
Perceived Helpfulness of a Moderated Online Social Therapy Network for Young People Experiencing Social Anxiety

 , , ,
, , , 
Abstract
:1. Introduction
1.1. Social Anxiety Disorder and Young People
1.2. CBT-Based Digital Interventions
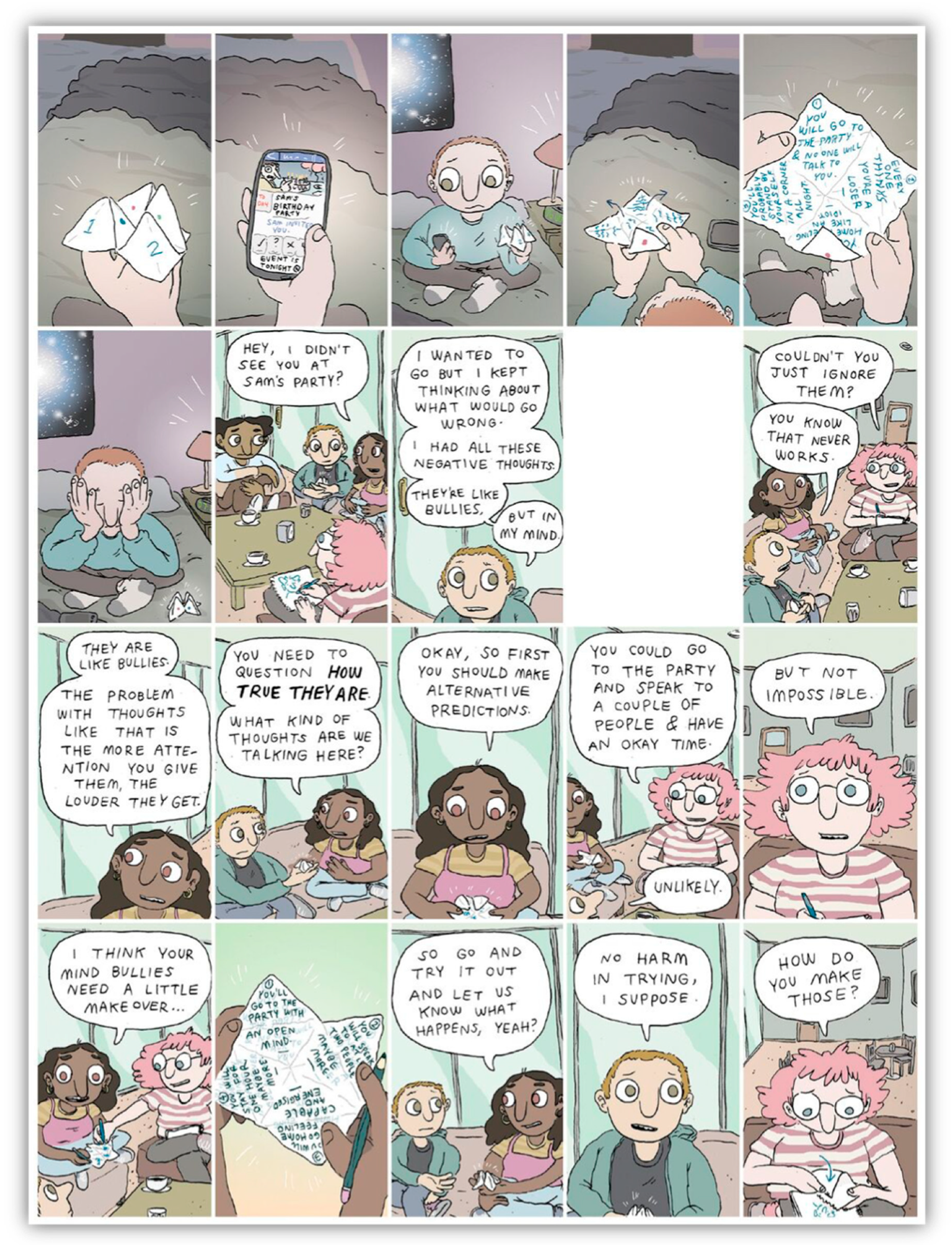
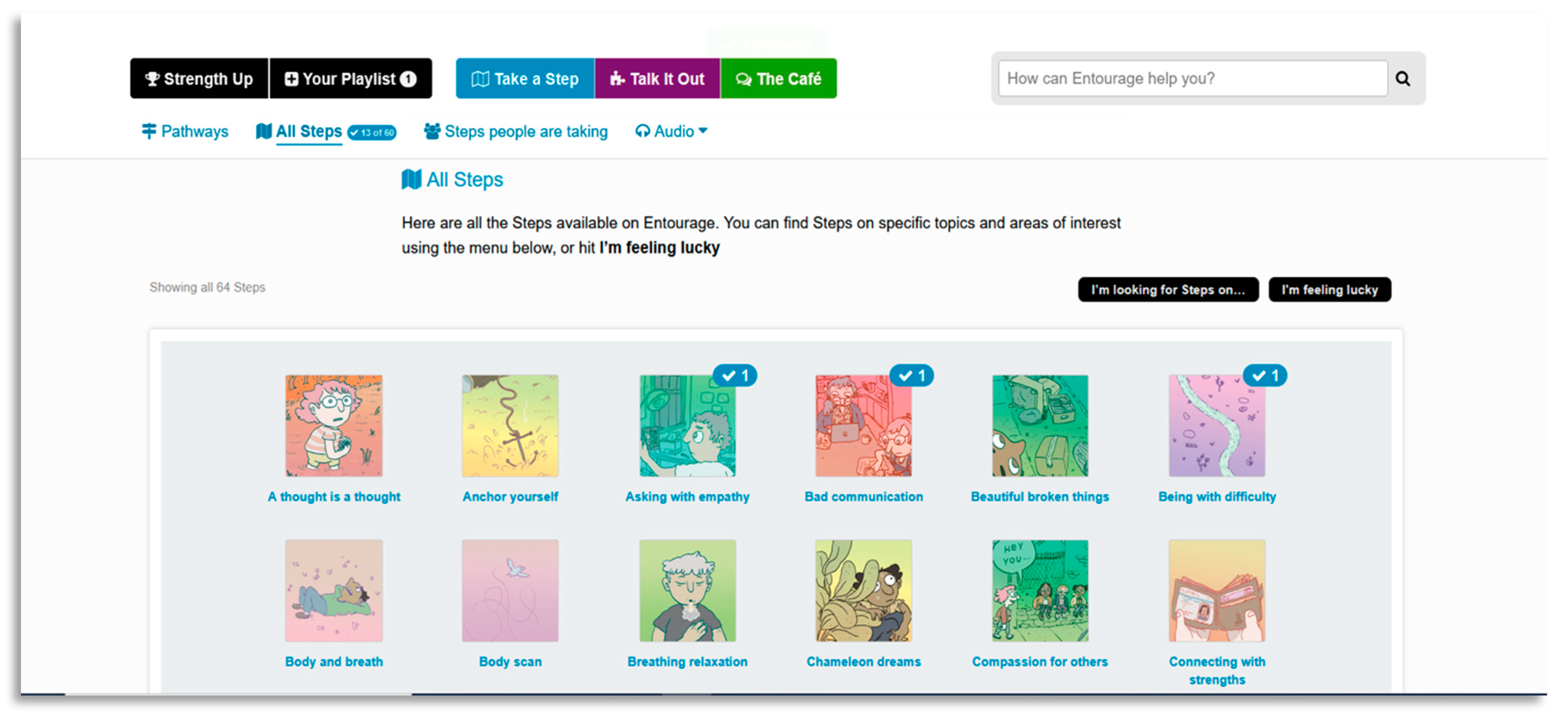
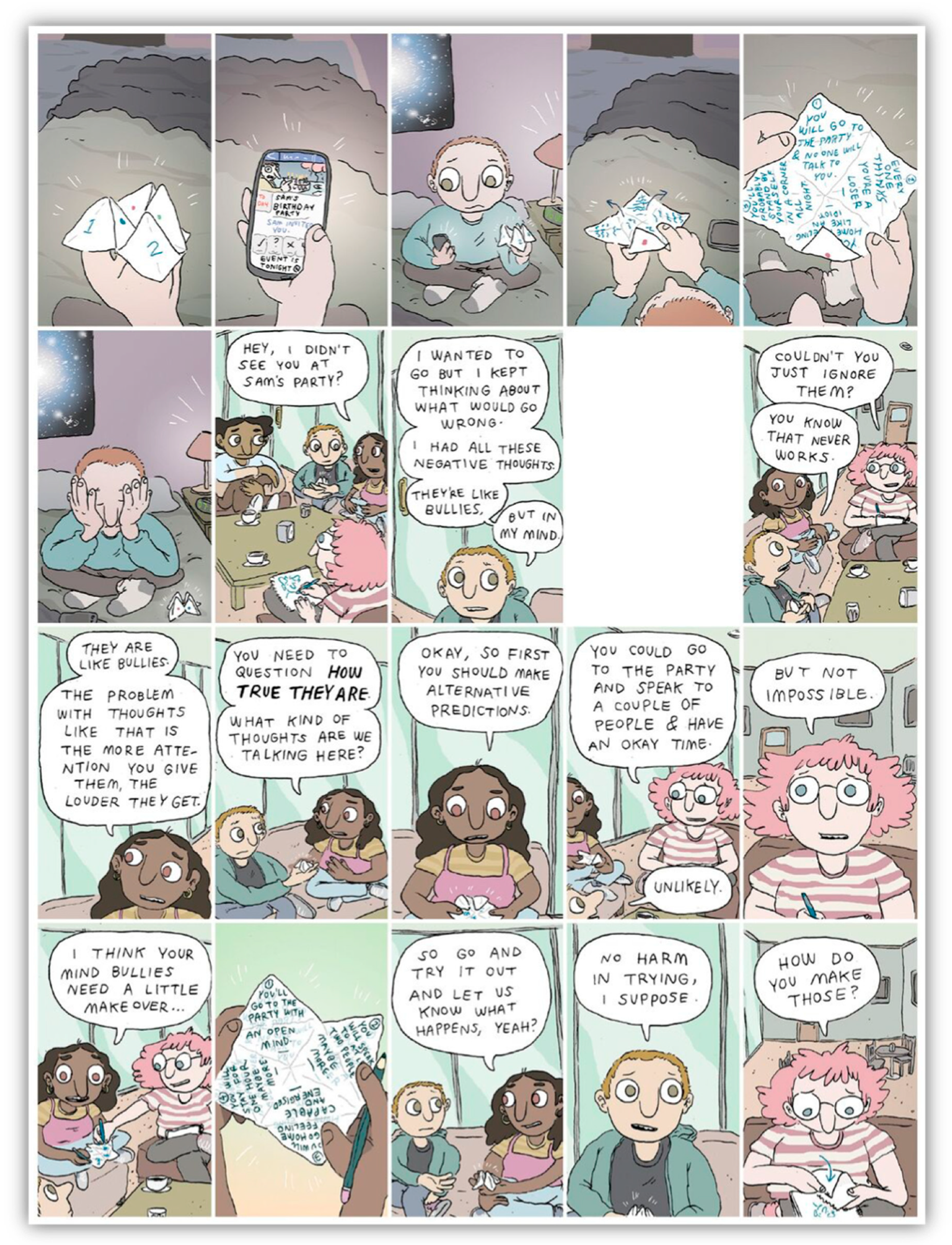
1.3. Program Design—Entourage
1.4. Aims
2. Materials and Methods
2.1. Research Design
2.2. Participants
2.3. Procedure
2.4. Intervention
2.5. Data Collection
2.5.1. Demographics/Quantitative Data
2.5.2. Semi-Structured Interviews
2.6. Qualitative Data Analysis
3. Results
3.1. Connection
I think, yeah, it came down to the fact that I wasn’t really alone in this, you know? Like, you could actually see and read the situations other people found themselves in and the ones that were similar to me and things like that so, I just like a sense of connection to the community of Entourage and I think that’s what I liked.(E230, Male, 23 years)
Just like knowing other people are going through it as well. Because I really felt like it was like a one-person thing, like my own thing. But now like, I know some other people now, there’s like 80 that are feeling the same thing. So just having that in the back of my head just feels a bit better.(E008, Female, 14 years)
3.2. Anxiety Management
Gaining a lot more skills and knowledge about how I can change my thinking about certain things or do things and get through situations and how to communicate better and things like that gave me a lot of resources that I can still go back and use.(E229, Male, 17 years)
I think just overall, I felt sort of when I went back out with into other social situations I felt better doing so. I didn’t feel as nervous doing things that beforehand I would have been freaking out.(E011, Female, 17 years)
3.3. Appeal
I really liked the cartoon comics; they were really good. It’s just like better than just having to read babble, it gives you a realistic live situation and you can really empathise and put yourself in the shoes of the comics, it just gives you a better understanding, seeing an animation play out what I’m thinking.(E225, Male, 23 years)
I think the fact that you can just do it by yourself. Yeah, you don’t have to take yourself anywhere, you can just stay in your pyjamas, you can… just be gentle with yourself. Yeah, to me it was kind of like therapy at home.(E031, Female, 17 years)
Appeal to Young Males
I think stigma is the biggest thing. But implementing it is the hardest thing. The only thing you can do is just talk, just get the conversation going…other than getting … people, not even like athletes or anything, just people that have their lives together, you know what I mean? Talking about it saying, talking about their experiences, I imagine that definitely helps.(E018, Male, 24 years)
Probably just to reinforce the safety of it, you know what I mean? Like, that is a safe place to be and there’s no judgment or prejudice or anything like that.(E230, Male, 23 years)
3.4. Disengagement
Giving people the opportunity to connect with other young people and that sense of community for working to better themselves; yeah, I’m not sure if it was super helpful for me. I think that’s particularly an age thing. Just because I’m right at that upper end of the age thing. I think it’s probably suited for a little bit younger than I am.(E231, Male, 25 years)
