Experience and Health-Related Behavior in Times of the Corona Crisis in Germany: An Exploratory Psychological Survey Considering the Identification of Compliance-Enhancing Strategies


Abstract
:1. Introduction
2. Theoretical Background
2.1. Health Beliefs and Behavior
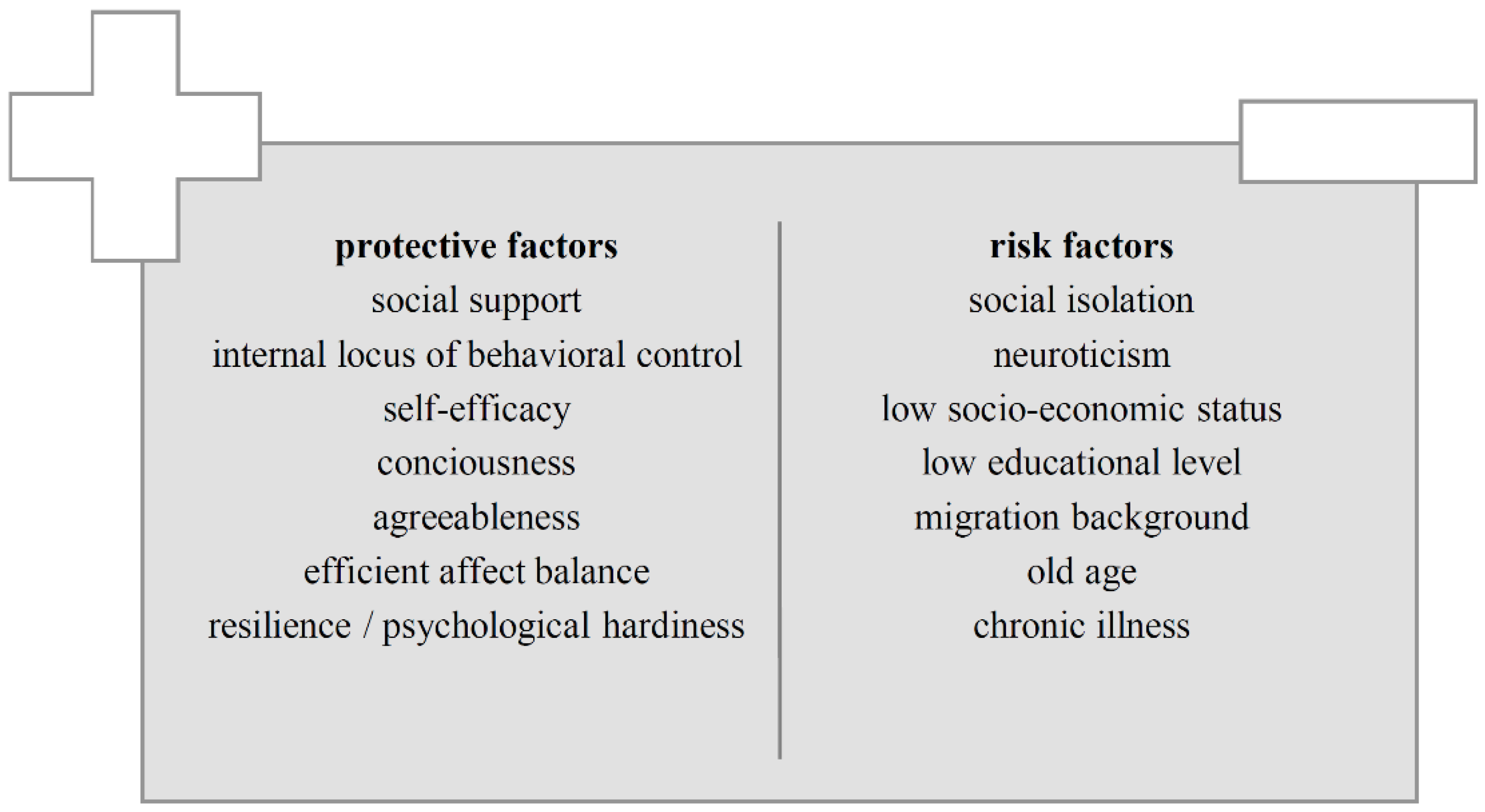
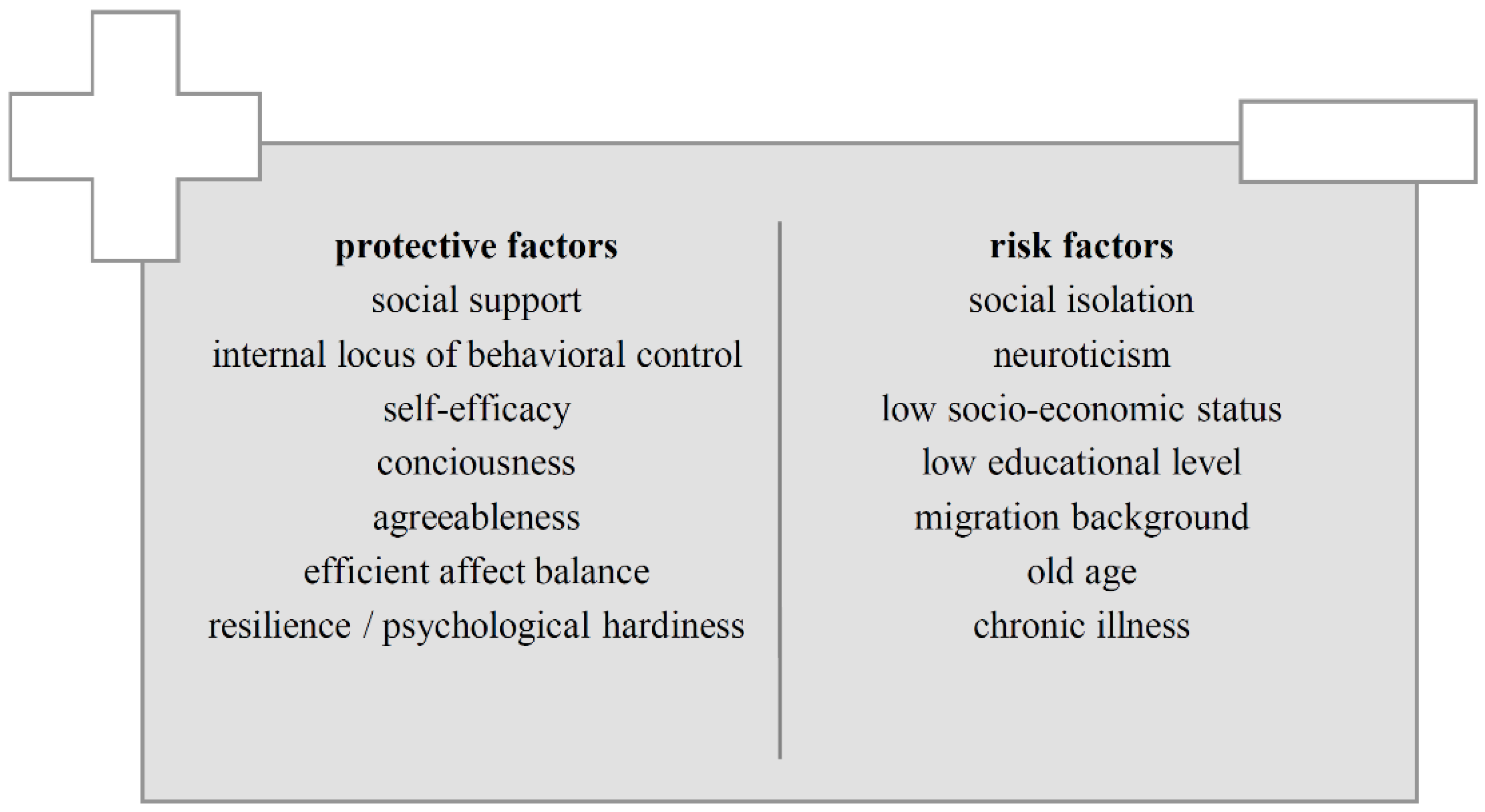
- Perceived severity and vulnerability: First, people perceive a general health risk, then take preventive measures to reduce this risk; for example, many people do sports to reduce the risk of overweight or cardiovascular diseases. In addition, the likelihood of preventive behavior is further increased if people consider themselves to be at specific risk, for example, because there is corresponding previous illness in their family.
- Perceived benefits of behavior modification and low barriers: Furthermore, if a certain preventive behavior is regarded as actually effective in minimizing personal risk, this again increases the probability of corresponding behavioral performance. Finally, potential barriers and the effort involved in preventive behavior should be assessed as low as possible in order to increase the likelihood of its realization.
2.2. Preventive Behavior in Times of the COVID-19 Pandemic
- In the case of COVID-19, its extensive health-damaging potential was recognized and communicated in its entirety. Based on the previous and still incomplete data situation, the mortality risk for COVID-19 is estimated to be several times higher compared to seasonal influenza [32].
- The effectiveness of the preventive measures may well be confirmed, since flattened curves of the infection numbers could be observed after these measures came into force. The risk of a droplet or smear infection with COVID-19 seems to be drastically reduced, especially due to the social contact restrictions and strict compliance with hygiene practice [3,5,32].
- Regarding the estimation of required individual effort in order to perform preventive behavior, two classes of preventive measures must be distinguished first: (a) those who ask to practice additional behavior and (b) those who ask to refrain from habitual behavior patterns. The first category includes relatively inexpensive and time-efficient measures (such as regular thorough hand washing, use of disinfectants, wearing face masks) and is therefore associated with comparatively little behavioral effort. Regarding the second category, from a physical point of view it can be stated that it is energetically favorable to refrain from doing something rather than to do it. Regardless of these advantages however, the ‘costs’ of such an omission must always be considered, which—in the case of social isolation for example—could again act as a health risk factor.
