1. Introduction
School-based smoking preventive initiatives are widely used, and, if well implemented, have the possibility to help prevent a new generation from starting to smoke [
1]. They may further help prevent or decrease socioeconomic inequality later in life [
2].
Some have argued that interventions themselves may generate or increase socioeconomic inequalities in smoking prevalence [
3]. This may be due to different aspects of the implementation process—i.e., access to materials and tools, uptake, and compliance [
4]. Therefore, it is important that smoking preventive initiatives aim at being equally effective across socioeconomic groups [
5] or at being more effective among individuals from low socioeconomic positions.
Generally, the best effect of school-based smoking prevention is seen in interventions that target adolescent smoking from multiple sides simultaneously—i.e., structural as well as individual initiatives [
1]. Among structural initiatives are, for example, smoke-free policies implemented for all pupils and/or staff at the same time, whereas smoke-free contracts or dialogues between parents and children are oriented at the individual pupil and require action from each individual participant. Therefore, there is a risk that especially individually oriented initiatives in the school setting may be implemented differently among pupils, causing inequalities in the intervention effect [
6].
In Denmark, there is no significant difference in smoking among boys and girls in younger age groups [
7]. However, boys and girls may have different reasons for smoking initiation [
8], and gender may also play an important role in the implementation of smoking preventive activities. Among other factors, gender affects decision-making, engagement, and preferences for intervention uptake [
9]. Overall, there is a variety of determinants for adolescent smoking at different levels—i.e., in individual, social, and societal levels. Adolescents with lower socio-economic backgrounds are at higher risk of smoking initiation, as well as adolescents with low academic performance [
10,
11]. At the social level are peer and parental behavior and attitudes, whereas the societal level includes restrictions and advertising [
11].
Most evaluations of school-based smoking prevention have not addressed these aspects and therefore the mechanisms behind any inequality in individual intervention uptake is unknown. We hypothesized that families of higher socioeconomic position more often would sign the smoke-free contract. To our knowledge, there are no studies of the implementation of smoke-free contracts in relation to family socioeconomic position or gender. Therefore, the aim of this study was to examine the implementation of a smoke-free contract. Specifically, we examined the intervention uptake across family occupational social class (OSC) separately for boys and girls, the joint effect of OSC and gender, and the participants’ own reasons for not signing a contract.
2. Methods
2.1. Evaluation of the X:IT Intervention
This study is based upon data from an effective smoking preventive intervention X:IT which was evaluated in a cluster randomized controlled trial with 97 schools in 2010–2013. Overall, X:IT was effective in preventing adolescent smoking; the odds ratio for smoking among pupils in intervention schools compared to the control group after one year of intervention was 0.61 (95% CI: 0.45–0.81) [
