1. Introduction
The global increase in human population is associated with an increased demand for foods of animal origin [
1]. Consequently, ensuring the security, quality, and safety of food is a worldwide concern [
2]. It is a particularly significant problem in developing countries as animals and products there are often produced under sub-optimal hygienic conditions [
3,
4].
Most of the meatborne bacterial outbreaks are usually attributed to contamination along the supply chain due to poor handling practices [
5]. Food-producing animals are the major sources of many foodborne pathogens and can lead to meat contamination, which may result in a widespread occurrence of foodborne diarrheal illnesses in humans [
6,
7]. Cattle slaughterhouses are one of the critical units in the supply chain from which foodborne pathogens can disseminate along the processing and distribution continuum including retail shops subsequently reaching the consumers. As a result, good hygienic practices at slaughterhouses and during distribution to and storage at retail shops and during sales are key points in ensuring the quality and safety of meat to safeguard public health [
8,
9]. Inadequate facilities and improper handling of the animals at the slaughterhouses further aggravate the microbial contamination of beef which can result in the transmission of foodborne pathogens to humans [
10,
11].
Meat hygiene and safety is usually less controlled in many developing countries where meat for human consumption is approved based on visual inspection, if at all, without routine microbiological testing [
11]. Several studies investigated the occurrence of pathogens along the entire beef supply chain [
12,
13,
14,
15,
16], while others identified contamination at specific levels such as at slaughterhouses [
17,
18,
19,
20] and in retail shops [
19,
21,
22] in different countries including Ethiopia. Contamination and cross-contamination from raw meat is a major cause of foodborne diseases particularly in developing countries [
23,
24]. According to World Health Organization estimation, foodborne diseases resulted in 600 million cases and 420,000 deaths resulting in nearly 33 million disability-adjusted life years globally with the highest mortality burden in Africa in 2010 [
25]. Foods of animal origin such as beef are major contributors to the burden. The global burden of foodborne diseases due to all animal source foods and beef was estimated at 168 and 10 disability-adjusted life years per 100,000 population, respectively [
26]. However, information on the burden of foodborne diseases due to poor meat handling practices is limited. Improving hygienic handling practices by meat handlers during meat production, distribution, storage and sales at retail shops prevent or reduce microbial contamination [
8]. It is very evident that food safety problems require intervention measures along the entire beef supply chain. To identify specific targets for intervention in specified settings, a clear understanding of local drivers for microbial meat contamination along the meat production, processing, and distribution chain is needed.
In Ethiopia, there are over 300 local slaughterhouses that supply meat for local consumption with different capacities and facilities, however all with low basic hygienic standards [
27]. Although foodborne bacteria have been reported from cattle at slaughterhouses and beef in the retail shops as reviewed by Abayneh et al. [
13], little information is available concerning beef hygienic handling practices along the beef production and distribution continuum in Ethiopia. Therefore, the objective of this study was to assess beef hygienic handling practices at cattle slaughterhouses and retail shops to contribute to the identification of intervention targets.
4. Discussion
Proper meat handling practices play a significant role in ensuring meat quality and safety [
9]. Knowledge of meat hygienic handling practices during beef production, processing and distribution is essential to formulate preventive measures to mitigate the contribution of meat to foodborne diseases [
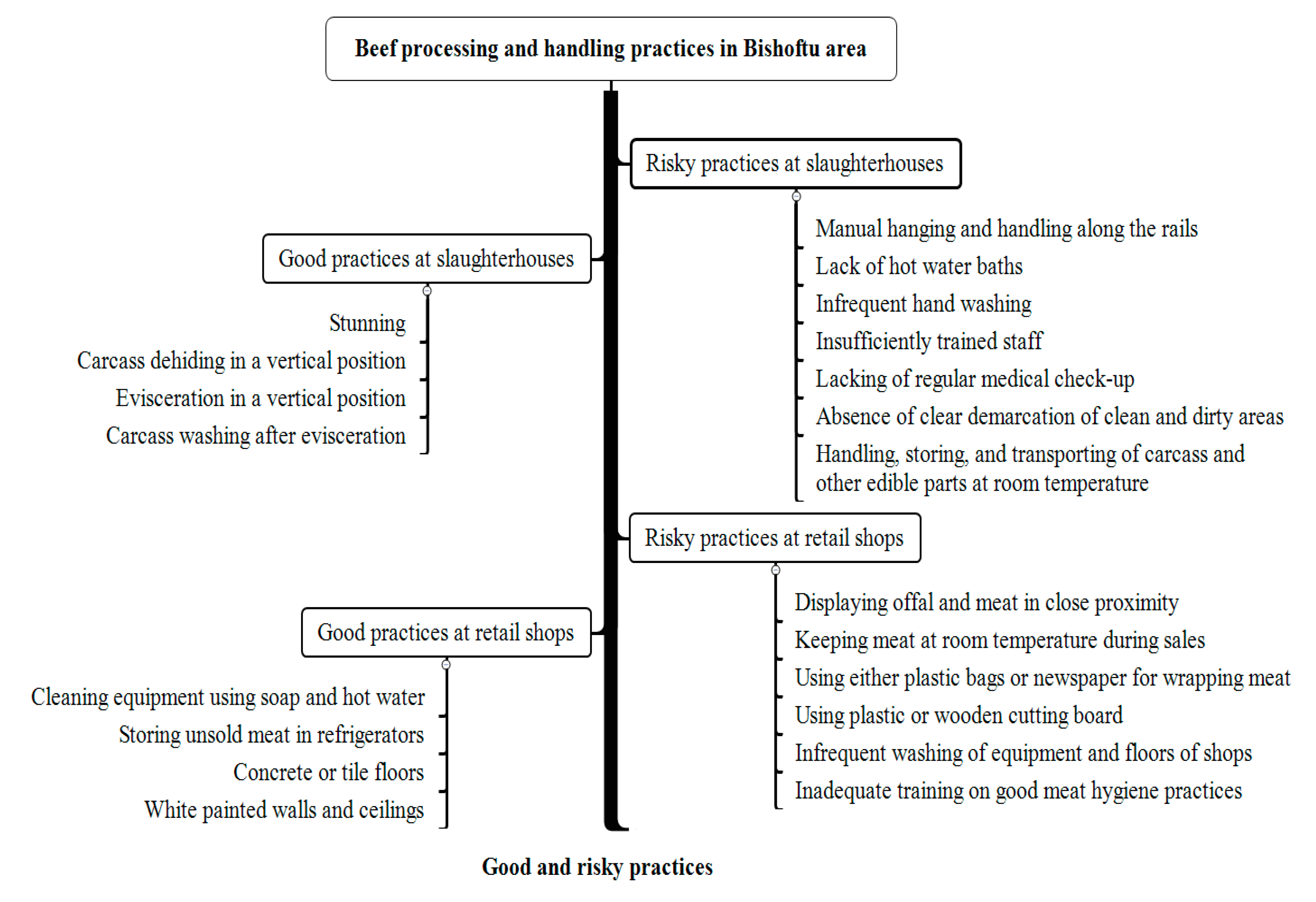
