
Menopause, Ultraviolet Exposure, and Low Water Intake Potentially Interact with the Genetic Variants Related to Collagen Metabolism Involved in Skin Wrinkle Risk in Middle-Aged Women



Abstract
1. Background
2. Methods
2.1. Baseline Characteristics of Subjects
2.2. Survey Questionnaires
2.3. Dermal Measurement
2.4. Genotyping, Single Nucleotide Polymorphism (SNP) Imputation, and Quality Control
2.5. GWAS for Wrinkles and Construction of PRS
2.6. Statistical Analysis
3. Results
3.1. Demographical Characteristics and Associations with Wrinkle Risk
3.2. Characteristics of the Three Selected Genetic Variants Related to Wrinkle Risk
3.3. Adjusted ORs for Wrinkle Risk According to the PRSs Generated by Three Selected Collagen Metabolism-Related SNPs
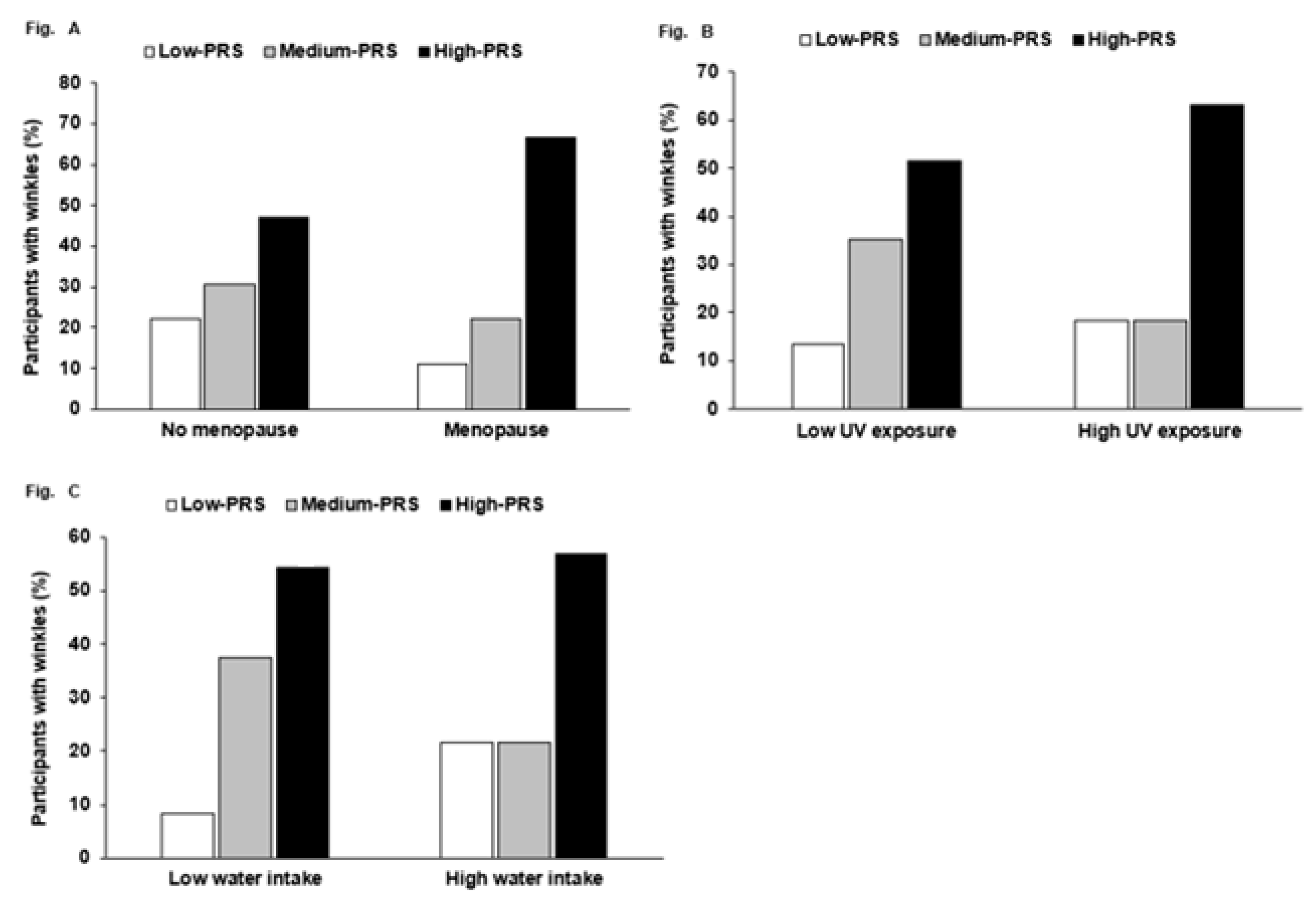
3.4. Interaction of PRS and Lifestyles for Wrinkle Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.M.; Jeon, S.W.; Lee, W.G.; Nam, H.J.; Kim, Y.B. Study of preventing methods for skin aging and wrinkles. J. Physiol. Pathol. Korean Med. 2012, 24, 533–726. [Google Scholar]
- Coté, T.R.; Mohan, A.K.; Polder, J.A.; Walton, M.K.; Braun, M.M. Botulinum toxin type A injections: Adverse events reported to the US Food and Drug Administration in therapeutic and cosmetic cases. J. Am. Acad. Dermatol. 2005, 53, 407–415. [Google Scholar] [CrossRef]
- Makrantonaki, E.; Zouboulis, C.C. Characteristics and pathomechanisms of endogenously aged skin. Dermatology 2007, 214, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Kammeyer, A.; Luiten, R.M. Oxidation events and skin aging. Ageing Res. Rev. 2015, 21, 16–29. [Google Scholar] [CrossRef] [PubMed]
- Pullar, J.M.; Carr, A.C.; Vissers, M.C.M. The roles of vitamin C in skin health. Nutrients 2017, 9, 866. [Google Scholar] [CrossRef]
- Rittie, L.; Fisher, G.J. Natural and sun-induced aging of human skin. Cold Spring Harb. Perspect. Med. 2015, 5, a015370. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Geyer, S.; Weninger, W.; Guimberteau, J.C.; Wong, J.K. The dynamic anatomy and patterning of skin. Exp. Dermatol. 2016, 25, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Zawrotniak, M.; Bartnicka, D.; Rapala-Kozik, M. UVA and UVB radiation induce the formation of neutrophil extracellular traps by human polymorphonuclear cells. J. Photochem. Photobiol. B 2019, 196, 111511. [Google Scholar] [CrossRef]
- Ren, J.; Yang, M.; Chen, J.; Ma, S.; Wang, N. Anti-inflammatory and wound healing potential of kirenol in diabetic rats through the suppression of inflammatory markers and matrix metalloproteinase expressions. Biomed. Pharmacother. 2020, 129, 110475. [Google Scholar] [CrossRef] [PubMed]