12]. A thorough assessment of the school-wise implementation showed that one fourth of the participating schools succeeded in implementing all three intervention components as prescribed in the program. Schools with a high implementation showed reduced risk for pupil smoking, with an odds ratio of 0.44 (95% CI: 0.32–0.68) [
13].
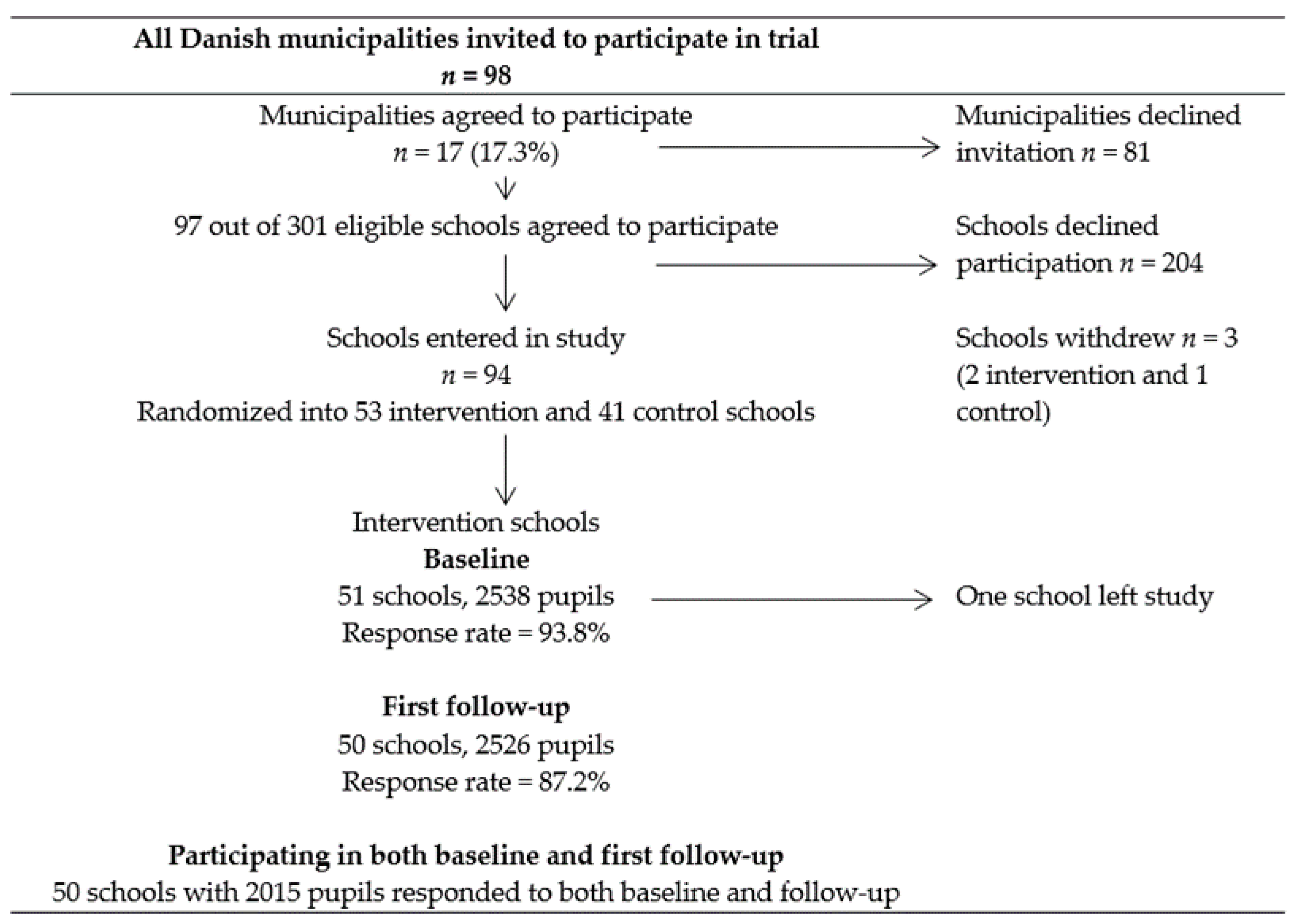
2.2. Study Population
All the 98 Danish municipalities were invited to join the X:IT study and 17 agreed to participate (17.3%). A total of 97 of 302 eligible schools were enrolled (32.1%). Schools were randomly assigned to either the intervention or control group using a stratified simple randomization procedure, meaning that, within each municipality, schools had an equal chance of becoming an intervention or control school. All the pupils from seventh grade (13-year-olds) were invited to participate (
n = 4468). This paper was restricted to pupils from intervention schools with responses to baseline and first follow-up (
n = 2015). See the flowchart in
Figure 1.
2.3. The X:IT Intervention
The main intervention components were (1) smoke-free school grounds implemented at the school level (no smoking for pupils, teachers, or visitors at school), (2) curricular activities implemented at the school class level (at least eight lessons a year for three years from a specially developed curricular material), and (3) smoke-free contracts between parents and their children implemented at the individual level. Further details about the intervention can be found in the X:IT study protocol [
14].
The smoke-free contract.
The smoke-free contracts were handed out to pupils at the beginning of the school year. Teachers handled the distribution of contracts during a school lesson. One part of the contract should be kept at home, preferably at a visible place, and the other part returned to the teacher. By signing the contract, the pupil promised to stay smoke-free for the following year, and the parent committed oneself to help create a smoke-free environment around the child.
2.4. Measures
Pupils answered a web-based questionnaire during a school lesson after a standardized instruction given by the teacher.
The outcome was the smoke-free contract. Pupils were asked to report whether they had signed a smoke-free contract in the beginning of the school year. We dichotomized responses into yes vs. no/I do not know.
Socioeconomic position was measured as family occupational social class (OSC) based on pupils’ responses to two items on father’s and mother’s occupations (work place and job function). The pupils’ information on parental occupation was coded from (I) high to (V) low social class and (VI) indicating parents receiving social benefits. Family occupational social class was then determined by the highest-ranking parent according to the standards of the Danish National Institute of Social Research. This coding is almost similar to the Registrar General classification used in the UK [
15]. In the joint effect analysis, OSC was grouped into three categories: high (I+II), medium (III+IV), and low (V+VI).
