1. Introduction
Oral anticoagulants (OAs) are used to prevent stroke in atrial fibrillation (AF). The American guidelines recommend using warfarin, a vitamin K antagonist (VKA), and direct-acting oral anticoagulants (DOACs) to prevent stroke in AF in patients with CHA2DS2-VASC ≥ 2, taking into account individual risk/benefit of bleeding [
1]. The European Society of Cardiology guidelines recommend the use of DOACs as first-line treatment for non-valvular atrial fibrillation (NVAF) [
2].
In Catalonia, anticoagulant therapy for NVAF follows the “Informe de Posicionamiento terapéutico” (IPT) (Therapeutic Positioning Report) and the “Pautes per a l’harmonització del tractament” (PHT) (Therapeutic Harmonization Guidelines for the Use of Oral Anticoagulants) [
3,
4] from the Ministry of health, social services and equality of Spain and the Catalan Health Service, respectively. Under these guidelines, VKA are the first-line treatment for AF cases requiring anticoagulation, while DOAC are used in specific situations of NVAF [
4].
The various DOACs are at least as effective as warfarin at preventing stroke in NVAF. The four DOACs (dabigatran, rivaroxaban, apixaban, and edoxaban) commercialized up to 2017 in Spain, and currently in many European countries, reduce the rates of stroke, systemic embolism, major bleeding, intracranial hemorrhage (ICH), cardiovascular mortality and total mortality, but are associated with a higher risk of intestinal bleeding [
5,
6,
7,
8]. Despite the dosage and interaction advantages of DOACs over VKAs, physicians individually evaluate the choice of anticoagulant [
3,
4]. Since VKAs remain the first-line treatment for NVAF in Spain, prescription of DOACs in Spain is amongst the lowest in Europe [
9], although DOAC prescription is currently increasing. However, there is a trend towards inadequate OA prescription in NVAF patients that was not yet sufficiently described with population data [
10].
This study analyzes the adequacy of the anticoagulant therapy prescription (VKAs and DOACs) in NVAF under the current recommendation criteria in primary care (PC) Catalan population, using real-world health care data.
4. Study Variables
Main variable. Adequacy of anticoagulant treatment (VKAs and DOACs) under IPT criteria (
Table 1).
Adequacy of VKA prescription. Patients receiving a VKA who met one of the following conditions [
4]: TTR
R ≥ 65% (according to Rosendaal’s formula [
15]), TTR
R < 65% and glomerular filtration (
eGFR estimated using CKD-EPI) < 15/min/1.73 m
2, history of adverse drug reaction (ADR) to DOACs (including allergy), a missing value of
eGFR or TTR
R. Inadequate prescription of VKAs was concluded for patients receiving a VKA who met one of the following conditions: history of ADR to VKAs or intracranial hemorrhage (ICH) with
eGFR > 15/min/1.73 m
2.
Adequacy of DOAC prescription. Patients who received one DOAC and met one of the following conditions [
4]: pre-DOAC TTR
R < 65% if the first OA was a VKA, or ADR to VKA, thromboembolic event (TEE) after starting VKA with TTR ≥ 65% (post-VKA TTE), ICH or stroke with a high risk of bleeding (SHRB). Inadequate prescription of DOACs was concluded for patients receiving DOACs who met one of the following conditions: ADR to DOAC,
eGFR < 15/min/1.73 m
2, or a missing
eGFR value, or when the DOAC was prescribed as first-line anticoagulant with no history of post-VKA TTE, SHRB or ICH.
Secondary variables. Sociodemographic variables, type of anticoagulant treatment, place of OA prescription, history of cardiovascular disease (CVD), ICH, morbidity, gastrointestinal hemorrhage (GH), history of high risk of bleeding (HRB) and other hemorrhages, estimated scores [
15,
16,
17,
18] based on participants’ real world data (
Table 2) and calculated constructed variables (see
Table 3). Diseases were classified as specified in the ICD10 code list [
14].
