
Trypsin-Like Activity in Oral Cavity Is Associated with Risk of Fever Onset in Older Residents of Nursing Homes: An 8-Month Longitudinal Prospective Cohort Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
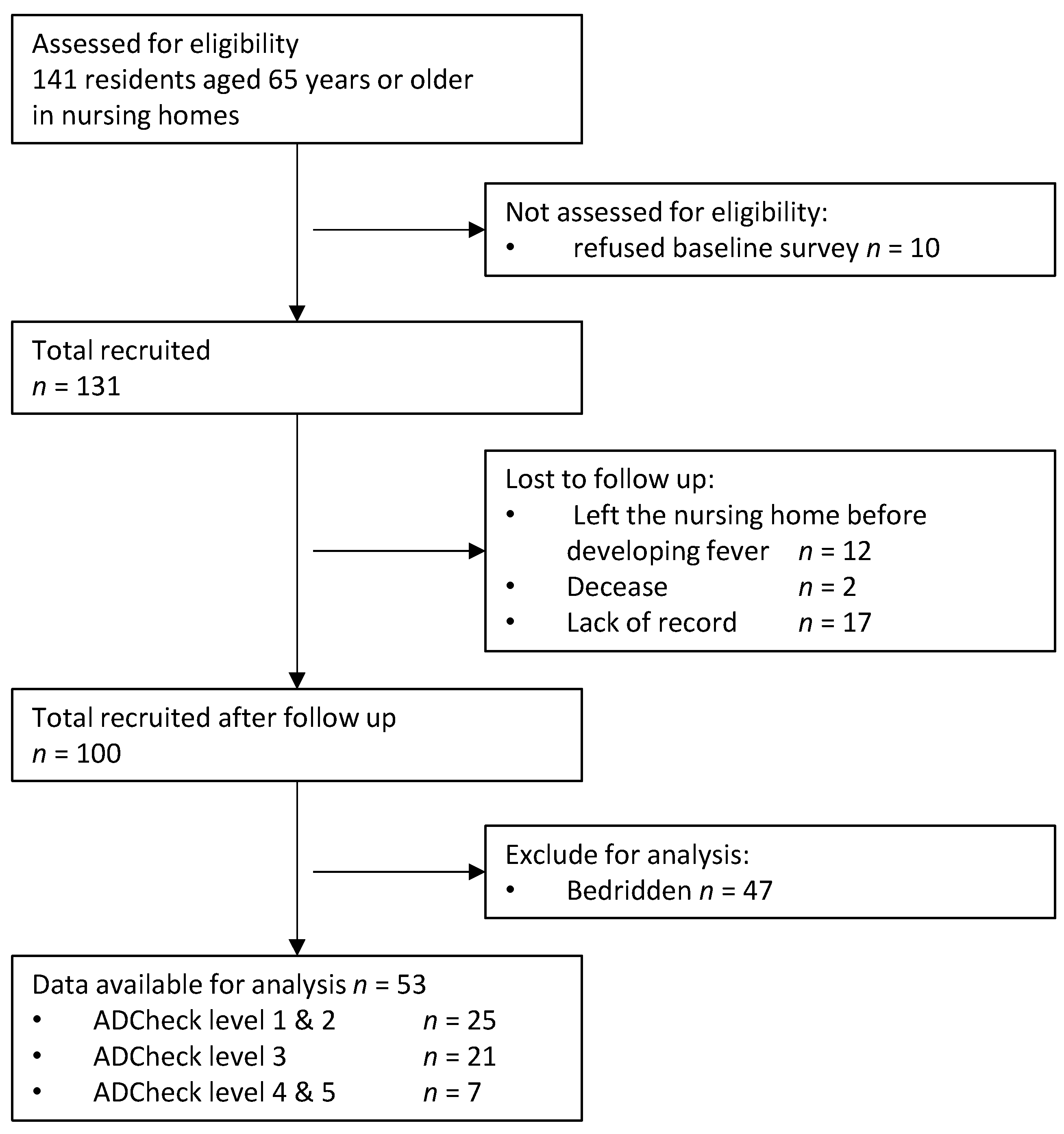
2.1. Study Setting and Population
2.2. Data Collection
2.3. Swallowing Function
2.4. Tooth and Periodontal Examination
2.5. Maximum Tongue Pressure
2.6. Lip-Closure Strength
2.7. ADL, Cognitive Activity, and Comorbidity Conditions
2.8. Trypsin-Like Activity and Bacterial Count
2.9. Hand Grip and 5 m Gait
2.10. Outcome
2.11. Sample Size
2.12. Bias
2.13. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Norman, D.C. Fever in the elderly. Clin. Infect. Dis. 2000, 31, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.D.; Pals, J.K.; Levesque, P.G.; Beal, L.F.; Cunningham, T.J.; Minaker, K.L. Dehydration and death during febrile episodes in the nursing home. J. Am. Geriatr. Soc. 1994, 42, 968–971. [Google Scholar] [CrossRef]
- Pals, J.K.; Weinberg, A.D.; Beal, L.F.; Levesque, P.G.; Cunningham, T.J.; Minaker, K.L. Clinical triggers for detection of fever and dehydration. Implications for long-term care nursing. J. Gerontol. Nurs. 1995, 21, 13–19. [Google Scholar] [CrossRef]
- Ikematsu, H.; Yamaga, S.; Nabeshima, A.; Yamaji, K.; Kakuda, K.; Ueno, K.; Hayashi, J.; Hara, H.; Shirai, T.; Kashiwagi, S. Incidence and duration of febrile episodes in a hospitalized geriatric cohort. Kansenshogaku Zasshi 1996, 70, 1079–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, D.C.; Grahn, D.; Yoshikawa, T.T. Fever and aging. J. Am. Geriatr. Soc. 1985, 33, 859–863. [Google Scholar] [CrossRef]
- Finkelstein, M.S.; Petkun, W.M.; Freedman, M.L.; Antopol, S.C. Pneumococcal bacteremia in adults: Age-dependent differences in presentation and in outcome. J. Am. Geriatr. Soc. 1983, 31, 19–27. [Google Scholar] [CrossRef]
- Castle, S.C.; Norman, D.C.; Yeh, M.; Miller, D.; Yoshikawa, T.T. Fever response in elderly nursing home residents: Are the older truly colder? J. Am. Geriatr. Soc. 1991, 39, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Labour and Welfare of Japan. Survey of Dental Diseases; Ministry of Health Labour and Welfare of Japan: Tokyo, Japan, 2016. [Google Scholar]
- Kebede, T.G.; Holtfreter, B.; Kocher, T.; Meisel, P.; Dietrich, T.; Biffar, R.; Dörr, M.; Völzke, H.; Pink, C. Association of Periodontal Destruction and Diabetes with Mortality. J. Dent. Res. 2017, 96, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Michaud, D.S.; Fu, Z.; Shi, J.; Chung, M. Periodontal Disease, Tooth Loss, and Cancer Risk. Epidemiol. Rev. 2017, 39, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Van Dyke, T.E. Periodontitis and atherosclerotic cardiovascular disease: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Clin. Periodontol. 2013, 40 (Suppl. 14), S24–S29. [Google Scholar] [CrossRef]