Current smoking among pupils was measured by: How often do you smoke? Responses were dichotomized in “Daily”, “Weekly”, “Monthly”, or “More seldom” vs. “Never”.
Pupils, who responded ‘no’ to having a contract were asked about the reason: “Why didn´t you sign a contract?” Response options included: “I smoke”, “My parents wouldn´t sign the contract”, “I just didn´t do it”, or “I never received a contract”.
2.5. Statistical Analyses
Due to a substantial number of missing on the variable measuring occupational social class, we used a dataset with imputed values for the missing items. We performed multistage imputation and two rounds of 20 imputations as recommended by Graham (2012). [
16]. The agreement between the original and the imputed data set was good [
10].
We performed multiple logistic regression analyses to estimate the odds ratio for having a signed contract, with girls from a high OSC as the reference group. We used the Proc mianalyze procedure in SAS version 9.3. We provided a crude analysis and an adjusted analysis that considered pupils own smoking at baseline, as this may influence the probability of signing a smoke-free contract.
3. Results
Descriptive statistics are provided in the left part of
Table 1. Overall, 81.8% of the pupils signed a contract. The proportion was higher among girls compared to boys—85.1 vs. 78.6% (
p = 0.001).
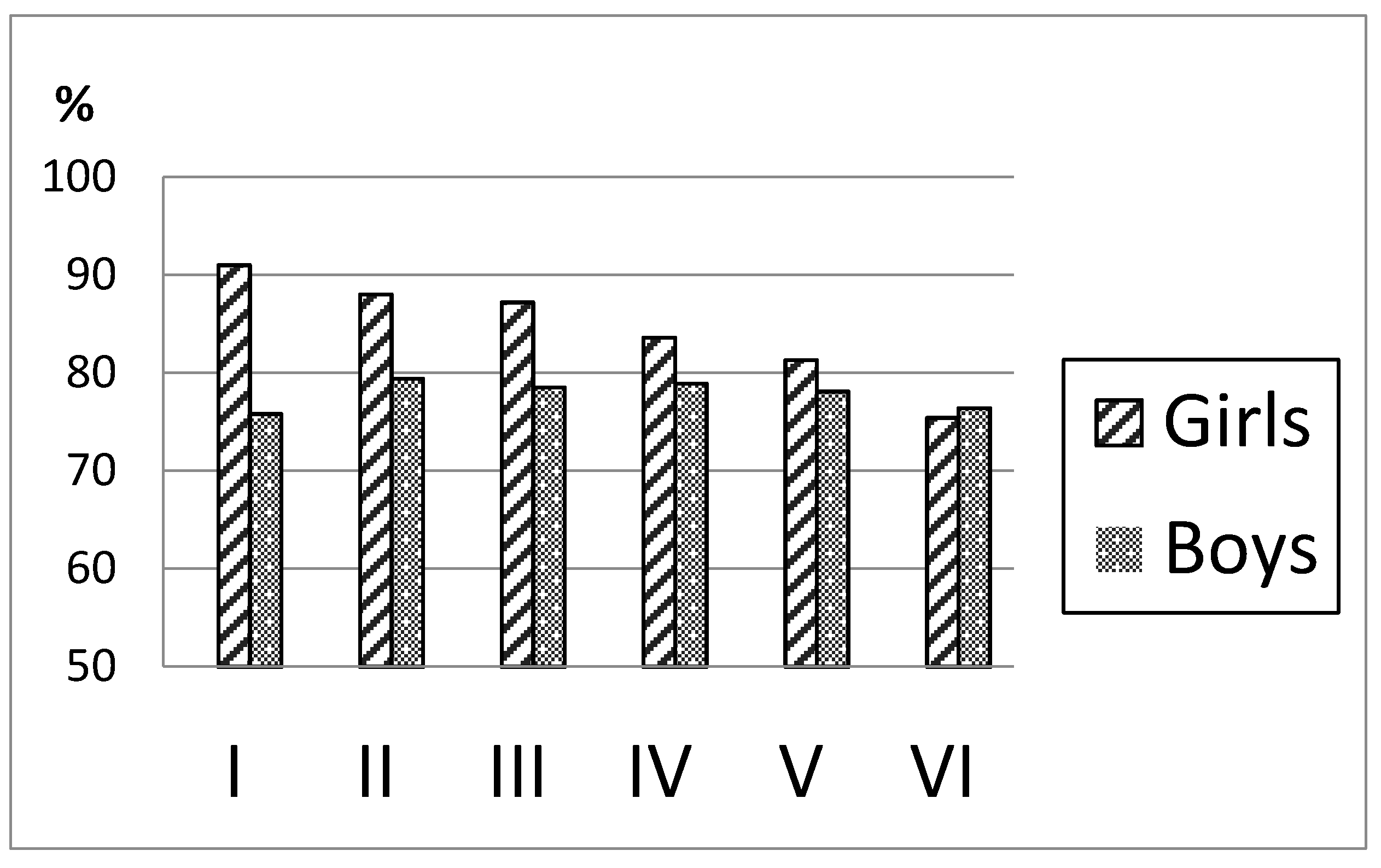
As seen in
Figure 2, there was a clear social gradient in contracts among girls, with more than 90% in OSC group I vs. 75% in group VI. Among boys, however, we found no differences across the socioeconomic groups.