31]. We investigated the status of beef hygienic handling practices in cattle slaughterhouses and retail shops in Bishoftu town, Ethiopia. Our study revealed both good and unhygienic handling practices at the slaughterhouses and retail shops. The discussion below focuses on the main meat handling practices identified with their potential implication for public health. Moreover, the practices are discussed in view of the requirements of the Ethiopian proclamations: Meat inspection proclamation (No. 274/1970) [
32], Public health Proclamation (No. 200/2000) [
33] and Food, Medicine and Health Care Administration and Control Proclamation (No. 661/2009) which enables controlling the safety and quality of food [
34] and the Codex Alimentarius Commission (CAC) on general principles of food hygiene [
35] and code of hygienic practice for meat [
36] that have been formulated to ensure the production and marketing of sound, wholesome and quality meat and meat products for the consumer’s protection. Ethiopia is a member of the Codex Alimentarius Commission and the Codex standards are the basic reference materials for standard setting and serve as enforcing tools for food safety where there are no developed Ethiopian standards [
37,
38].
In the present study, lack of hot water baths for hand washing and dipping of knives, infrequent hand washing, insufficiently trained operational employees, lack of regular medical check-up and lack of cooling facilities were bad practices identified both at the slaughterhouses and retail shops. Hot water, which is essential for hand and knife washing to remove potential surface contaminants and to prevent further cross contamination of meat, was lacking at washing basins of both at slaughterhouses and retail shops [
39]. Even though Ethiopia is a member of CAC, the present finding indicated lack of adherence to the requirements of CAC that demands the presence of an adequate and easily accessible supply of hot and cold potable water at all times during handling meat for effective sanitizing of equipment and hand washing [
36].
According to 53.6% of the respondents at slaughterhouses hand washing was not a frequent practice during slaughter operations, and few (9.4%) employees at retail shops did not wash their hands before touching meat. This practice is not consistent with the requirements of the CAC which recommends that food handlers should wash their hands at every stage of food production to safeguard the consumer from foodborne diseases [
35].
About 40% of slaughterhouses and 85.8% of retails shops employees did not receive training on hygienic handlings of meat. Previous studies also reported that a considerable proportion of meat processing employees [
30,
40,
41] and meat retail shops employees [
30,
41] did not receive basic training on hygienic handling of meat. This is contrary to the basic requirements for personnel working in the food industry. Employees working in food establishments such as slaughterhouses and retail shops should be trained on food safety issues [
42]. According to Food, Medicine and Health Care Administration and Control Proclamation (No. 661/2009) of Ethiopia, a certificate of competence from the appropriate organ is required for any person working in food catering [
34]. The Food and Agriculture Organization (FAO) also recommends the provision of food safety training to food handlers as an important intervention to improve their knowledge and skills [
43].
All employees at the slaughterhouses and 98% of the respondents at retail shops confirmed having had a medical check-up. However, when asked about the frequency of the check-up, answers were variable and not in line with the actual requirement by the Ethiopian regulatory body. Having a periodic medical check-up would partly limit the transmission of pathogens from sick or potentially carrier employees [
44]. In addition, strict regulation in the uniformity of the frequency of the check-up as mentioned by the requirements of the Oromia Health Bureau—recommending the need for medical check-up of all employees in food establishments every three months—is essential.