First thing, offering ways to encourage talking to other people. Encouraging more interaction between everyone. E.g. an optional thing where you can join a group to do something online, which could encourage people to talk about that thing outside of the group. Real life events would also help.(E214, Male, 19 years)
When I was talking in one of my headspace sessions the other week about Entourage, we mentioned about how we are all so anxious and afraid about talking online it is difficult to contribute on a site like Entourage, like if there was something to prompt engagement without feeling too exposed. Some anonymous and like an icebreaker sort of forum. Some kind of bridge to connect with other people.(E217, Female, 18 years)
3.5. System Improvement
Regarding what wasn’t helpful—it wasn’t as though Entourage set me back or had a negative impact, some parts of it just weren’t for me.(E013, Male, 16 years)
I think keep it all, because not everyone might, specifically, want to do this. Just have it all different ways of addressing the same thing, just all different versions. Just keep it all, I think, can be so helpful.(E033, Male, 22 years)
4. Discussion
4.1. Social Anxiety and Engagement
4.2. Gendered Experiences
4.3. Individual Needs
4.4. Study Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Participant Inclusion Criteria |
|---|
| Aged 12–25 years inclusive; Recent symptoms of social anxiety in the past 4 weeks indicated by a score of at least 30 on the Leibowitz Social Anxiety Scale; Are attending one of four headspace centres across north-western Melbourne; Are able to give informed consent; Have regular and ongoing use to the internet/a smartphone. |
| Participant Exclusion Criteria |
| Presence of an intellectual disability; Not able to converse in, or read English; Presence of comorbid physical health conditions requiring a high level of medical care; Current diagnosis of a schizophrenia spectrum or psychotic disorder. |
Appendix B
| Researcher | BOB | MW | LV |
|---|---|---|---|
| Interviews Conducted | 28 | 35 | 7 |
| Credentials | BA (Hons) | BA (Hons) | MSOCWK |
| Gender | Female | Male | Non-Binary |
| Experience and Training | Training completed on Entourage interview schedule. | Training completed on Entourage interview schedule in addition to previous qualitative interviewing experience. | Training completed on Entourage interview schedule in addition to previous qualitative interviewing experience. |
Appendix C
| Research Questions | Interview Questions |
|---|---|
| How did the project’s recruitment strategies influence the uptake and use of the project, and how did different populations of males respond? | Why did you join the Entourage project? |
| How did the gender sensitization of the project influence the ways that participants engaged with the program, and how did this differ by male characteristics? | What do you think is the single most important thing that a project like Entourage could do to get guys to join? [or insert other pronoun here for other genders] Do you think that Entourage hit the mark as far as [that thing]? |
| How did aspects of project implementation influence participant engagement with the project? | What kept you coming back to Entourage? |
| How did males interact with the project in ways that mobilize or constrain social connectedness or other outcomes, and how did this vary by context? | What would you say was the biggest benefit for you from the Entourage project? Can you give me an example of a time when Entourage helped you? What would you say was least helpful in the project? Can you give me an example of a time when the project did not help you? How has participating in Entourage changed how you connect with other fellas? What aspects of Entourage have helped enhance your social involvement? |
