
Social Functioning as a Mediator between Developmental Language Disorder (DLD) and Emotional Problems in Adolescents


Abstract
:1. Introduction
1.1. DLD and Emotional Difficulties
1.2. DLD and Social Functioning
1.3. The Emotional Impact of Social Difficulties
1.4. Current Study
2. Materials and Methods
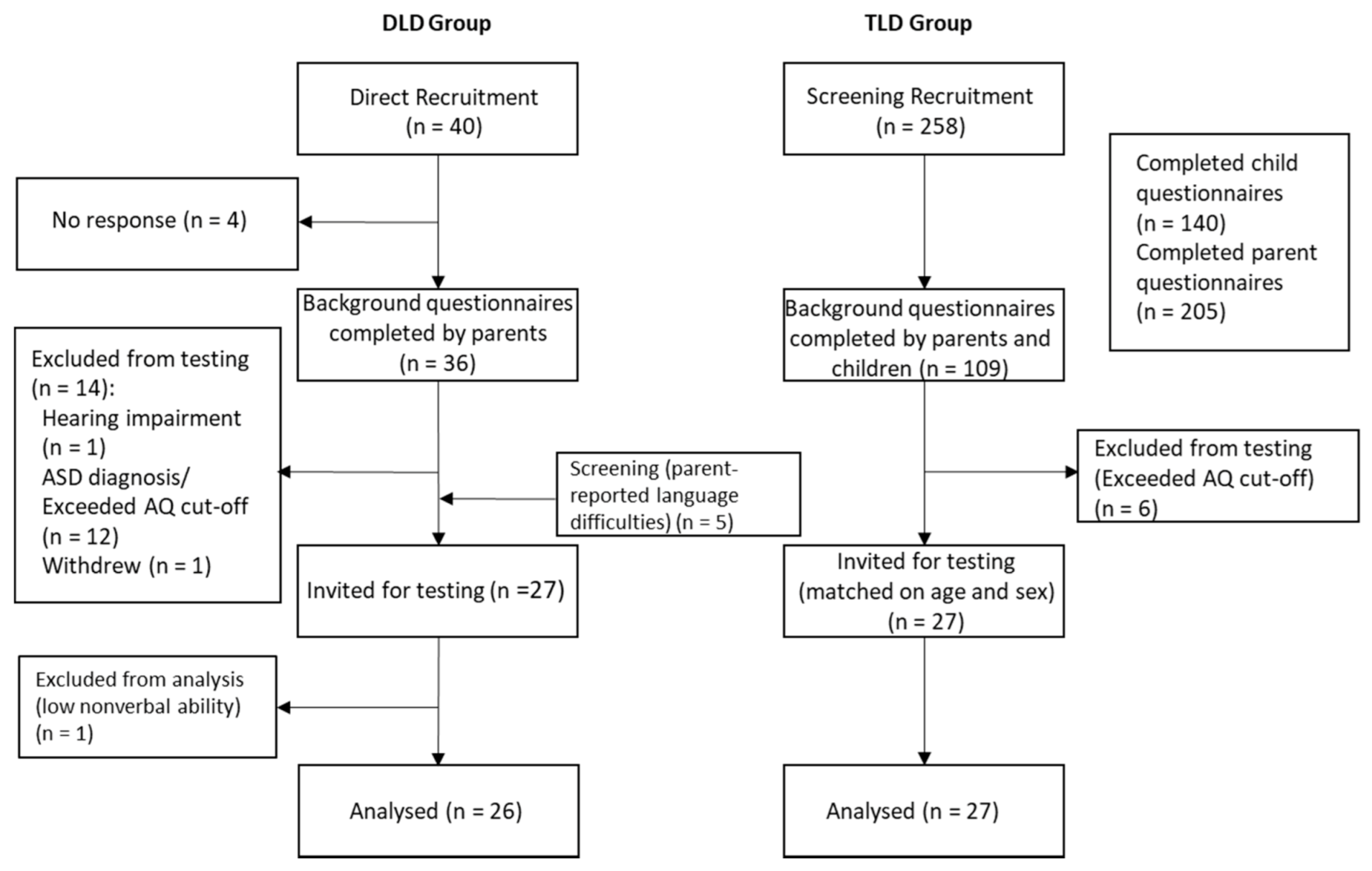
2.1. Recruitment
2.2. Participants
2.3. Measures
2.3.1. Parent-Report
Parent-Report of Socioemotional Abilities
Parent-Report of Autism
2.3.2. Adolescent-Report for Screening Sample Only
Adolescent-Report of Language Abilities
2.3.3. Adolescent Assessment
Language Assessment
Nonverbal Ability
2.3.4. Adolescent Self-Report of Social and Emotional Outcomes
Friendships
Social Support
Mental Well-Being
Anxiety
Depressive Symptoms
2.4. Procedure
2.5. Statistical Analysis
3. Results
3.1. Cognitive and Language Measures
3.2. Social and Emotional Outcomes
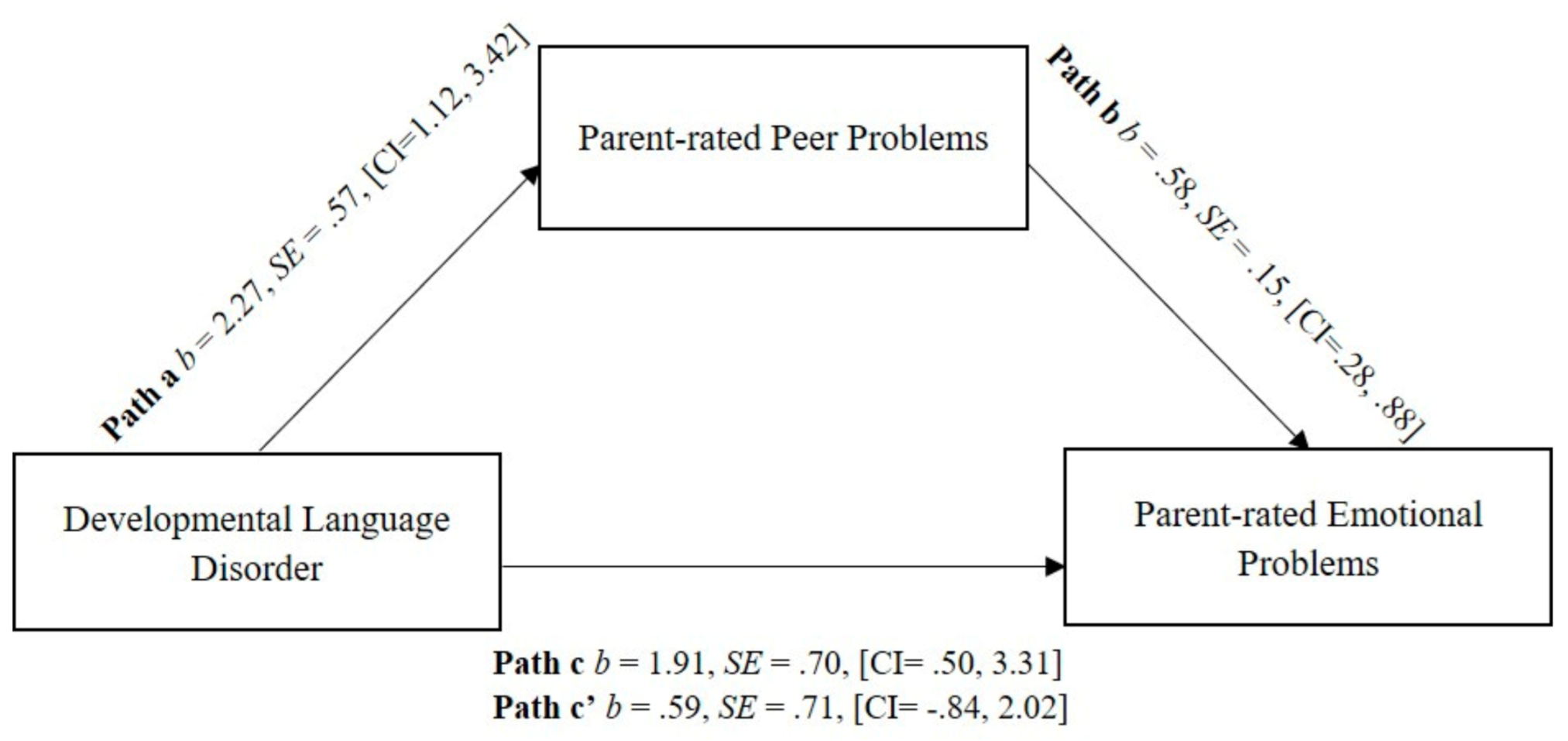
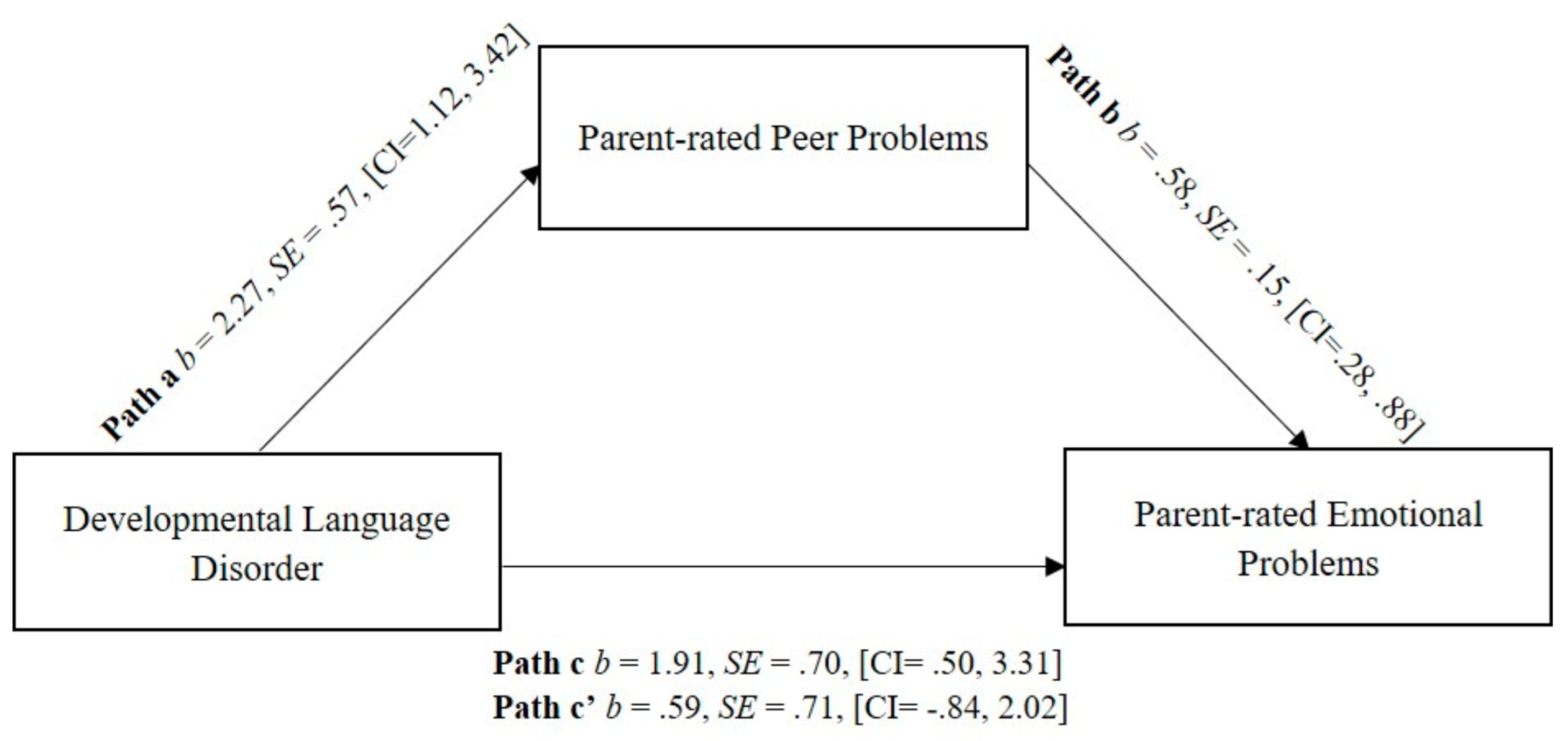
3.3. Social Functioning as a Mediator
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- St Clair, M.C.; Goodyer, I.M.; Dunn, V.; Herbert, J.; Jones, P.B.; Croudace, T. Depressive symptoms during adolescence: Comparison between epidemiological and high risk sampling. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1333–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St Clair, M.C.; Pickles, A.; Durkin, K.; Conti-Ramsden, G. A longitudinal study of behavioral, emotional and social difficulties in individuals with a history of specific language impairment (SLI). J. Commun. Disord. 2011, 44, 186–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, D.V.M.; Snowling, M.J.; Thompson, P.A.; Greenhalgh, T. The Catalise-2 Consortium. Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J. Child Psychol. Psychiatry 2017, 58, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Norbury, C.F.; Gooch, D.; Wray, C.; Baird, G.; Charman, T.; Simonoff, E.; Vamvakas, G.; Pickles, A. The impact of nonverbal ability on prevalence and clinical presentation of