3. Objectives
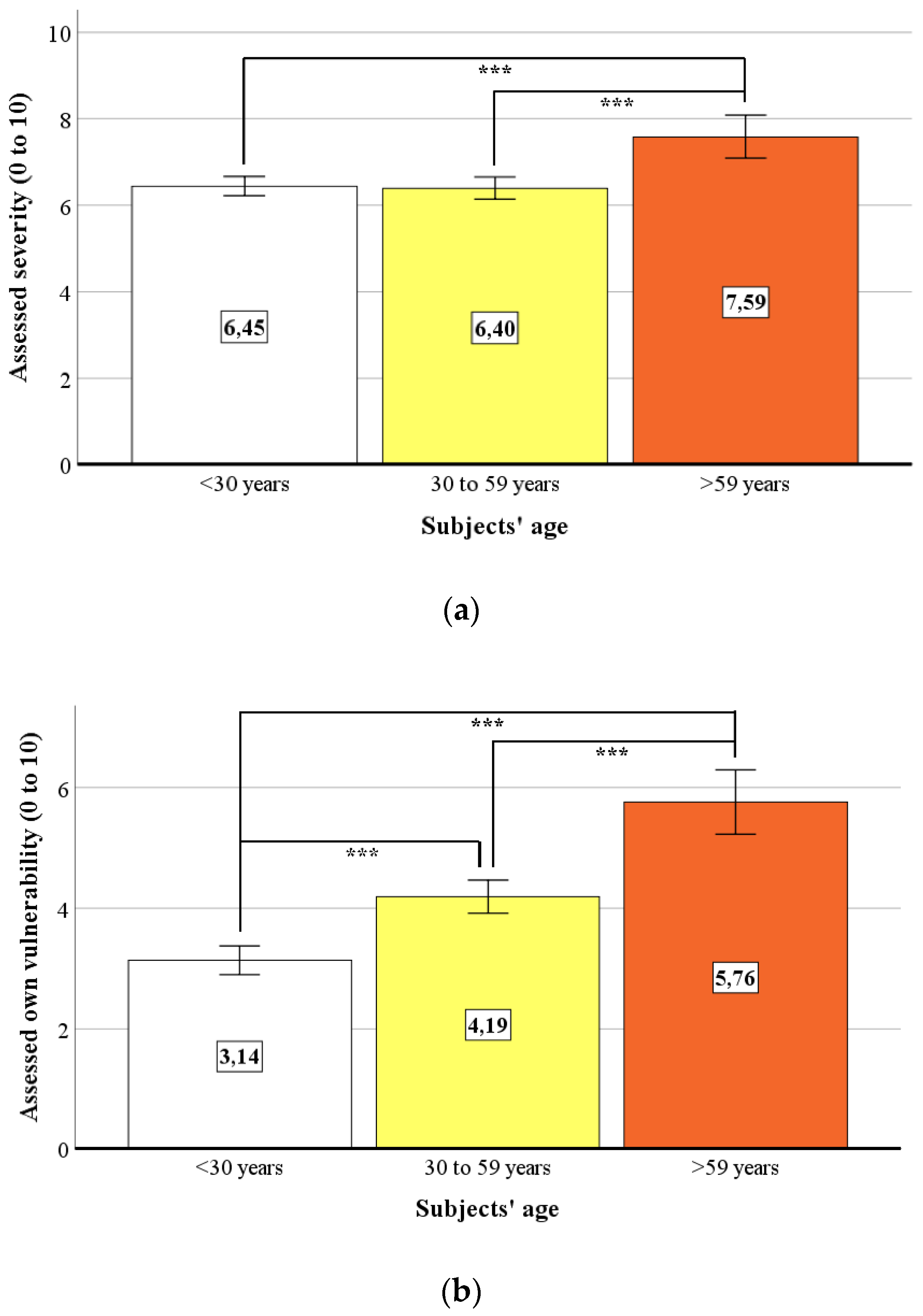
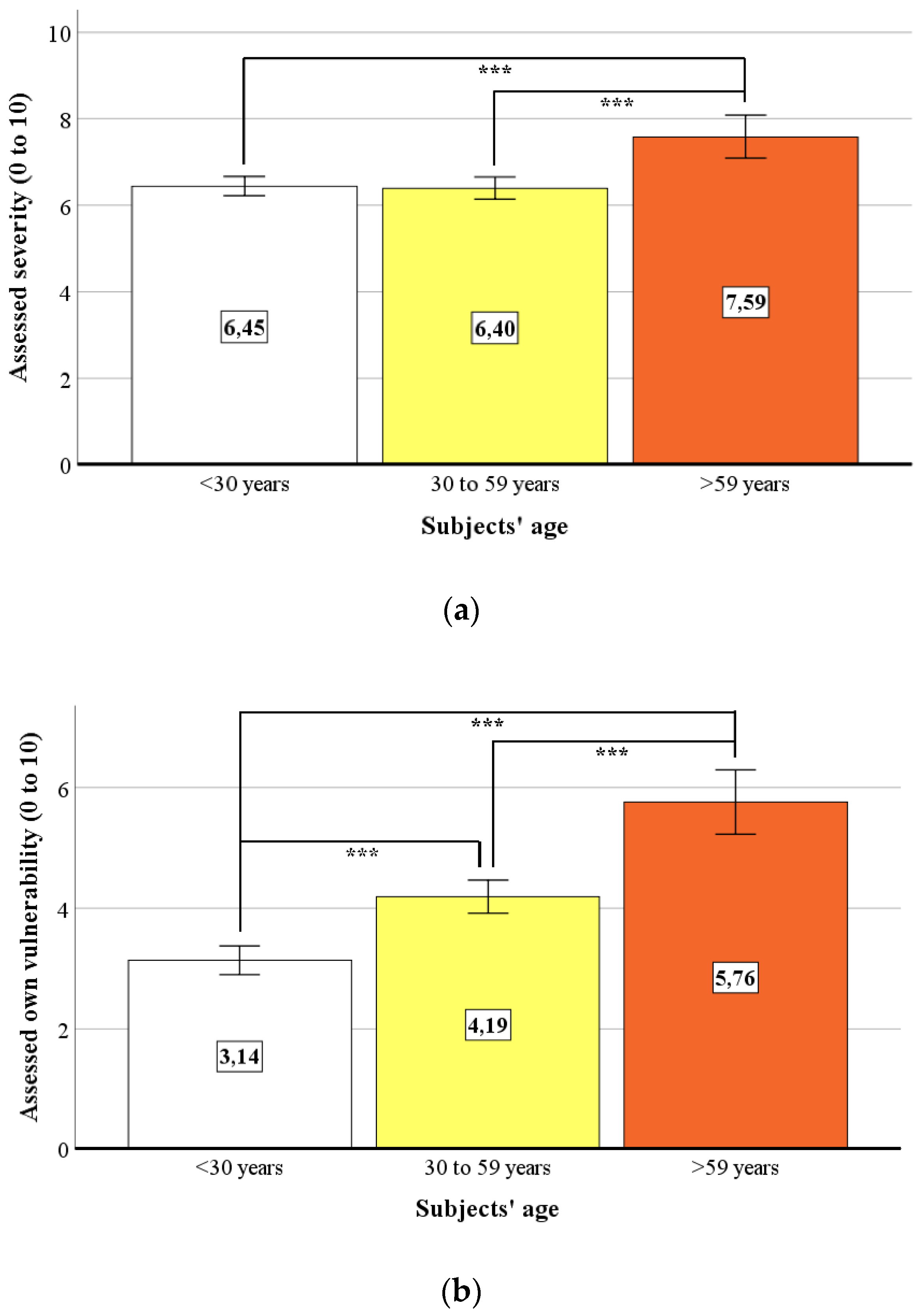
- How does our sample assess the severity of COVID-19 and its own vulnerability to an infection in terms of the HBM? Is there an optimistic bias regarding the assessment of one’s own risk of infection compared to the risk of other people?
- What and how many behavioral preventive measures are taken to protect oneself and others from an infection with COVID-19? Does the extent of the preventive behavior vary systematically between different subgroups of persons (e.g., between different ages or marital status) or are there relevant associations with other characteristics (e.g., affective or personality characteristics, satisfaction with information available, or the political management of COVID-19)?
- Is there any evidence that either the extent of the preventive behavior shown and/or other variables relevant to health behavior changed during our four-week period of investigation?
- What quality of affect balance can be determined in times of the COVID-19 pandemic compared to times before?
- Based on exploratory correlational analyses between all captured variables relevant to health behavior, can specific central clusters be identified, which can serve as effective starting points for designing public health strategies to promote compliance in times of the COVID-19 pandemic?