- Varani, J.; Dame, M.K.; Rittie, L.; Fligiel, S.E.G.; Kang, S.; Fisher, G.J.; Voorhees, J.J. Decreased collagen production in chronologically aged skin: Roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. Am. J. Pathol. 2006, 168, 1861–1868. [Google Scholar] [CrossRef]
- Kim, M.; Park, Y.G.; Lee, H.-J.; Lim, S.J.; Nho, C.W. Youngiasides A and C isolated from Youngia denticulatum inhibit UVB-Induced MMP expression and promote type I procollagen production via repression of MAPK/AP-1/NF-κB and activation of AMPK/Nrf2 in HaCaT cells and human dermal fibroblasts. J. Agric. Food Chem. 2015, 63, 5428–5438. [Google Scholar] [CrossRef] [PubMed]
- Moon, N.R.; Kang, S.; Park, S. Consumption of ellagic acid and dihydromyricetin synergistically protects against UV-B induced photoaging, possibly by activating both TGF-β1 and wnt signaling pathways. J. Photochem. Photobiol. B 2018, 178, 92–100. [Google Scholar] [CrossRef]
- Rawlings, A.V. Ethnic skin types: Are there differences in skin structure and function? J. Cosmet. Sci. 2006, 28, 79–93. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Gao, W.; Koellmann, C.; Le Clerc, S.; Huls, A.; Li, B.; Peng, Q.; Wu, S.; Ding, A.; Yang, Y.; et al. Genome-wide scan identified genetic variants associated with skin aging in a Chinese female population. J. Dermatol. Sci. 2019, 96, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Tan, J.; Huls, A.; Ding, A.; Liu, Y.; Matsui, M.S.; Vierkotter, A.; Krutmann, J.; Schikowski, T.; Jin, L.; et al. Genetic variants associated with skin aging in the Chinese Han population. J. Dermatol. Sci. 2017, 86, 21–29. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cho, S.B.; Kim, H.-J.; Kim, H.; Yoo, K.H. Argon plasma: A new approach for the effective treatment of inflammatory acne vulgaris and enlarged pores in asian patients. Med. Lasers 2018, 7, 97–101. [Google Scholar] [CrossRef]
- Chan, I.L.; Cohen, S.; da Cunha, M.G.; Maluf, L.C. Characteristics and management of Asian skin. Int. J. Dermatol. 2019, 58, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kim, J.I.; Yang, Y.J.; Nam, J.H.; Kim, W.S. Treatment of periorbital wrinkles with a novel fractional radiofrequency microneedle system in dark-skinned patients. Dermatol. Surg. 2015, 41, 615–622. [Google Scholar] [CrossRef]