7. Discussion
This population-based study demonstrates the adequacy of anticoagulant treatment according to IPT [
4] criteria in PC patients with NVAF in 2018 in Catalonia. To our knowledge, this is the first real-word data study with a large cohort of Catalan population that evaluates prescription adequacy of anticoagulant therapy for patients with NVAF in relation to IPT [
4] criteria (also incorporated into the PHT [
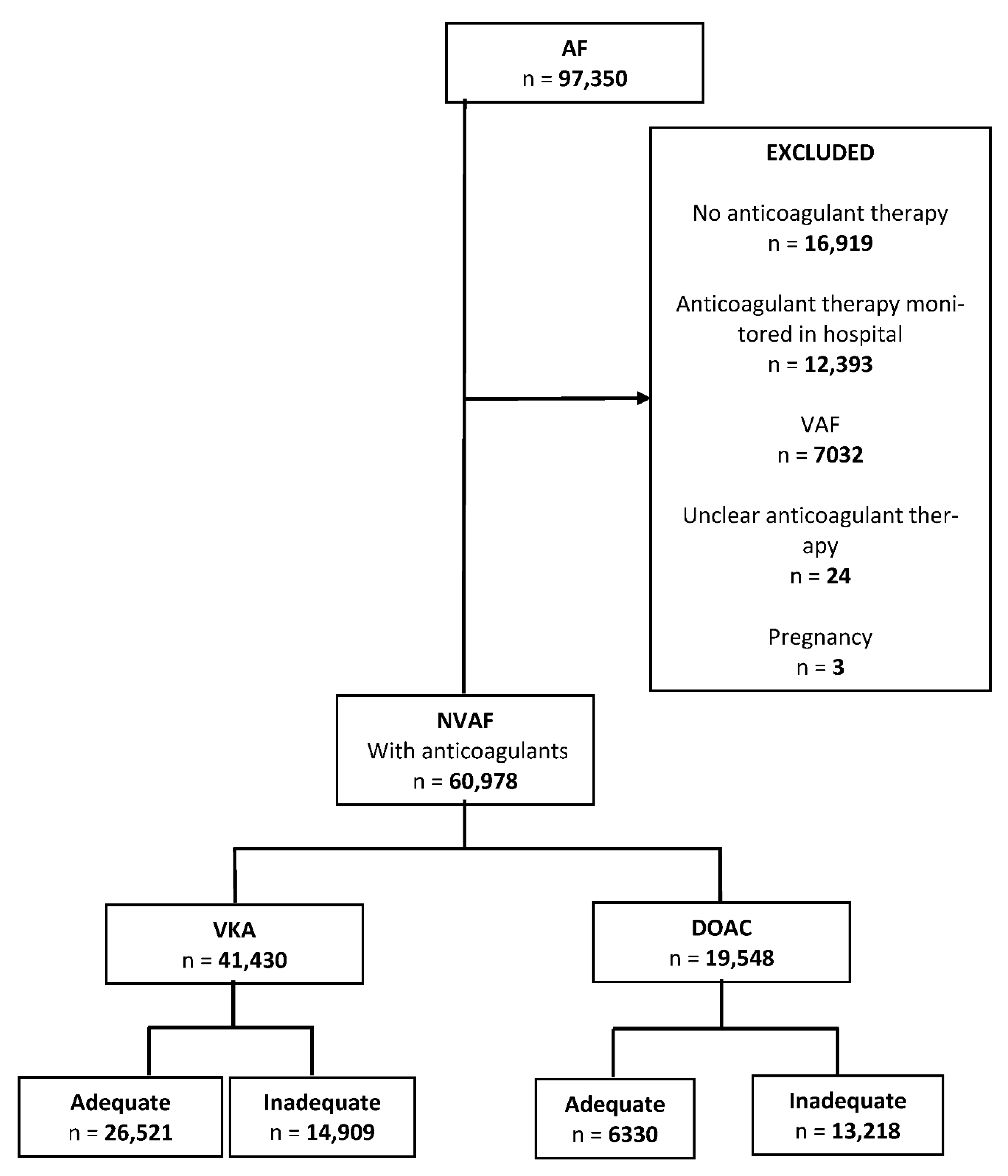
3]). Inadequate treatment was more common for DOACs (67.6%) than for VKAs (36%). Most of the inadequacy of DOAC prescription arose because it was prescribed as first-line anticoagulant when there was no history of TEEs or ICH. Another substantial part of the inadequacy stems from missing
eGFR values. Common causes of inadequate VKA prescription were poor TTR control and some cases of ICH.