4. Materials and Methods
4.1. Measure and Operationalization
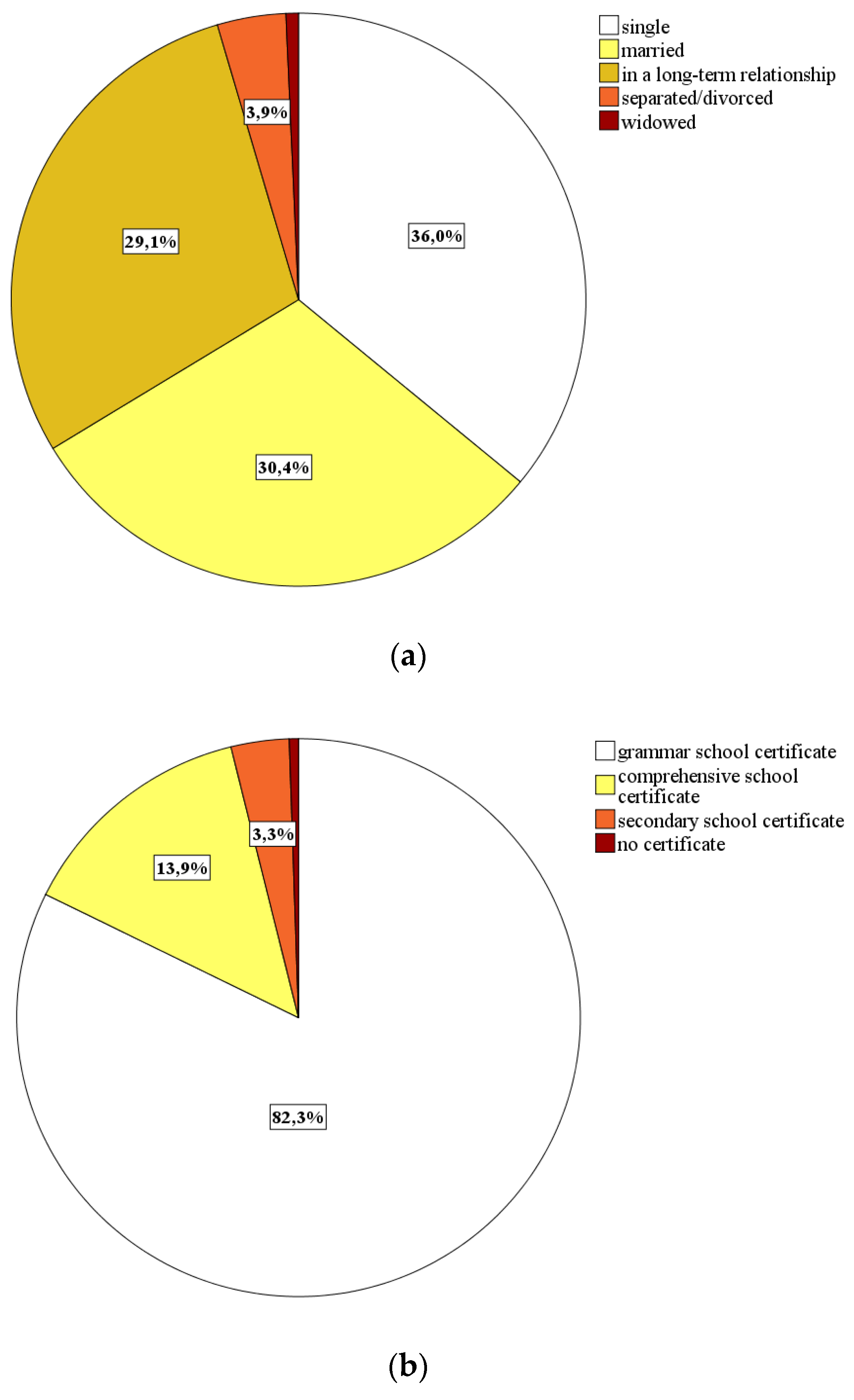
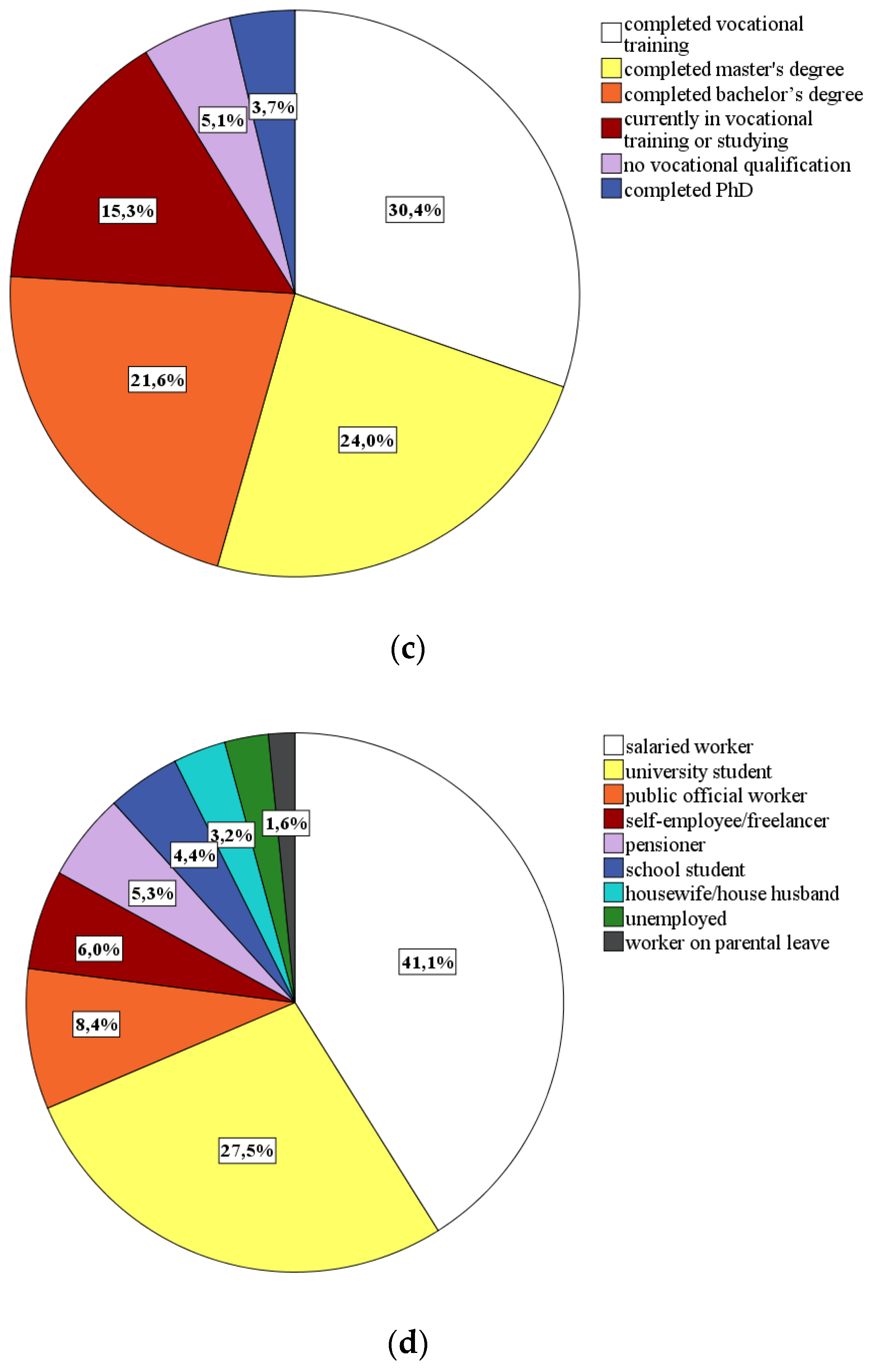
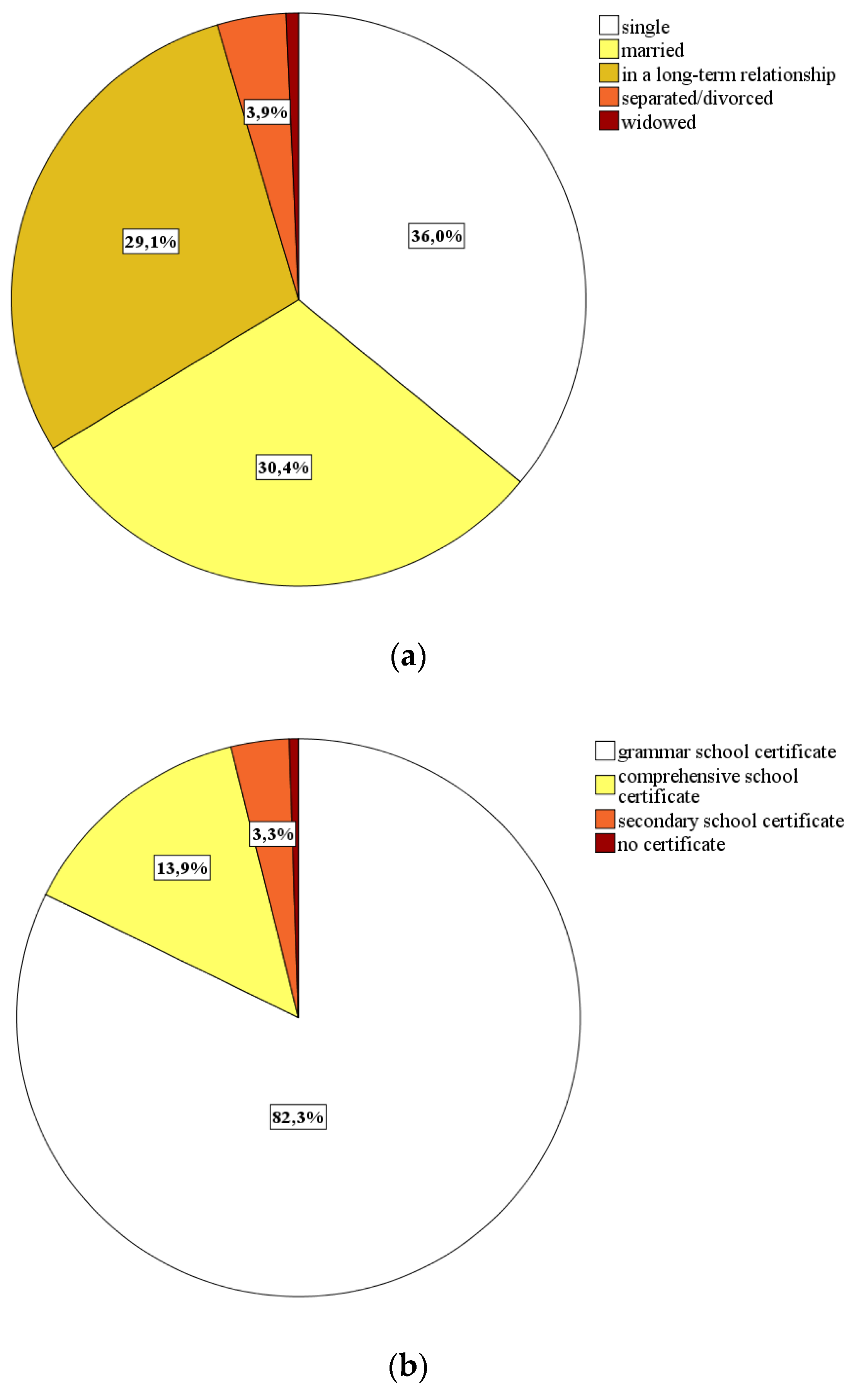
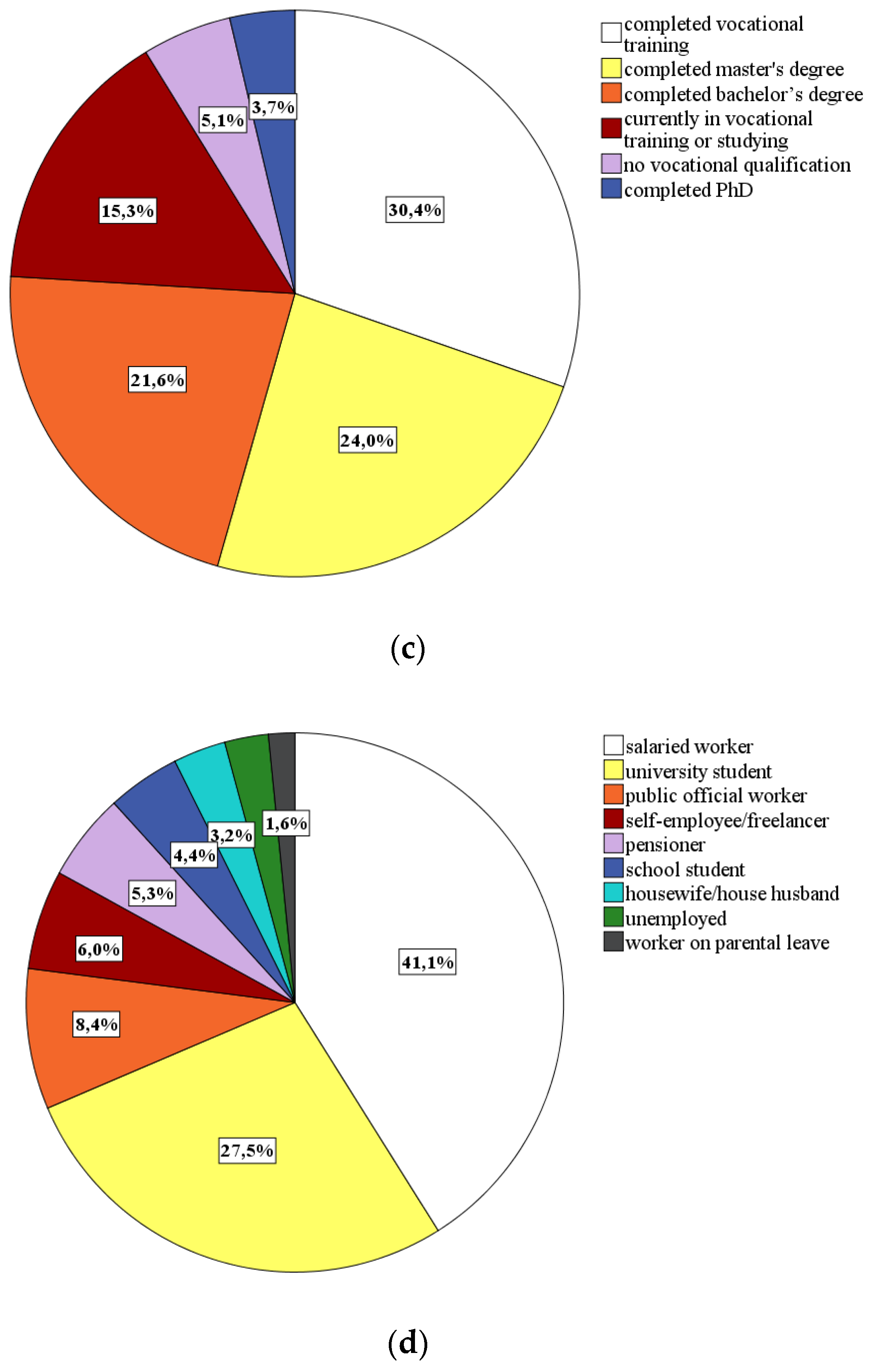
- Sociodemographic characteristics: By means of eight self-constructed items, we collected data for the participants’ gender, age, nationality, marital status, postcode, household size, level of education, and professional status.
- In order to quantify the characteristics of the components specified in the HBM, we captured the following COVID-19-related personal information by means of 10 self-constructed items:
- Perceived severity of the COVID-19 pandemic (visual analogue scale, ranging from 0 = “not dangerous at all” to 10 = “extremely dangerous”);
- Perceived own vulnerability to COVID-19 (visual analogue scale, ranging from 0 = “not at risk at all” to 10 = “extremely at risk”);
- Possible affiliation to the COVID-19 high-risk group (dichotomous item answered by stating “yes” or “no”);
- Presence of symptoms of a COVID-19 infection (cough, pyrexia, coryza, and/or sore throat; dichotomous items answered by stating “yes” or “no”) and, if applicable, virus screening including test results (adaptive question if COVID-19 symptoms were present);
- Concerns about an own infection with COVID-19 as well as about infections of closely related persons (each designed as dichotomous item answered by stating “yes” or “no”);
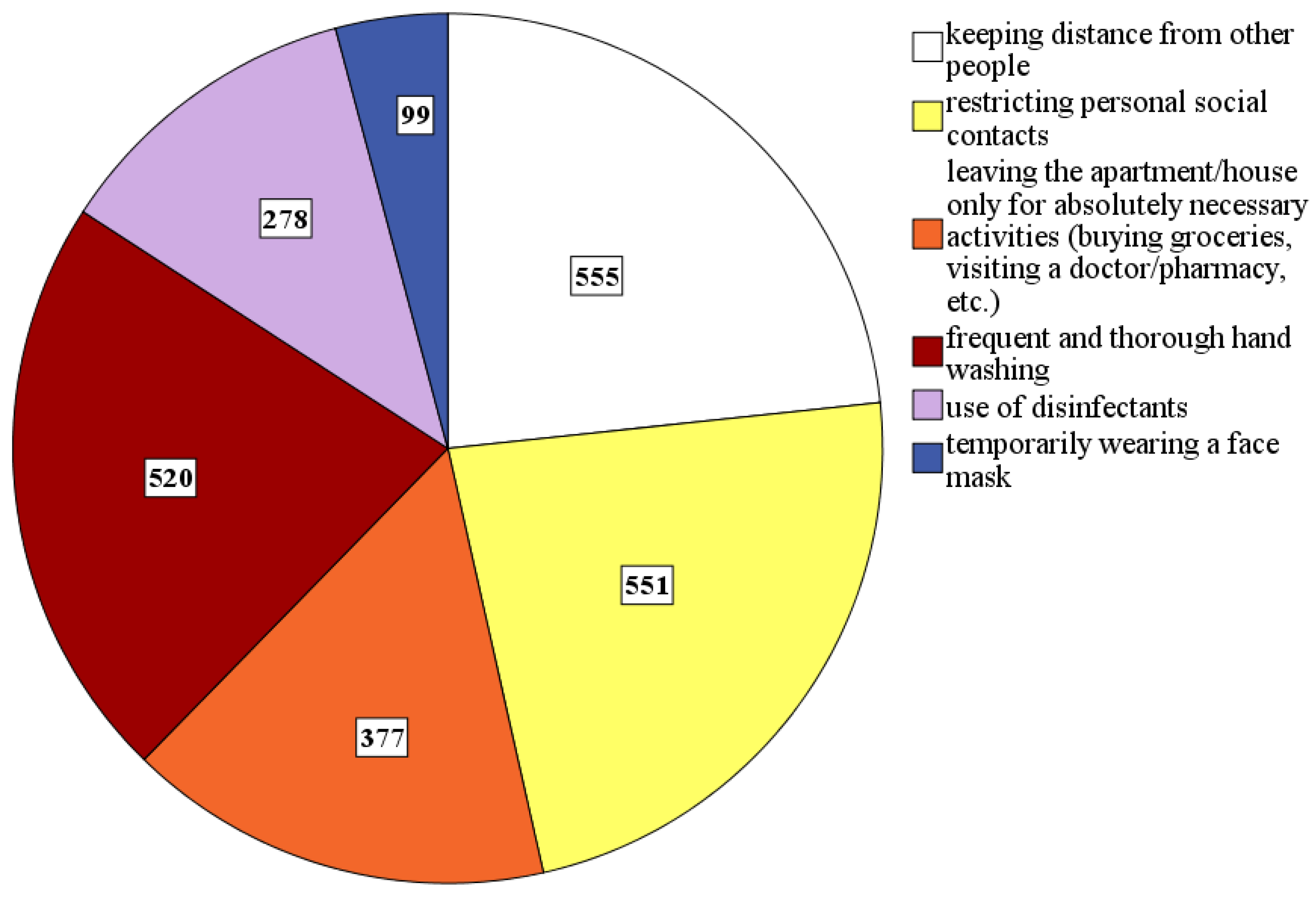
- Preventive measures taken (keeping distance, restricting contacts, following the stay-at-home-appeal, frequent hand washing, using disinfectants, and/or wearing face masks; dichotomous format answered by stating “taken” or “not taken”);
- Satisfaction with the measures taken by politicians to contain the COVID-19 pandemic or reduce the number of new infections (categorical rating scale answered by stating “generally happy with it”, “more needs to be done”, “less needs to be done”, or “not sufficiently informed to rate this”), and, where appropriate, own suggestions for further measures (free text field);
