
Access to Healthcare Following Serious Injury: Perspectives of Allied Health Professionals in Urban and Regional Settings



Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Recruitment Strategy
2.3. Data Collection
2.4. Data Analysis
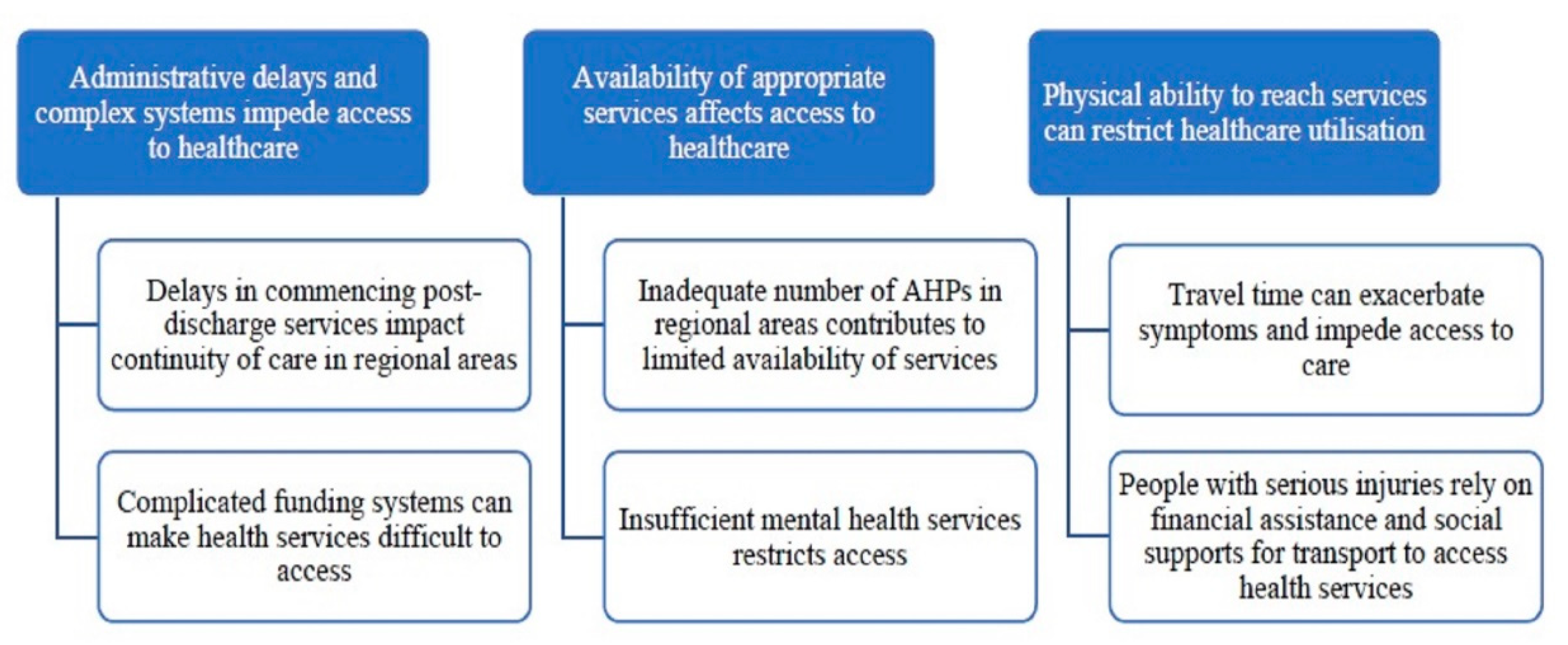
3. Results
3.1. Administrative Delays and Complex Systems Impede Access to Healthcare
3.1.1. Delays in Commencing Post-Discharge Services Impact Continuity of Care in Regional Areas
“The clients I see in the country … they take months to get a team organised after discharge … In the city that would happen in a week.”ID 14_Statewide_Other_F_37-43
“… unfortunately, the most common scenario is that the referral from the metro hospital hasn’t been activated … So they’ve been discharged from hospital, sent back to [regional town] and then no follow-up rehab has happened … we would see those guys potentially four, five, unfortunately sometimes six months post-accident.”* ID17_Regional_EP_M_30-36
3.1.2. Complicated Funding Systems Can Make Health Services Difficult to Access
“… every different agency is so different, and that’s the frustration. There are all different policies and procedures, and it always seems a lot harder to provide the services with [Injury_Insurer_1].”ID15_Urban_OT_F_30–36
“Since [Injury_Insurer_2] changed their funding model to moving to a pre-approved approach has been really beneficial for patients and for the therapy team … We know we can put together a program and not be placing our organisation at financial risk, and putting the patient under extra stress to say we have to wait for things to be approved.”ID22_Regional_PT_M_37–43
“I think if those sorts of [NDIS] services aren’t flexible enough from a funding perspective to allow quick access to funds, and things like that, that you end up fighting tooth and nail just to get someone what they’re actually entitled to.”ID24_Regional_OT_F_37–43
3.2. Availability of Appropriate Services Affects Access to Healthcare
3.2.1. Inadequate Number of AHPs in Regional Areas Contributes to Limited Availability of Services
“… physios are booked out for weeks in advance, but someone needs intensive physiotherapy … obviously [physiotherapy] is an existing resource, you’re still always scraping for appointments in a timely manner. That goes for all allied health. The speech therapist has waiting lists, the dietetics have waiting lists. Sorry, everyone has waiting lists.”ID7_Regional_Other_F_30–36
“… there’s not enough therapists in that town, or their therapists that don’t have the level of expertise that they might need for their really complex therapy needs.”* ID12_Statewide_PT_F_30–36
“when you’re dealing with more complex patients there will be a lot of different [medical specialists] involved … which can be a little bit more challenging, because you’re going to have to wait til they travel out this way from a bigger hub, or patients have to travel a long way to get to them, and often wait a long time to see them.”ID2_Regional_EP_M_23–29
3.2.2. Insufficient Mental Health Services Restricts Access
“… that’s a real key, that if clients were provided with the emotional support and the psychological support right from the word go, and that ability for them to be able to accept their injury, and work with the allied health professionals, then they would have much more positive outcomes.”* ID8_Regional_OT_F_44–51