The European Society of Cardiology [
2] and the American Heart Association [
1] were prompted to recommend the use of DOACs as first-line treatment instead of VKAs, because the results of pivotal clinical trials with DOACs [
5,
6,
7,
8,
19] showed a reduction in the incidence of stroke by at least the same degree as produced by warfarin, and presented a lower rate of ICH.
More recently, some real-world effectiveness studies have highlighted the limitations of the pivotal DOAC clinical trials, showing that DOACs and warfarin have similar effectiveness and safety with respect to TTE and severe non-intracranial hemorrhages [
20,
21]. Some studies also showed similar bleeding ratios for DOACs and VKAs [
22]. Conversely, other studies with real-world data that compared warfarin and DOACs underlined the effectiveness of DOACs for preventing TTE and reducing the risk of intracranial hemorrhage [
23,
24]. To resolve these conflicting results, health institutions require cost-effectiveness studies based on real-world data that analyze DOACs and VKAs in their specific settings. Recent studies have shown that DOACs are more cost-effective for patients who are poorly controlled with VKAs and for patients at high risk of thromboembolism and bleeding [
25,
26], supporting the IPT’s recommendations concerning DOAC use in specific situations.
In our study, control was poor (TTR < 65%) in 38.8% patients who received VKAs, similar to the levels in other regions of Spain (39.4%) [
27]. TTR was calculated based on the INR and the timings registered in the EHRs. Poor control of anticoagulation is associated with increased risks of stroke, bleeding and all-cause mortality [
28,
29]. Therefore, good control of the INR is essential for the patient, but often not achieved in Catalonia [
27], Spain or other countries [
30]. Typically, patients treated with VKAs are infracoagulated and not so much overcoagulated, thus increasing the risk of TTE and not so much the bleeding risk. Management of VKAs outside of clinical trials is associated with poor control, particularly at the start of VKA therapy. Good access to TTR values in PC would improve the control of patients treated with VKAs and decision-making regarding adequate switching to DOACs [
31], although most PCCs in Spain do not currently have access to such information. On the other hand, patients who receive VKAs and have had HIC should be considered for switching to DOAC as this has been shown to be superior in preventing ICH.
Measurement of GFR is essential for choosing anticoagulant therapy. The absence of this information leads to inadequate prescribing of DOAC. In clinical practice, various equations estimate the GFR [
32], one of the most commonly used for DOACs being the CKD-EPI [
18]. This was developed to improve the estimate, and is the one we use in our own setting. Not all PCCs include this calculated formula in their EHRs, which hinders the determination of the correct DOAC dose and the transition between VKAs and DOACs. Importantly, while VKAs can be used regardless of the GFR value, it can determine the adequacy in the case of DOACs [
4]. For instance, they are contraindicated in some cases. Dabigatran cannot be used with
eGFR <30 mL/min, and rivaroxaban, apixaban and edoxaban when
eGFR is <15 [
4]. In this study it was not differentiated the DOAC type and therefore eGFR <15 was considered to be the contraindication criterion of most DOAC. PCCs can access hospital creatinine results, and the number of laboratories providing GFR calculations to adjust anticoagulants is increasing. In this study, we used creatinine to estimate GFR. Records of a substantial proportion of patients receiving DOACs lack a measurement of creatinine from the previous year. It was not possible to estimate their
eGFR, which is essential for deciding the prescription and for adjusting the DOAC treatment dose. Probably, the lack of experience on DOACs management, in our setting, explains the absence of
eGFR in patients receiving this treatment. This study wants to provide evidence for this problem. While VKA treatments can be adjusted without recourse to renal function information, this is not possible for DOACs. The increase and decrease of DOAC plasma levels, which are closely related to renal function, are associated with hemorrhagic and ischemic events, respectively [
33]. Thus,
eGFR is essential to initiate dosing and to monitor the appropriate dose of DOAC, avoiding problems with DOACs underdoses and overdoses. DOAC dose adjustment is based primarily on
eGFR, and other factors such as age, weight and interactions with other drugs.