- Hwang, J.-Y.; Lee, H.J.; Go, M.J.; Jang, H.B.; Park, S.I.; Kim, B.-J.; Lee, H.-J. An integrative study identifies KCNC2 as a novel predisposing factor for childhood obesity and the risk of diabetes in the Korean population. Sci. Rep. 2016, 6, 33043. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Bagci, I.S.; Ruini, C.; Niesert, A.C.; Horvath, O.N.; Berking, C.; Ruzicka, T.; von Braunmuhl, T. Effects of short-term moisturizer application in different ethnic skin types: Noninvasive assessment with optical coherence tomography and reflectance confocal microscopy. Skin Pharmacol. Physiol. 2018, 31, 125–133. [Google Scholar] [CrossRef]
- Mercurio, D.G.; Jdid, R.; Morizot, F.; Masson, P.; Maia Campos, P.M. Morphological, structural and biophysical properties of French and Brazilian photoaged skin. Br. J. Dermatol. 2016, 174, 553–561. [Google Scholar] [CrossRef]
- Baroni, E.d.R.V.; Biondo-Simoes, M.d.L.P.; Auersvald, A.; Auersvald, L.A.; Montemor Netto, M.R.M.; Ortolan, M.C.; Kohler, J.N. Influence of aging on the quality of the skin of white women: The role of collagen. Acta Cir. Bras. 2012, 27, 736–740. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Romana-Souza, B.; Silva-Xavier, W.; Monte-Alto-Costa, A. Topical retinol attenuates stress-induced ageing signs in human skin ex vivo, throughEGFR activation viaEGF, but notERK andAP-1 activation. Exp. Dermatol. 2019, 28, 906–913. [Google Scholar] [CrossRef]
- Lee, W.J.; Ahn, H.M.; Roh, H.; Na, Y.; Choi, I.K.; Lee, J.H.; Kim, Y.O.; Lew, D.H.; Yun, C.O. Decorin-expressing adenovirus decreases collagen synthesis and upregulates MMP expression in keloid fibroblasts and keloid spheroids. Exp. Dermatol. 2015, 24, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Matsumura, H.; Kato, T.; Ichinose, S.; Takada, A.; Namiki, T.; Asakawa, K.; Morinaga, H.; Mohri, Y.; De Arcangelis, A.; et al. Stem cell competition orchestrates skin homeostasis and ageing. Nature 2019, 568, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Shaver, J.L.; Woods, N.F. Sleep and menopause: A narrative review. Menopause 2015, 22, 899–915. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Nayak, A.; Narayan, R.; Nayak, U.Y. Anti-aging and sunscreens: Paradigm shift in cosmetics. Adv. Pharm. Bull. 2019, 9, 348–359. [Google Scholar] [CrossRef]
- Iizaka, S.; Nagata, S.; Sanada, H. Nutritional status and habitual dietary intake are associated with frail skin conditions in community-dwelling older people. J. Nutr. Health Aging 2017, 21, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, T.; Tsunenaga, M.; Miyanaga, M.; Ueda, O.; Ogo, M. Oral intake of lingonberry and amla fruit extract improves skin conditions in healthy female subjects: A randomized, double-blind, placebo-controlled clinical trial. Biotechnol. Appl. Biochem. 