language disorder: Evidence from a population study. J. Child Psychol. Psychiatry 2016, 57, 1247–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, P.L.H.; Pickles, A.; Durkin, K.; Conti-Ramsden, G. Longitudinal trajectories of peer relations in children with specific language impairment. J. Child Psychol. Psychiatry 2014, 55, 516–527. [Google Scholar] [CrossRef] [Green Version]
- Beitchman, J.H.; Wilson, B.; Johnson, C.J.; Atkinson, L.; Young, A.; Adlaf, E.; Escobar, M.; Douglas, L. Fourteen-year follow-up of speech/language-impaired and control children: Psychiatric outcome. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 75–82. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Botting, N. Emotional health in adolescents with and without a history of specific language impairment (SLI). J. Child Psychol. Psychiatry 2008, 49, 516–525. [Google Scholar] [CrossRef]
- Clegg, J.; Hollis, C.; Mawhood, L.; Rutter, M. Developmental language disorders a follow-up in later adult life. Cognitive, language and psychosocial outcomes. J. Child Psychol. Psychiatry 2005, 46, 128–149. [Google Scholar] [CrossRef]
- Yew, S.G.K.; O’Kearney, R. Emotional and behavioural outcomes later in childhood and adolescence for children with specific language impairments: Meta-analyses of controlled prospective studies. J. Child Psychol. Psychiatry 2013, 54, 516–524. [Google Scholar] [CrossRef]
- Lloyd-Esenkaya, V.; Russell, A.J.; St Clair, M.C. What Are the Peer Interaction Strengths and Difficulties in Children with Developmental Language Disorder? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3140. [Google Scholar] [CrossRef]
- Jones, P.B. Adult mental health disorders and their age at onset. Br. J. Psychiatry 2013, 202, s5–s10. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, G.; Dockrell, J.E.; Strand, S. Longitudinal patterns of behaviour problems in children with specific speech and language difficulties: Child and contextual factors. Br. J. Educ. Psychol. 2007, 77 Pt 4, 811–828. [Google Scholar] [CrossRef] [PubMed]