- Satisfaction with the media information regarding the COVID-19 pandemic (categorical rating scale answered by stating “generally happy with it”, “too little or too little reliable information”, or “confronted with too much information”);
- Satisfaction with the with the measures taken by politicians to contain the economic consequences of the COVID-19 pandemic (categorical rating scale answered by stating “generally happy with it”, “more needs to be done”, “less needs to be done”, or “not sufficiently informed to rate this”).
- Cognitive appraisal: The construct is based on the transactional stress theory by Lazarus and Folkman [45] and was captured using the Primary Appraisal Secondary Appraisal questionnaire (PASA) [46]. The 16 items of the PASA focus on the individually experienced strain within a stressful situation like the COVID-19 pandemic: The primary appraisal of such a stressor includes its perception as frightening (Subscale 1) and/or as challenging (Subscale 2), while the secondary appraisal takes the stressor-related self-concept of abilities (Subscale 3) and the locus of control (Subscale 4) into account. Overall, the questionnaire can therefore be used to relate the situation’s perception and evaluation to the assessment of individual available coping skills regarding this situation. The respective significance of this relationship in the context of the COVID-19 pandemic has already been shown by the exemplary reported findings by Roma et al. [15]. The four subscales are captured by four items each that should be assessed on a six-point rating scale. The mean is then calculated from the two mean values of the subscales of one dimension in order to obtain the values for the primary and secondary appraisal. The difference between the primary and secondary appraisal is finally used to calculate the total experienced strain as a stress index. The homogeneities of the primary scales in a reference sample were α = 0.61–0.83.