- Awano, S.; Ansai, T.; Takata, Y.; Soh, I.; Akifusa, S.; Hamasaki, T.; Yoshida, A.; Sonoki, K.; Fujisawa, K.; Takehara, T. Oral health and mortality risk from pneumonia in the elderly. J. Dent. Res. 2008, 87, 334–339. [Google Scholar] [CrossRef]
- Moghadam, S.A.; Shirzaiy, M.; Risbaf, S. The Associations between Periodontitis and Respiratory Disease. J. Nepal Health Res. Counc. 2017, 15, 1–6. [Google Scholar] [CrossRef]
- Gomes-Filho, I.S.; Cruz, S.S.D.; Trindade, S.C.; Passos-Soares, J.S.; Carvalho-Filho, P.C.; Figueiredo, A.; Lyrio, A.O.; Hintz, A.M.; Pereira, M.G.; Scannapieco, F. Periodontitis and respiratory diseases: A systematic review with meta-analysis. Oral Dis. 2020, 26, 439–446. [Google Scholar] [CrossRef]
- Iwasaki, M.; Usui, M.; Ariyoshi, W.; Nakashima, K.; Nagai-Yoshioka, Y.; Inoue, M.; Nishihara, T. A Preliminary Study on the Ability of the Trypsin-Like Peptidase Activity Assay Kit to Detect Periodontitis. Dent. J. 2020, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.C.; Ebersole, J.L. Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: The “red complex”, a prototype polybacterial pathogenic consortium in periodontitis. Periodontology 2000 2005, 38, 72–122. [Google Scholar] [CrossRef] [PubMed]
- Castle, S.C.; Yeh, M.; Toledo, S.; Yoshikawa, T.T.; Norman, D.C. Lowering the temperature criterion improves detection of infections in nursing home residents. Aging Immun. Infect. Dis. 1993, 4, 67–76. [Google Scholar]
- Sakai, Y.; Ohira, M.; Yokokawa, Y. Cough Strength Is an Indicator of Aspiration Risk When Restarting Food Intake in Elderly Subjects with Community-Acquired Pneumonia. Respir. Care 2020, 65, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Yanagisawa, T.; Shinada, K.; Ohara, S.; Kawaguchi, Y. Masticatory ability and functional tooth units in Japanese adults. J. Oral Rehabil. 2008, 35, 337–344. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, E.S.; Kim, G.M.; Jung, H.I.; Lee, J.W.; Kwon, H.K.; Kim, B.I. Unilateral Mastication Evaluated Using Asymmetric Functional Tooth Units as a Risk Indicator for Hearing Loss. J. Epidemiol. 2019, 29, 302–307. [Google Scholar] [CrossRef]
- Izumi, M.; Sonoki, K.; Ohta, Y.; Fukuhara, M.; Nagata, M.; Akifusa, S. Impact of Tongue Pressure and Peak Expiratory Flow Rate on Nutritional Status of Older Residents of Nursing Homes in Japan: A Cross-Sectional Study. J. Nutr. Health Aging 2020, 24, 512–517. [Google Scholar] [CrossRef]
- Izumi, M.; Akifusa, S.; Takahashi, Y.; Funahara, M.; Tsujisawa, T.; Nakamichi, A. The Relation of Oral Function(s) and the Levels of Oral Bacteria in Community-Dwelling Older Adults Pilot Study. J. Oral Health Dent. 2018, 1, 9–14. [Google Scholar]