When examining the combined effect of OSC and gender, we saw that the boys in all socioeconomic groups had about half the odds of signing a smoke-free contract compared to girls from high OSC. Girls in low OSC had odds that corresponded to boys—0.56 (0.33–0.97)—whereas the odds for girls from a medium OSC were 0.76 (0.50–1.19) (results presented on the right side of
Table 1).
Among pupils with no smoke-free contract (49 girls and 65 boys), the main reasons for not having a contract were the same for boys and girls; that they never received a contract or that there were no specific reasons for not signing.
The question, “Why didn´t you sign a contract?”, was answered by “I smoke” (8.2% girls, 6.2% boys); “My parents wouldn´t sign the contract” (2.0% girls, 10.8% boys); “I just didn´t do it” (53.1% girls, 52.3% boys); “I never received a contract” (49.0% girls, 44.6% boys).
4. Discussion
We found that more girls compared to boys signed a smoke-free contract with their parents; however, the overall compliance for both genders was high. Further, we showed a social gradient in signed contracts for girls, so that more girls from higher OSCs had a contract. When examining the combined effect of OSC and gender, we saw that the boys from all OSC had about half the odds of signing a smoke-free contract compared to girls from the highest OSC. Only few studies examined the combined effect of OSC and gender among adolescents [
17]. It has been argued that differences in socializing patterns between boys and girls may explain differences in health-related behavior according to socioeconomic position [
17], which also may apply here. In example, boys tend to cope with development in a more externalized way, whereas girls tend to be more internally focused [
17].
We found that girls from a higher OSC more often signed a contract, whereas boys in all OSCs and girls from the lower OSCs had lower proportions of signed contracts. Several studies have found a link between smoking and OSC [
18,
19]. A possible explanation for this is that parents with higher versus lower educational attainment may be more concerned about the health risks of smoking because of their greater knowledge about them [
19]; however, it is surprising that our study did not detect a OSC gradient for boys. When trying to explain these OSC and gender-related differences, it can be important to look at the different steps in relation to the implementation of the contracts. First, contracts should be handed out to all participating pupils. As contracts were handed out by teachers during a school lesson, we assume no systematic differences according to socioeconomic position or gender in this step
Next, the contract was brought home by the children and (hopefully) shown to parents. Fewer boys than girls signed a contract, which may be related to this step; girls may generally be better at involving parents in school activities. However, the difference may also be explained by other factors such as maturity; boys in this age are more immature than girls—and boys may not perceive the contract as important, or the simply may forget the contract in the bag. However, we found no markedly different reasons for not having a contract when asking the children themselves.
Afterwards, the children and parents should preferably talk about the contract and smoking related issues in general and thereafter both sign the contract. We do not know how this is done and what happens at home in this situation. Two previous studies observed parents and children having conversations about smoking and tobacco and found positive associations between the quality of these conversations and not starting to smoke or not increasing smoke. None of these studies, however, examined whether there were differences according to gender of the child [
20,
21].