2019, 66, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, H.N.; Hardman, M.J. The role of estrogen in cutaneous ageing and repair. Maturitas 2017, 103, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Yeager, D.G.; Lim, H.W. What’s New in photoprotection: A review of new concepts and controversies. Dermatol. Clin. 2019, 37, 149–157. [Google Scholar] [CrossRef]
- Franco, O.H.; Chowdhury, R.; Troup, J.; Voortman, T.; Kunutsor, S.; Kavousi, M.; Oliver-Williams, C.; Muka, T. Use of plant-based therapies and menopausal symptoms: A systematic review and meta-analysis. JAMA 2016, 315, 2554–2563. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Li, N.; Yan, Y.-Q.; Liu, Y.; Xiong, K.; Liu, Y.; Xia, Q.-M.; Zhang, H.; Liu, Z.-D. Recent advances in the anti-aging effects of phytoestrogens on collagen, water content, and oxidative stress. Phytother. Res. 2020, 34, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Crane, J.D.; MacNeil, L.G.; Lally, J.S.; Ford, R.J.; Bujak, A.L.; Brar, I.K.; Kemp, B.E.; Raha, S.; Steinberg, G.R.; Tarnopolsky, M.A. Exercise-stimulated interleukin-15 is controlled by AMPK and regulates skin metabolism and aging. Aging Cell 2015, 14, 625–634. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Question Category | Main Questions | Answers |
|---|---|---|
| Personal condition | Age | ( ) |
| Sun exposure | ( ) hours | |
| Having metabolic diseases | Yes or no | |
| Menopause | No, yes with HRT treatment, or yes without treatment | |
| Sleep | Normal or cannot sleep because of mental stress | |
| Tiredness | Normal or tired | |
| Exercise | Outside, inside, or none | |
| UV exposure | Less than 1 h/day, 1~3 h/day, or >3 h/day | |
| Sunscreen usage | Always, sometimes, rarely, or not at all | |
| Food and water intake | Vitamin supplementation | Fatigue recovery: yes, no, or not sure |
| Fruit or fruit juice intake | Every day, occasionally (1–2 times/week), or rarely | |
| Fried food intake | Every day, occasionally (1–2 times/week), or rarely | |
| Water intake | ( ) glasses 1 per day | |
| Coffee intake | ( ) cups 1 per day | |
| Fast food intake | Frequently, occasionally (1–2 times/week), or rarely |
| Less-Wrinkled (n = 51) | Wrinkled (n = 77) | Adjusted ORs (95% CI) c | |
|---|---|---|---|
| Age (years) | 52.4 ± 7.0 a | 56.3 ± 9.2 * | 4.221 (0.345–10.01) d |
| Fitzpatrick skin type (scores) | |||
| 3 | 13 (25.4) b | 11 (14.3) | 1 |
| 4 | 35 (68.6) | 42 (54.5) | 1.166 (0.364–3.741) |
| 5 | 3 (5.88) | 24 (31.3) ** | 6.526 (1.093–38.95) * |
| Menopause (Yes, %) | 10 (19.6) | 44 (57.1) *** | 1.285 (0.268–6.163) e |
