
Effects of Virtual Reality-Based Therapy on Quality of Life of Patients with Subacute Stroke: A Three-Month Follow-Up Randomized Controlled Trial

 ,
,  ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
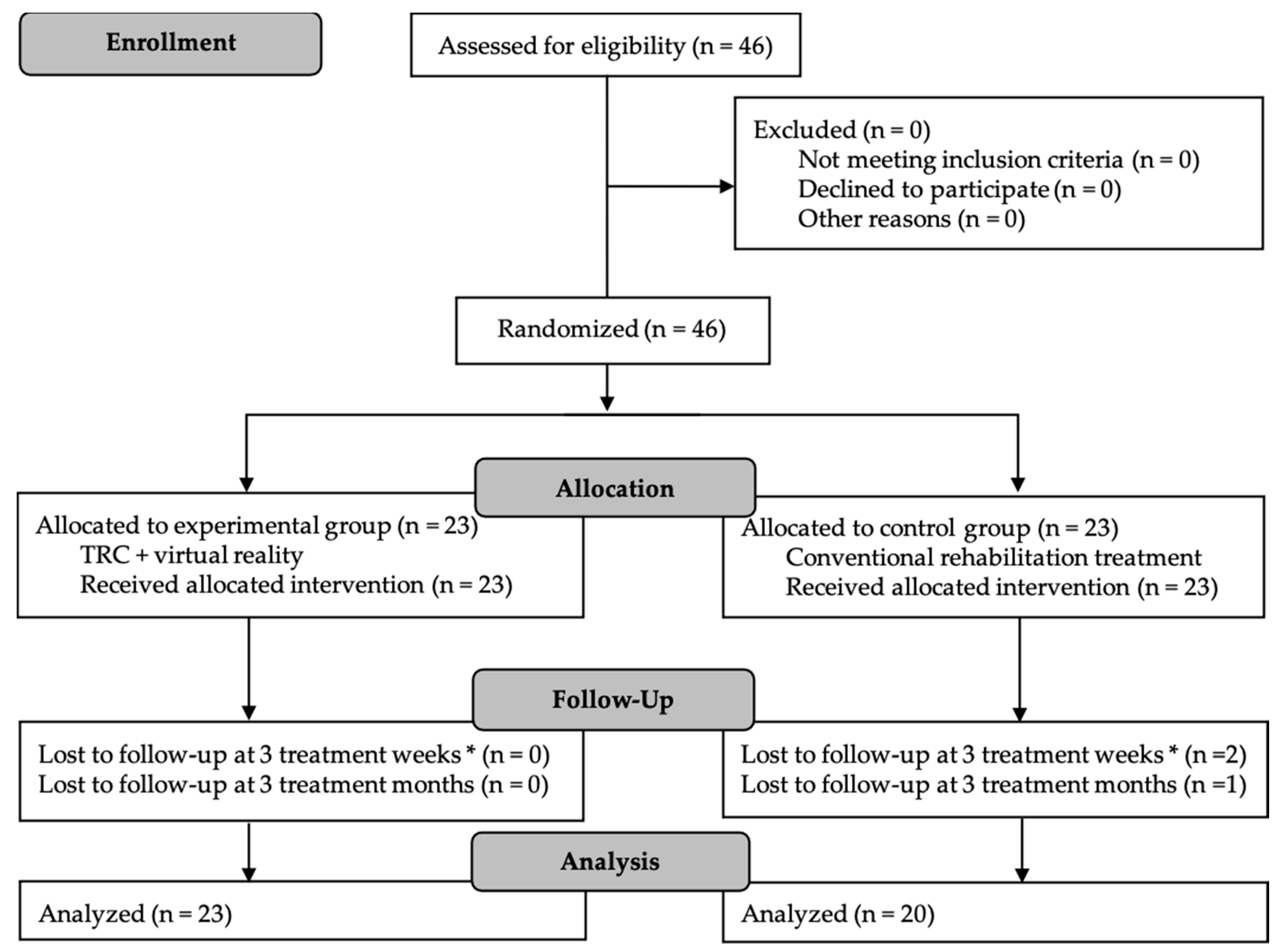
2.1. Study Design
2.2. Participant and Settings
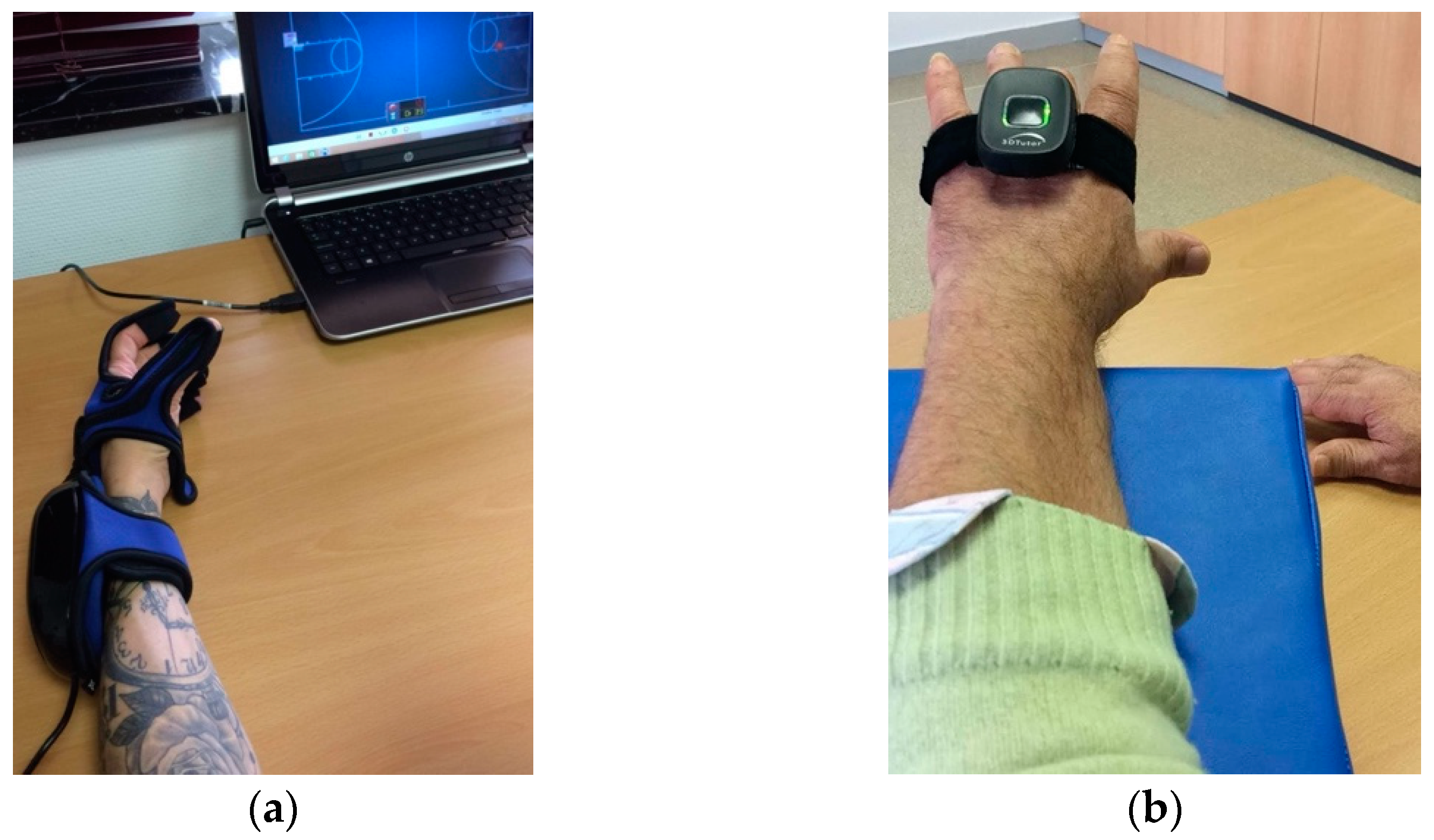
2.3. Intervention
2.4. Outcomes Measures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mendis, S. Stroke Disability and Rehabilitation of Stroke: World Health Organization Perspective. Int. J. Stroke 2013, 8, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, C.B.; Medeiros, I.R.T.; Greters, M.G.; Frota, N.A.F.; Tavares, L.; Scaff, M.; Conforto, A.B. Abnormal sensory integration affects balance control in hemiparetic patients within the first year after stroke. Clinics 2011, 66, 2043–2048. [Google Scholar] [CrossRef] [Green Version]
- Duncan, J.; Van Wijck, F.; Pollock, A.; Ali, M. Outcome measures in post-stroke arm rehabilitation trials: Do existing measures capture outcomes that are important to stroke survivors, carers, and clinicians? Clin. Rehabil. 2019, 33, 737–749. [Google Scholar] [CrossRef] [Green Version]
- Bosomworth, H.; Rodgers, H.; Shaw, L.; Smith, L.; Aird, L.; Howel, D.; Wilson, N.; Alvarado, N.; Andole, S.; Cohen, D.L.; et al. Evaluation of the enhanced upper limb therapy programme within the Robot-Assisted Training for the Upper Limb after Stroke trial: Descriptive analysis of intervention fidelity, goal selection and goal achievement. Clin. Rehabil. 2020, 35, 119–134. [Google Scholar] [CrossRef]
- Schnabel, S.; Van Wijck, F.; Bain, B.; Barber, M.; Dall, P.; Fleming, A.; Kerr, A.; Langhorne, P.; McConnachie, A.; Molloy, K.; et al. Experiences of augmented arm rehabilitation including supported self-management after stroke: A qualitative investigation. Clin. Rehabil. 