
Epidemiological Characteristics of Severe Fever with Thrombocytopenia Syndrome from 2010 to 2019 in Mainland China

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection and Management
2.2. Data Analysis
3. Results
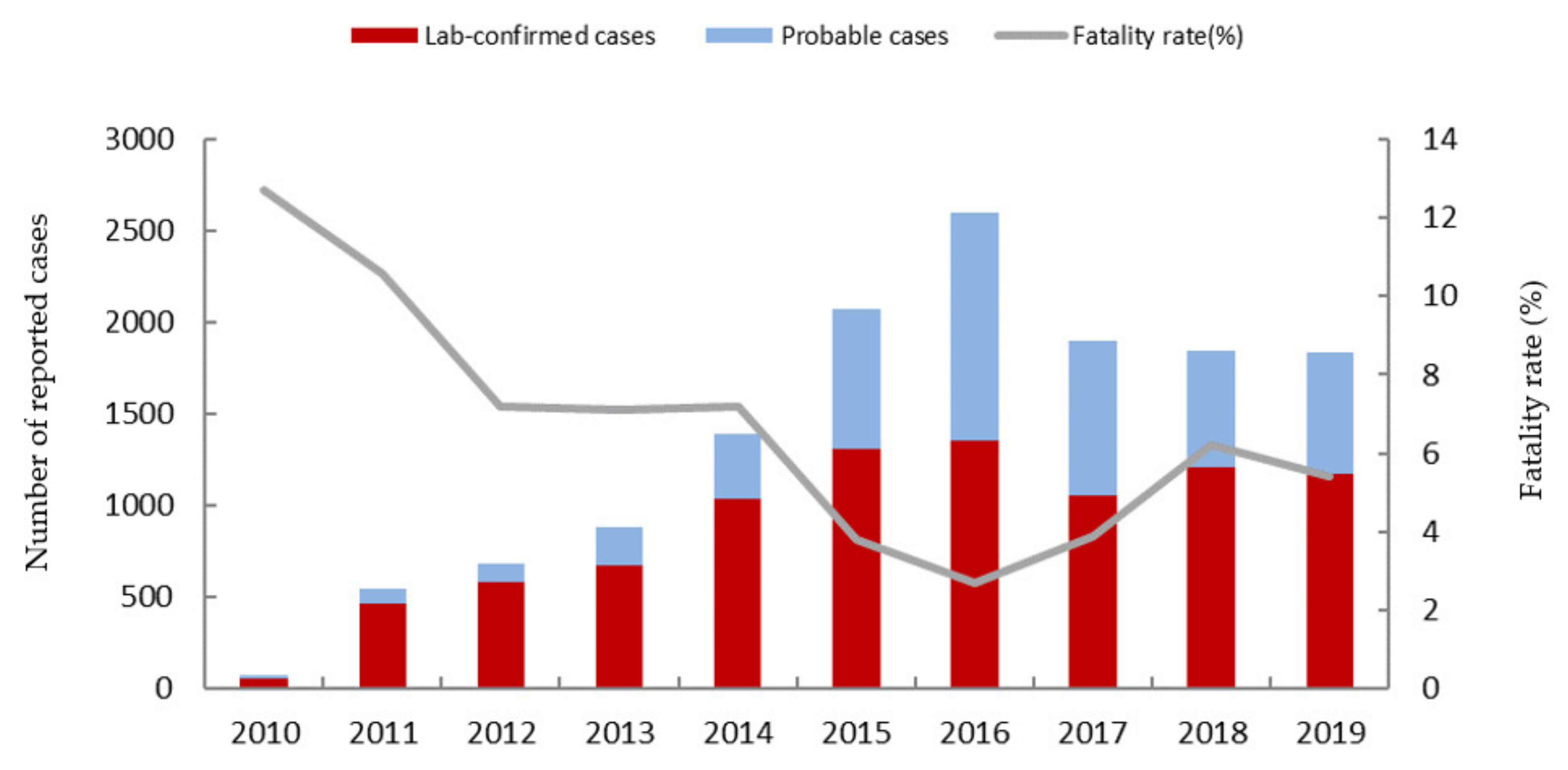
3.1. Overview of SFTS in Mainland China
3.2. Analysis of the SFTS Epidemiological Characteristics from 2010 to 2019
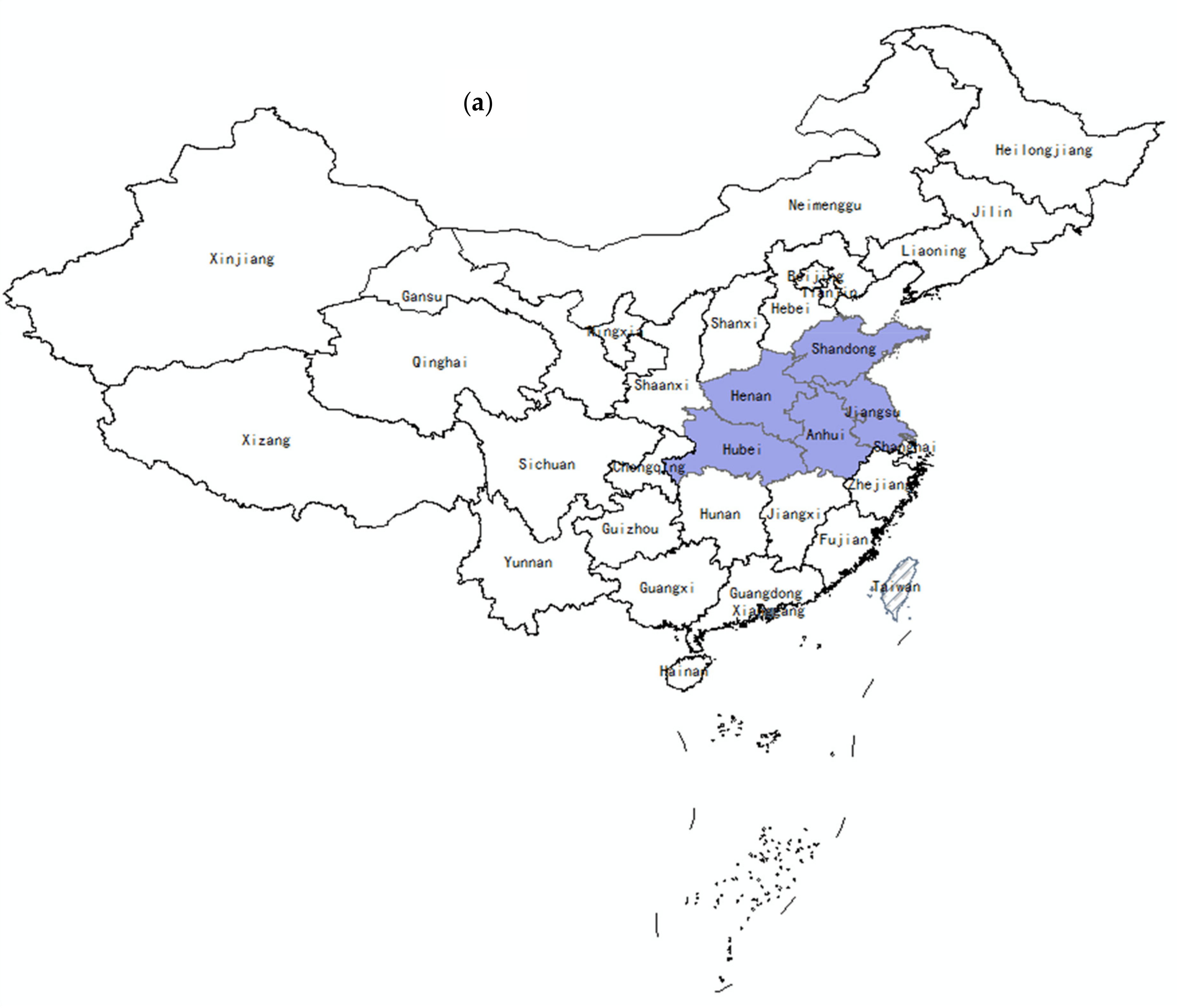
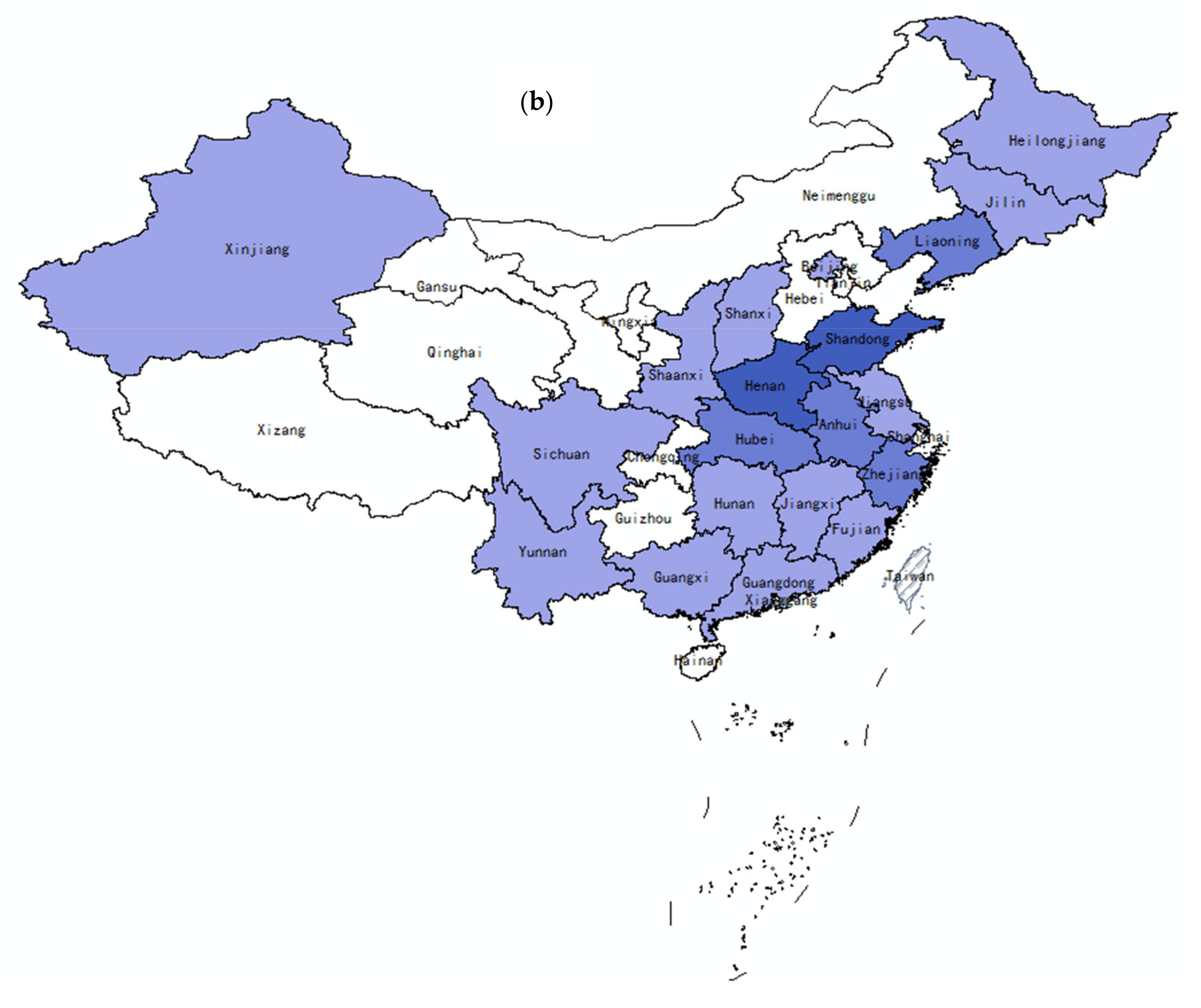
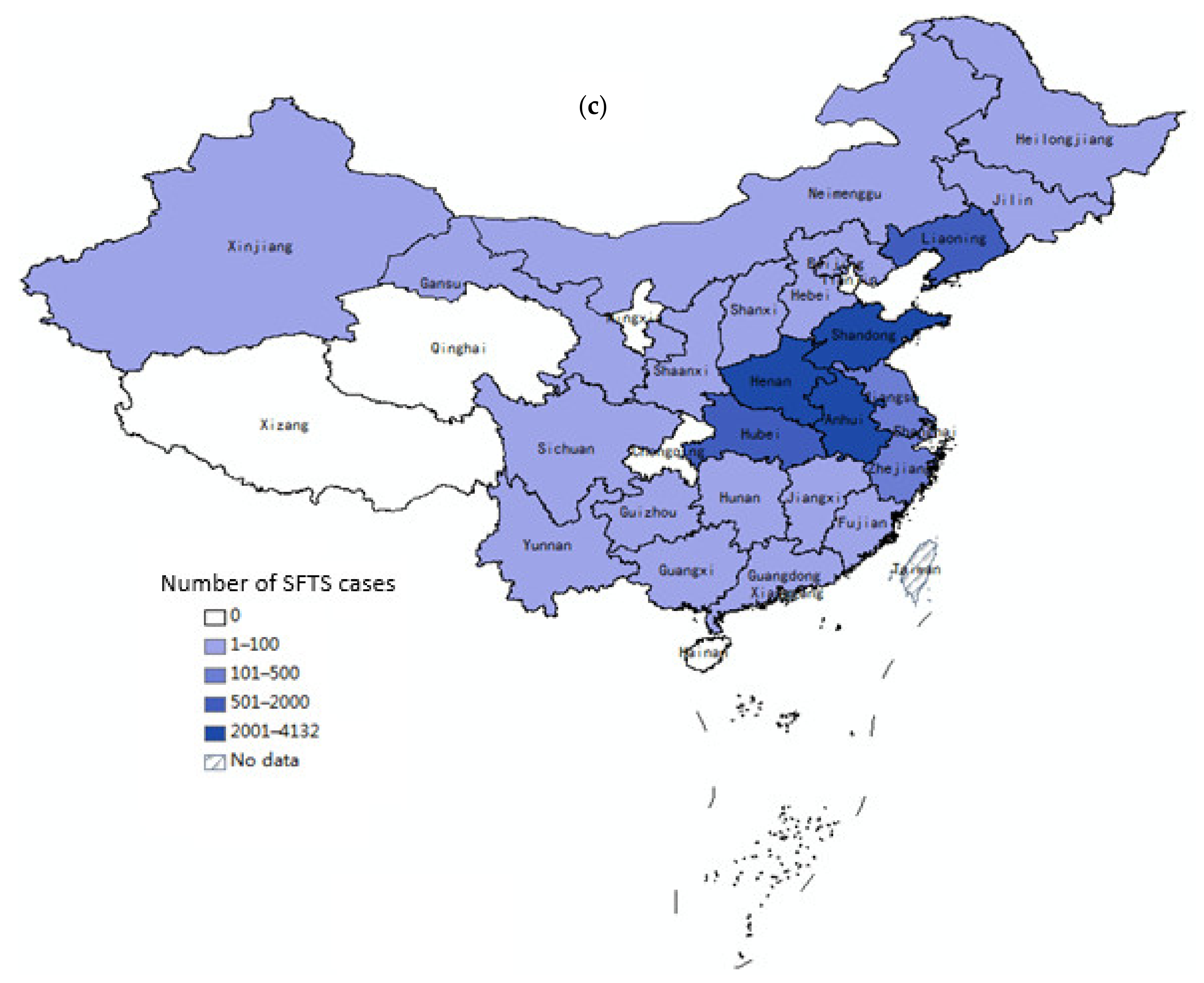
3.2.1. SFTS Regional Distribution
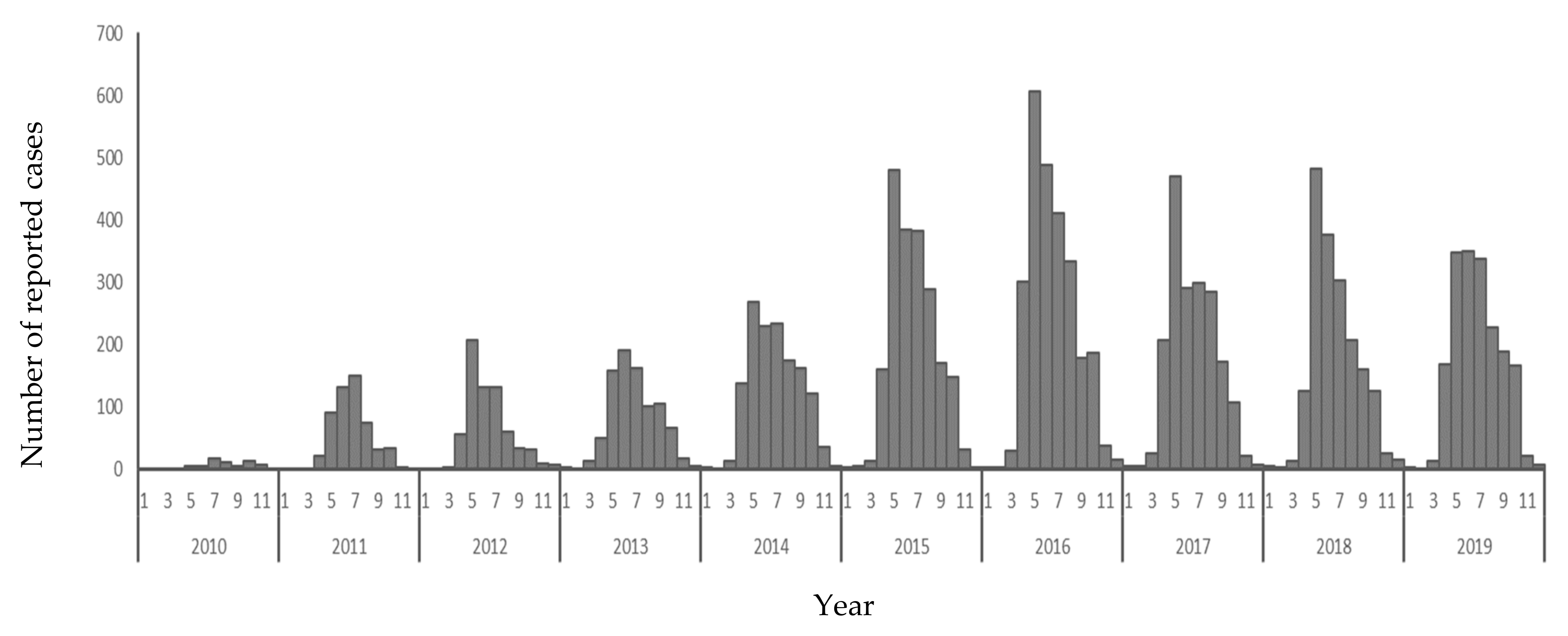
3.2.2. SFTS Temporal Distribution
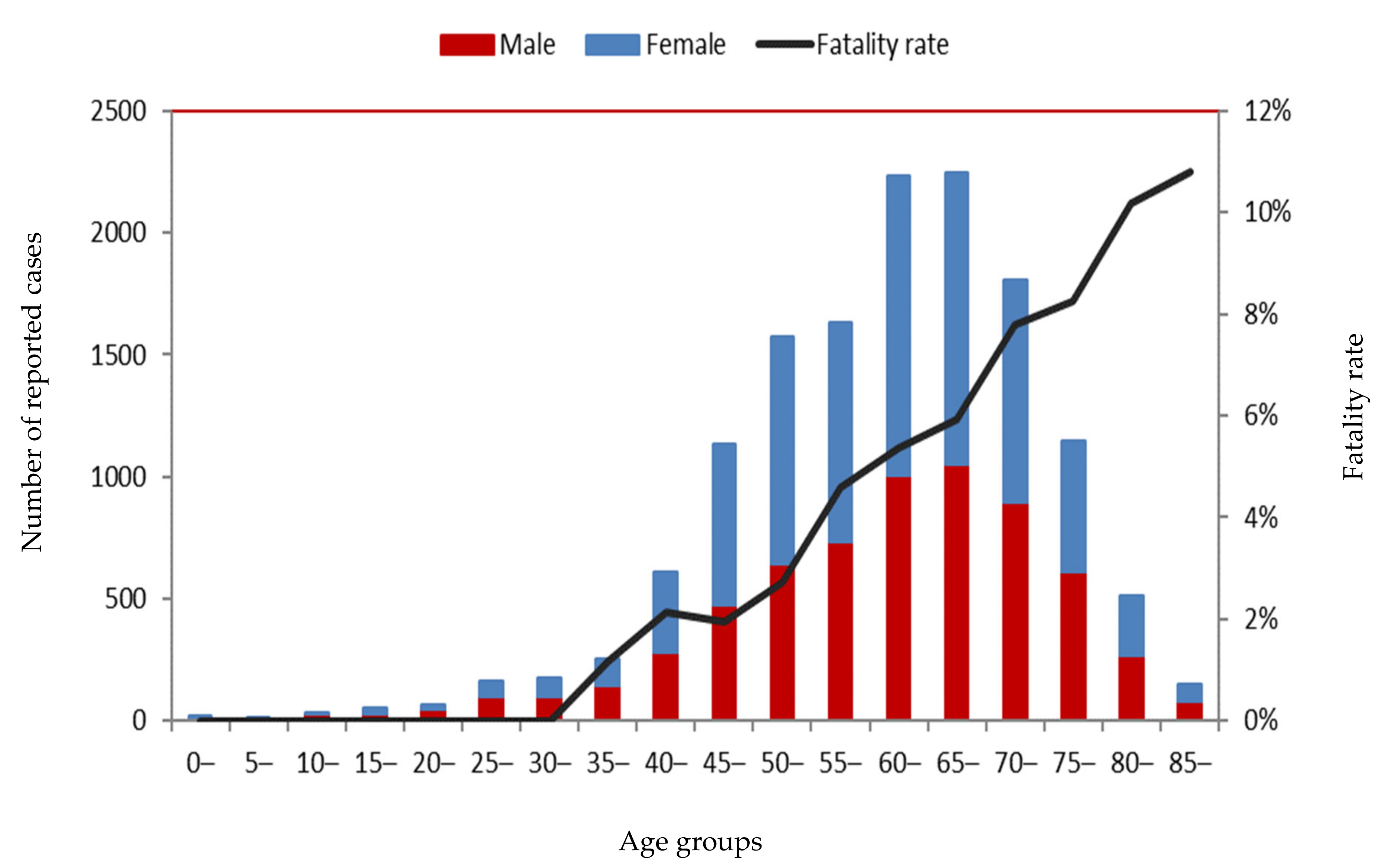
3.2.3. SFTS Population Distribution
3.3. SFTS Death Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yu, X.-J.; Liang, M.-F.; Zhang, S.-Y.; Liu, Y.; Li, J.-D.; Sun, Y.-L.; Zhang, L.; Zhang, Q.