- Tsubone, A.; Murakami, T.; Kurumadani, H.; Shimizu, J.; Fujiwara, N. Relationship between criteria for evaluating the degree of independence of disabled elderly persons in performing activities of daily living. J. Jpn. Occup. Ass. 2002, 21, 455–462. [Google Scholar]
- Handa, S.; Imai, Y. Relationship between nursing care levels and ADL, BPSD as well as independence degree in daily living for elderly with dementia. Jpn. J. Geriatr. Psych. 2016, 27, 667–674. [Google Scholar]
- Christensen, S.; Johansen, M.B.; Christiansen, C.F.; Jensen, R.; Lemeshow, S. Comparison of Charlson comorbidity index with SAPS and APACHE scores for prediction of mortality following intensive care. Clin. Epidemiol. 2011, 3, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Hirota, K.; Inagaki, S.; Hamada, R.Y.O.; Ishihara, K.; Miyake, Y. Evaluation of a Rapid Oral Bacteria Quantification System Using Dielectrophoresis and the Impedance Measurement. Biocontrol. Sci. 2014, 19, 45–49. [Google Scholar] [CrossRef] [Green Version]
- Iwawaki, Y.; Muraoka, Y.; Higashiyama, H.; Kishimoto, T.; Liu, L.; Goto, T.; Ichikawa, T. Comparison between Two Assessment Tests for Oral Hygiene: Adenosine Triphosphate + Adenosine Monophosphate Swab Test and Bacteria Number Counting by Dielectrophoretic Impedance Measurement. Dent. J. 2019, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, K.; Akagi, J. Sarcopenia is an independent risk factor of dysphagia in hospitalized older people. Geriatr. Gerontol. Int. 2016, 16, 515–521. [Google Scholar] [CrossRef]
- Afilalo, J.; Kim, S.; O’Brien, S.; Brennan, J.M.; Edwards, F.H.; Mack, M.J.; McClurken, J.B.; Cleveland, J.C., Jr.; Smith, P.K.; Shahian, D.M.; et al. Gait Speed and Operative Mortality in Older Adults Following Cardiac Surgery. JAMA Cardiol. 2016, 1, 314–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohse, H.; Ito, T.; Saito, K.; Kohno, Y.; Kobayashi, M.; Takeuchi, R.; Shimizu, Y.; Matsuzaki, H.; Wadano, Y. Examination of the exothermic cases in the recovery rehabilitation unit of our hospital. M. J. Ibaraki P. H. 2014, 31, 23–27. [Google Scholar]
- Tada, A.; Hanada, N. Opportunistic respiratory pathogens in the oral cavity of the elderly. FEMS Immunol. Med. Microbiol. 2010, 60, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komiyama, K.; Gibbons, R.J. Interbacterial adherence between Actinomyces viscosus and strains of Streptococcus pyogenes, Streptococcus agalactiae, and Pseudomonas aeruginosa. Infect. Immun. 1984, 44, 86–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komiyama, K.; Habbick, B.F.; Gibbons, R.J. Interbacterial adhesion between Pseudomonas aeruginosa and indigenous oral bacteria isolated from patients with cystic fibrosis. Can. J. Microbiol. 1987, 33, 27–32. [Google Scholar] [CrossRef]