“navigating (GP) mental health care plans … even the Medicare rebate in psychology is out of reach for a lot of people … then there is still a huge gap for each appointment. That’s not achievable for a lot of people.”* ID7_Regional_Other_F_30–36
“And the country clients are really disjointed … there are no neuropsyches in the country. It’s crazy, they fund me 3½ hours, 4 h to drive each way to see a client because there’s no-one closer … it’s completely nuts.”ID14_Statewide_Other_F_37–43
3.3. Physical Ability to Reach Services Can Restrict Healthcare Utilisation
3.3.1. Travel Time Can Exacerbate Symptoms and Impede Access to Healthcare
“A lot of clients talk about how hard [travelling to Melbourne] is, whether it’s because of pain … [the travel] brings up a lot of anxiety for them …”ID19_Urban_PT_F_30–36
“there’s problems when the patients go back to the acute hospitals, to the big trauma hospitals in the city, for reviews and plans … a lot of people from the country don’t like going up to the big city, or the big city hospitals, they find it really stressful and annoying.”* ID3_Urban_Other_F_37–43
“I think telehealth can play a much bigger part in [medical reviews] … But it’s really hard to get specialists to consider telehealth as an option.”ID19_Urban_PT_F_30–36
3.3.2. People with Serious Injuries Rely on Financial Assistance and Social Support for Transport to Access Health Services
“A lot of our clients have to travel. And because a lot of them are waiting compensation claims, or awaiting trying to get on the [disability support pension]. Their finances are in a pretty poor state … a lot of them will not go to appointments, or not schedule appointments because of the costs of travelling to Melbourne to see those specialists.”ID4_Regional_OT_F_37–43
“I’ve got elderly people catching public transport, which is really inappropriate… We’ve got people that just don’t go down to their follow-up appointments because they literally can’t get down there.”ID7_Regional_Other_F_30–36
“The NDIS pays for vehicle modifications, but for someone who requires a van to get around… sometimes that’s just too expensive for the participant to buy, so they have no way of accessing the local community … they’re very limited.”ID12_Statewide_PT_F_30–36
“[For compensable patients] I think there’s more available services because by funding carers and trainers you can get access to community facilities that are setup, and the carer can provide the support in that facility, which a non-compensable patient struggles to access.”ID10_Urban_PT_F_51+
“We have issues with transport at our repat campus. We have volunteer transport at [urban_health_service], which makes it a lot easier for us for clients to access our services.”ID10_Urban_PT_F_51+
“I’ve got a client in [regional town] … [Injury_Insurer_2] will say we’ll fund you a taxi transport to get to your appointment. Well, there is no taxi there …”* ID14_Statewide_Other_F_37–43
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Interview Topic Guide
Appendix A.1. Participant Attributes
- Age;
- Gender;
- Profession;
- Job title (manager/senior/junior);
- Years of experience as a health professional;
- Years of experience in current role;
- Public or private setting;
- Treatment of compensable patients, yes/no;
- Geographic remoteness region;
- Postcode of health facility.