As a part of the evaluation of X:IT, we conducted interviews with parents from lower socioeconomic positions. Generally, parents from low socioeconomic positions did not recognize themselves and their children in the materials; the persons pictured did not look like them and the wording was too academic. This may explain some of the tendency towards the lower proportions of contracts among these groups, at least among girls. The missing social gradient among boys may imply different mechanisms for boys and girls. Boys may be more strongly influenced by other factors—i.e., youth culture or general peer influence—or families with teenage boys may not talk about smoking and tobacco-related issues to the same extent as families with teenage girls.
5. Limitations
Data were self-reported and thereby the results could be biased by social desirability for having a signed contract, as well as being a non-smoker. However, self-reporting is regarded as a valuable method of gaining insight into pupils’ explicit attitudes, experiences and behaviors, and we know from previous studies that adolescents can answer items about smoking with good validity [
22,
23]. Further, answers about signed contracts from the questionnaire data corresponded well with copies of the actual contracts, and therefore we believe that they are able to answer this question. Lastly, we assume that asking adolescents themselves about their own behavior provides the best picture of their lives. The use of questionnaire data among pupils limits our ability to gain insight into the situation where the families talked about tobacco and signed the contract. We cannot eliminate the risk that the quality of this situation is associated to factors such as parental smoking status. However, previous research underlines the fact that parents that are smokers themselves can talk to their kids about anti-smoking issues in an effective way [
24].
The schools included in this study were not randomly selected. Participation could be motivated by a high prevalence of smoking or a high level of resources and a general focus on health, potentially more profound among schools with low levels of smoking. The direction of this possible selection bias is unknown. However, the possibility for each participating school to become an intervention or a control school was completely random, and this issue is assumed to have no influence on the social gradient in signed smoke-free contracts.
6. Conclusions
From a public health point of view, the differential implementation of the contract according to socioeconomic position could potentially widen the social inequality in smoking. Future interventions should ensure that all OSC groups are equally represented in the selection and randomization and take into account the fact that different strategies may appeal to adolescents and families of different socioeconomic positions. Further, boys and girls may benefit from different initiatives.
Author Contributions
L.S.B., S.A., S.G., M.T.D. and A.A. made substantial contributions to conception and design. L.S.B. analyzed the data and drafted the manuscript and all authors revised it critically. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the TrygFoundation and the Danish Cancer Society. The Danish Cancer Society developed and implemented the X:IT intervention in schools. Funding bodies did not have any influence on the process of evaluating, analyzing, or reporting the results, or in the manuscript writing.
Institutional Review Board Statement
In Denmark, there is no formal institution for ethical assessment and approval of questionnaire-based population studies. The X:IT study is registered at the Danish Data Protection Agency, ref: 2010-54-0930. Schools were invited through written information to the school headmaster.
Informed Consent Statement
Students and their parents were informed about the study, that participation was voluntary, and that their information was used for research only and treated with confidence. Parents were informed that they could have their child withdrawn from study at any point in time. We did not collect written consent from parents. We used passive verbal consent to minimize non-participance and optimize the representativeness of participants.
Data Availability Statement
Data are available upon request.
Acknowledgments
We wish to thank participating schools and municipalities in the X:IT Study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Thomas, R.E.; McLellan, J.; Perera, R. School-based programmes for preventing smoking. Interv. Rev. 2013. [Google Scholar] [CrossRef]
- Due, P.; Krolner, R.; Rasmussen, M.; Andersen, A.; Damsgaard, M.T.; Graham, H.; Holstein, B.E. Pathways and mechanisms in adolescence contribute to adult health inequalities. Scand. J. Public Health 2011, 39 (Suppl. 6), 62–78. [Google Scholar] [CrossRef]