2020, 35, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.; Tallis, R.C. Balance Disability after Stroke. Phys. Ther. 2006, 86, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Tessem, S.; Hagstrøm, N.; Fallang, B. Weight distribution in standing and sitting positions, and weight transfer during reaching tasks, in seated stroke subjects and healthy subjects. Physiother. Res. Int. 2007, 12, 82–94. [Google Scholar] [CrossRef] [PubMed]
- Cano-Mañas, M.J.; Collado-Vázquez, S.; Rodríguez, J.; Muñoz, A.J.; Cano-de-la-Cuerda, R. Effects of Video-Game Based Therapy on Balance, Postural Control, Functionality, and Quality of Life of Patients with Subacute Stroke: A Randomized Controlled Trial. J. Healthc. Eng. 2020, 2020, 5480315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.H.; Van Wijck, F.; Joice, S.; Donaghy, M. Predicting health related quality of life 6 months after stroke: The role of anxiety and upper limb dysfunction. Disabil. Rehabil. 2013, 35, 291–299. [Google Scholar] [CrossRef]
- Salter, K.L.; Moses, M.B.; Foley, N.C.; Teasell, R.W. Health-related quality of life after stroke: What are we measuring? Int. J. Rehabil. Res. 2008, 31, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Testa, M.A.; Simonson, D.C. Assessment of Quality-of-Life Outcomes. N. Engl. J. Med. 1996, 334, 835–840. [Google Scholar] [CrossRef]
- Barrera, Y.M.; Concepción, O.F.; Hernández, T.E. Calidad de vida en pacientes post-ictus: Factores determinantes desde la fase aguda. Rev. Haban. Cienc. Med. 2016, 15, 508–524. [Google Scholar]
- García-Moriche, N.; Rodríguez-Gonzalo, A.; Muñoz-Lobo, M.J.; Parra-Cordero, S.; Fernández-De Pablos, A. Quality of life in stroke patients. A phenomenological study. Enferm. Clin. 2010, 20, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Aceituno-Gómez, J.; García-Madero, V.M.; Blázquez-Gamallo, R.; Harto-Martínez, A.M.; Mohedano, A.; Viñuela, A.; Avendaño-Coy, J.; Gómez-Soriano, J.; Muñoz-González, A.; González-González, J.; et al. Health-related quality of life in patients diagnosed with subacromial syndrome in the Talavera Integrated Area. Rev. Esp. Salud Publica 2019, 93, e201910094. [Google Scholar]