- Mackowiak, P.A.; Wasserman, S.S.; Levine, M.M. A Critical Appraisal of 98.6°F, the Upper Limit of the Normal Body Temperature, and Other Legacies of Carl Reinhold August Wunderlich. JAMA 1992, 268, 1578–1580. [Google Scholar] [CrossRef]
- Norman, D.C.; Yoshikawa, T.T. Fever in the elderly. Infect. Dis. Clin. N. Am. 1996, 10, 93–99. [Google Scholar] [CrossRef]
- Chapman, S.W.; Dismukes, W.E.; Proia, L.A.; Bradsher, R.W.; Pappas, P.G.; Threlkeld, M.G.; Kauffman, C.A. Clinical Practice Guidelines for the Management of Blastomycosis: 2008 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 1801–1812. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J.; Bretz, W.A.; Kerschensteiner, D.; Stoll, J.; Socransky, S.S.; Hujoel, P.; Lopatin, D.E. Development of a diagnostic test for anaerobic periodontal infections based on plaque hydrolysis of benzoyl-DL-arginine-naphthylamide. J. Clin. Microbiol. 1990, 28, 1551–1559. [Google Scholar] [CrossRef] [Green Version]
- Morita, M.; Wang, H.-L. Relationship of Sulcular Sulfide Level to Severity of Periodontal Disease and BANA Test. J. Periodontol. 2001, 72, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Izuno, H.; Hori, K.; Sawada, M.; Fukuda, M.; Hatayama, C.; Ito, K.; Nomura, Y.; Inoue, M. Physical fitness and oral function in community-dwelling older people: A pilot study. Gerodontology 2016, 33, 470–479. [Google Scholar] [CrossRef]
- Tamura, F.; Kikutani, T.; Nishiwaki, K.; Enomoto, R.; Inaba, S.; Yoneyama, T. Relation between the level of care needed and frailty for labial functions. Jpn. J. Geriatr. 2006, 43, 398–402. [Google Scholar] [CrossRef]
- Tamura, F.; Fukui, T.; Kikutani, T.; Machida, R.; Yoshida, M.; Yoneyama, T.; Hamura, A. Lip-closing function of elderly people during ingestion: Comparison with young adults. Int. J. Orofac. Myol. 2009, 35, 33–43. [Google Scholar]
- Chen, Y.; Zhou, R.; Yi, Z.; Li, Y.; Fu, Y.; Zhang, Y.; Li, P.; Li, X.; Pan, Y. Porphyromonas gingivalis induced inflammatory responses and promoted apoptosis in lung epithelial cells infected with H1N1 via the Bcl-2/Bax/Caspase-3 signaling pathway. Mol. Med. Rep. 2018, 18, 97–104. [Google Scholar] [PubMed] [Green Version]
- Yasuoka, S.; Miki, M.; Tsutsumi, R.; Yoshioka, M.; Bando, T.; Michishige, F. Human airway trypsin-like protease (HAT) is released into saliva. J. Med. Invest. 2018, 65, 258–267. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Rank | Status | Classification |
|---|---|---|
| Rank J | Almost independent living indoors and outdoors with any disabilities | Not bedridden or independent |
| Rank A | Almost independent living indoors, but not outdoors | |
| Rank B | Dependent living with requirement of care, and almost bedridden in the daytime | Dependent |
| Rank C | Bedridden at all times with care required for meals, evacuation, and changing clothes |