| What aspects of the project and project at large support the sustainability and scalability of the projects? | What parts of this project do you think should be continued so that other youth can benefit from them? If there was one thing the people running the project could improve, what would that be? For our final question, we’d like to know if there is anything else that you would like to share that we haven’t already asked about? |
References
- Burstein, M.; He, J.-P.; Kattan, G.; Albano, A.M.; Avenevoli, S.; Merikangas, K.R. Social phobia and subtypes in the National Comorbidity Survey–Adolescent Supplement: Prevalence, correlates, and comorbidity. J. Am. Acad. Child. Adolesc. Psychiatry 2011, 50, 870–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R. The impairments caused by social phobia in the general population: Implications for intervention. Acta Psychiatr. Scand. 2003, 108, 19–27. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Stein, D.J.; Lim, C.C.; Roest, A.M.; de Jonge, P.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Benjet, C.; Bromet, E.J.; Bruffaerts, R. The cross-national epidemiology of social anxiety disorder: Data from the World Mental Health Survey Initiative. BMC Med. 2017, 15, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Stein, D.J.; Scott, K.M.; de Jonge, P.; Kessler, R.C. Epidemiology of anxiety disorders: From surveys to nosology and back. Dialogues Clin. Neurosci. 2017, 19, 127–136. [Google Scholar] [CrossRef]
- Aderka, I.M.; Hofmann, S.G.; Nickerson, A.; Hermesh, H.; Gilboa-Schechtman, E.; Marom, S. Functional impairment in social anxiety disorder. J. Anxiety Disord. 2012, 26, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Nordh, M.; Vigerland, S.; Öst, L.-G.; Ljótsson, B.; Mataix-Cols, D.; Serlachius, E.; Högström, J. Therapist-guided internet-delivered cognitive–behavioural therapy supplemented with group exposure sessions for adolescents with social anxiety disorder: A feasibility trial. BMJ Open 2017, 7, e018345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, K.M.; Walker, J.; Batterham, P.J. Help seeking for social anxiety: A pilot randomised controlled trial. Digit. Health 2017, 3, 2055207617712047. [Google Scholar] [CrossRef]
- Koyuncu, A.; İnce, E.; Ertekin, E.; Tükel, R. Comorbidity in social anxiety disorder: Diagnostic and therapeutic challenges. Drugs Context 2019, 8. [Google Scholar] [CrossRef]
- Nicholas, J.; Oliver, K.; Lee, K.; O’Brien, M. Help-seeking behaviour and the Internet: An investigation among Australian adolescents. Aust. E-J. Adv. Ment. Health 2004, 3, 16–23. [Google Scholar] [CrossRef]
- Renton, T.; Tang, H.; Ennis, N.; Cusimano, M.D.; Bhalerao, S.; Schweizer, T.A.; Topolovec-Vranic, J. Web-based intervention programs for depression: A scoping review and evaluation. J. Med. Internet Res. 2014, 16, e209. [Google Scholar] [CrossRef]
- Rice, S.M.; Purcell, R.; McGorry, P.D. Adolescent and young adult male mental health: Transforming system failures into proactive models of engagement. J. Adolesc. Health 2018, 62, S9–S17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridout, B.; Campbell, A. The use of social networking sites in mental health interventions for young people: Systematic review. J. Med. Internet Res. 2018, 20, e12244. [Google Scholar] [CrossRef] [Green Version]
