
How Framed Messages Influence Depression Assessment Intentions: Interactivity of Social Media as a Moderator



Abstract
:1. Introduction
- RQ1: Will individuals have different intentions to take a depression assessment after reading gain-framed messages versus loss-framed messages?
2. Materials and Methods
2.1. Design and Participants
2.2. Stimulus and Manipulation
2.3. Measures
2.3.1. Manipulation Check
2.3.2. Dependent Variable
2.3.3. Control Variables
3. Results
3.1. Statistical Analysis
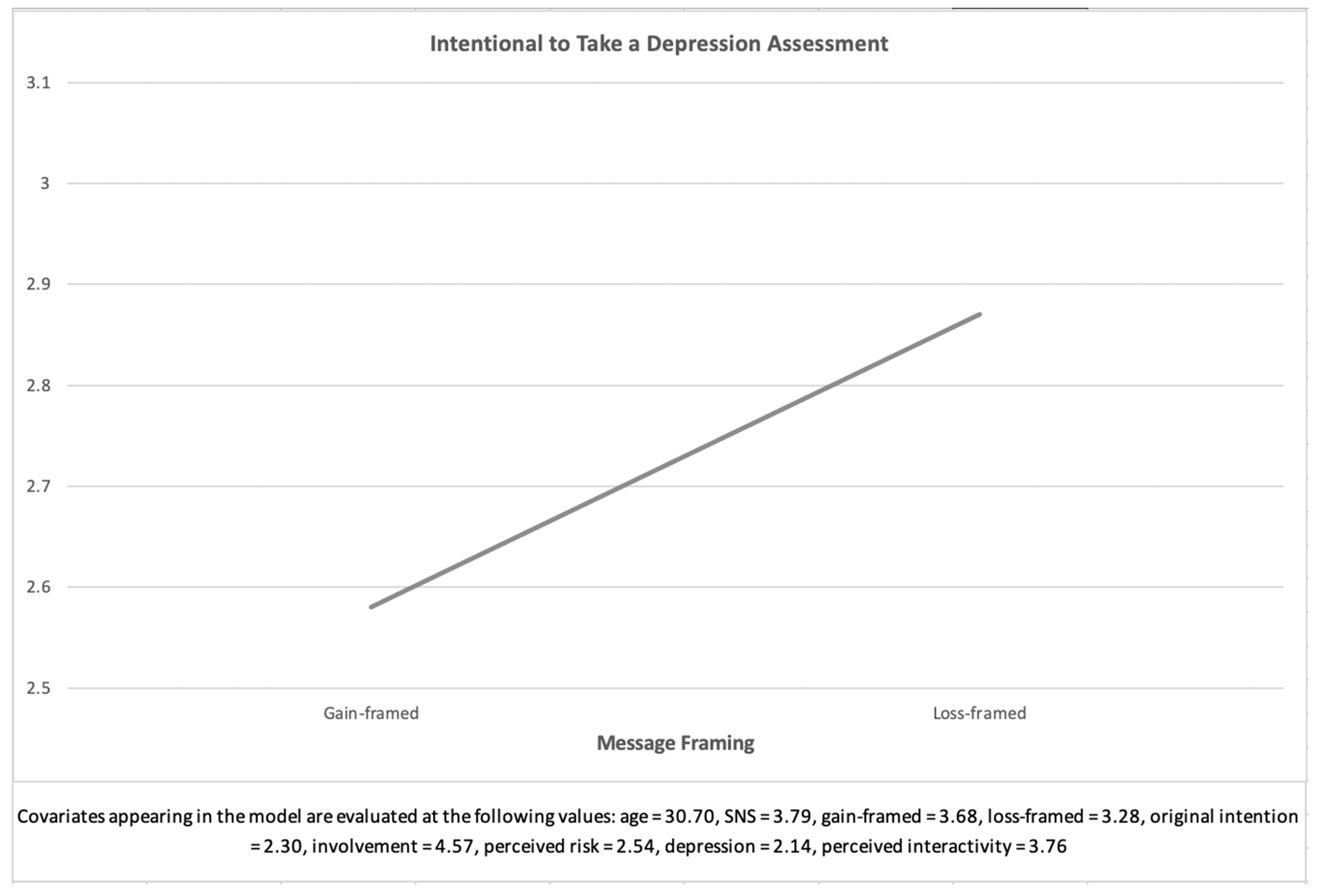
3.2. The Main Effect of Message Framing on the Intention to Take a Depression Assessment (RQ1)