A report from our setting concerning the use of anticoagulants in NVAF, based on 2014–2017 data, showed the same usage of VKAs (69%) and DOACs (31%) as in our current study (VKAs, 68%; DOACs, 32%) [
34]. The same study also showed that 29.5% of patients treated with DOACs lacked clinical data with which to evaluate the dosage correctly [
34]. Measures are currently being evaluated and used to increase the availability of GFR determinations in PCCs of the ICS for patients treated with DOACs. To ensure that dosage determination takes kidney function into account, each physician can check their patients who are treated with a DOAC, with no measurement of
eGFR recorded during the previous 12 months.
A history of ICH should be considered when prescribing DOACs [
4], and treatment should be personalized. Clinical trials have shown the effectiveness of DOACs compared with warfarin at reducing stroke and mortality. DOACs involve a similar risk of major bleeding as with warfarin, but a lower risk of ICH and a higher risk of intestinal bleeding [
35].
Results of clinical trials are often difficult to translate into clinical practice, since patients often have more comorbidities, take more medication and cannot be followed up so closely. With regard to ICH, effectiveness studies with real-world data have confirmed that DOACs have fewer associated risks than VKAs [
23], so the IPT advises DOAC treatment in such cases [
4]. Most patients with a history of ICH received DOACs, probably because they were started on them after this event.
Studies also reveal the risk of gastrointestinal hemorrhage with DOACs [
5,
19]. A history of gastrointestinal hemorrhage is more common in patients treated with DOACs than with VKAs. Even though gastrointestinal hemorrhage is not a criterion in the IPT, clinicians need to consider this risk and advise their patients accordingly.
This study provides a real-world snapshot of anticoagulation in patients with NVAF. We consider that these recently acquired data on adequacy with respect to the criteria in force in Catalonia and Spain could be generalized to other geographical areas. Our results highlight the urgency of facilitating access to TTR by all specialists who manage anticoagulants, and the need for renal function measurements when DOACs are prescribed. It also shows that DOACs are frequently prescribed to young patients who have not previously experienced either the TEE or ICH that would justify this choice.
The study has some limitations. First, the cross-sectional design, used to investigate current patterns, does not allow causal inferences to be made. Nevertheless, it serves to generate hypotheses that could be examined in further studies. Second, there was a high frequency of missing scores, which had to be calculated from available patient data. Type of reporting and underreporting might constitute a limitation in this real-word data based study. The IPT does not take into account treatment adherence or lack of access to INR monitoring. However, access to INR is very high in PC patients of the ICS, considering that patients who are unable to attend the PCC are monitored at home. Guidelines agreed by experts and based on scientific evidence are key instruments for making individual decisions, although other factors, such as compliance and adherence to drugs, must frequently be considered. Both, compliance with VKA and adherence to DOAC are key factors in oral anticoagulant treatment in NVAF and should be consider in further studies.
The Spanish IPT criteria are more restrictive with respect to the use of DOACs than the European guidelines, although both are supported by scientific evidence. Regarding the main factors associated with inadequate OA prescription, our study highlights the need for improved strategies that can be generalized to other locations. The OA prescription criteria of different countries’ guidelines can differ in aspects related to first-line treatment or specific situations when the use of DOACs or VKAs is recommended. However, in clinical practice, the adherence to official criteria guidelines improves patient safety.

 ,
, 


{kind=link}