- Valentine, L.; McEnery, C.; D’Alfonso, S.; Phillips, J.; Bailey, E.; Alvarez-Jimenez, M. Harnessing the potential of social media to develop the next generation of digital health treatments in youth mental health. Curr. Treat. Options Psychiatry 2019, 1–12. [Google Scholar] [CrossRef]
- Grist, R.; Croker, A.; Denne, M.; Stallard, P. Technology Delivered Interventions for Depression and Anxiety in Children and Adolescents: A Systematic Review and Meta-analysis. Clin. Child. Fam. Psychol. Rev. 2019, 22, 147–171. [Google Scholar] [CrossRef] [Green Version]
- Podina, I.R.; Mogoase, C.; David, D.; Szentagotai, A.; Dobrean, A. A meta-analysis on the efficacy of technology mediated CBT for anxious children and adolescents. J. Ration. -Emot. Cogn. -Behav. Ther. 2016, 34, 31–50. [Google Scholar] [CrossRef]
- Carpenter, J.K.; Andrews, L.A.; Witcraft, S.M.; Powers, M.B.; Smits, J.A.; Hofmann, S.G. Cognitive behavioral therapy for anxiety and related disorders: A meta-analysis of randomized placebo-controlled trials. Depress. Anxiety 2018, 35, 502–514. [Google Scholar] [CrossRef] [PubMed]
- Mayo-Wilson, E.; Dias, S.; Mavranezouli, I.; Kew, K.; Clark, D.M.; Ades, A.; Pilling, S. Psychological and pharmacological interventions for social anxiety disorder in adults: A systematic review and network meta-analysis. Lancet Psychiatry 2014, 1, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Spence, S.H.; Donovan, C.L.; March, S.; Gamble, A.; Anderson, R.E.; Prosser, S.; Kenardy, J. A randomized controlled trial of online versus clinic-based CBT for adolescent anxiety. J. Consult. Clin. Psychol. 2011, 79, 629. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G. The law of attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- Rickwood, D.; Bradford, S. The role of self-help in the treatment of mild anxiety disorders in young people: An evidence-based review. Psychol. Res. Behav. Manag. 2012. [Google Scholar] [CrossRef] [Green Version]
- Naslund, J.A.; Aschbrenner, K.A.; Marsch, L.A.; Bartels, S.J. The future of mental health care: Peer-to-peer support and social media. Epidemiol. Psychiatr. Sci. 2016, 25, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, M.H.; Rodebaugh, T.L.; Zyphur, M.J.; Gleeson, J.F. Loneliness over time: The crucial role of social anxiety. J. Abnorm. Psychol. 2016, 125, 620. [Google Scholar] [CrossRef]
- Clarke, A.M.; Kuosmanen, T.; Barry, M.M. A systematic review of online youth mental health promotion and prevention interventions. J. Youth Adolesc. 2015, 44, 90–113. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Jimenez, M.; Bendall, S.; Lederman, R.; Wadley, G.; Chinnery, G.; Vargas, S.; Larkin, M.; Killackey, E.; McGorry, P.D.; Gleeson, J.F. On the HORYZON: Moderated online social therapy for long-term recovery in first episode psychosis. Schizophr. Res. 2013, 143, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, J.; Lederman, R.; Herrman, H.; Koval, P.; Eleftheriadis, D.; Bendall, S.; Cotton, S.M.; Alvarez-Jimenez, M. Moderated online social therapy for carers of young people recovering from first-episode psychosis: Study protocol for a randomised controlled trial. Trials 2017, 18, 27. [Google Scholar] [CrossRef] [Green Version]
- Rice, S.; Gleeson, J.; Davey, C.; Hetrick, S.; Parker, A.; Lederman, R.; Wadley, G.; Murray, G.; Herrman, H.; Chambers, R. Moderated online social therapy for depression relapse prevention in young people: Pilot study of a ‘next generation’online intervention. Early Interv. Psychiatry 2018, 12, 613–625. [Google Scholar] [CrossRef]