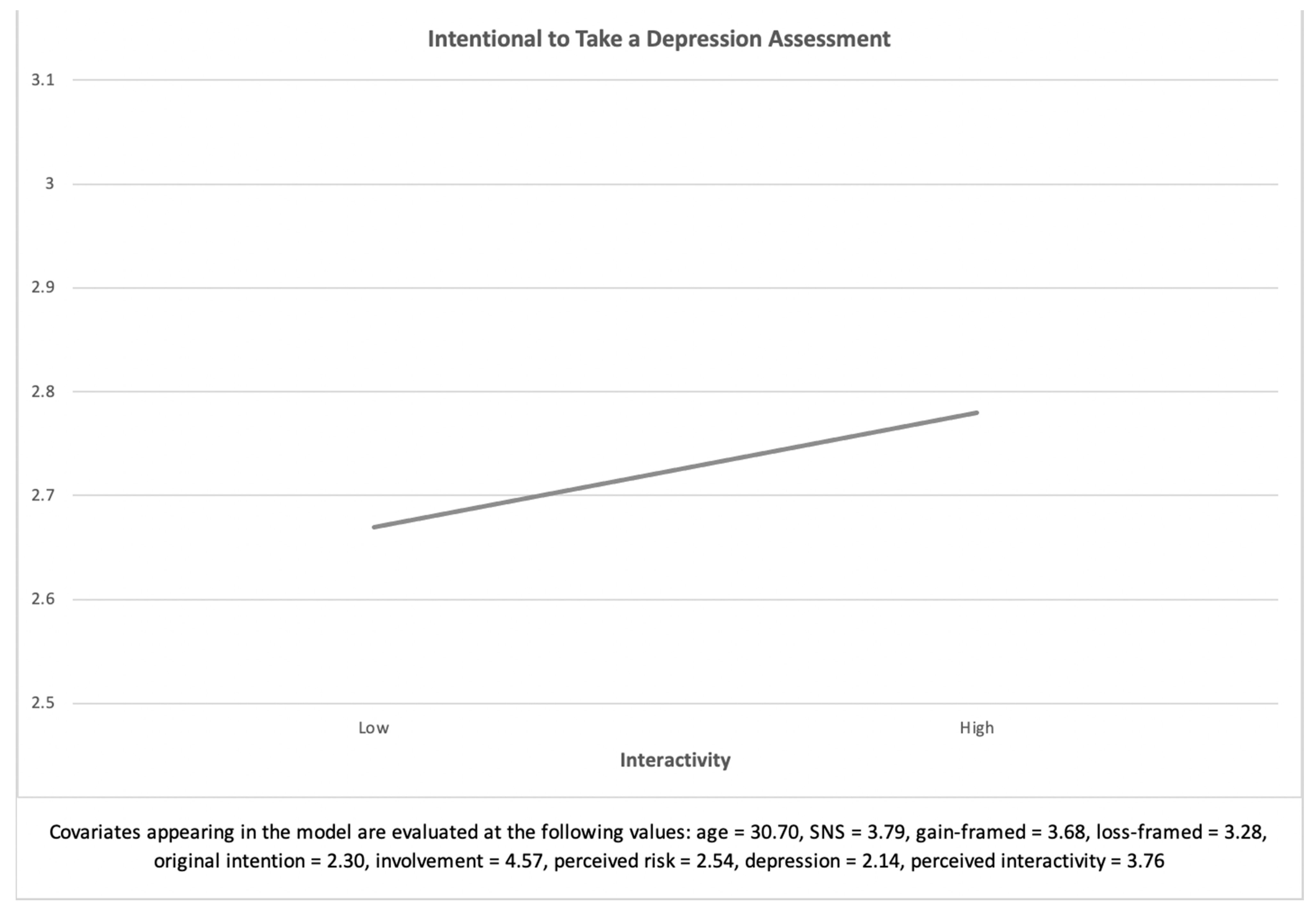
3.3. The Main Effect of Interactivity on the Intention to Take a Depression Assessment (H1)
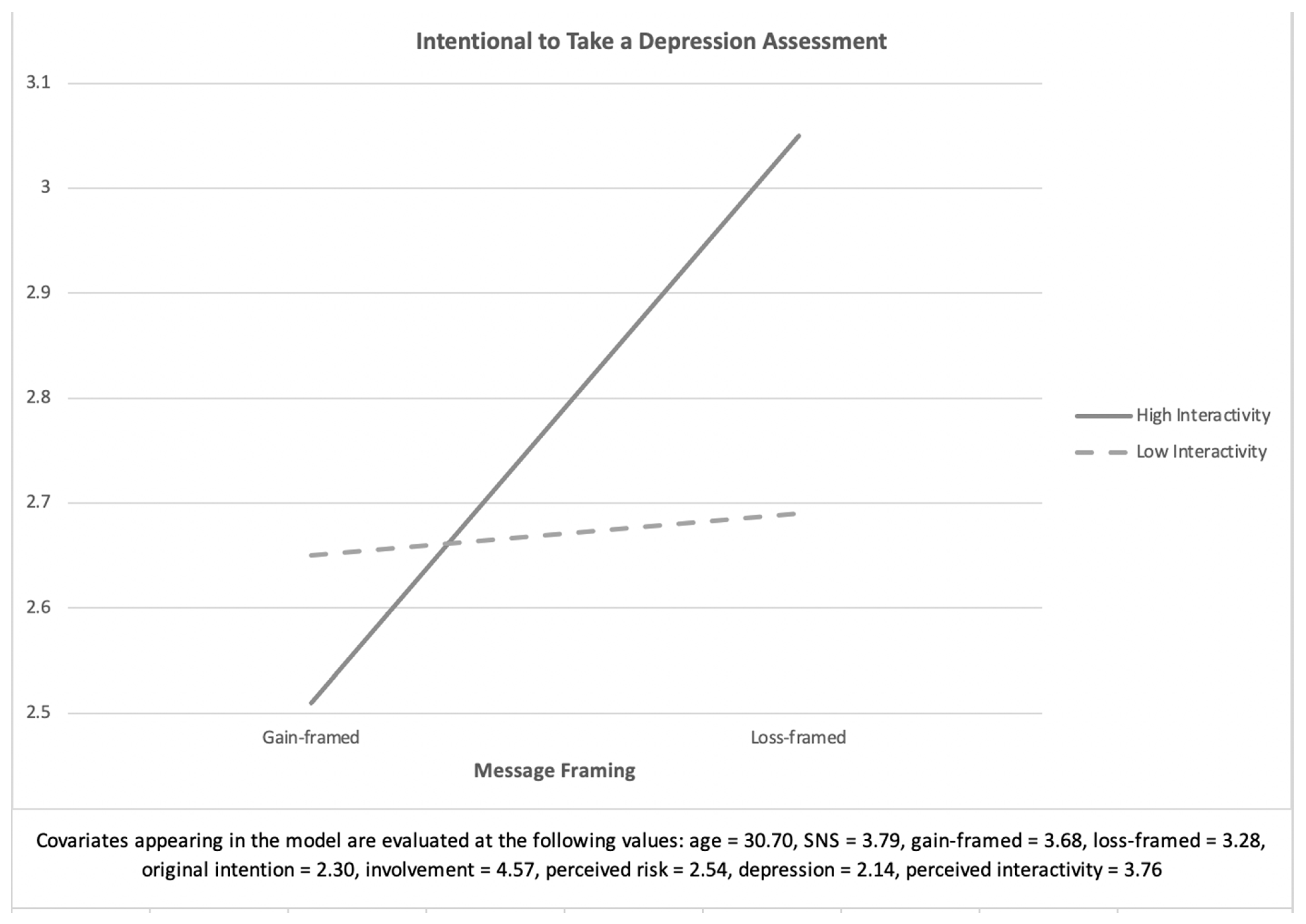
3.4. The Interaction Effect of Message Framing and Interactivity on the Intention to Take a Depression Assessment (H2)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Available online: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf?sequence=1 (accessed on 6 October 2020).
- World Health Organization. Home Page-Depression. Available online: https://www.who.int/health-topics/depression#tab=tab_1 (accessed on 1 December 2020).
- Sina News. There are 540 Million Depression Patients in China. 2019. Available online: http://news.sina.com.cn/s/2019-06-13/doc-ihvhiqay5294266.shtml (accessed on 6 October 2020).
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Yu, Y.; Kou, C.; Xu, X.; Lu, J.; et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef]
- Beijing Daily. Only Ten Percent of Patients with Depression Take a Screening in China. 2017. Available online: http://www.xinhuanet.com/local/2017-12/06/c_129757638.htm (accessed on 1 December 2020).