- Personality: The Big Five represent the five cross-cultural and time-stable personality dimensions (1) openness to new experience, (2) conscientiousness, (3) extraversion, (4) agreeableness, and (5) neuroticism [47,48]. The importance of these personality traits in the context of the COVID-19 pandemic has already been shown by Nofal et al. [14]. To capture the Big Five, we used the short scale Big Five Inventory 10 (BFI-10) which comprises 10 items that should be assessed on a five-point rating scale [49,50]. The retest reliabilities of the five subscales in a reference sample were rtt = 0.58–0.84. The decision for this short scale, which covers the Big Five dimensions with only two items each, was made in view of less strain on the participants, although the questionnaire is proven to be less reliable than other questionnaires comprising more items to measure the same personality constructs [51].
- Social competence: As social support or perceived and communicated social norms are decisive influencing variables of individual health behavior [16,36,37,38,39,40], we have decided to capture selected aspects of social competence using 24 items from the Interpersonal Competence Questionnaire (ICQ) [52,53,54]. Overall, the questionnaire contains five scales with eight items each that should be assessed on a five-point rating scale. In our study, we decided to focus only on three subscales: (1) negative assertion (i.e., standing up for own rights and ability to criticize others), (2) emotional support to others, and (3) effective handling of interpersonal conflicts. The first omitted subscale “initiation of interactions and relationships” is largely redundant with the extraversion items of the BFI-10, and the second omitted subscale “disclosure of personal information” seemed to be irrelevant for the purpose of our study. The homogeneities of the three subscales in a reference sample were α = 0.77–0.84.
- Reactance: According to Brehm [55] and Miron and Brehm [56], reactance describes an inner motivational resistance to perceived social influence, such as demands or prohibitions, which is experienced as restricting an individual’s freedom of behavior and control. In terms of behavior, reactance (now more than ever and/or attraction of the forbidden) is comparable to defiance as an active insistence on one’s own position. Fear appeals, which are increasingly used in times of the COVID-19 pandemic by decision-makers and the media, do not automatically result in a favorable effect regarding health behavior, but can even lead to reactance, especially if coping skills are not supported at the same time [28]. We used the unidimensional Reactance Scale [57,58], to capture reactance tendencies in our sample. The scale consists of 12 items that should be assessed on a four-point rating scale. The retest reliabilities of the five subscales in a reference sample were rtt = 0.71.
- Affect: The emotional situation of the test subjects in the last two weeks before participation in the study was captured using the Positive and Negative Affect Schedule (PANAS) [59,60]. The questionnaire comprises 20 items/mood-related adjectives that should be assessed on a five-point rating scale. When completing this questionnaire, subjects are asked to judge the adjectives in terms of how often they experienced a specific mood in the defined 14-day interval. Ten adjectives each represent the two dimensions of negative and positive affect, so it can be determined whether an individual’s affectivity was overall positive or negative and whether there are significant deviations compared with a reference sample from non-COVID-19 times. The homogeneity of the two subscales was α = 0.85 and 0.89 in a reference sample.
- Resilience: The unidimensional Resilience Scale (RS-13) was used to capture the participants’ psychological resilience to stress and strain situations [61,62]. In contrast to the PASA items, which predominantly address situation-specific aspects, resilience rather describes a stable habitual tendency to react to stressors. As a short scale with 13 items that should be assessed on a seven-point rating scale, the RS-13 measures the extent to which stress experiences and negative emotions can be ‘cushioned’, to what extent people remain able to act, and whether they initiate necessary actions to cope with the stress/straining situation. The homogeneity of the scale was α = 0.90 in a reference sample.
4.2. Procedure
- aims and course of the investigation,
- absolute voluntariness of participation,
- possibility of dropping out of participation at any time,
- guaranteed protection of data privacy (collection of only anonymized data),
- possibility of requesting data cancelation at any time,
- no-risk character of study participation,
- contact information in case of any questions or problems.
4.3. Sample
4.4. Statistical Methods
5. Results
5.1. COVID-19-Related Personal Information and Assessments (Research Question 1)
5.2. Preventive Behavior in Times of COVID-19 (Research Question 2)
- Rigorous curfew (i.e., permission to leave the house only for essential activities): n = 60 (57.1% out of n = 105);
- Closedown of all nonessential facilities, shops, and businesses: n = 59 (56.2% out of n = 105);
- Special opening times of the essential businesses for high-risk groups: n = 58 (55.2% out of n = 105);
- Provision of protective clothing and disinfectants for private use: n = 39 (37.1% out of n = 105);
- Border closure for all non-supply-related entry, exit, and transit traffic: n = 53 (50.5% out of n = 105);
- Rigorous ban on travel: n = 47 (44.8% out of n = 105);
- Others (especially obligatory use of face masks, volume testing, stronger checks on compliance with preventive measures): n = 11 (10.5% out of n = 105).
5.3. Influence of Time Course (Research Question 3)
5.4. Affect Balance (Research Question 4)
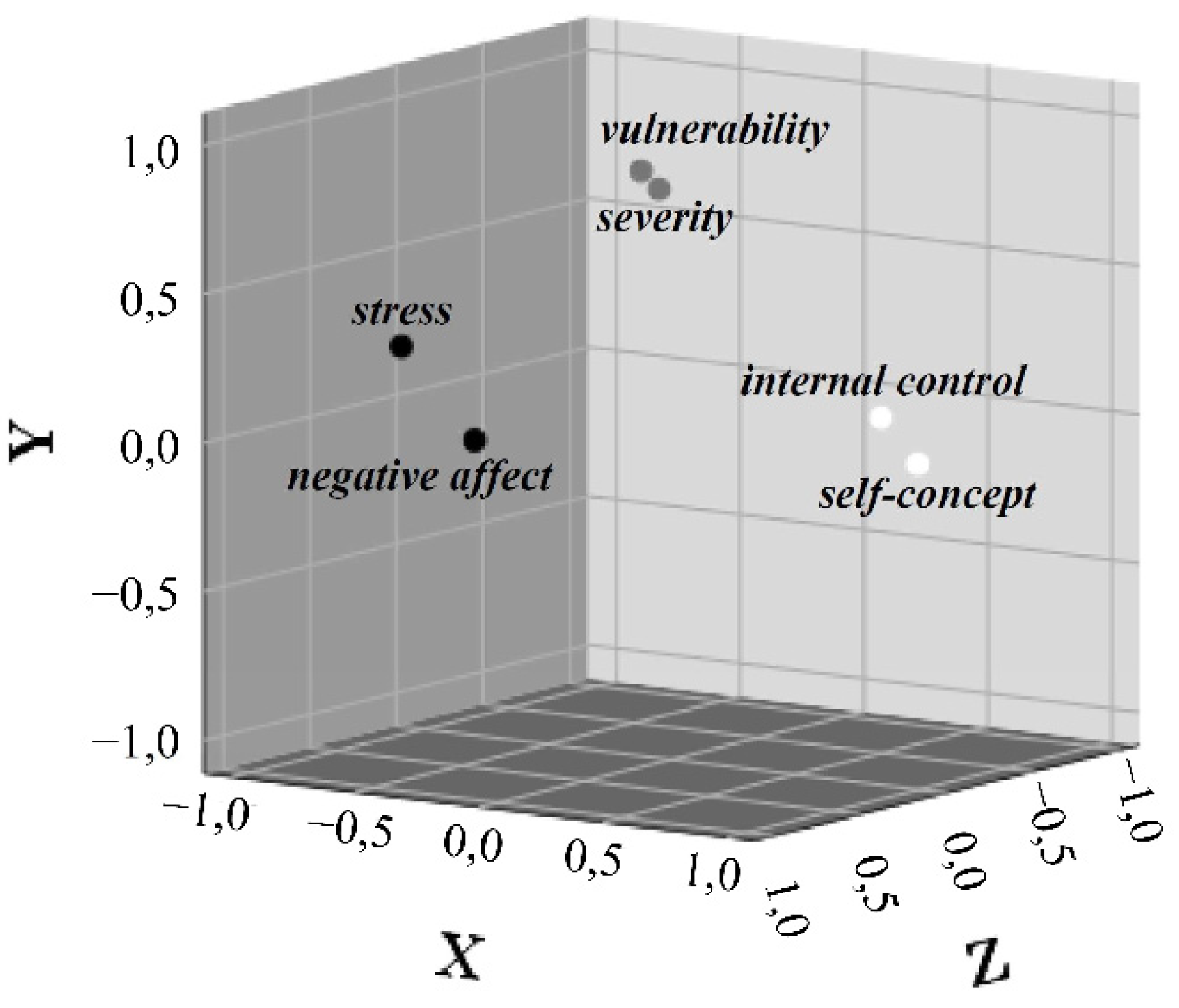
5.5. Correlational Findings (Research Question 5)
- The higher the severity of COVID-19 is assessed, r(568) = 0.21, p < 0.001;
- The higher one’s own vulnerability to COVID-19 is assessed, r(568) = 0.21, p < 0.001;
- The more the COVID-19 pandemic is perceived as frightening, r(568) = 0.23, p < 0.001;
- The more the COVID-19 pandemic is perceived as challenging, r(568) = 0.30, p < 0.001;
- The higher the current stress index is, r(568) = 0.21, p < 0.001;
- The more neurotic a person is, r(568) = 0.13, p < 0.01;
- The more open to new experiences a person is, r(568) = 0.14, p < 0.01;
- The better a person can emotionally support others, r(568) = 0.10, p < 0.05;
- The better a person can handle interpersonal conflicts, r(568) = 0.08, p < 0.05;
- The more negative affect a person is currently experiencing, r(568) = 0.15, p < 0.001.