-F.; Popov, V.L.; Li, C.; et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N. Engl. J. Med. 2011, 364, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Li, D.X. Fever with thrombocytopenia associated with a Novel Bunyavirus in China. Chin. J. Exp. Clin. Virol. 2011, 25, 81–84. [Google Scholar]
- Li, D.X. Severe fever with thrombocytopenia syndrome: A newly discovered emerging infectious disease. Clin. Microbiol. Infect. 2015, 21, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y.; Liu, J.; Niu, G.; Ding, S.; Gong, L.; Liu, J. Epidemiological investigation of predominance tick and the infectious status of severe fever thrombocytopenia syndrome virus in Penglai and Laizhou counties, Shandong province. Zhonghua Yu Fang Yi Xue Za Zhi 2015, 49, 993–997. [Google Scholar] [PubMed]
- Niu, G.; Li, J.; Liang, M.; Jiang, X.; Jiang, M.; Yin, H.; Wang, Z.; Li, C.; Zhang, Q.; Jin, C.; et al. Severe fever with thrombocytopenia syndrome virus among domesticated animals, China. Emerg. Infect. Dis. 2013, 19, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, J.; Niu, G.; Wang, X.; Ding, S.; Jiang, X.; Li, C.; Zhang, Q.; Liang, M.; Bi, Z.; et al. Sfts virus in ticks in an endemic area of china. Am. J. Trop Med. Hyg. 2015, 92, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Zhang, S.; Jiang, M.; Bi, Z.; Liang, M.; Ding, S.; Wang, S.; Liu, J.; Zhou, S.; Zhang, X.; et al. A cluster of person-to-person transmission cases caused by SFTS virus in Penglai, China. Clin. Microbiol. Infect. 2015, 21, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Wu, W.; Wang, H.; Du, Y.; Liu, L.; Kang, K.; Huang, X.; Ma, H.; Mu, F.; Zhang, S.; et al. Human-to-human transmission of severe fever with thrombocytopenia syndrome bunyavirus through contact with infectious blood. J. Infect. Dis. 2013, 207, 736–739. [Google Scholar] [CrossRef] [PubMed]