- Alvarez-Jimenez, M.; Rice, S.; D’Alfonso, S.; Leicester, S.; Bendall, S.; Pryor, I.; Russon, P.; McEnery, C.; Santesteban-Echarri, O.; Da Costa, G. A Novel multimodal digital service (moderated online social therapy+) for help-seeking young people experiencing mental ill-health: Pilot evaluation within a national youth e-mental health service. J. Med. Internet Res. 2020, 22, e17155. [Google Scholar] [CrossRef]
- Alvarez-Jimenez, M.; Gleeson, J.F.; Bendall, S.; Penn, D.L.; Yung, A.R.; Ryan, R.M.; Eleftheriadis, D.; D’Alfonso, S.; Rice, S.; Miles, C.; et al. Enhancing social functioning in young people at Ultra High Risk (UHR) for psychosis: A pilot study of a novel strengths and mindfulness-based online social therapy. Schizophr. Res. 2018, 202, 369–377. [Google Scholar] [CrossRef]
- Rice, S.; O’Bree, B.; Wilson, M.; McEnery, C.; Lim, M.H.; Hamilton, M.; Gleeson, J.; Bendall, S.; D’Alfonso, S.; Russon, P. Leveraging the social network for treatment of social anxiety: Pilot study of a youth-specific digital intervention with a focus on engagement of young men. Internet Interv. 2020, 100323. [Google Scholar] [CrossRef]
- Gleeson, J.F.; Alvarez-Jimenez, M.; Lederman, R. Moderated online social therapy for recovery from early psychosis. Psychiatr. Serv. 2012, 63, 719. [Google Scholar] [CrossRef]
- Stallard, P.; Richardson, T.; Velleman, S.; Attwood, M. Computerized CBT (Think, Feel, Do) for depression and anxiety in children and adolescents: Outcomes and feedback from a pilot randomized controlled trial. Behav. Cogn. Psychother. 2011, 39, 273–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glasgow, R.E. Enhancing the scientific foundation of internet intervention research. Ann. Behav. Med. 2009, 38, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Proudfoot, J.; Klein, B.; Barak, A.; Carlbring, P.; Cuijpers, P.; Lange, A.; Ritterband, L.; Andersson, G. Establishing guidelines for executing and reporting internet intervention research. Cogn. Behav. Ther. 2011, 40, 82–97. [Google Scholar] [CrossRef]
- Beattie, A.; Shaw, A.; Kaur, S.; Kessler, D. Primary-care patients’ expectations and experiences of online cognitive behavioural therapy for depression: A qualitative study. Health Expect. 2009, 12, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Barker, C.; Pistrang, N.; Elliott, R. Research Methods in Clinical Psychology: An. Introduction for Students and Practitioners; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar] [CrossRef]
- Rice, S.; O’Bree, B.; Wilson, M.; McEnery, C.; Lim, M.H.; Hamilton, M.; Gleeson, J.; Bendall, S.; D’Alfonso, S.; Russon, P. Development of a graphic medicine-enabled social media-based intervention for youth social anxiety. Clin. Psychol. 2020. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- McEnery, C.; Lim, M.H.; Knowles, A.; Rice, S.; Gleeson, J.; Howell, S.; Russon, P.; Miles, C.; D’Alfonso, S.; Alvarez-Jimenez, M. Social anxiety in young people with first-episode psychosis: Pilot study of the EMBRACE moderated online social intervention. Early Interv. Psychiatry 2019. [Google Scholar] [CrossRef] [PubMed]
- Erlingsson, C.; Brysiewicz, P. A hands-on guide to doing content analysis. Afr. J. Emerg. Med. 2017, 7, 93–99. [Google Scholar] [CrossRef]
- Krippendorff, K. Content Analysis: An Introduction to its Methodology; Sage Publications: New York, NY, USA, 2018. [Google Scholar]