- Novick, D.; Montgomery, W.; Vorstenbosch, E.; Moneta, M.V.; Dueñas, H.; Haro, J.M. Recovery in patients with major depressive disorder (MDD): Results of a 6-month, multinational, observational study. Patient Prefer. Adherence 2017, 11, 1859. [Google Scholar] [CrossRef] [Green Version]
- De Choudhury, M. Role of social media in tackling challenges in mental health. In Proceedings of the 2nd International Workshop on Socially-Aware Multimedia, Barcelona, Spain, 21 October 2013; pp. 49–52. [Google Scholar]
- Chen, L.L.; Cheng, C.H.; Gong, T. Inspecting vulnerability to depression from social media affect. Front. Psychiatry 2020, 11, 54. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.Y.; Sidani, J.E.; Shensa, A.; Radovic, A.; Miller, E.; Colditz, J.B.; Hoffman, B.L.; Giles, L.M.; Primack, B.A. Primack Association between social media use and depression among US young adults. Depress. Anxiety 2016, 33, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.; Bonnette, A.; Howard, K.; Ceballos, N.; Dailey, S.; Lu, Y.; Grimes, T. Social comparisons, social media addiction, and social interaction: An examination of specific social media behaviors related to major depressive disorder in a millennial population. J. Appl. Biobehav. Res. 2019, 24, e12158. [Google Scholar] [CrossRef]
- Lueck, J.A. Matching Message Design and Depressed Cognition: An Exploration of Attention Patterns for Gain- and Loss-Framed Depression Help-Seeking Messages. J. Health Commun. 2017, 22, 593–603. [Google Scholar] [CrossRef]
- Lueck, J.A. Examining determinants of seeking help for depression: Implications for effective health promotion messages. J. Commun. Health 2017, 11, 19–29. [Google Scholar] [CrossRef]
- Mavandadi, S.; Wright, E.; Klaus, J.; Oslin, D. Message Framing and Engagement in Specialty Mental Health Care. Psychiatr. Serv. 2018, 69, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Rothman, A.J.; Salovey, P. Shaping perceptions to motivate healthy behavior: The role of message framing. Psychol. Bull. 1997, 121, 3. [Google Scholar] [CrossRef]
- Meyerowitz, B.E.; Wilson, D.K.; Chaiken, S. Loss-Framed Messages Increase Breast Self-Examination for Women Who Perceive Risk. In Proceedings of the Annual Convention of the American Psychological Society, Washington, DC, USA, 13–16 June 1991. [Google Scholar]
- Hull, S.J. Perceived risk as a moderator of the effectiveness of framed HIV-test promotion messages among women: A randomized controlled trial. Health Psychol. 2012, 31, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Keyworth, C.; Nelson, P.A.; Bundy, C.; Pye, S.R.; Griffiths, C.E.M.; Cordingley, L. Does message framing affect changes in behavioural intentions in people with psoriasis? A randomized exploratory study examining health risk communication. Psychol. Health Med. 2018, 23, 763–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tversky, A.; Kahneman, D. The framing of decisions and the psychology of choice. Science 1981, 211, 453–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, K.M.; Updegraff, J.A. Health message framing effects on attitudes, intentions, and behavior: A meta-analytic review. Ann. Behav. Med. 2012, 43, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Harrington, N.G.; Kerr, A.M. Rethinking Risk: Prospect Theory Application in Health Message Framing Research. Health Commun. 2016, 32, 1–11. [Google Scholar] [CrossRef]
- Maheswaran, D.; Meyers-Levy, J. The Influence of Message Framing and Issue Involvement. J. Mark. Res. 1990, 27, 361–367. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Coley, B. Context framing to enhance HIV-antibody-testing messages targeted to African American women. Health Psychol. 1995, 14, 247–254. [Google Scholar] [CrossRef]
- Block, L.G.; Keller, P.A. When to Accentuate the Negative: The Effects of Perceived Efficacy and Message Framing on Intentions to Perform a Health-Related Behavior. J. Mark. Res. 1995, 32, 192–203. [Google Scholar] [CrossRef]