| Variables | ADCHECK® | p-Value § | ||
|---|---|---|---|---|
| Score 1 and 2 (n = 25) | Score 3 (n = 21) | Score 4 and 5 (n = 7) | ||
| Age (m) | 86 (62–94) | 89 (74–102) | 87 (76–93) | 0.140 |
| Gender (n, %) men | 10 (40.0) | 4 (19.0) | 2 (28.6) | 0.303 |
| women | 15 (60.0) | 17 (81.0) | 5 (71.4) | |
| Teeth number (m) | 3 (0–28) | 10 (0–26) | 16 (5–20) | 0.297 |
| Teeth with PD > 4 (m) | 0 (0–10) | 1 (0–18) | 6 (0–16) | 0.077 |
| Teeth with PD > 6 (m) | 0 (0–3) | 0 (0–3) | 0 (0–12) | 0.338 |
| Teeth with BOP (m) | 0 (0–6) * | 0 (0–9) * | 5 (0–10) | 0.007 |
| Functional tooth unit (m) | 12 (0–12) | 12 (0–12) | 12 (0–12) | 0.919 |
| Bacterial count (m ×106) | 3.9 (0.1–20.3) | 5.3 (0.7–40.1) | 7 (0.1–14.6) | 0.087 |
| Lip closing force (m, N) | 9.4 (3.6–14) * | 7.6 (3–12.5) | 5.5 (1–11.4) | 0.034 |
| Tongue pressure (m, kPa) | 23 (10–38.7) | 23.9 (4.5–34.9) | 16 (7.3–21.3) | 0.066 |
| BMI (m, kg/m2) | 20.7 (16–26.4) | 22.8 (18.9–28.4) | 22.2 (19.5–23.4) | 0.229 |
| Hand grip (m, kg) | 15 (6.9–30.7) | 10.6 (0–21.5) | 11.8 (6.7–20) | 0.062 |
| 5 m gait (m, s) | 6.9 (3.7–24.8) | 7.2 (5.5–8) | 4.4 (4.2–9.1) | 0.649 |
| Cognitive function (n, %) | 7 (28.0) | 7 (33.3) | 1 (14.3) | 0.625 |
| Charlson commodity index (m) | 1 (0–4) | 0 (0–2) | 1 (0–1) | 0.611 |
| Fever days (m) | 0 (0–6) | 0.5 (0–11) | 1 (0–4) | 0.095 |
| Variables | Crude Model | Adjusted Model § | ||||
|---|---|---|---|---|---|---|
| B ± SE | HR (95% CI) | p-Value | B ± SE | HR (95% CI) | p-Value | |
| ADCHECK® scores | ||||||
| Score 1 and 2 | 1 (reference) | 1 (reference) | ||||
| Score 3 | 1.1 ± 0.6 | 3.0 (0.9–10.0) | 1.1 ± 0.6 | 1.5 ± 0.7 | 4.4 (1.2–16.2) | 0.025 |
| Score 4 and 5 | 1.4 ± 0.7 | 4.2 (1.1–15.6) | 0.034 | 1.8 ± 0.7 | 5.9 (1.4–23.9) | 0.013 |
| Age | −0.0 ± 0.0 | 1.0 (0.9–1.0) | 0.500 | −0.1 ± 0.0 | 0.9 (0.9–1.0) | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izumi, M.; Isobe, A.; Akifusa, S. Trypsin-Like Activity in Oral Cavity Is Associated with Risk of Fever Onset in Older Residents of Nursing Homes: An 8-Month Longitudinal Prospective Cohort Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 2255. https://doi.org/10.3390/ijerph18052255
Izumi M, Isobe A, Akifusa S. Trypsin-Like Activity in Oral Cavity Is Associated with Risk of Fever Onset in Older Residents of Nursing Homes: An 8-Month Longitudinal Prospective Cohort Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(5):2255. https://doi.org/10.3390/ijerph18052255
Chicago/Turabian StyleIzumi, Maya, Ayaka Isobe, and Sumio Akifusa. 2021. "Trypsin-Like Activity in Oral Cavity Is Associated with Risk of Fever Onset in Older Residents of Nursing Homes: An 8-Month Longitudinal Prospective Cohort Pilot Study" International Journal of Environmental Research and Public Health 18, no. 5: 2255. https://doi.org/10.3390/ijerph18052255