- Redmond, S.M.; Rice, M.L. The socioemotional behaviors of children with SLI: Social adaptation or social deviance? J. Speech Lang. Hear. Res. 1998, 41, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Durkin, K.; Conti-Ramsden, G. Language, social behavior, and the quality of friendships in adolescents with and without a history of specific language impairment. Child Dev. 2007, 78, 1441–1457. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, G.; Dockrell, J.E. Longitudinal Patterns of Behavioral, Emotional, and Social Difficulties and Self-Concepts in Adolescents with a History of Specific Language Impairment. Lang. Speech Hear. Serv. Sch. 2012, 43, 445–460. [Google Scholar] [CrossRef]
- Wadman, R.; Botting, N.; Durkin, K.; Conti-Ramsden, G. Changes in emotional health symptoms in adolescents with specific language impairment. Int. J. Lang. Commun. Disord. 2011, 46, 641–656. [Google Scholar] [CrossRef]
- Arseneault, L.; Bowes, L.; Shakoor, S. Bullying victimization in youths and mental health problems: ‘Much ado about nothing’? Psychol. Med. 2010, 40, 717–729. [Google Scholar] [CrossRef]
- Hawker, D.S.J.; Boulton, M.J. Twenty Years’ Research on Peer Victimization and Psychosocial Maladjustment: A Meta-analytic Review of Cross-sectional Studies. J. Child Psychol. Psychiatry 2000, 41, 441–455. [Google Scholar] [CrossRef]
- Van Harmelen, A.L.; Gibson, J.L.; St Clair, M.C.; Owens, M.; Brodbeck, J.; Dunn, V.; Lewis, G.; Croudace, T.; Jones, P.B.; Kievit, R.A.; et al. Friendships and Family Support Reduce Subsequent Depressive Symptoms in At-Risk Adolescents. PLoS ONE 2016, 11, e0153715. [Google Scholar]
- Longobardi, E.; Spataro, P.; Frigerio, A.; Rescorla, L. Language and social competence in typically developing children and late talkers between 18 and 35 months of age. Early Child Dev. Care 2016, 186, 436–452. [Google Scholar] [CrossRef]
- Hart, K.I.; Fujiki, M.; Brinton, B.; Hart, C.H. The Relationship between Social Behavior and Severity of Language Impairment. J. Speech Lang. Hear. Res. 2004, 47, 647–662. [Google Scholar] [CrossRef]