Appendix A.2. Introduction
Appendix A.3. The Injured Patients
- What are your experiences with treating trauma patient’s post-hospital discharge? Probe: Have you experienced any particularly complex or difficult patients?
- What type/s of seriously injured patients do you treat? Probe: multiple orthopaedic trauma; TBI; SCI; falls.
Appendix A.4. Treatment of Injuries
- Can you tell me about the types of treatment and services that you offer to seriously injured patients? How do you feel about providing care to seriously injured patients?
- What information or advice did you receive about your patient’s injury? Is there any other information would you have liked to receive and from who?
- What supports are available to you when you need advice on or assistance with treating a seriously injured patient?
- Do you feel that the service you provide are able to meet the needs of your patients? How could they be improved?
- What other services do you feel are required in your local area to better meet the needs of injured patients?
Appendix A.5. Resources
- What resources are available to you when caring for seriously injured patients?
- What additional resources do you feel would enable you improve the care of seriously injured patients, if any?
- Can you tell me about your experiences in receiving support from more experienced clinicians or a time you have provided support for more isolated services providers?
Appendix A.6. Experience with Funding Bodies
- Do you provide care for seriously injured patients who are funded by injury insurers for their injury?
- Can you tell us about your experiences with compensable funding bodies?
- Have your experiences with these injury insurers changed over time?
- Is there anything you feel could be done differently by injury insurers to help your patient’s recovery?
- Is there anything the injury insurers could do differently to work effectively with service providers?
Appendix A.7. General
- How do you feel about being able to ensure adequate continuity of care between acute hospitals and your service?
- Can you tell me about your experiences with other services or policies relating to optimising different aspects of your patients care? For example, health, transportation, disability or rehabilitation for your patients?
- What else can you tell me about trauma care in your community, specific issues you face, and barriers or facilitators to optimal care for seriously injured patients?
Appendix A.8. Concluding
- Do you have anything else you would like to add or is there anything that I have not covered that you thought I should?
- Do you have any questions about what we have discussed?
Appendix B. Additional Supporting Quotes
Appendix B.1. Administrative Delays and Complex Systems Impede Access to Healthcare
“… unfortunately, the most common scenario is that the referral from the metro hospital hasn’t been activated, so whether it’s been lost or not sent through in a timely way. So they’ve been discharged from hospital, sent back to [regional town] and then no follow-up rehab has happened… we would see those guys potentially four, five, unfortunately sometimes six months post-accident. Probably not six months, maybe more like four months. It’s more common to get that than a direct referral from a metro hospital in the orthopaedic and pain rehab clinics especially. That’s not so the case for spinal clinic, the referrals for spinal tend to be a little bit more successful in getting from metro to Bendigo.”ID17, Regional, EP, M, 30–36
“… making things a little bit more kind of user-friendly so the patients can actually access what they want. I think that’s sort of part of the benefit to the NDIS is having a bit more of that decision-making, like empowering the patient, but if the system is too complicated for them to be able to navigate, then it just puts that same barrier backup that the NDIS is trying to address.”ID2, Regional, EP, M, 23–29
“Claims with [Injury Insurer 1] … they still require a lot more information than what [Injury Insurer 2] does have, there’s a lot more report writing … giving them every inch or millimetre of information to get things approved.”ID8, Regional, OT, F, 44–51