- Lorenc, T.; Petticrew, M.; Welch, V.; Tugwell, P. What types of interventions generate inequalities? Evidence from systematic reviews. J. Epidemiol. Community Health 2013, 67, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Tugwell, P.; de Savigny, D.; Hawker, G.; Robinson, V. Applying clinical epidemiological methods to health equity: The equity effectiveness loop. Br. Med J. 2006, 332, 358–361. [Google Scholar] [CrossRef]
- Lynch, J.; Law, C.; Brinkman, S.; Sawyer, M. Inequalities in child healthy development: Some challenges for effective implementation. Soc. Sci. Med. 2010, 71, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
- McLaren, L.; McIntyre, L.; Kirkpatrick, S. Rose’s population strategy of prevention need not increase social inequalities in health. Int. J. Epidemiol. 2010, 39, 372–377. [Google Scholar] [CrossRef]
- Rasmussen, M.; Pedersen, T.P.; Due, P. Skolebørnsundersøgelsen 2014 [Health Behaviour in School Aged Children]; National Institute of Public Health: Copenhagen, Denmark, 2015. [Google Scholar]
- Okoli, C.; Greaves, L.; Fagyas, V. Sex differences in smoking initiation among children and adolescents. Public Health 2013, 127, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Tannenbaum, C.; Greaves, L.; Graham, I.D. Why sex and gender matter in implementation research. BMC Med Res. Methodol. 2016, 27, 145. [Google Scholar] [CrossRef] [PubMed]
- Doku, D.T.; Acacio-Claro, P.J.; Koivusilta, L.; Rimpelä, A. Social determinants of adolescent smoking over three generations. Scand. J. Public Health 2020, 48, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Geckova, A.; van Dijk, J.P.; van Ittersum-Gritter, T.; Groothoff, J.W.; Post, D. Determinants of adolescents’ smoking behaviour: A literature review. Cent. Eur. J. Public Health 2002, 10, 79–87. [Google Scholar]
- Andersen, A.; Krølner, R.; Bast, L.S.; Thygesen, L.C.; Due, P. Effects of the X:IT smoking intervention: A school-based cluster randomised trial. Int. J. Epidemiol. 2015, 44, 1900–1908. [Google Scholar] [CrossRef]
- Bast, L.S.; Due, P.; Bendtsen, P.; Ringgaard, L.; Wohllebe, L.; Damsgaard, M.T.; Grønbæk, M.; Ersbøll, A.K.; Andersen, A. High impact of implementation on school-based smoking prevention: The X:IT Study—A randomized smoking prevention trial. Implement. Sci. 2016, 11, 125. [Google Scholar] [CrossRef]
- Andersen, A.; Bast, L.S.; Ringgaard, L.W.; Wohllebe, L.; Jensen, P.D.; Svendsen, M.; Dalum, P.; Due, P. Design of a school-based randomised trial to reduce smoking among 13-15 year olds, the X:IT study. BMC Public Health 2014, 14, 518. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, S.; McKay, L.; Der, G.; Hiscock, R. Socio-economic position and health: What you observe depends on how you measure it. J. Public Health Med. 2003, 25, 288–294. [Google Scholar] [CrossRef]
- Graham, J.W. Multiple imputation and analysis with multilevel (cluster) data. In Missing Data: Analysis and Design, Statistics for Social and Behavioral Sciences; Springer Science + Business Media: New York, NY, USA, 2012. [Google Scholar]
- Pitel, L.; Gecková, M.A.; Reijneveld, S.A.; van Dijk, J.P. Socioeconomic differences in adolescent health-related behavior differ by gender. J. Epidemiol. 2013, 23, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Conrad, K.M.; Flay, B.R.; Hill, D. Why children start smoking cigarettes: Predictors of onset. Br. J. Addict. 1992, 87, 1711–1724. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.S.; Chassin, L.; Presson, C.C. Demographic factors in adult smoking status: Mediating and moderating influences. Psychol. Addict. Behav. 1996, 10, 28–37. [Google Scholar] [CrossRef]
- Wakschlag, L.S.; Metzger, A.; Darfler, A.; Ho, J.; Mermelstein, R.; Rathouz, P.J. The Family Talk About Smoking (FTAS) paradigm: New directions for assessing parent-teen communications about smoking. Nicotine Tob. Res. 2011, 13, 103–112. [Google Scholar] [CrossRef]
- Richmond, M.J.; Mermelstein, R.J.; Wakschlag, L.S. Direct observations of parenting and real-time negative affect among adolescent smokers and nonsmokers. J. Clin. Child Adolesc. Psychol. 2013, 42, 617–628. [Google Scholar] [CrossRef]
- Kentala, J.; Utriainen, P.; Pahkala, K.; Mattila, K. Verification of adolescent self-reported smoking. Addict. Behav. 2004, 29, 405–411. [Google Scholar] [CrossRef]
- Post, A.; Gilljam, H.; Rosendahl, I.; Meurling, L.; Bremberg, S.; Galanti, M.R. Validity of self reports in a cohort of Swedish adolescent smokers and smokeless tobacco (snus) users. Tob. Control 2005, 14, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Harakeh, Z.; Scholte, R.H.J.; de Vries, H.; Engels, R.C.M.E. Parental rules and communication: Their association with adolescent smoking. Addiction 2005, 100, 862–870. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}