- Maggio, V.; Granana, N.E.; Richaudeau, A.; Torres, S.; Giannotti, A.; Suburo, A.M. Behavior problems in children with specific language impairment. J. Child Neurol. 2014, 29, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Brinton, B.; Fujiki, M.; Spencer, J.C.; Robinson, L.A. The ability of children with specific language impairment to access and participate in an ongoing interaction. J. Speech Lang. Hear. Res. 1997, 40, 1011–1025. [Google Scholar] [CrossRef] [PubMed]
- Crick, N.R.; Dodge, K.A. A Review and Reformulation of Social Information-Processing Mechanisms in Childrens Social-Adjustment. Psychol. Bull. 1994, 115, 74–101. [Google Scholar] [CrossRef]
- Bakopoulou, I.; Dockrell, J.E. The role of social cognition and prosocial behaviour in relation to the socio-emotional functioning of primary aged children with specific language impairment. Res. Dev. Disabil. 2016, 49, 354–370. [Google Scholar] [CrossRef] [PubMed]
- Marton, K.; Abramoff, B.; Rosenzweig, S. Social cognition and language in children with specific language impairment (SLI). J. Commun. Disord. 2005, 38, 143–162. [Google Scholar] [CrossRef]
- Brinton, B.; Fujiki, M.; Hurst, N.Q.; Jones, E.R.; Spackman, M.P. The Ability of Children with Language Impairment to Dissemble Emotions in Hypothetical Scenarios and Natural Situations. Lang. Speech Hear. Serv. Sch. 2015, 46, 325–336. [Google Scholar] [CrossRef]
- Brinton, B.; Spackman, M.P.; Fujiki, M.; Ricks, J. What Should Chris Say? The Ability of Children with Specific Language Impairment to Recognize the Need to Dissemble Emotions in Social Situations. J. Speech Lang. Hear. Res. 2007, 50, 798–811. [Google Scholar] [CrossRef]
- Andres-Roqueta, C.; Adrian, J.E.; Clemente, R.A.; Villanueva, L. Social cognition makes an independent contribution to peer relations in children with Specific Language Impairment. Res. Dev. Disabil. 2016, 49, 277–290. [Google Scholar] [CrossRef]