- Ayis, S.; Wellwood, I.; Rudd, A.G.; McKevitt, C.; Parkin, D.; Wolfe, C.D.A. Variations in Health-Related Quality of Life (HRQoL) and survival 1 year after stroke: Five European population-based registers. BMJ Open 2015, 5, e007101. [Google Scholar] [CrossRef]
- Devlin, N.J.; Parkin, D.; Browne, J. Patient-reported outcome measures in the NHS: New methods for analysing and reporting EQ-5D data. Health Econ. 2010, 19, 886–905. [Google Scholar] [CrossRef]
- Da Silva, M.; Bermúdez, S.; Duarte, E.; Verschure, P.F.M.J. Virtual reality based rehabilitation speeds up functional recovery of the upper extremities after stroke: A randomized controlled pilot study in the acute phase of stroke using the rehabilitation gaming system. Restor. Neurol. Neurosci. 2011, 29, 287–298. [Google Scholar] [CrossRef] [Green Version]
- Mekbib, D.B.; Han, J.; Zhang, L.; Fang, S.; Jiang, H.; Zhu, J.; Roe, A.W.; Xu, D. Virtual reality therapy for upper limb rehabilitation in patients with stroke: A meta-analysis of randomized clinical trials. Brain Inj. 2020, 34, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.A.; Singh, D.K.A.; Mohd, N.A.; Hooi, K.; Ibrahim, N. Virtual Reality Games as an Adjunct in Improving Upper Limb Function and General Health among Stroke Survivors. Int. J. Environ. Res. Public Health 2019, 16, 5144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akinladejo, F.O. Virtual Environments in Physical Therapy. In Virtual Reality and Environments; Sík Lányi, C., Ed.; IntechOpen: University of Pannonia, Veszprém, Hungary, 2012; pp. 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sveistrup, H. Motor rehabilitation using virtual reality. J. Neuroeng. Rehabil. 2004, 1, 10. [Google Scholar] [CrossRef] [Green Version]
- ISRCTN—ISRCTN27760662: Effectiveness of Virtual Reality Devices in the Rehabilitation of Adults with Stroke. Available online: http://www.isrctn.com/ISRCTN27760662 (accessed on 8 January 2021).