- Liebowitz, M.R. Social Phobia. Mod. Probl. Pharm. 1987, 22, 141–173. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Rau, P.P.-L.; Ma, L. Understanding lurkers in online communities: A literature review. Comput. Hum. Behav. 2014, 38, 110–117. [Google Scholar] [CrossRef]
- Bonetti, L.; Campbell, M.A.; Gilmore, L. The relationship of loneliness and social anxiety with children’s and adolescents’ online communication. Cyberpsychologybehav. Soc. Netw. 2010, 13, 279–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentine, L.; McEnery, C.; O’Sullivan, S.; Gleeson, J.; Bendall, S.; Alvarez-Jimenez, M. Young People’s Experience of a Long-Term Social Media–Based Intervention for First-Episode Psychosis: Qualitative Analysis. J. Med. Internet Res. 2020, 22, e17570. [Google Scholar] [CrossRef]
- Addis, M.E.; Mahalik, J.R. Men, masculinity, and the contexts of help seeking. Am. Psychol. 2003, 58, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millet, N.; Longworth, J.; Arcelus, J. Prevalence of anxiety symptoms and disorders in the transgender population: A systematic review of the literature. Int. J. Transgend. 2017, 18, 27–38. [Google Scholar] [CrossRef]
- Yardley, L.; Spring, B.J.; Riper, H.; Morrison, L.G.; Crane, D.H.; Curtis, K.; Merchant, G.C.; Naughton, F.; Blandford, A. Understanding and promoting effective engagement with digital behavior change interventions. Am. J. Prev. Med. 2016, 51, 833–842. [Google Scholar] [CrossRef] [Green Version]
- Baldwin, S.A.; Berkeljon, A.; Atkins, D.C.; Olsen, J.A.; Nielsen, S.L. Rates of change in naturalistic psychotherapy: Contrasting dose–effect and good-enough level models of change. J. Consult. Clin. Psychol. 2009, 77, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGorry, P.; Trethowan, J.; Rickwood, D. Creating headspace for integrated youth mental health care. World Psychiatry 2019, 18, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kealy, D.; Rice, S.M.; Ogrodniczuk, J.S.; Spidel, A. Childhood trauma and somatic symptoms among psychiatric outpatients: Investigating the role of shame and guilt. Psychiatry Res. 2018, 268, 169–174. [Google Scholar] [CrossRef]
- Callow, T.J.; Moffitt, R.L.; Neumann, D.L. External shame and its association with depression and anxiety: The moderating role of self-compassion. Aust. Psychol. 2021, 1–11. [Google Scholar] [CrossRef]


| Phase. | Examples of Procedure for Each Step |
|---|---|
| 1. Familiarisation with the data | Transcribe data; read and re-read transcripts; document reflective thoughts; store raw data in well-organised archives |
| 2. Identify and Condense Meaning Units | Divide the text into meaning units; condense meaning units further keeping the central meaning intact; researcher triangulation |
| 3. Formulate Codes | Generate a coding framework from initial meaning units; Code features of the data systematically across the dataset, collate data relevant to each code; researcher triangulation; supervision; document all meetings and decisions |
| 4. Develop Categories | Organise codes into potential categories, gather all data relevant to each potential category; keep detailed notes about development and organisation of concepts |
| 5. Review Categories | Researcher triangulation; Supervision and vetting of categories; check if categories are consistent in relation to coded extracts and entire data-set; team consensus of categories |
| 6. Produce Report | Final opportunity for analysis; select appropriate extracts; thick descriptions of context; description of coding and analysis; produce report that includes theoretical, methodological and analytical choices throughout entire study |