- Gertner, B.L.; Rice, M.L.; Hadley, P.A. Influence of Communicative Competence on Peer Preferences in a Preschool Classroom. J. Speech Lang. Hear. Res. 1994, 37, 913–923. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Mok, P.L.H.; Pickles, A.; Durkin, K. Adolescents with a history of specific language impairment (SLI): Strengths and difficulties in social, emotional and behavioral functioning. Res. Dev. Disabil. 2013, 34, 4161–4169. [Google Scholar] [PubMed]
- Kilpatrick, T.; Leitão, S.; Boyes, M. Mental health in adolescents with a history of developmental language disorder: The moderating effect of bullying victimisation. Autism Dev. Lang. Impair. 2019, 4, 2396941519893313. [Google Scholar] [CrossRef]
- Van den Bedem, N.P.; Dockrell, J.E.; van Alphen, P.M.; Kalicharan, S.V.; Rieffe, C. Victimization, Bullying, and Emotional Competence: Longitudinal Associations in (Pre)Adolescents With and Without Developmental Language Disorder. J. Speech Lang. Hear. Res. 2018, 61, 2028–2044. [Google Scholar] [CrossRef] [PubMed]
- Redmond, S.M. Peer Victimization among Students with Specific Language Impairment, Attention-Deficit/Hyperactivity Disorder, and Typical Development. Lang. Speech Hear. Serv. Sch. 2011, 42, 520–535. [Google Scholar] [PubMed] [Green Version]
- Lindsay, G.; Dockrell, J.E.; Mackie, C. Vulnerability to bullying in children with a history of specific speech and language difficulties. Eur. J. Spec. Needs Educ. 2008, 23, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Bornstein, M.H.; Hahn, C.S.; Haynes, O.M. Social competence, externalizing, and internalizing behavioral adjustment from early childhood through early adolescence: Developmental cascades. Dev. Psychopathol. 2010, 22, 717–735. [Google Scholar] [CrossRef] [Green Version]
- Wadman, R.; Durkin, K.; Conti-Ramsden, G. Social stress in young people with specific language impairment. J. Adolesc. 2011, 34, 421–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voci, S.C.; Beitchman, J.H.; Brownlie, E.B.; Wilson, B. Social anxiety in late adolescence: The importance of early childhood language impairment. J. Anxiety Disord. 2006, 20, 915–930. [Google Scholar] [CrossRef]
