scholar] [CrossRef] [Green Version]
- Khan, I.D.; Khan, S.A.; Asima, B.; Hussaini, S.B.; Zakiuddin, M.; Faisal, F.A. Morbidity and mortality amongst Indian Hajj pilgrims: A 3-year experience of Indian Hajj medical mission in mass-gathering medicine. J. Infect. Public Health 2018, 11, 165–170. [Google Scholar] [CrossRef]
- Pane, M.; Kong, F.Y.M.; Purnama, T.B.; Glass, K.; Imari, S.; Samaan, G.; Oshitani, H. Indonesian Hajj Cohorts and Mortality in Saudi Arabia from 2004 to 2011. J. Epidemiol. Glob. Health 2019, 9, 11–18. [Google Scholar] [CrossRef]
- Madani, T.A.; Ghabrah, T.M.; Albarrak, A.M.; Alhazmi, M.A.; Alazraqi, T.A.; Althaqafi, A.O.; Ishaq, A.H. Causes of admission to intensive care units in the Hajj period of the Islamic year 1424 (2004). Ann. Saudi Med. 2007, 27, 101–105. [Google Scholar]
- Khan, N.A.; Ishag, A.M.; Ahmad, M.S.; El-Sayed, F.M.; Bachal, Z.A.; Abbas, T.G. Pattern of medical diseases and determinants of prognosis of hospitalization during 2005 Muslim pilgrimage (Hajj) in a tertiary care hospital. A prospective cohort study. Saudi Med. J. 2006, 27, 1373–1380. [Google Scholar]
- Al-Ghamdi, S.A.; Akbar, H.O.; Qari, Y.A.; Fathaldin, O.A.; Al-Rashed, R.S. Pattern of admission to hospitals during muslim pilgrimage (Hajj). Saudi Med. J. 2003, 24, 1073–1076. [Google Scholar] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pr. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteghamati, A.; Etemad, K.; Koohpayehzadeh, J.; Abbasi, M.; Meysamie, A.; Noshad, S.; Asgari, F.; Mousavizadeh, M.; Rafei, A.; Khajeh, E.; et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005-2011. Diabetes Res. Clin. Pr. 2014, 103, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Lailler, G.; Piffaretti, C.; Fuentes, S.; Nabe, H.D.; Oleko, A.; Cosson, E.; Fosse-Edorh, S. Prevalence of prediabetes and undiagnosed type 2 diabetes in France: Results from the national survey ESTEBAN, 2014-2016. Diabetes Res. Clin. Pr. 2020, 165, 108252. [Google Scholar] [CrossRef] [PubMed]
- Bonaldi, C.; Vernay, M.; Roudier, C.; Salanave, B.; Oleko, A.; Malon, A.; Castetbon, K.; Fagot-Campagna, A. A first national prevalence estimate of diagnosed and undiagnosed diabetes in France in 18- to 74-year-old individuals: The French Nutrition and Health Survey 2006/2007. Diabet. Med. 2011, 28, 583–589. [Google Scholar] [CrossRef]
- Fosse-Edorh, S.; Fagot-Campagna, A.; Detournay, B.; Bihan, H.; Gautier, A.; Dalichampt, M.; Druet, C. Type 2 diabetes prevalence, health status and quality of care among the North African immigrant population living in France. Diabetes Metab. 2014, 40, 143–150. [Google Scholar] [CrossRef]
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Hassen Abate, K.; Akinyemiju, T.F.; et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.B.; Zhang, Y.; Wang, T.D.; Liu, J.X.; Yi, Y.J.; Liu, Y.; Xu, R.H.; Hu, Y.M.; Chen, M. Prevalence, awareness, treatment, and control of hypertension in southwestern China. Sci. Rep. 2019, 9, 19098. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.Y.; Chen, W.W.; Gao, R.L.; Liu, L.S.; Zhu, M.L.; Wang, Y.J.; Wu, Z.S.; Li, H.J.; Gu, D.F.; Yang, Y.J.; et al. China cardiovascular diseases report 2018: An updated summary. J. Geriatr. Cardiol. 2020, 17, 1–8. [Google Scholar]