Appendix B.2. Availability of Appropriate Services Affects Access to Healthcare
“Because we have a lot of clients in the community who live in a town, they might have huge personal care needs, but those needs aren’t being met because there’s not enough carers in the town that they live in. So they’re missing out on services that way, or there’s not enough therapists in that town, or their therapists that don’t have the level of expertise that they might need for their really complex therapy needs. So it is a challenge for sure.”ID12, Statewide, PT, F, 30–36
“… that’s a real key, that if clients were provided with the emotional support and the psychological support right from the word go, and that ability for them to be able to accept their injury, and work with the allied health professionals, then they would have much more positive outcomes…I think the key things are the people that have had traumatic events need to be provided with services to deal with their psychological and emotional health, which isn’t being done effectively at the moment. Their care services need to be improved in this area.”ID8, Regional OT, F, 44–51
“Psychology would also be really helpful for the team, but we, as I said, just have the neuropsyche, and largely assessment based. At the moment psychology just has to be through GP, getting onto a (mental health) care plan. There sort of used to be a tiny bit of access we could get through the hospital for people who had been seen by hospital psychologists. But it’s pretty little access now.”ID6, Urban, PT, F, 22–29
“There’s a real gap with social work services in our community, and even access in psychology. Because even the Medicare rebate in psychology is out of reach for a lot of people. Navigating mental health plans, but also then there is still a huge gap, like you’re talking 60, 80 a hundred dollar gap for each psychology appointment. That’s not achievable for a lot of people.”ID7, Regional, Other, F, 30–36
Appendix B.3. Physical Ability to Reach Services Can Restrict Healthcare Utilisation
“Transportation is a real issue for a lot of people. And that has a flow-on effect for things like being able to attend therapy appointments. A lot of small towns don’t have maxi taxis, and all of our clients need maxi taxis to get around, if they don’t have their own wheelchair accessible vans and things like that. So it is really challenging for a lot of the rural and regional clients.”ID12, Statewide, PT, F, 30–36
I’ve got a client in [regional town] … [Injury Insurer 2] will say we’ll fund you a taxi transport to get to your appointment. Well, there is no taxi there. Everything’s just much harder for them. They can’t just jump in a taxi or a train, or whatever, to get to see a doctor because firstly, they’re three hours away, and they don’t have taxis out in these areas sometimes.”ID14, Statewide, Other, F, 37–43
“There’s problems when the patients go back to the acute hospitals, to the big trauma hospitals in the city, for reviews and plans and all that kind of thing, and probably 50 per cent of the time the communication back from there is not very good. And so that leads to anxiety and concern about what’s going on. And a lot of people from the country don’t like going up to the big city, or the big city hospitals, they find it really stressful and annoying …”ID3, Urban, Other, F, 37–43
References
- Evans, D.B.; Hsu, J.; Boerma, T. Universal Health Coverage and Universal Access; World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- Caplan, B.; Bogner, J.; Brenner, L.; Simpson, G.K.; Daher, M.; Hodgkinson, A.; Strettles, B. Comparing the injury profile, service use, outcomes, and comorbidities of people with severe TBI across urban, regional, and remote populations in New South Wales: A multicentre study. J. Head Trauma Rehab. 2016, 31, E26–E38. [Google Scholar]