6. Discussion
Health-Educational Sources for Enhancing Compliance with Preventive Behavior
7. Limitations and Conclusions
- The first one relates to the usual methodological aspects of a self-selected sample and the resulting lack of representativity, which is associated with decreased external validity. As a result of the recruitment of subjects primarily in an academic context, the proportions regarding the educational level and professional status were distorted compared to the total population. We were therefore unable to carry out group comparisons in this regard, which focus on the assessment of the pandemic and preventive measures taken, although we had intended to do so. In addition, due to the design of the study as an online survey, fewer older than younger subjects could be addressed, since only 67% of all people at the age of >65 years have internet access at all (in contrast to 96–99% of all people at the age of <65 years) [88]. Correspondingly, our results can be interpreted as a valid indication of certain processes in the population, but they should not be transferred offhand and to the total population.
- Secondly, some subscales of our questionnaire showed low or even insufficient reliability coefficients. A total of five subscales (three of the PASA and two of the BFI-10) of the overall 16 standardized subscales used, showed reliability coefficients only between 0.64 and 0.69. Nevertheless, we think that this did not affect internal validity excessively, since the comparatively large sample as well as the partly convergent other scales, which show good to excellent reliability coefficients, and whose results are in line with those of the less-reliable scales, compensate most of this particular lack of reliability. However, considering the two BFI-10 subscales consciousness and agreeableness, the reliability was completely insufficient (<0.60), so we had to exclude these subscales from further statistical analyses to avoid impairment of our conclusions’ validity. Of course, such an exclusion is always associated with a loss of information. Although the BFI-10′s test authors reported good psychometric properties within the questionnaire’s validation for a German sample, other studies recently carried out also seem to consistently meet reliability problems, especially with regard to the two subscales consciousness and agreeableness [89,90]. This indicates some shortcomings within the specification of the original measurement model and/or the test authors’ validation procedure. Future studies specifically focusing on the influence of personality traits on individual health behavior should therefore use other instruments to assess the Big Five, which offer better psychometric properties.
- Thirdly, both the sample bias and the reliability problems made it impossible for us to give extensive valid subgroup-specific recommendations regarding health promotion strategies to enhance compliance with preventive measures. Particularly, with regard to behavior-relevant competencies related to compliance with preventive measures during the COVID-19 pandemic, other relevant studies pointed out the differential effectiveness of implemented campaigns regarding communication of information and behavioral instructions. This means that in addition to culture-specific differences, attention must be paid to demographic, motivational, affective, cognitive, psychosocial, political, and religious characteristics of different target groups as well, as these can have a decisive influence on the reception and interpretation of information [42,43,91]. Accordingly, it seems plausible that certain behavioral appeals can cause the desired behavior by acting as effective social norms (especially in collectivistically oriented cultures like many Arab and Asian countries) or the same appeals rather tend to cause reactance (especially in individually oriented cultures like western industrial nations) [91,92]. In addition to such fundamental problems regarding the reception of information, there are many other aspects affecting the specific design of communication. For example, the complexity of the information provided should be aligned with the educational level and language barriers should be taken into account as well in order to simply ensure comprehensibility [42,43,91]. Due to these factors, it is conceivable that people who live in problem districts, or the rural population compared to metropolitans need different messages in order to address them effectively. The accessibility of different target groups in terms of their preferred sources of information must also be considered. For example, younger people are more likely to use social media, while older people are more likely to use traditional print or broadcast media [68]. Another decisive factor affecting the acceptance of information is who is providing the information. Different population subgroups differ in who they perceive as a peer or authority, so social norms intended to implement by communication can have differential effects [91,92]. This differential effectiveness of information management should be examined systematically in longitudinal studies in order to be able to implement effective campaigns without delay in the future.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Binti Hamzah, F.A.; Lau, C.; Nazri, H.; Ligot, D.V.; Lee, G.; Tan, C.L. Corona Tracker: Worldwide COVID-19 Outbreak Data Analysis and Prediction. Bull World Health Organ 2020. [Google Scholar] [CrossRef]
- Bundesrepublik Deutschland. Gesetz zum Schutz der Bevölkerung bei einer Epidemischen Lage von Nationaler Tragweite. J. Laws 2020. Available online: http://www.bgbl.de/xaver/bgbl/start.xav?startbk=Bundesanzeiger_BGBl&jumpTo=bgbl120s0587.pdf (accessed on 1 June 2020).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease, Situation Report No. 108. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 1 June 2020).
- WHO. Report of the WHO China Joint Mission on Coronavirus Disease 2019, Final Report. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 1 June 2020).
- Nationale Akademie der Wissenschaften Leopoldina. Ad-hoc-Stellungnahmen zur Coronavirus-Pandemie, Reports No. 1–4. 2020. Available online: https://www.leopoldina.org/publikationen/stellungnahmen/ (accessed on 27 May 2020).
- Bundeszentrale für Gesundheitliche Aufklärung. Verhaltensregeln und -Empfehlungen zum Schutz vor dem Coronavirus im Alltag und im Miteinander. 2020. Available online: https://www.infektionsschutz.de/coronavirus/verhaltensregeln.html (accessed on 1 May 2020).
- Carothers, T.; Press, B. The Global Rise of Anti-Lockdown Protests—And What to Do about It. World Politics Rev. 2020. Available online: https://www.worldpoliticsreview.com/articles/29137/amid-the-covid-19-pandemic-protest-movements-challenge-lockdowns-worldwide (accessed on 13 November 2020).
- Kane, P.L. The Anti-Mask League: Lockdown Protests Draw Parallels to 1918 Pandemic. The Guardian. 2020. Available online: https://www.theguardian.com/world/2020/apr/29/coronavirus-pandemic-1918-protests-california (accessed on 13 November 2020).
- Hameleers, M.; Van Der Meer, T.G.L.A.; Brosius, A. Feeling “disinformed” lowers compliance with COVID-19 guidelines: Evidence from the US, UK, Netherlands and Germany. Harv. Kennedy Sch. Misinf. Rev. 2020, 1. [Google Scholar] [CrossRef]
- Imhoff, R.; Lamberty, P. A Bioweapon or a Hoax? The Link Between Distinct Conspiracy Beliefs About the Coronavirus Disease (COVID-19) Outbreak and Pandemic Behavior. Soc. Psychol. Pers. Sci. 2020, 11, 1110–1118. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Harvey, N. The concept of “fatigue” in tackling covid-19. BMJ 2020, 371, m4171. [Google Scholar] [CrossRef]
- Nivette, A.; Ribeaud, D.; Murray, A.; Steinhoff, A.; Bechtiger, L.; Hepp, U.; Shanahan, L.; Eisner, M. Non-compliance with COVID-19-related public health measures among young adults in Switzerland: Insights from a longitudinal cohort study. Soc. Sci. Med. 2021, 268, 113370. [Google Scholar] [CrossRef]
- Nofal, A.M.; Cacciotti, G.; Lee, N. Who complies with COVID-19 transmission mitigation behavioral guidelines? PLoS ONE 2020, 15, e0240396. [Google Scholar] [CrossRef]
- Roma, P.; Monaro, M.; Muzi, L.; Colasanti, M.; Ricci, E.; Biondi, S.; Napoli, C.; Ferracuti, S.; Mazza, C. How to Improve Compliance with Protective Health Measures during the COVID-19 Outbreak: Testing a Moderated Mediation Model and Machine Learning Algorithms. Int. J. Environ. Res. Public Health 2020, 17, 7252. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlȏt, R.; Lambert, H.; Oliver, I.; Robin, C.; Yardley, L.; Rubin, G. Factors associated with adherence to self-isolation and lockdown measures in the UK: A cross-sectional survey. Public Health 2020, 187, 41–52. [Google Scholar] [CrossRef]
- Brinkmann, R. Angewandte Gesundheitspsychologie, 1st ed.; Pearson Education: London, UK, 2014; ISBN 978-3868941654. [Google Scholar]
- Fuchs, R. Modelle des Gesundheitsverhaltens. In Public Health: Sozial- und Präventivmedizin Kompakt, 1st ed.; Egger, M., Razum, O., Eds.; De Gruyter: Berlin, Germany, 2012; pp. 132–142. ISBN 978-3110254525. [Google Scholar]
- Becker, M.H. The Health Belief Model and Sick Role Behavior. Health Educ. Monogr. 1974, 2, 409–419. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Why People Use Health Services. Milbank Q. 2005, 83, 94–124. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Stroebe, W. Social Psychology and Health, 3rd ed.; McGraw-Hill: Maidenhead, UK, 2011; ISBN 978-0335238095. [Google Scholar]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Harrison, J.A.; Mullen, P.D.; Green, L.W. A meta-analysis of studies of the Health Belief Model with adults. Health Educ. Res. 1992, 7, 107–116. [Google Scholar] [CrossRef]
- Abraham, C.; Scheeran, P. The health belief model. In Predicting Health Behaviour; Conner, M., Norman, P., Eds.; Open University Press: London, UK, 2005; pp. 28–80. ISBN 978-0335211760. [Google Scholar]
- Vogt, I. Grundlagen der Gesundheitspsychologie. In Gesundheitswissenschaften, 1st ed.; Haring, R., Ed.; Springer: Heidelberg, Germany, 2019; pp. 29–36. ISBN 978-3662583135. [Google Scholar]
- Lippke, S.; Renneberg, B. Theorien und Modelle des Gesundheitsverhaltens. In Gesundheitspsychologie, 1st ed.; Renneberg, B., Hammelstein, P., Eds.; Springer: Heidelberg, Germany, 2006; pp. 35–60. ISBN 978-3540254621. [Google Scholar]
- Pietrowsky, R. Ernährung. In Gesundheitspsychologie, 1st ed.; Renneberg, B., Hammelstein, P., Eds.; Springer: Heidelberg, Germany, 2006; pp. 174–194. ISBN 978-3540254621. [Google Scholar]
- Schwarzer, R. Psychologie des Gesundheitsverhaltens. Einführung in die Gesundheitspsychologie, 3rd ed.; Hogrefe: Göttingen, Germany, 2004; ISBN 978-3801718169. [Google Scholar]
- De Hoog, N.; Stroebe, W.; De Wit, J.B.F. The Impact of Vulnerability to and Severity of a Health Risk on Processing and Acceptance of Fear-Arousing Communications: A Meta-Analysis. Rev. Gen. Psychol. 2007, 11, 258–285. [Google Scholar] [CrossRef]
- WHO. Similarities and Differences—COVID-19 and Influenza. Questions & Answers. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-similarities-and-differences-covid-19-and-influenza?gclid=EAIaIQobChMIq9v_itWp6QIVDbTVCh2dmg3GEAAYASAAEgJFzvD_BwE (accessed on 1 July 2020).