- Durkin, K.; Toseeb, U.; Botting, N.; Pickles, A.; Conti-Ramsden, G. Social Confidence in Early Adulthood Among Young People With and Without a History of Language Impairment. J. Speech Lang. Hear. Res. 2017, 60, 1635–1647. [Google Scholar]
- Wadman, R.; Durkin, K.; Conti-Ramsden, G. Self-esteem, shyness, and sociability in adolescents with specific language impairment (SLI). J. Speech Lang. Hear. R 2008, 51, 938–952. [Google Scholar] [CrossRef] [Green Version]
- Raffaelli, M.; Duckett, E. “We were just talking...”: Conversations in early adolescence. J. Youth Adolesc. 1989, 18, 567–582. [Google Scholar] [CrossRef] [PubMed]
- Rubin, K.H.; Bukowski, W.M.; Parker, J.G. Peer interactions, relationships, and groups. In Handbook of Child Psychology; Wiley: Hoboken, NJ, USA, 1998. [Google Scholar]
- Parker, J.G.; Rubin, K.H.; Erath, S.A.; Wojslawowicz, J.C.; Buskirk, A.A. Peer Relationships, Child Development, and Adjustment: A Developmental Psychopathology Perspective; American Psychological Association (APA): Washington, DC, USA, 2006. [Google Scholar]
- Fujiki, M.; Brinton, B.; Clarke, D. Emotion Regulation in Children with Specific Language Impairment. Lang. Speech Hear. Serv. Sch. 2002, 33, 102–111. [Google Scholar] [CrossRef]
- Forrest, C.L.; Gibson, J.L.; Halligan, S.L.; St Clair, M.C. A longitudinal analysis of early language difficulty and peer problems on later emotional difficulties in adolescence: Evidence from the Millennium Cohort Study. Autism Dev. Lang. Impair. 2018, 3, 2396941518795392. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Hoekstra, R.A.; Knickmeyer, R.; Wheelwright, S. The autism-spectrum quotient (AQ)—Adolescent version. J. Autism Dev. Disord. 2006, 36, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J. Autism Dev. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef]
- Bishop, D.V.M. An Index of Neighbourhood Advantage from English Postcode Data. In BishopBlog; Available online: Deevybee.blogspot.com/2018/09/an-index-of-neighbourhood-advantage.html (accessed on 15 September 2018).