- Braaf, S.; Ameratunga, S.; Christie, N.; Teague, W.J.; Ponsford, J.; Cameron, P.A.; Gabbe, B.J. Care coordination experiences of people with traumatic brain injury and their family members in the 4-years after injury: A qualitative analysis. Brain Inj. 2019, 33, 574–583. [Google Scholar] [CrossRef] [Green Version]
- Gabbe, B.J.; Sleney, J.S.; Gosling, C.M.; Wilson, K.; Hart, M.J.; Sutherland, A.M.; Christie, N. Patient perspectives of care in a regionalised trauma system: Lessons from the Victorian State Trauma System. Med. J. Aust. 2013, 198, 149–152. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Simpson, P.M.; Cameron, P.A.; Ponsford, J.; Lyons, R.A.; Collie, A.; Fitzgerald, M.C.; Judson, R.; Teague, W.J.; Braaf, S.; et al. Long-term health status and trajectories of seriously injured patients: A population-based longitudinal study. PLoS Med. 2017, 14, e1002322. [Google Scholar] [CrossRef]
- Braaf, S.; Ameratunga, S.; Ponsford, J.; Cameron, P.; Collie, A.; Harrison, J.; Ekegren, C.; Christie, N.; Nunn, A.; Gabbe, B. Traumatic injury survivors’ perceptions of their future: A longitudinal qualitative study. Disabil. Rehabil. 2020, 42, 2707–2717. [Google Scholar] [CrossRef]
- Christie, N.; Braaf, S.; Ameratunga, S.; Nunn, A.; Jowett, H.; Gabbe, B. The role of social networks in supporting the travel needs of people after serious traumatic injury: A nested qualitative study. J. Transp. Health 2017, 6, 84–92. [Google Scholar] [CrossRef]
- Keeves, J.; Braaf, S.C.; Ekegren, C.L.; Beck, B.; Gabbe, B.J. Caring for people with serious injuries in urban and regional communities: A qualitative investigation of healthcare providers’ perceptions. Disabil. Rehabil. 2020, 1–9. [Google Scholar] [CrossRef]
- Levesque, J.F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [Green Version]
- Christie, N.; Beckett, K.; Earthy, S.; Kellezi, B.; Sleney, J.; Barnes, J.; Jones, T.; Kendrick, D. Seeking support after hospitalisation for injury: A nested qualitative study of the role of primary care. Br. J. Gen. Pr. 2015, 66, e24–e31. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.; Amatya, B.; Hoffman, K. Systematic review of multidisciplinary rehabilitation in patients with multiple trauma. BJS 2012, 99, 88–96. [Google Scholar] [CrossRef]
- Ruseckaite, R.; Gabbe, B.J.; Vogel, A.P.; Collie, A. Health care utilisation following hospitalisation for transport-related injury. Injury 2012, 43, 1600–1605. [Google Scholar] [CrossRef]
- Beckett, K.; Earthy, S.; Sleney, J.; Barnes, J.; Kellezi, B.; Barker, M.; Clarkson, J.; Coffey, F.; Elder, G.; Kendrick, D.; et al. Providing effective trauma care: The potential for service provider views to enhance the quality of care (qualitative study nested within a multicentre longitudinal quantitative study). BMJ Open 2014, 4, e005668. [Google Scholar] [CrossRef] [Green Version]
- Statistics, A.B.o. Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure, July 2011. 2013. Available online: http://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/A277D01B6AF25F64CA257B03000D7EED/$File/1270055005_july%202011.pdf (accessed on 13 October 2020).
- Australian Bureau of Statistics. Regional Population Growth, Australia, 2017–2018. 2019. Available online: www.abs.gov.au/ausstats/[email protected]/0/B7616AB91C66CDCFCA25827800183B7B?Opendocument (accessed on 9 July 2020).
- Victorian State Trauma Outcome Registry Monitoring Group (VSTORM). Victorian State Trauma Registry Annual Report V3 2017–2018; VSTORM: Melbourne, Australia, 2019. [Google Scholar]
- Purcal, C.; Fisher, K.R.; Meltzer, A. Social insurance for individualised disability support: Implementing the Australian National Disability Insurance Scheme (NDIS). Soc. Policy Rev. 2016, 28, 173–190. [Google Scholar] [CrossRef]
- Tongco, M.D.C. Purposive Sampling as a Tool for Informant Selection. Ethnobot. Res. Appl. 2007, 5, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Australia, A.H.P. What Is Allied Health? 2020. Available online: https://ahpa.com.au/what-is-allied-health/ (accessed on 22 October 2020).
- Auatralian Government Department of Health. All Registered Health Practitioners 2019. Health Workforce Data 2020. Available online: https://hwd.health.gov.au/summary.html#part-3 (accessed on 22 October 2020).