- Weinstein, N.D. Optimistic biases about personal risks. Science 1989, 246, 1232–1233. [Google Scholar] [CrossRef]
- Conner, M. Cognitive Determinants of Health Behavior. In Handbook of Behavioral Medicine; Steptoe, A., Ed.; Springer: New York, NY, USA, 2010; pp. 19–30. ISBN 978-0387094878. [Google Scholar]
- Faltermaier, T. Laienperspektiven auf Gesundheit und Krankheit. In Soziologie von Gesundheit und Krankheit, 1st ed.; Richter, M., Hurrelmann, K., Eds.; Springer: Heidelberg, Germany, 2016; pp. 229–241. ISBN 978-3658110093. [Google Scholar]
- Faltermaier, T. Gesundheitspsychologie, 2nd ed.; Kohlhammer: Stuttgart, Germany, 2017; Volume 21, ISBN 978-3170261495. [Google Scholar]
- Hammelstein, P.; Pohl, J.; Reimann, S.; Roth, M. Persönlichkeitsmerkmale. In Gesundheitspsychologie, 1st ed.; Renneberg, B., Hammelstein, P., Eds.; Springer: Heidelberg, Germany, 2006; pp. 61–105. ISBN 978-3540254621. [Google Scholar]
- Kienle, R.; Knoll, N.; Renneberg, B. Soziale Ressourcen und Gesundheit: Soziale Unterstützung und dyadisches Bewältigen. In Gesundheitspsychologie, 1st ed.; Renneberg, B., Hammelstein, P., Eds.; Springer: Heidelberg, Germany, 2006; pp. 108–122. ISBN 978-3540254621. [Google Scholar]
- Reimann, S.; Hammelstein, P. Ressourcenorientierte Ansätze. In Gesundheitspsychologie, 1st ed.; Renneberg, B., Hammelstein, P., Eds.; Springer: Heidelberg, Germany, 2006; pp. 13–28. ISBN 978-3540254621. [Google Scholar]
- Sirois, F.M.; Hirsch, J.K. Big Five traits, affect balance and health behaviors: A self-regulation resource perspective. Pers. Individ. Differ. 2015, 87, 59–64. [Google Scholar] [CrossRef]
- Chen, X.; Chen, H. Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. Int. J. Environ. Res. Public Health 2020, 17, 4437. [Google Scholar] [CrossRef]
- Pan, Y.; Fang, Y.; Xin, M.; Dong, W.; Zhou, L.; Hou, Q.; Li, F.; Sun, G.; Zheng, Z.; Yuan, J.; et al. Self-Reported Compliance with Personal Preventive Measures Among Chinese Factory Workers at the Beginning of Work Resumption Following the COVID-19 Outbreak: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e22457. [Google Scholar] [CrossRef]
- Pan, Y.; Xin, M.; Zhang, C.; Dong, W.; Fang, Y.; Wu, W.; Li, M.; Pang, J.; Zheng, Z.; Wang, Z.; et al. Associations of Mental Health and Personal Preventive Measure Compliance with Exposure to COVID-19 Information During Work Resumption Following the COVID-19 Outbreak in China: Cross-Sectional Survey Study. J. Med. Internet Res. 2020, 22, e22596. [Google Scholar] [CrossRef]
- Staatskanzlei des Landes Nordrhein-Westfalen. Straftaten und Ordnungswidrigkeiten nach dem Infektionsschutzgesetz im Zusammenhang mit der Coronaschutzverordnung, Schedule of Fines, Enacted 2020 March 22. Available online: https://www.land.nrw/sites/default/files/asset/document/200323_bussgeldkatalog_zur_rechtsverordnung_22.03.2020.pdf (accessed on 1 May 2020).
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping, 1st ed.; Springer: New York, NY, USA, 1984; ISBN 978-0826141910. [Google Scholar]
- Gaab, J. PASA—Primary Appraisal Secondary Appraisal. Ein Fragebogen zur Erfassung von situationsbezogenen kognitiven Bewertungen. Verhaltenstherapie 2009, 19, 114–115. [Google Scholar] [CrossRef] [Green Version]
- De Raad, B. The Big Five Personality Factors. The Psycholexical Approach to Personality, 1st ed.; Hogrefe: Seattle, WA, USA, 2001; ISBN 978-0889372368. [Google Scholar]
- Wiggins, J.S.; Trapnell, P.D. Personality structure: The return of the big five. In Handbook of Personality Psychology, 1st ed.; Hogan, R., Johnson, J.A., Briggs, S.R., Eds.; Academic Press: San Diego, CA, USA, 1997; pp. 737–765. ISBN 978-0121346461. [Google Scholar]
- Rammstedt, B. The 10-Item Big Five Inventory. Norm Values and Investigation of Sociodemographic Effects Based on a German Population Representative Sample. Eur. J. Psychol. Assess 2007, 23, 193–201. [Google Scholar] [CrossRef]
- Rammstedt, B.; John, O.P. Measuring personality in one minute or less: A 10-item short version of the Big Five Inventory in English and German. J Res Pers 2007, 41, 203–212. [Google Scholar] [CrossRef]
- Berth, H.; Goldschmidt, S.; Ostendorf, F.; Angleitner, A. Testinformation. Diagnostica 2006, 52, 95–99. [Google Scholar] [CrossRef]
- Buhrmester, D.; Furman, W.; Wittenberg, M.T.; Reis, H.T. Five domains of interpersonal competence in peer relationships. J. Pers. Soc. Psychol. 1988, 55, 991–1008. [Google Scholar] [CrossRef]
- Graf, A. Schlüsselqualifikation Soziale Kompetenz—Eine Vergleichsstudie in deutschen und US-amerikanischen Versicherungsunternehmen. Ger. J. Hum. Resour. Manag. Z. Pers. 2002, 16, 376–391. [Google Scholar] [CrossRef]
- Kanning, U.P. Development and Validation of a German-Language Version of the Interpersonal Competence Questionnaire (ICQ). Eur. J. Psychol. Assess. 2006, 22, 43–51. [Google Scholar] [CrossRef]
- Brehm, J.W. A Theory of Psychological Reactance, 1st ed.; Academic Press: San Diego, WA, USA, 1966; ISBN 978-0121298500. [Google Scholar]
- Miron, A.M.; Brehm, J.W. Reactance Theory—40 Years Later. Z. Soz. 2006, 37, 9–18. [Google Scholar] [CrossRef]
- Herzberg, P.Y. Zur psychometrischen Optimierung einer Reaktanzskala mittels klassischer und IRT-basierter Analysemethoden. Diagnostica 2002, 48, 163–171. [Google Scholar] [CrossRef]
- Merz, J. Fragebogen zur Messung der psychologischen Reaktanz. Diagnostica 1983, 29, 75–82. [Google Scholar]
- Crawford, J.R.; Henry, J.D. The Positive and Negative Affect Schedule (PANAS): Construct validity, measurement properties and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2004, 43, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Leppert, K.; Koch, B.; Brähler, E.; Strauß, B. Die Resilienzskala (RS)—Überprüfung der Langform RS-25 und einer Kurzform RS-13. Klin. Diagn. Eval. 2008, 2, 226–243. [Google Scholar]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- SAP America. Qualtrics Survey (Online Survey Software). Available online: https://www.qualtrics.com/de/ (accessed on 25 April 2020).
- Leibniz-Zentrum für Psychologische Information und Dokumentation. Blog: Aktuelle Online-Untersuchungen in der Psychologie. Available online: http://estudy.zpid.de/ (accessed on 25 March 2020).
- Deutsche Gesellschaft für Psychologie. Berufsethische Richtlinien des Berufsverbandes Deutscher Psychologinnen und Psychologen e. V. und der Deutschen Gesellschaft für Psychologie. Available online: https://www.bdp-verband.de/binaries/content/assets/beruf/ber-foederation-2016.pdf (accessed on 24 March 2020).
- World Medical Association. WMA’s Declaration of Helsinki Serves as Guide to Physicians. AMA J. Ethics 1964, 189, 33–34. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. AMA J. Ethics 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Statistisches Bundesamt. Statistisches Jahrbuch: Deutschland und Internationales; Destatis: Wiesbaden, Germany, 2019; ISBN 978-3-8246-1086-0.
- IBM Corp. Released 2017. IBM SPSS Statistics for Windows; Version 25.0 (Statistical Analyses Software); IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Krohne, H.W.; Egloff, B.; Kohlmann, C.-W.; Tausch, A. Positive and Negative Affect Schedule--German Version. PsycTESTS Dataset 1996, 42, 139–156. [Google Scholar] [CrossRef]
- Piasta, S.B.; Justice, L.M. Cohen’s d statistic. In Encyclopedia of Research Design, 1st ed.; Salkind, N.J., Ed.; SAGE: Thousand Oaks, CA, USA, 2010; pp. 180–185. ISBN 978-1412961271. [Google Scholar]
- Franzowiak, P. Präventionsparadox. Available online: https://www.leitbegriffe.bzga.de/alphabetisches-verzeichnis/praeventionsparadox/ (accessed on 28 June 2020).
- Krapp, A. Interesse, Lernen und Leistung. Neue Forschungsansätze in der Pädagogischen Psychologie. Zeitschrift Pädagogik 1992, 38, 747–770. [Google Scholar]
- Segerstrom, S.C. Personality and the immune system: Models, methods, and mechanisms. Ann. Behav. Med. 2000, 22, 180–190. [Google Scholar] [CrossRef]
- Weber, H. Persönlichkeit und Gesundheit. In Gesundheitspsychologie, 1st ed.; Schwarzer, R., Ed.; Hogrefe: Göttingen, Germany, 2005; Volume 1, pp. 130–148. ISBN 978-3801715007. [Google Scholar]
- E Lucas, R.; Donnellan, M.B. Personality development across the life span: Longitudinal analyses with a national sample from Germany. J. Pers. Soc. Psychol. 2011, 101, 847–861. [Google Scholar] [CrossRef] [PubMed]
- Mobil in Deutschland. BE SMART—Die Bundesweite Verkehrssicherheitskampagne Gegen Ablenkung am Steuer Durch das Smartphone, Prevention Campaign Initiated. 2015. Available online: https://www.besmart-mobil.de/ (accessed on 3 August 2020).