- Li, Y.; Wang, L.; Feng, X.; Zhang, M.; Huang, Z.; Deng, Q.; Zhou, M.; Astell-Burt, T.; Wang, L. Geographical variations in hypertension prevalence, awareness, treatment and control in China: Findings from a nationwide and provincially representative survey. J. Hypertens 2018, 36, 178–187. [Google Scholar] [CrossRef]
- Tailakh, A.; Mentes, J.C.; Morisky, D.E.; Pike, N.A.; Phillips, L.R.; Evangelista, L.S. Prevalence, awareness, treatment, and control of hypertension among Arab Americans. J. Cardiovasc. Nurs. 2013, 28, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfelali, M.; Barasheed, O.; Alshehri, J.; Bokhary, H.; Alsaedi, S.; Alhamzi, A.; Aljohani, N.; Driscoll, T.; Rashid, H. Foot injuries among Hajj pilgrims with and without diabetes mellitus: Implications for infection management. Infect. Disord. Drug Targets 2014, 14, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Vinay, R.; Goldman, J.M. Diabetic foot complications associated with the Haj (Islamic pilgrimage). Pract. Diabetes Int. 2004, 21, 138. [Google Scholar] [CrossRef]
- Khan, S.A.; Bhat, A.R.; Khan, L.A. Hypoglycemia in diabetics during Hajj. Saudi Med. J. 2002, 23, 1548. [Google Scholar]
- Lackland, D.T.; Weber, M.A. Global burden of cardiovascular disease and stroke: Hypertension at the core. Can. J. Cardiol. 2015, 31, 569–571. [Google Scholar] [CrossRef]
- Almekhlafi, M.A.; Alhazmi, M.A.; Alsulami, S.S.; Almorsy, S.A. Incidence and impact of stroke during Hajj. Results of 2015 Hajj stroke registry. Neurosciences 2017, 22, 181–185. [Google Scholar] [CrossRef] [Green Version]
- Arabi, Y.M.; Alhamid, S.M. Emergency room to the intensive care unit in Hajj. The chain of life. Saudi Med. J. 2006, 27, 937–941. [Google Scholar]
- Global Burden of Diseases (G. B. D.)-Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- McAloon, C.J.; Osman, F.; Glennon, P.; Lim, P.B.; Hayat, S.A. Global Epidemiology and Incidence of Cardiovascular Disease. In Cardiovascular Diseases: Genetic Susceptibility, Environmental Factors and Their Interaction; Papageorgiou, N., Ed.; Academic Press: Cambridge, MA, USA, 2017; Chapter 4. [Google Scholar]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll Cardiol 2017, 70, 1–25. [Google Scholar] [CrossRef]
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the Global Burden of Chronic Liver Diseases From 2012 to 2017: The Growing Impact of Nonalcoholic Fatty Liver Disease. Hepatology 2020, 75, 1605–1616. [Google Scholar] [CrossRef] [PubMed]
- The International Agency for Research on Cancer. Latest Global Cancer Data; The International Agency for Research on Cancer: Geneva, Switzerland, 2018. [Google Scholar]
- Yezli, S.; Alotaibi, B.M.; Bin Saeed, A.A. The Hajj Health Requirements: Time for a serious review? Lancet 2016, 387, 845–846. [Google Scholar] [CrossRef]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Report on Diabetes; WHO: Geneva, Switzerland, 2016. [Google Scholar]