| Category | Number of Transcripts Mentioned in (Males Mentioned) n = 70 | Category | Number of Transcripts Mentioned in (Males Mentioned) n = 70 | ||||
|---|---|---|---|---|---|---|---|
| Connection | n | % Total | % Males | Appeal (Young Males) | n | % Total | % Males |
| Shared experiences normalised own experiences | 33 (17) | 47.1 | 51.5 | Uncertain what appeals to young males | 18 (9) | 25.7 | 50.0 |
| Increased confidence to talk or connect with other people | 32 (15) | 45.7 | 46.9 | Address stigma and normalise help-seeking | 15 (9) | 21.4 | 60.0 |
| The environment felt supportive | 27 (11) | 38.6 | 40.7 | Accessible online | 14 (8) | 20.0 | 57.1 |
| Connecting with other users on Entourage | 26 (12) | 37.1 | 46.2 | A safe and trustworthy environment | 14 (7) | 20.0 | 50.0 |
| Therapist support was helpful | 21 (12) | 30.0 | 57.1 | Familiarity is appealing to young males (e.g., games) | 6 (6) | 8.6 | 100.0 |
| The opportunity to connect with others was appealing | 21 (10) | 30.0 | 47.6 | Evidence-based content | 6 (6) | 8.6 | 100.0 |
| Being able to discuss and problem solve issues as a group | 20 (7) | 28.6 | 35.0 | Authentic, relatable content | 5 (5) | 7.1 | 100.0 |
| Entourage helped to share problems and be more open | 15 (9) | 21.4 | 60.0 | Support from other male peers | 5 (2) | 7.1 | 40.0 |
| Entourage has not enhanced social environment | 14 (6) | 20.0 | 42.9 | Privacy | 4 (1) | 5.7 | 25.0 |
| Entourage helped to form new relationships | 6 (2) | 8.6 | 33.3 | Having real people on Entourage | 3 (3) | 4.3 | 100.0 |
| Peer moderator support was helpful | 3 (1) | 4.3 | 33.3 | Mental health content from role models | 2 (2) | 2.9 | 100.0 |
| Having real people as support on Entourage was helpful | 1 (1) | 1.4 | 100.0 | Recommended by a peer or someone trustworthy | 2 (2) | 2.9 | 100.0 |
| Appeal (Overall) | Anxiety Management | ||||||
| Open to trying something new to help themselves | 41 (20) | 58.6 | 48.8 | Anxiety psychoeducation and management strategies were helpful | 57 (29) | 81.4 | 50.9 |
| Opportunity to learn anxiety management techniques | 41 (17) | 58.6 | 41.5 | The therapy modules (steps) were beneficial | 49 (25) | 70.0 | 51.0 |
| Easy to use and accessible when needed | 29 (11) | 41.4 | 37.9 | Available as a back-up support to use when needed | 19 (9) | 27.1 | 47.4 |
| Content was relatable and appropriate | 25 (12) | 35.7 | 48.0 | Entourage helped to reduce anxiety symptoms | 17 (8) | 24.3 | 47.1 |
| Worked reliably and as it was expected to | 23 (14) | 32.9 | 60.9 | The mindfulness tracks were beneficial | 11 (5) | 15.7 | 45.5 |
| Entourage was a desirable platform | 20 (9) | 28.6 | 45.0 | Notifications were helpful as a reminder | 10 (6) | 14.3 | 60.0 |
| Entourage appeared like a safe environment | 4 (0) | 5.7 | 0.0 | Reading other’s experiences of anxiety was reassuring | 10 (4) | 14.3 | 40.0 |
| Entourage was recommended to them | 18 (3) | 25.7 | 16.7 | Entourage could be used for solving problems | 9 (3) | 12.9 | 33.3 |
| Could be used in a self-directed way | 13 (4) | 18.6 | 30.8 | Reinforced strategies learned in face-to-face therapy | 6 (2) | 8.6 | 33.3 |
| Interested in helping others through research or on the platform | 11 (7) | 15.7 | 63.6 | Entourage provided the opportunity to practice skills | 6 (2) | 8.6 | 33.3 |
| Anonymity | 8 (3) | 11.4 | 37.5 | ||||
| Having real people on Entourage was appealing | 5 (2) | 7.1 | 40.0 | ||||