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmeli, E.; Peleg, S.; Bartur, G.; Elbo, E.; Vatine, J.J. HandTutorTM enhanced hand rehabilitation after stroke—A pilot study. Physiother. Res. Int. 2011, 16, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Hernández, M.; Fernández-Panadero, C.; López-Martín, O.; Polonio-López, B. Hand Rehabilitation after Chronic Brain Damage: Effectiveness, Usability and Acceptance of Technological Devices: A Pilot Study. In Physical Disabilities—Therapeutic Implications; Tan, U., Ed.; IntechOpen: Cukurova University, Sarıçam/Adana, Turkey, 2017; pp. 57–72. [Google Scholar] [CrossRef] [Green Version]
- Chua, K.S.G.; Kuah, C.W.K. Innovating With Rehabilitation Technology in the Real World: Promises, Potentials, and Perspectives. Am. J. Phys. Med. Rehabil. 2017, 96, S150–S156. [Google Scholar] [CrossRef] [Green Version]
- Grefkes, C.; Fink, G.R. Connectivity-based approaches in stroke and recovery of function. Lancet Neurol. 2014, 13, 206–216. [Google Scholar] [CrossRef]
- Saposnik, G.; Cohen, L.G.; Mamdani, M.; Pooyania, S.; Ploughman, M.; Cheung, D.; Shaw, J.; Hall, J.; Nord, P.; Dukelow, S.; et al. Efficacy and safety of non-immersive virtual reality exercising in stroke rehabilitation (EVREST): A randomised, multicentre, single-blind, controlled trial. Lancet Neurol. 2016, 15, 1019–1027. [Google Scholar] [CrossRef] [Green Version]
- Sampaio-Baptista, C.; Sanders, Z.B.; Johansen-Berg, H. Structural Plasticity in Adulthood with Motor Learning and Stroke Rehabilitation. Annu. Rev. Neurosci. 2018, 41, 25–40. [Google Scholar] [CrossRef]
- Handtutor MediTouch. Available online: https://meditouch.co.il/products/handtutor/ (accessed on 9 January 2021).
- 3DTutor MediTouch. Available online: https://meditouch.co.il/products/3dtutor/ (accessed on 9 January 2021).
- Rehametrics|Cuantificando la Rehabilitación Física y Cognitiva. Available online: https://rehametrics.com/ (accessed on 9 January 2021).