{kind=link}
{kind=link}
| Study | Study Population | Prevalence of UHCs n/N (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Study Period | Study Design | Evaluation Method | Nationality | Sample Size | Age (Years) | Gender (Male: Female) | Diabetes | Hypertension | Other | At Least One UHC |
| Baomer and Elbushra. 1998 [20] | 1996 | CS | - | Oman | 10,800 | NR | NR | 169/10800 (1.6%) | NR | - | NR |
| Afshin-Nia et al., 1999 [21] | 1993 | CS | C | Iran | 4059 | Mean = 60.6 ± 9.4 | NR | NR | 627/4059 (15.5%) | Heart failure: 143/4059 (3.5%) Ischemic heart disease: 102/4059 (2.5%) Other cardiovascular diseases: 147/4059 (3.6%) | NR |
| Choudhry et al., 2006 [22] | 2003 | CO | Q | KSA 1 | 1027 | Mean = 33.5 ± 11.7 | 2.7:1 | 47/1027 (4.6%) | NR | Bronchial asthma: 16/1027 (1.6%) Chronic sinusitis: 19/1027 (1.9%) Chronic tonsillitis: 16/1027 (1.6%) | 83/1027 (8.1%) |
| Azarpazhooh et al., 2008 [23] | 2005 | CO | C | Iran | 896 | NR | NR | 29/896 (3.2%) | 46/896 (5.1%) | Hyperlipidaemia: 34/896 (3.8%) | NR |
| Gautret et al., 2009 [24] | 2007 | CO | Q | France | 545 | Median = 61.0, range (02–87) | 1.3:1 | 114/545 (21.0%) | 113/545 (20.7%) | Chronic respiratory disease: 32/545 (6.0%) Chronic diarrhoea: 4/545 (1.0%) Walking disability: 134/545 (26%) Hypercholesterolemia: 52/545 (10.0%) | 146/545 (27.0%) |
| Gautret et al., 2009 [25] | 2006 | CO | Q | France | 580 | Mean = 58.0, range (20–85) | 1.3:1 | 132/580 (22.8%) | 147/580 (25.3%) | Chronic respiratory disease: 23/580 (4.0%) Hypercholesterolemia: 60/580 (10.3%) | 249/580 (43.0%) |
| Deris et al., 2010 [26] | 2007 | CS | Q | Malaysia | 387 | Mean = 50.3 ± 10.9 | 1.3:1 | 47/387 (12.1%) | 37/387 (9.6%) | Cardiac disease: 2/387 (0.5%) Cancer: 1/387 (0.2%) COPD: 34/387 (8.8%) Allergic rhinitis: 28/387 (7.20%) | NR |
| Gautret et al., 2013 [27] | 2010 | CS | Q | France | 523 | Median = 60.0, range (19–86) | 1.2:1 | 131/523 (25.0%) | 133/523 (25.4%) | - | NR |
| Razavi et al., 2013 [28] | 2004–2008 | CO | C | Iran | 254823 | Mean = 51.0, range (15–95) | 1.1:1 | 13471/254823 (5.3%) | 30398/254823 (12.0%) | Cardiac disease: 9513/254823 (3.7%) Stroke: 249/195949 (0.1%) Asthma and COPD: 4976/254823 (1.9%) Musculoskeletal disease: 42324/224786 (18.8%) Psychiatric disorders: 2212/224786 (1.0%) Dementia: 438/254823 (0.2%) | NR |
| Benkouiten et al., 2013 [29] | 2012 | CO | Q | France | 167 | Mean = 59.3 ± 12.4, range (21–83) | 0.6:1 | 46/167 (27.5%) | 44/167 (26.3%) | Chronic respiratory disease: 13/167 (7.8%) Chronic cardiac disease: 12/167 (7.2%) | 96/167 (57.5%) |
| Gautret et al., 2013 [30] | 2013 | CS | Q | France | 360 | Mean = 58.0, range (20–85) | 1.1:1 | 83/360 (23.1%) | NR | Chronic kidney disease: 1/360 (0.3%) Chronic lung disease: 17/360 (4.7%) Chronic cardiac disease: 34/360 (9.4%) Cancer: 0/360 (0.0%) Immune deficiency: 6/360 (1.7%) | 116/360 (32.2%) |