| Reimbursement for participating | 2 (1) | 2.9 | 50.0 | ||||
| Disengagement | System Improvement | ||||||
| Did not have enough time to fully engage with Entourage | 24 (12) | 34.3 | 50.0 | Useful to different people in different ways | 31 (15) | 44.3 | 48.4 |
| Entourage was not very user-friendly | 18 (9) | 25.7 | 50.0 | Could be more user-friendly (e.g., fewer system glitches) | 25 (15) | 35.7 | 60.0 |
| Anxiety stopped them from engaging | 18 (1) | 25.7 | 5.6 | Increased study promotion | 19 (9) | 27.1 | 47.4 |
| The social element of Entourage was not relevant | 15 (8) | 21.4 | 53.3 | More encouragement or assistance to connect with other users would have been helpful | 15 (6) | 21.4 | 40.0 |
| Not interested in social aspect of Entourage | 14 (6) | 20.0 | 42.9 | Uncertain what could have improved Entourage | 15 (5) | 21.4 | 33.3 |
| The information on Entourage was not relevant | 14 (2) | 20.0 | 14.3 | Would be more user-friendly as an application (app) | 12 (8) | 17.1 | 66.7 |
| Did not feel connected to other users on Entourage | 9 (4) | 12.9 | 44.4 | Notifications could be improved | 8 (5) | 11.4 | 62.5 |
| Too much information on Entourage | 8 (5) | 11.4 | 62.5 | Tailor the platform for individual preferences | 8 (4) | 11.4 | 50.0 |
| Forgot to use Entourage | 8 (3) | 11.4 | 37.5 | Information on Entourage could be too complicated | 4 (2) | 5.7 | 50.0 |
| There was not a lot of activity occurring on Entourage | 8 (3) | 11.4 | 37.5 | Some content on Entourage was too simple | 3 (1) | 4.3 | 33.3 |
| Notifications from Entourage could feel overwhelming | 7 (4) | 10.0 | 57.1 | More gamification | 2 (1) | 2.9 | 50.0 |
| Preferred in-person support | 7 (4) | 10.0 | 57.1 | More rewards for engaging in content | 2 (0) | 2.9 | 0.0 |
| Avoided using Entourage (e.g., when feeling guilty or mental health had worsened) | 7 (3) | 10.0 | 42.9 | ||||
| Did not get support or answers as quickly as desired | 3 (1) | 4.3 | 33.3 | ||||
| Distrusting because had not met anyone in real life | 2 (0) | 2.9 | 0.0 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Bree, B.; Walton, C.C.; Bendall, S.; Wilson, M.; Valentine, L.; McEnery, C.; D’Alfonso, S.; Alvarez-Jimenez, M.; Rice, S. Perceived Helpfulness of a Moderated Online Social Therapy Network for Young People Experiencing Social Anxiety. Int. J. Environ. Res. Public Health 2021, 18, 2796. https://doi.org/10.3390/ijerph18062796
O’Bree B, Walton CC, Bendall S, Wilson M, Valentine L, McEnery C, D’Alfonso S, Alvarez-Jimenez M, Rice S. Perceived Helpfulness of a Moderated Online Social Therapy Network for Young People Experiencing Social Anxiety. International Journal of Environmental Research and Public Health. 2021; 18(6):2796. https://doi.org/10.3390/ijerph18062796
Chicago/Turabian StyleO’Bree, Bridget, Courtney C Walton, Sarah Bendall, Michael Wilson, Lee Valentine, Carla McEnery, Simon D’Alfonso, Mario Alvarez-Jimenez, and Simon Rice. 2021. "Perceived Helpfulness of a Moderated Online Social Therapy Network for Young People Experiencing Social Anxiety" International Journal of Environmental Research and Public Health 18, no. 6: 2796. https://doi.org/10.3390/ijerph18062796
APA StyleO’Bree, B., Walton, C. C., Bendall, S., Wilson, M., Valentine, L., McEnery, C., D’Alfonso, S., Alvarez-Jimenez, M., & Rice, S. (2021). Perceived Helpfulness of a Moderated Online Social Therapy Network for Young People Experiencing Social Anxiety. International Journal of Environmental Research and Public Health, 18(6), 2796. https://doi.org/10.3390/ijerph18062796