- Sandelowski, M. Sample size in qualitative research. Res. Nurs. Health 1995, 18, 179–183. [Google Scholar] [CrossRef]
- Eatough, V.; Smith, J.A. Interpretative phenomenological analysis. In Handbook of Qualitative Research in Psychology; The Sage: London, UK, 2008; Volume 179, p. 194. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V.; Hayfield, N.; Terry, G. Thematic Analysis. In Handbook of Research Methods in Health Social Sciences; Springer: Singapore, 2019; pp. 843–860. [Google Scholar] [CrossRef]
- Maxwell, J. Understanding and Validity in Qualitative Research. Harv. Educ. Rev. 1992, 62, 279–301. [Google Scholar] [CrossRef] [Green Version]
- Morse, J.M. Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual. Health. Res. 2015, 25, 1212–1222. [Google Scholar] [CrossRef]
- Creswell, J.W.; Poth, C.N. Qualitative inquiry and research design. In Choosing among Five Approaches; Sage Publications: London, UK, 2016. [Google Scholar]
- Cornish, F.; Gillespie, A.; Zittoun, T. Collaborative analysis of qualitative data. In The Sage Handbook of Qualitative Data Analysis; Sage Publications Ltd.: London, UK, 2013; pp. 79–93. [Google Scholar]
- Robards, F.; Kang, M.; Steinbeck, K.S.; Hawke, C.; Jan, S.; Sanci, L.; Liew, Y.Y.; Kong, M.; Usherwood, T. Health care equity and access for marginalised young people: A longitudinal qualitative study exploring health system navigation in Australia. Int. J. Equity Health 2019, 18, 41. [Google Scholar] [CrossRef] [Green Version]
- Braaf, S.; Ameratunga, S.; Nunn, A.; Christie, N.; Teague, W.J.; Judson, R.; Gabbe, B.J. Patient-identified information and communication needs in the context of major trauma. BMC Health. Serv. Res. 2018, 18, 163. [Google Scholar] [CrossRef]
- Foster, M.; Henman, P.; Tilse, C.; Fleming, J.; Allen, S.; Harrington, R. ‘Reasonable and necessary’ care: The challenge of operationalising the NDIS policy principle in allocating disability care in Australia. Aust. J. Soc. Issues 2016, 51, 27–46. [Google Scholar] [CrossRef]
- Roufeil, L.; Lipzker, A. Psychology Services in Rural and Remote Australia; InPsych, The Bulletin of the Australian Psychological Society Ltd.: Melbourne, Australia, 2007; Volume 29, p. 8. [Google Scholar]
- Chapman, J.E.; Ponsford, J.; Bagot, K.L.; Cadilhac, D.A.; Gardner, B.; Stolwyk, R.J. The use of videoconferencing in clinical neuropsychology practice: A mixed methods evaluation of neuropsychologists’ experiences and views. Aust. Psychol. 2020, 55, 618–633. [Google Scholar] [CrossRef]
- Langarizadeh, M.; Tabatabaei, M.S.; Tavakol, K.; Naghipour, M.; Moghbeli, F. Telemental Health Care, an Effective Alternative to Conventional Mental Care: A Systematic Review. Acta Inform. Medica 2017, 25, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Gabbe, B.J.; Sleney, J.S.; Gosling, C.M.; Wilson, K.; Sutherland, A.; Hart, M.; Watterson, D.; Christie, N. Financial and employment impacts of serious injury: A qualitative study. Injury 2014, 45, 1445–1451. [Google Scholar] [CrossRef]
- Robards, F.; Kang, M.; Usherwood, T.; Sanci, L. How Marginalized Young People Access, Engage with, and Navigate Health-Care Systems in the Digital Age: Systematic Review. J. Adolesc. Health 2018, 62, 365–381. [Google Scholar] [CrossRef]
- Lowe, M.; Boulangé, C.; Giles-Corti, B. Urban design and health: Progress to date and future challenges. Health Promot. J. Aust. 2014, 25, 14–18. [Google Scholar] [CrossRef]
- Schulz, T.R.; Long, K.; Kanhutu, K.; Bayrak, I.; Johnson, D.; Fazio, T. Telehealth during the coronavirus disease 2019 pandemic: Rapid expansion of telehealth outpatient use during a pandemic is possible if the programme is previously established. J. Telemed. Telecare 2020. [Google Scholar] [CrossRef]
- Hunt, G.; Michael, K. COVID-19: Whole of Population Telehealth for Patients, General Practice, Primary Care and Other Medical Services; Department of Health: Canberra, Australia, 2020. [Google Scholar]