Carcasses were stored at room temperature at the slaughterhouses and transported to beef retail shops using vehicles without cooling facilities. At all retail shops, meat was displayed openly with no cooling and no cover, being exposed to dust particles and domestic flies. The meat could remain as such for hours until sold. The mean annual temperature of the study area is estimated at 20.2 °C (range: 10.9–29.5 °C) [
45], which is the ideal temperature suitable for the growth of a wide range of spoilage and pathogenic organisms to potentially unsafe levels. Cold chain management in meat storage and supply is an exceedingly important requirement to ensure the quality and safety of meat and meat products [
46,
47].
None of the employees in slaughterhouses and retail shops wore hand gloves during handling of meat. The use of gloves may protect the meat against contamination [
48]. In countries where the frequent change of gloves is economically not feasible like in Ethiopia, frequent hand washing is an effective measure to prevent cross contamination of meat.
At the slaughterhouses, the use of aprons, white coats, boots and hair covering, as well as the presence of sinks for hand washing were good practices observed at both slaughterhouses. These practices are important to protect both the personnel and the meat from exposure to pathogens [
49].
Stunning of the animals, the hanging of carcasses over the rail system for dehiding and eviscerations, and carcass washing after eviscerations were good practices identified at the slaughterhouses. These practices are essential to ensure production of quality and safe meat and needs to be maintained at all times [
32,
33,
34,
35,
36]. However, we observed that bleeding was carried out on the ground, and the hanging and de-hiding of the carcass were done manually. These operations can lead to carcass contamination from the ground, workers’ hands and cross contamination from carcass to carcass contact [
43]. Automatic carcass hoisting, hide removal and sliding of carcasses reduces the risk of carcass contamination [
20]. Establishing slaughterhouses equipped with the necessary facilities and basic infrastructures would improve the hygienic production in slaughterhouses particularly in government-based municipal slaughterhouses in Ethiopia.
According to the respondent’s perception, feces during evisceration, hides, handler’s hands and knifes were the potential sources of carcass contamination at the slaughterhouses whereby feces as well hides were identified as the major sources by 36% of them. This was consistent with previous reports [
50,
51]. Previous studies reported the occurrence of foodborne pathogens such as
E. coli O157 and
Salmonella in cattle feces and on hides and the possibility of their transfer to carcass during slaughter operations [
52,
53,
54,
55,
56]. Further studies to identify all possible sources for carcass contamination and designing effective intervention measures are needed in these slaughterhouses. This would help to improve handling practices [
57].
At retail shops, the use of soap and water for hand and equipment washing, storing leftover meat in refrigerators, concrete/tile made floors, and white painted walls and ceilings were the identified good practices. These were in line with the basic requirements of Ethiopian proclamations and can contribute to hygienic handling of meat [
34,
36]. However, displaying offal and meat in close proximity (39.4%), use of either plastic bags or newspapers for wrapping meat (53.5%), use of plastic or wooden cutting boards, use of one coat for the entire day (85%) and infrequent washing of equipment and floors were sub-standard practices that can lead to carcass contamination [
34,
36].
The use of plastic bags or newspapers were contrary to the requirements of the Ethiopian Food, Medicine and Healthcare Administration and Control Authority Proclamation (No. 661/2009) that require packaging material to be made out of substances, which are safe and suitable for their intended use, and the product to be packed in container which will safeguard its hygienic, safety, quality and food grade. Furthermore, the proclamation states that “no packaging material shall be put into use unless it complies with the international and national safety and quality standards”, which was lacking in the beef retails shops in Bishoftu town [
34].
In most of the retail shops (>70%) equipment, floors and the display cabinet were cleaned once per day. Unclean retail shops ceilings and white walls with observable dirty spots were noticed in 79% of the shops. Frequent and scheduled cleaning of equipment and working environments at food establishments are the basic essential requirements to ensure the continuing effective control of food hazards likely to contaminate food [
35].
In general, the observed unhygienic practices at the slaughterhouses and retail shops can be linked with lack or inadequate knowledge of basic hygienic practices [
30,
58,
59,
60], lack of infrastructure or facilities [
61] and poor compliance to standards of good handling practices of food [
59]. Moreover, the insufficient implementation of the government control systems and ensuing timely corrective actions by the food regulatory bodies, which is common in most developing countries including Ethiopia, might contribute to sustaining such unhygienic practices leading to a higher risk for human infection necessitating urgent interventions [
4,
56].
The study has some limitations. The study used questionnaires as a data collection tool, which relies totally on the answers of the respondents that might not necessarily correspond to the actual situation. For example, 91% of the employees at the retail shops and 46% of employees at slaughterhouses responded that they washed their hands before touching the meat and between activities during work, which was contrary to our observations. All the respondents confirmed having had a medical check-up. However, when asked about the frequency of the check-up, answers were variable and not in line with the actual requirement by the regulatory body. Combining questionnaires with personal observations reduced the study limitations in part, while of course, the presence of the study team might have induced practice changes.


 ,
, 

{kind=link}