| UV exposure (Yes, %) | 18 (35.3) | 32 (41.6) | 1.253 (0.400–3.928) f |
| Sunscreen application (No, %) | 33 (64.7) | 33 (42.9) * | 3.806 (0.297–48.72) g |
| Water intake (cups/day) | 3.51 ± 2.04 | 3.59 ± 2.07 | 0.629 (0.216–1.831) h |
| Coffee intake (cups/day) | 1.10 ± 1.22 | 1.03 ± 1.41 | 0.861 (0.292–2.536) i |
| Alcohol intake (Yes, %) | 20 (39.2) | 37 (48.1) | 1.163 (0.382–3.542) j |
| Fruit intake (serving/day) | 2.06 ± 0.63 | 1.72 ± 0.64 * | 0.062 (0.001–0.772) k,* |
| Vitamin supplementation (Yes, %) | 43 (84.3) | 43 (55.8) ** | 0.056 (0.007–0.428) l,*** |
| Smoking (Yes, %) | 2 (3.92) | 5 (6.49) | 1.770 (0.062–50.6) m |
| Exercise (Yes, %) | 37 (72.5) | 37 (48.1) * | 0.540 (0.183–1.596) n |
| Sleep deprivation (Yes, %) | 33 (64.7) | 57 (74.0) | 1.375 (0.368–5.135) o |
| Tiredness after awakening (Yes, %) | 12 (29.4) | 40 (51.9) * | 2.314 (0.668–8.012) p |
| Chr a | SNP | Position | Mi b | Ma c | ORs (95% CI) d | p-Value for ORs e | MAF f | p-Value for HWE g | Gene | Feature |
|---|---|---|---|---|---|---|---|---|---|---|
| 7 | rs1861003 | 55184849 | G | A | 0.282 (0.083–0.952) | 4.14 × 10−2 | 0.1078 | 0.599 | EGFR | intron |
| 8 | rs6469206 | 88072463 | G | T | 0.481 (0.244–0.949) | 3.48 × 10−2 | 0.4752 | 0.4251 | MMP16 | intron |
| 10 | rs805698 | 104057158 | T | C | 11.49 (2.225–76.08) | 4.40 × 10−3 | 0.1127 | 0.3557 | COL17A1 | missense |
| 4 | rs4697073 | 24799121 | A | G | 0.206 (0.045–0.949) | 4.27 × 10−2 | 0.0546 | 1 | SOD3 | intron |
| 20 | rs1291206 | 63697816 | A | G | 2.76 (1.34–5.66) | 5.71 × 10−3 | 0.3614 | 0.5168 | TNFRSF6B | intron |
| 1 | rs6690493 | 12075469 | G | A | 0.189 (0.064–0.553) | 2.38 × 10−3 | 0.2108 | 0.2295 | TNFRSF8 | intron |
| 12 | rs9658535 | 117219805 | C | T | 3.81 (1.42–10.2) | 7.74 × 10−3 | 0.1765 | 0.7314 | NOS1 | intron |
| Low PRS a (n = 25) | Medium PRS (n = 48) | High PRS (n = 55) | |
|---|---|---|---|
| Age (yrs) | 52.4 ± 2.27 | 50.3 ± 1.61 | 53.1 ± 1.50 |
| Menopause (Yes, %) | 13 (52.0) | 19 (39.6) | 23 (41.8) |
| UV exposure (Yes, %) | 9 (36.0) | 7 (35.4) | 24 (43.6) |
| Sunscreen usage (No, %) | 16 (64.0) | 31 (64.6) | 31 (56.4) |
| Water intake (cups/day) | 2.89 ± 0.56 | 3.59 ± 0.40 | 3.87 ± 0.37 |
| Coffee intake (cups/day) | 1.06 ± 0.36 | 0.95 ± 0.25 | 1.26 ± 0.23 |
| Alcohol intake (Yes, %) | 13 (52.0) | 29 (60.4) | 29 (52.7) |
| Fruit intake (serving/day) | 1.93 ± 0.17 | 0.95 ± 0.25 | 1.26 ± 0.23 |
| Vitamin supplementation (Yes, %) | 20 (80.0) | 31 (64.6) | 36 (65.5) |
| Smoking (Yes, %) | 1 (4.0) | 2 (4.2) | 2 (3.6) |