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Goodman, R. The extended version of the strengths and difficulties questionnaire as a guide to child psychiatric caseness and consequent burden. J. Child Psychol. Psychiatry 1999, 40, 791–799. [Google Scholar] [CrossRef]
- Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef]
- Bishop, D.; Whitehouse, A.; Sharp, M. Communication Checklist-Self Report (CC-SR); Pearson: London, UK, 2009. [Google Scholar]
- Semel, E.; Wiig, E.; Secord, W. Clinical Evaluation of Language Fundamentals-UK (CELF-4 UK); Pearson Education: New York, NY, USA, 2006. [Google Scholar]
- Wechsler, D. The Wechsler Intelligence Scale for Children, 4th ed.; Pearson: London, UK, 2004. [Google Scholar]
- University of London. I. o. E. Centre for Longitudinal Studies. Millennium Cohort Study, 2001–2018. [Data Collection]; UK Data Service: Essex, UK, 2018. [Google Scholar]
- Procidano, M.E.; Heller, K. Measures of perceived social support from friends and from family: Three validation studies. Am. J. Community Psychol. 1983, 11, 1–24. [Google Scholar] [CrossRef]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [Green Version]
- St Clair, M.C.; Neufeld, S.; Jones, P.B.; Fonagy, P.; Bullmore, E.T.; Dolan, R.J.; Moutoussis, M.; Toseeb, U.; Goodyer, I.M. Characterising the latent structure and organisation of self-reported thoughts, feelings and behaviours in adolescents and young adults. PLoS ONE 2017, 12, e0175381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, C.R.; Richmond, B.O. What I Think and Feel—Revised Measure of Childrens Manifest Anxiety. J. Abnorm. Child Psychol. 1978, 6, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.J.; Angold, A. Scales to assess child and adolescent depression: Checklists, screens, and nets. J. Am. Acad. Child Adolesc. Psychiatry 1988, 27, 726–737. [Google Scholar] [CrossRef] [PubMed]
- Spss, I. IBM SPSS Statistics for Windows; Version 25; IBM SPSS Corp: Armonk, NY, USA, 2017. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. MethodsInstrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Botting, N.; Conti-Ramsden, G. The role of language, social cognition, and social skill in the functional social outcomes of young adolescents with and without a history of SLI. Br. J. Dev. Psychol. 2008, 26, 281–300. [Google Scholar] [CrossRef]
- Geoffroy, M.-C.; Boivin, M.; Arseneault, L.; Renaud, J.; Perret, L.C.; Turecki, G.; Michel, G.; Salla, J.; Vitaro, F.; Brendgen, M.; et al. Childhood trajectories of peer victimization and prediction of mental health outcomes in midadolescence: A longitudinal population-based study. Can. Med. Assoc. J. 2018, 190, E37–E43. [Google Scholar] [CrossRef] [Green Version]
- Van Harmelen, A.-L.; Kievit, R.; Ioannidis, K.; Neufeld, S.; Jones, P.B.; Bullmore, E.; Dolan, R.; Fonagy, P.; Goodyer, I.; Consortium, N. Adolescent friendships predict later resilient functioning across psychosocial domains in a healthy community cohort. Psychol. Med. 2017, 47, 2312–2322. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| DLD (n = 26) | TLD (n = 27) | Total (n = 53) | DLD vs. TLD | |
|---|---|---|---|---|
| Mean age in yrs; mths (SD months) | 13;6 (16.06) | 13;6 (17.13) | 13;6 (16.45) | -- |
| Female % (n) | 34.6 (10) | 37 (9) | 35.8 (19) | X2 0.03 |
| Mean IDACI Z-score (SD) a | 0.28 (0.91) | 0.84 (0.68) | 0.58 (0.83) | −0.56^(−1.01, −0.11) ** |
| Language spoken | X2 0.31 | |||
| English only % | 96.2 | 92.6 | 94.3 | |
| English plus other % | 3.8 | 7.4 | 5.7 | |
| Motor development | 0.49^(0.15, 1.59) | |||
| Delayed % | 26.9 | 3.7 | 15.1 | |
| Typical % | 53.8 | 81.5 | 67.9 | |
| Fast % | 19.2 | 14.8 | 17 | |
| Speech and language development | 0.05^(0.01, 0.21) *** | |||
| Delayed % | 69.2 | 7.4 | 37.7 | |