- Martínez, M.C.; Parejo, M.T.; Laiz, N.M. Valoración del uso de las nuevas tecnologías en personas con esclerosis múltiple. REDIS 2018, 6, 149–171. [Google Scholar] [CrossRef] [Green Version]
- Abreu, J.; Rebelo, S.; Paredes, H.; Barroso, J.; Martins, P.; Reis, A.; EuricoVasco, A. Assessment of Microsoft Kinect in the Monitoring and Rehabilitation of Stroke Patients. In Recent Advances in Information Systems and Technologies; Rocha, Á., Correia, A.M., Adeli, H., Reis, L.P., Costanzo, S., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 167–174. [Google Scholar] [CrossRef] [Green Version]
- Ashwini, K.; Amutha, R.; Nagarajan, K.K.; Raj, S.A. Kinect based Upper Limb Performance Assessment in Daily Life Activities. In Proceedings of the International Conference on Wireless Communications Signal Processing and Networking (WiSPNET), Chennai, India, 21–23 March 2019; pp. 201–205. [Google Scholar] [CrossRef]
- Mousavi, H.; Khademi, M. A Review on Technical and Clinical Impact of Microsoft Kinect on Physical Therapy and Rehabilitation. J. Med. Eng. 2014, 2014, 846514. [Google Scholar] [CrossRef] [Green Version]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. [The Spanish version of EuroQol: A description and its applications. European Quality of Life scale]. Med. Clin. 1999, 112, 79–85. [Google Scholar]
- Herdman, M.; Badia, X.; Berra, S. El EuroQol-5D: Una alternativa sencilla para la medición de la calidad de vida relacionada con la salud en atención primaria. Aten. Primaria 2001, 28, 425–429. [Google Scholar] [CrossRef] [Green Version]
- Räsänen, P.; Roine, E.; Sintonen, H.; Semberg-Konttinen, V.; Ryynänen, O.P.; Roine, R. Use of quality-adjusted life years for the estimation of effectiveness of health care: A systematic literature review. Int. J. Technol. Assess. Health Care 2006, 22, 235–241. [Google Scholar] [CrossRef]
- Yoshida, I.; Hirao, K.; Kobayashi, R. The effect on subjective quality of life of occupational therapy based on adjusting the challenge–skill balance: A randomized controlled trial. Clin. Rehabil. 2019, 33, 1732–1746. [Google Scholar] [CrossRef]
- Robinson, A.; Gyrd-Hansen, D.; Bacon, P.; Baker, R.; Pennington, M.; Donaldson, C. Estimating a WTP-based value of a QALY: The ‘chained’ approach. Soc. Sci. Med. 2013, 92, 92–104. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, I.; Hirao, K.; Nonaka, T. Adjusting Challenge-Skill Balance to Improve Quality of Life in Older Adults: A Randomized Controlled Trial. Am. J. Occup. Ther. 2018, 72, 7201205030p1–7201205030p8. [Google Scholar] [CrossRef]
- Cai, W.; Mueller, C.; Li, Y.J.; Shen, W.D.; Stewart, R. Post stroke depression and risk of stroke recurrence and mortality: A systematic review and meta-analysis. Ageing Res. Rev. 2019, 50, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Huang, L.L.; Lee, C.F.; Hsieh, C.L.; Lin, Y.C.; Liu, H.; Chen, M.-I.; Lu, W.-S. A controlled pilot trial of two commercial video games for rehabilitation of arm function after stroke. Clin. Rehabil. 2015, 29, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, L.R.A.; Carregosa, A.A.; Masruha, M.R.; Dos Santos, P.A.; Da Silveira, M.L.; Ferraz, D.D.; Ribeiro, N.M.D.S. The Use of Nintendo Wii in the Rehabilitation of Poststroke Patients: A Systematic Review. J. Stroke Cerebrovasc. Dis. 2015, 24, 2298–2305. [Google Scholar] [CrossRef]