- Gai, Z.; Liang, M.; Zhang, Y.; Zhang, S.; Jin, C.; Wang, S.; Sun, L.; Zhou, N.; Zhang, Q.; Sun, Y.; et al. Person-to-person transmission of severe fever with thrombocytopenia syndrome bunyavirus through blood contact. Clin. Infect. Dis. 2012, 54, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Maeda, K.; Suzuki, T.; Ishido, A.; Shigeoka, T.; Tominaga, T.; Kamei, T.; Honda, M.; Ninomiya, D.; Sakai, T.; et al. The first identification and retrospective study of severe Fever with thrombocytopenia syndrome in Japan. J. Infect. Dis. 2014, 209, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.S.; Woo, J.H. Severe fever with thrombocytopenia syndrome: Tick-mediated viral disease. J. Korean Med. Sci. 2013, 28, 795–796. [Google Scholar] [CrossRef] [PubMed]
- Tran, X.C.; Yun, Y.; Van An, L.; Kim, S.-H.; Thao, N.T.P.; Man, P.K.C.; Yoo, J.R.; Heo, S.T.; Cho, N.-H.; Lee, K.H. Endemic Severe Fever with Thrombocytopenia Syndrome, Vietnam. Emerg. Infect. Dis. 2019, 25, 1029–1031. [Google Scholar] [CrossRef] [PubMed]