| Typical % | 26.9 | 70.4 | 49.1 | |
| Fast % | 3.8 | 22.2 | 13.2 | |
| Self-help development | 0.17^(0.05, 0.63) ** | |||
| Delayed % | 46.2 | 3.7 | 24.5 | |
| Typical % | 42.3 | 85.2 | 64.2 | |
| Fast % | 11.5 | 11.1 | 11.3 | |
| Biological parents | X2 2.25 | |||
| Yes % | 92.0 | 100.0 | 96.2 | |
| No—adopted % | 8.0 | 0 | 3.8 | |
| Parental marital status | 3.85^(0.89, 16.55) | |||
| Married % | 68.0 | 88.9 | 78.8 | |
| Separated % | 16.0 | 7.4 | 11.5 | |
| Divorced % | 16.0 | 3.7 | 9.6 | |
| Parental psychological distress b | X2 0.01 | |||
| Yes % | 16.0 | 14.8 | 15.4 | |
| No % | 84.0 | 85.2 | 84.6 | |
| Parental education | 0.19^(0.06, 0.58) ** | |||
| Secondary school % | 44.0 | 18.5 | 30.8 | |
| Diploma % | 12.0 | 0 | 5.8 | |
| Undergraduate degree % | 36.0 | 44.4 | 40.4 | |
| Postgraduate degree % | 8.0 | 37.0 | 23.1 |
| DLD (n = 26) | TLD (n = 27) | F | p | ηp2 | |
|---|---|---|---|---|---|
| Spatial Reasoning a | 8.15 (2.84) | 11.89 (2.47) | 19.64 | <0.001 | 0.29 |
| Expressive Language b | 4.92 (2.93) | 9.93 (2.96) | 29.21 | <0.001 | 0.38 |
| Receptive Language c | 6.04 (2.92) | 13.00 (2.39) | 67.27 | <0.001 | 0.58 |
| DLD | TLD | DLD vs. TLD | Effect Size | |
|---|---|---|---|---|
| Self-report | ||||
| Best Friend | X2 3.20, n.s. | |||
| Yes (%) | 84.6 | 63.0 | - | |
| No (%) | 15.4 | 37.0 | ||
| Argue with friends | X2 5.64 * | Φ − 0.33 | ||
| Yes (%) | 46.2 | 77.8 | ||
| No (%) | 53.8 | 22.2 | ||
| Member of social clubs | X2 8.27 ** | Φ − 0.40 | ||
| Yes (%) | 65.4 | 96.3 | ||
| No (%) | 34.6 | 3.7 | ||
| Victim of bullying | X2 0.96, n.s. | - | ||
| Yes (%) | 61.5 | 48.1 | ||
| No (%) | 38.5 | 51.9 | ||
| Bully others | X2 2.18, n.s. | - | ||
| Yes (%) | 7.7 | 22.2 | ||
| No (%) | 92.3 | 77.8 | ||
| Perceived Social Support—Friendship Scale (PSS-Fr) | 11.15 (3.71) | 11.22 (2.65) | −0.13[−1.98, 1.71] n.s. | - |
| Parent-report | ||||
| SDQ Peer Problems | 3.31 (2.53) | 1.04 (1.56) | 1.11[0.43, 1.80] ** | d −1.09[−1.67, −0.51] *** |
| DLD | TLD | DLD vs. TLD | Cohen’s d [95% CI] | |
|---|---|---|---|---|
| Self-report | ||||
| Warwick Edinburgh Mental Wellbeing Scale (WEMWBS) | 51.96 (9.28) | 54.22 (6.52) | −1.27[−7.61, 2.19] n.s. | 0.28[−0.26, 0.82] |
| Revised Children’s Manifest Anxiety Scale (RCMAS) | 20.54 (15.77) | 12.93 (10.53) | 0.87[−0.15, 1.89] n.s. | −0.46[−1.0, −0.09] |
| Moods and Feelings Questionnaire (MFQ) | 14.65 (14.14) | 9.00 (9.46) | 0.48[−0.62, 1.58] n.s. | −0.27[−0.81, 0.27] |
| Parent-report | ||||
| SDQ Emotional Problems | 3.54 (2.97) | 1.63 (2.06) | 0.83[0.15, 1.50] * | −0.75[−1.30, −0.20] ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forrest, C.L.; Gibson, J.L.; St Clair, M.C. Social Functioning as a Mediator between Developmental Language Disorder (DLD) and Emotional Problems in Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 1221. https://doi.org/10.3390/ijerph18031221
Forrest CL, Gibson JL, St Clair MC. Social Functioning as a Mediator between Developmental Language Disorder (DLD) and Emotional Problems in Adolescents. International Journal of Environmental Research and Public Health. 2021; 18(3):1221. https://doi.org/10.3390/ijerph18031221
Chicago/Turabian StyleForrest, Claire L., Jenny L. Gibson, and Michelle C. St Clair. 2021. "Social Functioning as a Mediator between Developmental Language Disorder (DLD) and Emotional Problems in Adolescents" International Journal of Environmental Research and Public Health 18, no. 3: 1221. https://doi.org/10.3390/ijerph18031221
APA StyleForrest, C. L., Gibson, J. L., & St Clair, M. C. (2021). Social Functioning as a Mediator between Developmental Language Disorder (DLD) and Emotional Problems in Adolescents. International Journal of Environmental Research and Public Health, 18(3), 1221. https://doi.org/10.3390/ijerph18031221