- Erhart, M.; Wille, N.; Ravens-Sieberer, U. Empowerment bei Kindern und Jugendlichen—Die Bedeutung personaler und sozialer Ressourcen und persönlicher Autonomie für die subjektive Gesundheit. Gesundheitswesen 2008, 70, 721–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rappaport, J. Ein Plädoyer für die Wirklichkeit. Ein sozialpolitisches Konzept des “empowerment” anstelle präventiver Ansätze. Verhalt. Psychosoz. Prax. 1985, 2, 257–278. [Google Scholar]
- Rappaport, J.; Swift, C.; Hess, R. Studies in Empowerment. Steps towards Understanding and Action, 1st ed.; Haworth Press: Philadelphia, PA, USA, 1984; ISBN 978-0866562836. [Google Scholar]
- Wallston, K.A.; Maides, S.; Wallston, B.S. Health-related Information-Seeking as a function of Health-related Locus of Control and Health Value. J. Res. Pers. 1976, 10, 215–222. [Google Scholar] [CrossRef]
- Adams, J.R.; Drake, R.E. Shared Decision-Making and Evidence-Based Practice. Community Ment. Health J. 2006, 42, 87–105. [Google Scholar] [CrossRef]
- Joosten, E.A.; DeFuentes-Merillas, L.; de Weert Gerdien, H.; Sensky, T.; van der Staak, C.P.; de Jong, C.A.J. Systematic Review of the Effects of Shared Decision-Making on Patient Satisfaction, Treatment Adherence and Health Status. Psychother. Psychosom. 2008, 77, 219–226. [Google Scholar] [CrossRef]
- Scheibler, F. Shared Decision-Making. Von der Compliance zur Partnerschaftlichen Entscheidungsfindung, 1st ed.; Huber: Bern, Switzerland, 2003; ISBN 978-3456840475. [Google Scholar]
- Wilson, S.R.; Strub, P.; Buist, A.S.; Knowles, S.B.; Lavori, P.W.; Lapidus, J.; Vollmer, W.M. Shared Treatment Decision Making Improves Adherence and Outcomes in Poorly Controlled Asthma. Am. J. Respir. Crit. Care Med. 2010, 181, 566–577. [Google Scholar] [CrossRef]
- Klandermans, B. The Social Psychology of Protest, 1st ed.; Blackwell: Oxford, UK, 1997; ISBN 978-0631188797. [Google Scholar]
- Opp, K.-D. Theories of Political Protest and Social Movements. A Multidisciplinary Introduction, Critique, and Synthesis, 1st ed.; Routledge: New York, NY, USA, 2009; ISBN 978-0415483896. [Google Scholar]
- Statistisches Bundesamt. Internetnutzung von Personen nach Altersgruppen in %. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Einkommen-Konsum-Lebensbedingungen/_Grafik/_Interaktiv/it-nutzung-alter.htm (accessed on 10 June 2020).
- Ryser, V.A. Psychometric properties of extra-short Big Five personality measures in multi-topic surveys: Documenting personality traits in the SHP and MOSAiCH. FORS Work. Paper Ser. 2015, 5, 1–35. [Google Scholar] [CrossRef]
- Lovik, A.; Verbeke, G.; Molenberghs, G. BFI-10: A Very Short Personality Test to Measure the Big Five Factors. Leuven Statistics Days, October 2016. [Google Scholar]
- Bundeszentrale für Gesundheitliche Aufklärung. Leitbegriffe der Gesundheitsförderung und Prävention: Glossar zu Konzepten, Strategien und Methoden. 2018. Available online: https://www.leitbegriffe.bzga.de/ (accessed on 22 December 2020).
- Betsch, C.; Böhm, R.; Airhihenbuwa, C.O.; Butler, R.; Chapman, G.B.; Haase, N.; Herrmann, B.; Igarashi, T.; Kitayama, S.; Korn, L.; et al. Improving Medical Decision Making and Health Promotion through Culture-Sensitive Health Communication: An Agenda for Science and Practice. Med. Decis. Making 2016, 36, 811–833. [Google Scholar] [CrossRef]
- Belluz, J. The 4 simple reasons Germany is managing Covid-19 better than its neighbors. Vox Media. 2020. Available online: https://www.vox.com/21495327/covid-19-germany-coronavirus-cases-deaths (accessed on 12 December 2020).
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Sachs, J.D. What Asian Nations Know about squashing Covid-19. CNN Opin. 2020. Available online: https://edition.cnn.com/2020/05/02/opinions/us-can-learn-from-asia-sachs/index.html (accessed on 10 December 2020).
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus Pandemic. OurWorldInData. 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 10 December 2020).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Instrument | Subscale | Reliability |
|---|---|---|
| PASA | assessment as frightening | 0.80 1 |
| assessment as challenging | 0.69 1 | |
| self-concept of COVID-19-related abilities | 0.66 1 | |
| COVID-19-related locus of control | 0.64 1 | |
| BFI-10 | openness to new experience | 0.64 2 |
| conscientiousness | 0.52 2 | |
| extraversion | 0.72 2 | |
| agreeableness | 0.26 2 | |
| neuroticism | 0.64 2 | |
| ICQ | negative assertion | 0.84 1 |
| emotional support to others | 0.88 1 | |
| effective handling of interpersonal conflicts | 0.79 1 | |
| Reactance Scale | — | 0.80 1 |
| PANAS | positive affectivity | 0.83 1 |
| negative affectivity | 0.83 1 | |
| RS-13 | — | 0.89 1 |
| Preventive Measure | ntaken1 | Comparison | nobs2 | nexp3 | χ2-Test | p | φ |
|---|---|---|---|---|---|---|---|
| Keeping distance | 160 | Weeks 1 + 2 | 81.0 | 80.0 | χ2(1) = 1.03 | 0.31 | |
| Weeks 3 + 4 | 79.0 | 80.0 | |||||
| Restricting social contacts | 156 | Weeks 1 + 2 | 81.0 | 78.0 | χ2(1) = 4.73 | <0.05 | −0.17 |
| Weeks 3 + 4 | 75.0 | 78.0 | |||||
| Following the stay-at-home appeal | 104 | Weeks 1 + 2 | 58.0 | 52.0 | χ2(1) = 3.79 | 0.05 | |
| Weeks 3 + 4 | 46.0 | 52.0 | |||||
| Washing hands | 152 | Weeks 1 + 2 | 78.0 | 76.0 | χ2(1) = 1.44 | 0.23 | |
| Weeks 3 + 4 | 74.0 | 76.0 | |||||
| Using disinfectants | 81 | Weeks 1 + 2 | 36.0 | 40.5 | χ2(1) = 1.98 | 0.16 | |
| Weeks 3 + 4 | 45.0 | 40.5 | |||||
| Using face masks | 27 | Weeks 1 + 2 | 10.0 | 13.5 | χ2(1) = 2.17 | 0.14 | |
| Weeks 3 + 4 | 17.0 | 13.5 |
| Aspects of the Perception and Assessments of the COVID-19 Pandemic | Comparison | n1 | M2 | SD3 | t-Test | p | dCohen |
|---|---|---|---|---|---|---|---|
| Perceived severity | Weeks 1 + 2 | 82 | 6.62 | 2.01 | t(162) = 1.96 | 0.05 | |
| Weeks 3 + 4 | 82 | 6.04 | 1.80 | ||||
| Perceived own vulnerability | Weeks 1 + 2 | 82 | 3.84 | 2.30 | t(162) = 1.83 | 0.07 | |
| Weeks 3 + 4 | 82 | 3.23 | 1.96 | ||||
| Challenge assessment (PASA) 4 | Weeks 1 + 2 | 82 | 4.83 | 0.81 | t(162) = 2.35 | 0.02 | 0.37 |
| Weeks 3 + 4 | 82 | 4.54 | 0.78 | ||||
| Neuroticism (BFI-10) 5 | Weeks 1 + 2 | 82 | 3.05 | 1.00 | t(162) = 2.10 | 0.04 | 0.33 |
| Weeks 3 + 4 | 82 | 2.74 | 0.90 |
| Affectivity Dimension | Comparison | n1 | M2 | SD3 | dCohen |
|---|---|---|---|---|---|
| Positive affectivity | Reference sample | 349 | 27.35 | 6.38 | 0.15 |
| Analysis sample | 570 | 28.35 | 6.57 | ||
| Negative affectivity | Reference sample | 349 | 14.67 | 5.19 | 1.01 |
| Analysis sample | 570 | 20.78 | 6.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Welter, V.D.E.; Welter, N.G.E.; Großschedl, J. Experience and Health-Related Behavior in Times of the Corona Crisis in Germany: An Exploratory Psychological Survey Considering the Identification of Compliance-Enhancing Strategies. Int. J. Environ. Res. Public Health 2021, 18, 933. https://doi.org/10.3390/ijerph18030933
Welter VDE, Welter NGE, Großschedl J. Experience and Health-Related Behavior in Times of the Corona Crisis in Germany: An Exploratory Psychological Survey Considering the Identification of Compliance-Enhancing Strategies. International Journal of Environmental Research and Public Health. 2021; 18(3):933. https://doi.org/10.3390/ijerph18030933
Chicago/Turabian StyleWelter, Virginia Deborah Elaine, Naemi Georgina Eliane Welter, and Jörg Großschedl. 2021. "Experience and Health-Related Behavior in Times of the Corona Crisis in Germany: An Exploratory Psychological Survey Considering the Identification of Compliance-Enhancing Strategies" International Journal of Environmental Research and Public Health 18, no. 3: 933. https://doi.org/10.3390/ijerph18030933