| Gautret et al., 2013 [31] | 2013 | CS | Q | France | 114 | Mean = 55.0, range (10–83) | NR | 21/114 (18.4%) | NR | Chronic kidney disease: 1/114 (1.0%) Chronic lung disease: 7/114 (6.0%) Chronic cardiac disease: 6/114 (5.0%) Cancer: 0/114 (0.0%) Immune deficiency: 0/114 (0.0%) | 33/114 (29.0%) |
| Memish et al., 2014 [32] | 2013 | CS | Q | Multiple countries 2 | 5235 | Mean = 51.8, range (18–93) | 1.2:1 | 21/160 (13.1%) | 11/161 (6.8%) | - | |
| Gautret et al., 2014 [33] | 2013 | CO | Q | France | 129 | Mean = 61.7, range (34–85) | 0.7:1 | 34/129 (26.4%) | 43/129 (33.3%) | Chronic respiratory disease: 5/129 (3.9%) Chronic cardiac disease: 11/129 (8.5%) | 68/129 (52.7%) |
| Tashani et al., 2014 [34] | 2011–2013 | CS | Q | Australia | 954 | Mean = 43.0 ± 13.1 | 1.9:1 | 86/954 (9.0%) | NR | Chronic kidney disease: 9/954 (0.9%) Chronic lung disease: 29/954 (3.0%) Chronic cardiac disease: 32/954 (3.3%) Chronic neurological disease: 3/954 (0.3%) | NR |
| Gautret et al., 2015 [35] | 2012–2014 | CO | Q | France | 382 | Mean = 60.6, range (22–85) | 0.6:1 | 105/382 (27.5%) | 115/382 (30.2%) | Chronic kidney disease: 1/382 (0.3%) Chronic respiratory disease: 29/382 (7.6%) Chronic cardiac disease: 32/382 (8.4%) Immune deficiency: 5/382 (1.3%) | 210/382 (55.1%) |
| Sridhar et al., 2015 [36] | 2013 | CO | Q | France | 129 | Mean = 62.0 | 0.7:1 | 34/129 (26.4%) | 43/129 (33.3%) | Chronic respiratory disease: 5/129 (3.9%) Chronic cardiac disease: 11/129 (8.5%) | NR |
| Verhoeven et al., 2015 [37] | 2012 | CO | Q | France | 158 | Mean = 59.6 ± 12.2 | 0.7:1 | 43/158 (27.2%) | NR | - | 92/158 (58.2%) |
| Gagneux-Brunon et al., 2016 [38] | 2013–2014 | CS | Q | France | 388 | Mean = 52.9 ± 18.6 | NR | 78/364 (21.4%) | NR | - | 126/364 (34.6%) |
| Yezli et al., 2017 [39] | 2015 | CS | Q | Multiple countries 3 | 1164 | Mean = 54.5 ± 12.1, range (18–94) | 2.6:1 | 125/1069 (11.7%) | 174/1069 (16.3%) | Chronic kidney disease: 6/1069 (0.6%) Chronic respiratory disease: 13/1069 (1.2%) Chronic liver disease: 7/1069 (0.7%) Cardiovascular disease: 47/1069 (4.4%) Stroke: 1/1069 (0.1%) Cancer: 2/1069 (0.2%) Immune deficiency: 0/1069 (0%) Other: 36/1069 (3.4%) | 296/1069 (27.7%) |
| Sow et al., 2018 [40] | 2016 | CO | Q | France | 117 | Mean = 61.0 | 0.9:1 | 31/117 (26.5%) | 26/117 (22.2%) | Chronic respiratory disease: 11/117 (9.4%) Chronic cardiac disease: 4/117 (3.4%) Immune deficiency: 1/117 (0.9%) | NR |
| Hoang et al., 2019 [41] | 2014–2017 | CO | Q | France | 485 | Median = 61.5, range (21–96) | 0.8:1 | 136/475 (28.6%) | 140/475 (29.5%) | Chronic kidney disease: 5/475 (1.1%) Chronic respiratory disease: 56/475 (11.8%) Chronic cardiac disease: 32/475 (6.7%) Immune deficiency: 3/475 (0.6%) | NR |
| Alzahrani et al., 2019 [42] | 2017 | CS | Q | Multiple countries 4 | 340 | Mean = 66.3 ± 5.9 | 1.2:1 | 109/340 (32.1%) | 145/340 (42.6%) | Hyperlipidaemia: 52/340 (15.3%) Osteoarthritis, heart failure, allergies: 9/340 (2.6%) | NR |
| Hoang et al., 2019 [43] | 2018 | CO | Q | France | 121 | Median = 61.0, range (26–83) | 0.9:1 | 31/121 (25.6%) | 31/121 (25.6%) | Chronic kidney disease: 3/121 (2.5%) Chronic respiratory disease: 16/121 (13.2%) Chronic cardiac disease: 13/121 (10.7%) Immune deficiency: 4/121 (3.3%) | NR |