- Steuer, J. Defining Virtual Reality: Dimensions Determining Telepresence. J. Commun. 1992, 42, 73–93. [Google Scholar] [CrossRef]
- Sundar, S.S. Theorizing interactivity’s effects. Inf. Soc. 2004, 20, 387–391. [Google Scholar] [CrossRef]
- Rafaeli, S.; Sudweeks, F. Networked interactivity. J. Comput. Commun. 1997, 2, JCMC243. [Google Scholar] [CrossRef]
- Lee, J.S. Interactivity: A New Approach; AEJMC: Phoenix, AZ, USA, 2000. [Google Scholar]
- Kiousis, S. Interactivity: A concept explication. New Media Soc. 2002, 4, 355–383. [Google Scholar] [CrossRef]
- Sundar, S.S. Social psychology of interactivity in human-website interaction. In The Oxford Handbook of Internet Psychology; Joinson, A.N., Mckenna, K.Y., Postmes, T., Reips, U.D., Eds.; Oxford University Press: Oxford, UK, 2007; pp. 89–104. ISBN 978-0-1985-6800-1. [Google Scholar]
- Liu, Y.; Shrum, L.J. What is interactivity and is it always such a good thing? Implications of definition, person, and situation for the influence of interactivity on advertising effectiveness. J. Adv. 2002, 31, 53–64. [Google Scholar] [CrossRef]
- Oh, J.; Sundar, S.S. How does interactivity persuade? An experimental test of interactivity on cognitive absorption, elaboration, and attitudes. J. Commun. 2015, 65, 213–236. [Google Scholar] [CrossRef]
- Calisir, F.; Gurel, Z. Influence of text structure and prior knowledge of the learner on reading comprehension, browsing and perceived control. Comput. Hum. Behav. 2003, 19, 135–145. [Google Scholar] [CrossRef]
- Jin, E.; Oh, J. The Effects of Interactivity on the Attitudes and Intentions about Second-hand Smoke: Comparison of Two Mechanisms. Int. J. Human Comput. Interact. 2019, 36, 307–315. [Google Scholar] [CrossRef]
- Yang, F.; Shen, F. Effects of Web Interactivity: A Meta-Analysis. Commun. Res. 2018, 45, 635–658. [Google Scholar] [CrossRef]
- Chaiken, S. The Heuristic—Systematic. Dual-Process Theories in Social Psychology; Chaiken, S., Trope, Y., Eds.; The Guilford Press: New York, NY, USA, 1999; ISBN 978-1-5723-0421-5. [Google Scholar]
- Griffin, R.J.; Dunwoody, S.; Neuwirth, K. Proposed Model of the Relationship of Risk Information Seeking and Processing to the Development of Preventive Behaviors. Environ. Res. 1999, 80, S230–S245. [Google Scholar] [CrossRef] [PubMed]
- Hovick, S.; Freimuth, V.S.; Johnson-Turbes, A.; Chervin, D.D. Multiple health risk perception and information processing among African Americans and Whites living in poverty. Risk Anal. Int. J. 2011, 31, 1789–1799. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Zhao, M.; Wang, F.; Zhao, D. The effects of firm actions on customers’ responses to product recall crises: Analyzing an automobile recall in China. J. Risk Res. 2014, 19, 1–19. [Google Scholar] [CrossRef]
- Fiske, S.T. Attention and weight in person perception: The impact of negative and extreme behavior. J. Pers. Soc. Psychol. 1980, 38, 889–906. [Google Scholar] [CrossRef]
- Meyers-Levy, J.; Maheswaran, D. Exploring Message Framing Outcomes When Systematic, Heuristic, or Both Types of Processing Occur. J. Consum. Psychol. 2004, 14, 159–167. [Google Scholar]
- Kalyanaraman, S.; Sundar, S.S. The Psychological Appeal of Personalized Content in Web Portals: Does Customization Affect Attitudes and Behavior? J. Commun. 2006, 56, 110–132. [Google Scholar] [CrossRef]
- Petty, R.E.; Wegener, D.T. Attitude change: Multiple roles for persuasion variables. In The Handbook of Social Psychology, 4th ed.; Gilbert, D., Fiske, S., Lindzedy, G., Eds.; McGraw-Hill: New York, NY, USA, 1998; pp. 323–390. ISBN 978-0-4701-3747-5. [Google Scholar]
- Zaichkowsky, J.L. Measuring the Involvement Construct. J. Consum. Res. 1985, 12, 341–352. [Google Scholar] [CrossRef]
- Gallagher, K.M.; Updegraff, J.A.; Rothman, A.J.; Sims, L. Perceived susceptibility to breast cancer moderates the effect of gain-and loss-framed messages on use of screening mammography. Health Psychol. 2011, 30, 145. [Google Scholar] [CrossRef] [Green Version]