- Thornton, J. Covid-19: How coronavirus will change the face of general practice forever. BMJ 2020, 368, m1279. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T.; Koh, G.C.H.; Car, J. Covid-19: A remote assessment in primary care. BMJ 2020, 368, m1182. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The Role of Telehealth in Reducing the Mental Health Burden from COVID-19. Telemed. e-Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Bashshur, R.L.; Doarn, C.R.; Frenk, J.M.; Kvedar, J.C.; Woolliscroft, J.O. Telemedicine and the COVID-19 Pandemic, Lessons for the Future. Telemed. e-Health 2020, 26, 571–573. [Google Scholar] [CrossRef] [Green Version]
- Fisk, M.; Livingstone, A.; Pit, S.W. Telehealth in the Context of COVID-19: Changing Perspectives in Australia, the United Kingdom, and the United States. J. Med. Internet Res. 2020, 22, e19264. [Google Scholar] [CrossRef]
- Coyne, I.T. Sampling in qualitative research. Purposeful and theoretical sampling; merging or clear boundaries? J. Adv. Nurs. 1997, 26, 623–630. [Google Scholar] [CrossRef] [Green Version]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? An experiment with data saturation and variability. Field Methods 2006, 18, 59–82. [Google Scholar] [CrossRef]
- Miedema, B.; Easley, J.K. Comparing urban and rural young adult cancer survivors’ experiences: A qualitative study. Rural Remote Health 2013, 13, 225. [Google Scholar]
- Logan, T.K.; Walker, R.; Cole, J.; Ratliff, S.; Leukefeld, C. Qualitative Differences among Rural and Urban Intimate Violence Victimization Experiences and Consequences: A Pilot Study. J. Fam. Violence 2003, 18, 83–92. [Google Scholar] [CrossRef]
- Leung, L. Validity, reliability, and generalizability in qualitative research. J. Fam. Med. Prim. Care 2015, 4, 324–327. [Google Scholar] [CrossRef]


{kind=link}
| Strategy | Method of Implementation |
|---|---|
| Descriptive validity | The interviews were listened to and transcripts read and referred to multiple times. The initial five transcripts were coded by two investigators (J.K. and S.C.B.) to develop the coding framework [25]. |
| Negative case analysis | Any cases that were considered outliers were discussed by the authors [26]. |
| Peer review | Presentation and feedback from peers/colleagues. Authors regularly met to discuss the research design, develop the thematic framework and interpret the analysis [27]. |
| Researcher triangulation | Researcher triangulation involved the use of two researchers in the coding and analysis phases of the research. Authors met weekly to discuss the development of the coding framework, themes, interpretation of the results and recommendations developed from this research [28]. |
| Researcher subjectivity | Researcher positionality discussed to identify potential bias, reflection following each interview and early ideas about a coding framework. Further reflection and documentation continued through development and reporting of findings [28]. |
| Characteristic | n (%) | |
|---|---|---|
| Age, years (mean (SD)) | 36.2 (8.5) | |
| Gender | Male | 8 (32) |
| Female | 17 (68) | |
| Profession | Physiotherapist | 13 (52) |
| Occupational therapist | 5 (20) | |
| Exercise physiologist | 4 (16) | |
| Other a | 3 (12) | |
| Years of clinical experience | 1–4 | 4 (16) |
| 5–9 | 9 (36) | |
| 10–14 | 4 (16) | |
| 15+ | 7 (28) | |
| Healthcare setting | Hospital outpatients | 16 (64) |
| Community based | 6 (24) | |
| Private practice | 3 (12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keeves, J.; Braaf, S.C.; Ekegren, C.L.; Beck, B.; Gabbe, B.J. Access to Healthcare Following Serious Injury: Perspectives of Allied Health Professionals in Urban and Regional Settings. Int. J. Environ. Res. Public Health 2021, 18, 1230. https://doi.org/10.3390/ijerph18031230
Keeves J, Braaf SC, Ekegren CL, Beck B, Gabbe BJ. Access to Healthcare Following Serious Injury: Perspectives of Allied Health Professionals in Urban and Regional Settings. International Journal of Environmental Research and Public Health. 2021; 18(3):1230. https://doi.org/10.3390/ijerph18031230
Chicago/Turabian StyleKeeves, Jemma, Sandra C. Braaf, Christina L. Ekegren, Ben Beck, and Belinda J. Gabbe. 2021. "Access to Healthcare Following Serious Injury: Perspectives of Allied Health Professionals in Urban and Regional Settings" International Journal of Environmental Research and Public Health 18, no. 3: 1230. https://doi.org/10.3390/ijerph18031230