- Cheok, G.; Tan, D.; Low, A.; Hewitt, J. Is Nintendo Wii an Effective Intervention for Individuals With Stroke? A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2015, 16, 923–932. [Google Scholar] [CrossRef] [PubMed]
- Maier, M.; Rubio, B.; Duff, A.; Duarte, E.; Verschure, P.F.M.J. Effect of Specific Over Nonspecific VR-Based Rehabilitation on Poststroke Motor Recovery: A Systematic Meta-analysis. Neurorehabil. Neural Repair 2019, 33, 112–129. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.E.; George, S.; Thomas, S.; Deutsch, J.E.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2015, 2015, CD008349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, E.; Dodakian, L.; See, J.; McKenzie, A.; Le, V.; Wojnowicz, M.; Shahbaba, B.; Cramer, S.C. Neural function, injury, and stroke subtype predict treatment gains after stroke. Ann. Neurol. 2015, 77, 132–145. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.; Lin, K.; Liu, H.; Chen, Y.; Wu, C. Changes in structural integrity are correlated with motor and functional recovery after post-stroke rehabilitation. Restor. Neurol. Neurosci. 2015, 33, 835–844. [Google Scholar] [CrossRef]
- Fan, Y.T.; Wu, C.Y.; Liu, H.L.; Lin, K.C.; Wai, Y.Y.; Chen, Y.L. Neuroplastic changes in resting-state functional connectivity after stroke rehabilitation. Front. Hum. Neurosci. 2015, 9, 546. [Google Scholar] [CrossRef] [Green Version]
- Luque-Moreno, C.; Ferragut-Garcías, A.; Rodríguez-Blanco, C.; Heredia-Rizo, A.M.; Oliva-Pascual-Vaca, J.; Kiper, P.; Oliva-Pascual-Vaca, Á. A Decade of Progress Using Virtual Reality for Poststroke Lower Extremity Rehabilitation: Systematic Review of the Intervention Methods. BioMed Res. Int. 2015, 2015, 342529. [Google Scholar] [CrossRef] [Green Version]
- Colomer, C.; Llorens, R.; Noé, E.; Alcañiz, M. Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke. J. Neuroeng. Rehabil. 2016, 13, 45. [Google Scholar] [CrossRef] [Green Version]
- Ho, T.H.; Yang, F.C.; Lin, R.C.; Chien, W.C.; Chung, C.H.; Chiang, S.L.; Chou, C.-H.; Tsai, C.-K.; Lin, Y.-K.; Lee, J.-T. Impact of virtual reality-based rehabilitation on functional outcomes in patients with acute stroke: A retrospective case-matched study. J. Neurol. 2019, 266, 589–597. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Study Variables | Experimental Group (n = 23) | Control Group (n = 20) | Difference of Mean between Groups (p-Value) |
|---|---|---|---|
| Age | |||
| Mean (SD) Below 55 years (%) 55 to 70 years (%) Above 70 years (%) | 62.6 (13.5) 26.1 30.4 43.5 | 63.6 (12.2) 25.0 45.0 30.0 | −0.9 (0.812) 0.566 |
| Sex | |||
| Male Female | 78.3 21.7 | 85.0 15.0 | 0.571 |
| Main diagnostic | |||
| Ischemic/thrombotic Hemorrhagic | 91.3 8.7 | 90.0 10.0 | 0.883 |
| Middle cerebral artery lesion (%) | 60.9 | 55.0 | 0.697 |
| Time since diagnostic (days) * | |||
| Baseline (pre-intervention) Post-intervention (3 week follow-up) Follow-up (3 months) | 55.3 (34.3) 75.3 (34.3) 162.3 (36.9) | 54.2 (30.4) 74.2 (30.4) 157.2 (36.1) | 1.1 (0.909) 1.1 (0.909) 5.1 (0.650) |
| Hemispatial neglect syndrome (%) | 13.0 | 10.0 | 0.756 |
| Presence of pain in extremities | |||