- Burns, D.D. The Feeling Good Handbook; Plume: New York, NY, USA, 1999; ISBN 978-0-4522-8132-5. [Google Scholar]
- Beevers, C.G.; Miller, I.W. Depression-related negative cognition: Mood-state and trait dependent properties. Cogn. Ther. Res. 2004, 28, 293–307. [Google Scholar] [CrossRef]
- Uskul, A.K.; Sherman, D.K.; FitzGibbon, J. The cultural congruency effect: Culture, regulatory focus, and the effectiveness of gain- vs. loss-framed health messages. J. Exp. Soc. Psychol. 2009, 45, 535–541. [Google Scholar] [CrossRef] [Green Version]
- Ghani, J.A. Flow in human computer interactions: Test of a model. In Human Factors in Information Systems: Emerging Theoretical Bases, 3rd ed.; Carey, J.M., Ed.; Intellect Ltd.: Bristol, UK, 1996; pp. 291–311. [Google Scholar]
- Shipps, B.; Phillips, B. Social networks, interactivity and satisfaction: Assessing socio-technical behavioral factors as an extension to technology acceptance. J. Theor. Appl. Electron. Commer. Res. 2013, 8, 35–52. [Google Scholar] [CrossRef] [Green Version]
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. Risk as Analysis and Risk as Feelings: Some Thoughts about Affect, Reason, Risk, and Rationality. Risk Anal. 2004, 24, 311–322. [Google Scholar] [CrossRef]
- Kahlor, L.; Dunwoody, S.; Griffin, R.J.; Neuwirth, K.; Giese, J. Studying Heuristic-Systematic Processing of Risk Communication. Risk Anal. 2003, 23, 355–368. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Option | ||
|---|---|---|
| Emphasizing possible gains | A: “200 patients are sure to be saved” | B: “A 33% chance of saving all 600 patients and a 66% chance of saving no one” |
| Emphasizing possible loses | C: “400 patients are sure to die” | D: “A 33% chance of no patients dying and a 66% chance of all 600 patients dying” |
| Mean (SD) or Percentage | Range | |
|---|---|---|
| Age | M = 30.70 SD = 7.34 | 18–63 |
| Gender | Male: 122 (45.0%) Female: 147 (55.0%) | |
| Social Media Usage (h) | M = 3.79 SD = 2.28 | 0.50–15.00 |
| Measure | Response Options | Reliability (Cronbach’s Alpha) |
|---|---|---|
| The initial intention to take a depression assessment | 1 (strongly disagree) –5 (strongly agree) | 0.88 |
| ||
| Issue involvement (How you feel about depression) | 1 (close to the adjective on the left)–7 (close to the adjective on the right) | 0.91 |
| ||
| Perceived risk | 1 (extremely unlikely)–5 (extremely likely) | 0.84 |
| ||
| Perceived depression | 1 (not at all)–5 (extremely) | 0.94 |
| ||
| The intention to take a depression assessment | 1 (strongly disagree)–5 (strongly agree) | 0.87 |
|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1 Age | - | ||||||
| 2 SNS use | −0.22 ** | - | |||||
| 3 Initial intention to take depression assessment | −0.01 | −0.69 | - | ||||
| 4 Issue involvement | −0.16 ** | −0.01 | 0.42 ** | - | |||
| 5 Perceived risk | −0.06 ** | 0.06 | 0.70 ** | 0.46 ** | - | ||
| 6 Perceived depression | −0.10 | 0.04 | 0.65 ** | 0.33 ** | 0.70 ** | - | |
| 7 The Intention to take depression assessment | −0.10 | 0.33 | 0.74 ** | 0.52 ** | 0.65 ** | 0.55 ** | - |
| Mean | 30.70 | 3.79 | 2.30 | 4.57 | 2.54 | 2.14 | 2.72 |
| Standard deviation | 7.34 | 2.28 | 0.99 | 1.24 | 2.00 | 0.69 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Q.; Lee, H.E. How Framed Messages Influence Depression Assessment Intentions: Interactivity of Social Media as a Moderator. Int. J. Environ. Res. Public Health 2021, 18, 1787. https://doi.org/10.3390/ijerph18041787
Gao Q, Lee HE. How Framed Messages Influence Depression Assessment Intentions: Interactivity of Social Media as a Moderator. International Journal of Environmental Research and Public Health. 2021; 18(4):1787. https://doi.org/10.3390/ijerph18041787
Chicago/Turabian StyleGao, Quan, and Hye Eun Lee. 2021. "How Framed Messages Influence Depression Assessment Intentions: Interactivity of Social Media as a Moderator" International Journal of Environmental Research and Public Health 18, no. 4: 1787. https://doi.org/10.3390/ijerph18041787