| Zhang et al., 2019 [44] | 2017 | CS | C | China | 1465 | Mean = 57.0 ± 9.4, range (30–70) | 1.3:1 | 572/1465 (39.0%) | 688/1465 (47.0%) | - | NR |
| Hoang et al., 2019 [45] | 2015 | CO | Q | France | 119 | Mean = 61.0 | 1.1:1 | 39/119 (32.8%) | NR | Chronic kidney disease: 1/119 (0.8%) Chronic respiratory disease: 12/119 (10.1%) Chronic cardiac disease: 8/119 (6.7%) Immune deficiency: 0/119 (0.0%) | NR |
| Cross-Sectional Studies | Selection (Max Five Stars) | Comparability (Max Two Stars) | Outcome/Exposure (Max Three Stars) | Total Score |
| Baomer and Elbushra. 1998 [20] | ** | - | * | 3 |
| Afshin-Nia et al., 1999 [21] | *** | - | *** | 6 |
| Deris et al., 2010 [26] | ** | - | ** | 4 |
| Gautret et al., 2013 [27] | ** | - | ** | 4 |
| Gautret et al., 2013 [30] | *** | - | * | 4 |
| Gautret et al., 2013 [31] | * | - | * | 2 |
| Memish et al., 2014 [32] | *** | - | *** | 6 |
| Tashani et al., 2014 [34] | *** | - | ** | 5 |
| Gagneux-Brunon et al., 2016 [38] | *** | - | ** | 5 |
| Yezli et al., 2017 [39] | *** | - | *** | 6 |
| Alzahrani et al., 2019 [42] | **** | - | ** | 6 |
| Zhang et al., 2019 [44] | *** | - | *** | 6 |
| Cohort Studies | Selection (Max Four Stars) | Comparability (Max Two Stars) | Outcome/Exposure (Max Three Stars) | Total Score |
| Choudhry et al., 2006 [22] | ** | - | ** | 4 |
| Azarpazhooh et al., 2008 [23] | **** | - | *** | 7 |
| Gautret et al., 2009 [24] | ** | - | ** | 4 |
| Gautret et al., 2009 [25] | *** | - | ** | 5 |
| Razavi et al., 2013 [28] | **** | - | *** | 7 |
| Benkouiten et al., 2013 [29] | *** | - | *** | 6 |
| Gautret et al., 2014 [33] | *** | - | ** | 5 |
| Gautret et al., 2015 [35] | ** | - | * | 3 |
| Sridhar et al., 2015 [36] | * | - | * | 2 |
| Verhoeven et al., 2015 [37] | * | - | *** | 4 |
| Sow et al., 2018 [40] | *** | - | *** | 6 |
| Hoang et al., 2019 [41] | *** | - | *** | 6 |
| Hoang et al., 2019 [43] | *** | - | *** | 6 |
| Hoang et al., 2019 [45] | ** | - | *** | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yezli, S.; Mushi, A.; Almuzaini, Y.; Balkhi, B.; Yassin, Y.; Khan, A. Prevalence of Diabetes and Hypertension among Hajj Pilgrims: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1155. https://doi.org/10.3390/ijerph18031155
Yezli S, Mushi A, Almuzaini Y, Balkhi B, Yassin Y, Khan A. Prevalence of Diabetes and Hypertension among Hajj Pilgrims: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(3):1155. https://doi.org/10.3390/ijerph18031155
Chicago/Turabian StyleYezli, Saber, Abdulaziz Mushi, Yasir Almuzaini, Bander Balkhi, Yara Yassin, and Anas Khan. 2021. "Prevalence of Diabetes and Hypertension among Hajj Pilgrims: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 3: 1155. https://doi.org/10.3390/ijerph18031155
APA StyleYezli, S., Mushi, A., Almuzaini, Y., Balkhi, B., Yassin, Y., & Khan, A. (2021). Prevalence of Diabetes and Hypertension among Hajj Pilgrims: A Systematic Review. International Journal of Environmental Research and Public Health, 18(3), 1155. https://doi.org/10.3390/ijerph18031155