- China MoH. Guideline for prevention and treatment of severe fever with thrombocytopenia syndrome (2010 version). Chin. J. Clin. Infect. Dis. 2011, 4, 193–194. [Google Scholar]
- Li, Y.; Yang, M.; Mu, D.; Chen, Q.; Yin, W. Epidemiological analysis of severe fever with thrombocytopenia syndrome from 2010 to 2017, China. Chin. J. Emerg. Resusc. Disaster Med. 2018, 3, 1076–1079. [Google Scholar]
- Huang, X.; Wang, S.; Wang, X.; Lyu, Y.; Jiang, M.; Chen, D.; Li, K.; Liu, J.; Xie, S.; Lyu, T.; et al. Estimation of the incidence of severe fever with thrombocytopenia syndrome in high endemic areas in China: An inpatient-based retrospective study. BMC Infect. Dis. 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Hu, F.; Lei, C.; Yi, J. Prevention of ticks and tick-borne diseases. Shanghai Xumu Shouyi Tongxun 2013, 50–51. [Google Scholar]
- Li, Y.; Zhou, H.; Mu, D.; Yin, W.; Yu, H. Epidemiological analysis on severe fever with thrombocytopenia syndrome under the national surveillance data from 2011 to 2014, China. Chin. J. Epidemiol. 2015, 36, 598–602. [Google Scholar]
- Liu, J.; Ma, J.; Li, A.; Wang, S.; Zheng, R.; Chen, H. Analysis of clinical characteristics and death risk factors in patients infected with severe fever with thrombocytopenia syndrome bunyavirus. Chin. J. Postgrad. Med. 2018, 41, 429–433. [Google Scholar]
- Yang, Z.; Qin, S.; Zhao, P.; Wang, R.; Tang, F.; Chen, S.; Huang, M.; Gong, L.; Fan, X.; Wang, Z.; et al. Logistic regression analysis on risk factors of fatal and severe associated with thrombocytopenia syndrome. Inter. J. Epidemiol. Infect. Dis. 2015, 42, 115–119. [Google Scholar]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, X.; Li, J.; Li, A.; Wang, S.; Li, D. Epidemiological Characteristics of Severe Fever with Thrombocytopenia Syndrome from 2010 to 2019 in Mainland China. Int. J. Environ. Res. Public Health 2021, 18, 3092. https://doi.org/10.3390/ijerph18063092
Huang X, Li J, Li A, Wang S, Li D. Epidemiological Characteristics of Severe Fever with Thrombocytopenia Syndrome from 2010 to 2019 in Mainland China. International Journal of Environmental Research and Public Health. 2021; 18(6):3092. https://doi.org/10.3390/ijerph18063092
Chicago/Turabian StyleHuang, Xiaoxia, Jiandong Li, Aqian Li, Shiwen Wang, and Dexin Li. 2021. "Epidemiological Characteristics of Severe Fever with Thrombocytopenia Syndrome from 2010 to 2019 in Mainland China" International Journal of Environmental Research and Public Health 18, no. 6: 3092. https://doi.org/10.3390/ijerph18063092
APA StyleHuang, X., Li, J., Li, A., Wang, S., & Li, D. (2021). Epidemiological Characteristics of Severe Fever with Thrombocytopenia Syndrome from 2010 to 2019 in Mainland China. International Journal of Environmental Research and Public Health, 18(6), 3092. https://doi.org/10.3390/ijerph18063092