| Baseline (pre-intervention) Post-intervention (3 week follow-up) Follow-up (3 months) | 43.5 21.7 82.6 | 50.0 80.0 100.0 | 0.669 0.000 0.050 |
| Location of the brain injury (%) | |||
| Right Left | 82.6 17.4 | 85.0 15.0 | 0.832 |
| Dominance (change baseline to post-intervention) | |||
| Right Left | 100.0/100.0 0 | 100.0/85.0 0/15.0 | 0.054 |
| Intervention Group | Difference Follow-Up/Baseline | ||||||
|---|---|---|---|---|---|---|---|
| Baseline Mean (SD) | Post-Intervention Mean (SD) | Follow-Up Mean (SD) | Mean (CI95%) | ANOVA | |||
| F | p | η2 Parcial | |||||
| EQ-VAS (T-score) | |||||||
| Experimental group | 29.1 (12.8) | 86.5 (7.1) | 78.3 (10.7) | 49.2 (42.2–56.0) * | |||
| Control group | 25.5 (5.1) | 57.0 (4.7) | 58.5 (5.9) | 33.0 (29.1–36.8) * | 75.2 | 0.000 | 0.647 |
| p | 0.241 | 0.000 | 0.000 | ||||
| EuroQoL-5 Dimensions Instrument | Baseline (n = 43) % | Post-Intervention (n = 43) % | Follow-Up (n = 43) % | ||||||
|---|---|---|---|---|---|---|---|---|---|
| CG (n) | EG (n) | p | CG (n) | EG (n) | p | CG (n) | EG (n) | p | |
| D1. Mobility | |||||||||
| (1) (2) (3) | 0 60.0 (12) 40.0 (8) | 0 21.7 (5) 78.3 (18) | 0.011 | 0 90.0 (18) 10.0 (2) | 43.5 (10) 56.5 (13) 0 | 0.002 | 0 90.0 (18) 10.0 (2) | 39.1 (9) 60.9 (14) 0 | 0.007 |
| D2. Selfcare | |||||||||
| (1) (2) (3) | 0 60.0 (12) 40.0 (8) | 0 21.7 (5) 78.3 (18) | 0.011 | 20.0 (4) 80.0 (16) 0 | 60.9 (14) 39.1 (9) 0 | 0.014 | 25.0 (5) 75.0 (15) 0 | 65.2 (15) 34.8 (8) 0 | 0.014 |
| D3. Daily activities | |||||||||
| (1) (2) (3) | 0 20.0 (4) 80.0 (16) | 0 21.7 (5) 78.3 (18) | 0.019 | 0 100.0 (20) 0 | 34.8 (8) 65.2 (15) 0 | 0.000 | 0 100.0 (20) 0 | 34.8 (8) 65.2 (15) 0 | 0.000 |
| D4. Pain/discomfort | |||||||||
| (1) (2) (3) | 50.0 (10)45.0 (9)5.0 (1) | 56.5 (13)26.2 (6)17.3 (4) | 0.562 | 0100.0 (20)0 | 78.3 (18) 21.7 (5) 0 | 0.000 | 0 95.0 (19) 5.0 (1) | 17.4 (4) 82.6 (19) 0 | 0.147 |
| D5. Anxiety/depression | |||||||||
| (1) (2) (3) | 0 85.0 (17) 15.0 (3) | 0 78.3 (18) 21.7 (5) | 0.090 | 0 100.0 (20) 0 | 91.3 (21) 8.7 (2) 0 | 0.000 | 0 65.0 (13) 35.0 (7) | 30.4 (7) 65.2 (15) 4.4 (1) | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Hernández, M.; Criado-Álvarez, J.-J.; Corregidor-Sánchez, A.-I.; Martín-Conty, J.L.; Mohedano-Moriano, A.; Polonio-López, B. Effects of Virtual Reality-Based Therapy on Quality of Life of Patients with Subacute Stroke: A Three-Month Follow-Up Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 2810. https://doi.org/10.3390/ijerph18062810
Rodríguez-Hernández M, Criado-Álvarez J-J, Corregidor-Sánchez A-I, Martín-Conty JL, Mohedano-Moriano A, Polonio-López B. Effects of Virtual Reality-Based Therapy on Quality of Life of Patients with Subacute Stroke: A Three-Month Follow-Up Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(6):2810. https://doi.org/10.3390/ijerph18062810
Chicago/Turabian StyleRodríguez-Hernández, Marta, Juan-José Criado-Álvarez, Ana-Isabel Corregidor-Sánchez, José L. Martín-Conty, Alicia Mohedano-Moriano, and Begoña Polonio-López. 2021. "Effects of Virtual Reality-Based Therapy on Quality of Life of Patients with Subacute Stroke: A Three-Month Follow-Up Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 6: 2810. https://doi.org/10.3390/ijerph18062810