| Exercise (Yes, %) | 9 (36.0) | 29 (60.4) | 37 (67.3) |
| Sleep deprivation (Yes, %) | 5 (20.0) | 18 (37.5) | 25 (45.5) |
| Tiredness after awakening (Yes, %) | 19 (76.0) | 27 (56.3) | 44 (80.0) |
| Low PRS a (n = 25) | Medium PRS (n = 48) | High PRS (n = 55) | |
|---|---|---|---|
| Wrinkles | 1 b | 1.037 (0.175–6.153) c | 15.39 (2.480–120.5) *** |
| Refraction of the skin surface | 1 | 0.193 (00035–1.077) | 0.668 (0.144–3.088) |
| Melanin deposition | 1 | 0.690 (0.138–3.460) | 1.178 (0.242–5.735) |
| Browning color | 1 | 5.376 (0.266–108.5) | 2.781 (0.154–50.22) |
| Blushing | 1 | 0.482 (0.099–2.336) | 1.106 (0.230–5.328) |
| Gloss | 1 | 7.473 (0.994–55.63) | 5.060 (0.617–41.51) |
| Pore size | 1 | 0.702 (0.137–3.592) | 10.64 (1.269–89.23) ** |
| Fitzpatrick skin type d | 1 | 0.788 (0.178–3.494) | 1.908 (0.396–9.201) |
| Wrinkles | Pore Size | |
|---|---|---|
| Skin wrinkles | 1.0 | 0.609 *** |
| Reflection of skin surface | 0.155 | 0.112 |
| Melanin deposition | 0.398 *** | 0.436 *** |
| Brown skin color | 0.285 ** | 0.235 * |
| Blushing | 0.099 | 0.105 |
| Gloss | −0.042 | 0.189 |
| Pore size | 0.609 *** | 1.0 |
| Fitzpatrick skin type | 0.352 *** | 0.520 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Kang, S.; Lee, W.J. Menopause, Ultraviolet Exposure, and Low Water Intake Potentially Interact with the Genetic Variants Related to Collagen Metabolism Involved in Skin Wrinkle Risk in Middle-Aged Women. Int. J. Environ. Res. Public Health 2021, 18, 2044. https://doi.org/10.3390/ijerph18042044
Park S, Kang S, Lee WJ. Menopause, Ultraviolet Exposure, and Low Water Intake Potentially Interact with the Genetic Variants Related to Collagen Metabolism Involved in Skin Wrinkle Risk in Middle-Aged Women. International Journal of Environmental Research and Public Health. 2021; 18(4):2044. https://doi.org/10.3390/ijerph18042044
Chicago/Turabian StylePark, Sunmin, Suna Kang, and Woo Jae Lee. 2021. "Menopause, Ultraviolet Exposure, and Low Water Intake Potentially Interact with the Genetic Variants Related to Collagen Metabolism Involved in Skin Wrinkle Risk in Middle-Aged Women" International Journal of Environmental Research and Public Health 18, no. 4: 2044. https://doi.org/10.3390/ijerph18042044
APA StylePark, S., Kang, S., & Lee, W. J. (2021). Menopause, Ultraviolet Exposure, and Low Water Intake Potentially Interact with the Genetic Variants Related to Collagen Metabolism Involved in Skin Wrinkle Risk in Middle-Aged Women. International Journal of Environmental Research and Public Health, 18(4), 2044. https://doi.org/10.3390/ijerph18042044