
COVID-19 and Health-Related Quality of Life: A Community-Based Online Survey in Hong Kong

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
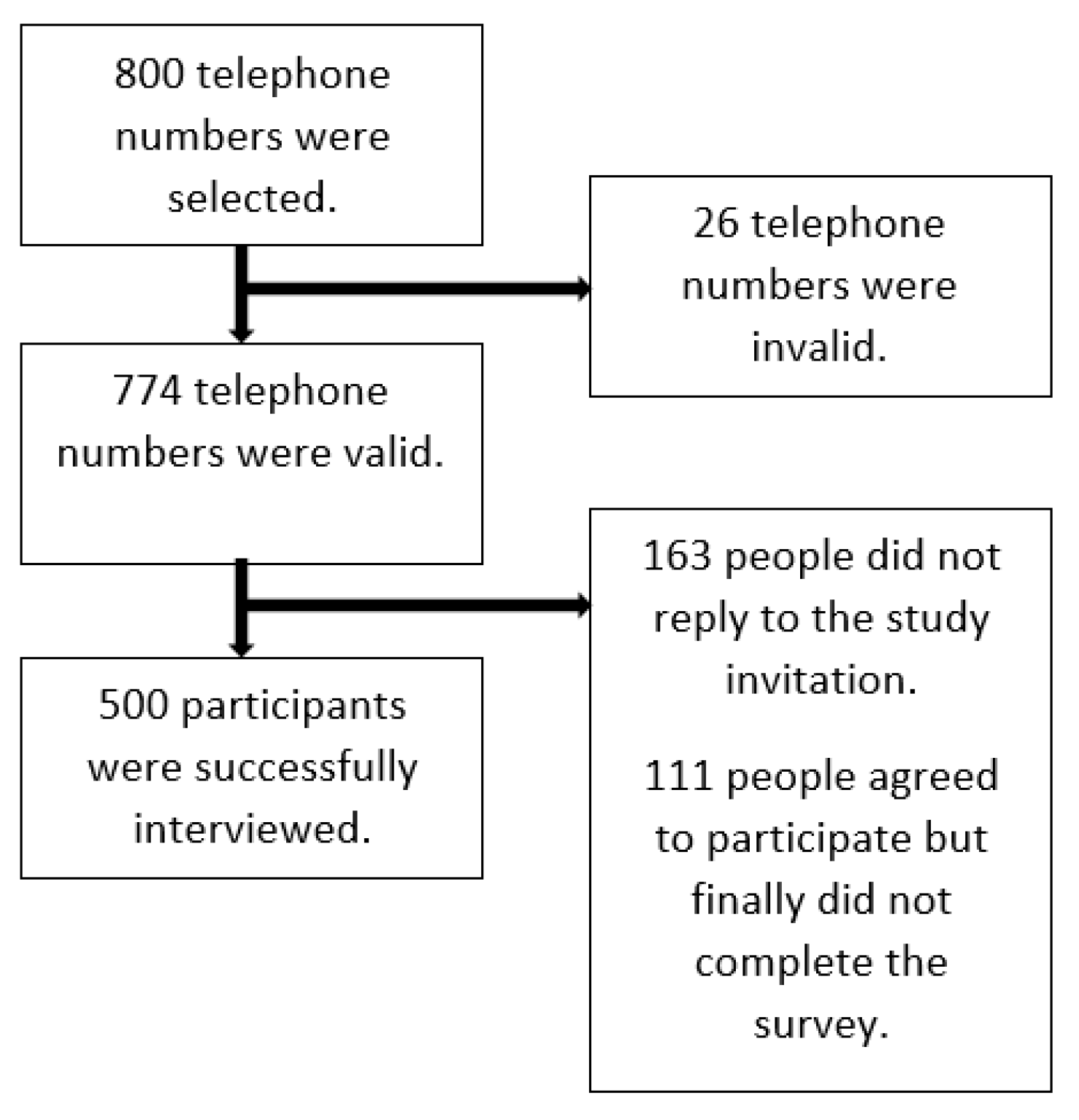
2.2. Setting and Participants
2.3. Study Instruments
- (i)
- I feel worried that I will be infected with COVID-19;
- (ii)
- I feel worried that my family members will be infected with COVID-19;
- (iii)
- I feel bothered because I often suspect that I have COVID-19 symptoms;
- (iv)
- I feel bothered because I do not have enough surgical masks;
- (v)
- I feel bothered because I do not have enough disinfectant supplies at home;
- (vi)
- I feel worried that I may lose my job because of COVID-19.
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Sample Characteristics
3.2. Impact of COVID-19
3.3. HRQOL Scores
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Cucinotta, D.; Vanelli, M. Who Declares Covid-19 a Pandemic? Acta Bio Med. Atenei Parm. 2020, 91, 157–160. [Google Scholar]
- Johns Hopkins University. Covid-19 Dashboard. Available online: https://coronavirus.jhu.edu/map.html (accessed on 15 July 2020).
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and anxiety in hong kong during covid-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.; Tsang, T.K.; Li, J.C.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Law, S.; Leung, A.W.; Xu, C. Severe acute respiratory syndrome (SARS) and coronavirus disease-2019 (COVID-19): From causes to preventions in hong kong. Int. J. Infect. Dis. 2020, 94, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.K.; Chan, H.H.; Yi, Y.Y.; Tang, A.; Wei, W.I.; Wong, S.Y. Community responses during early phase of covid-19 epidemic, hong kong. Emerg. Infect. Dis. 2020, 26, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ma, Z.F. Impact of the covid-19 pandemic on mental health and quality of life among local residents in liaoning province, china: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef] [Green Version]
- Bakas, T.; McLennon, S.M.; Carpenter, J.S.; Buelow, J.M.; Otte, J.L.; Hanna, K.M.; Ellett, M.L.; Hadler, K.A.; Welch, J.L. Systematic review of health-related quality of life models. Health Qual. Life Outcomes 2012, 10, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Haas, B.K. A multidisciplinary concept analysis of quality of life. West. J. Nurs. Res. 1999, 21, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Ul-Haq, Z.; Mackay, D.F.; Pell, J.P. Association between physical and mental health-related quality of life and adverse outcomes; a retrospective cohort study of 5272 scottish adults. BMC Public Health 2014, 14, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otero-Rodríguez, A.; León-Muñoz, L.M.; Balboa-Castillo, T.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Change in health-related quality of life as a predictor of mortality in the older adults. Qual. Life Res. 2010, 19, 15–23. [Google Scholar] [CrossRef]
- Bjorner, J.B.; Wallenstein, G.V.; Martin, M.C.; Lin, P.; Blaisdell-Gross, B.; Tak Piech, C.; Mody, S.H. Interpreting score differences in the sf-36 vitality scale: Using clinical conditions and functional outcomes to define the minimally important difference. Curr. Med. Res. Opin. 2007, 23, 731–739. [Google Scholar] [CrossRef]
- Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian J. Psychiatry 2020, 51, 102073. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and psychometric evaluation of the italian version of the fear of COVID-19 scale. Int. J. Ment. Health Addict. 2020, 1–10. [Google Scholar] [CrossRef]
- Gómez-Salgado, J.; Andrés-Villas, M.; Domínguez-Salas, S.; Díaz-Milanés, D.; Ruiz-Frutos, C. Related health factors of psychological distress during the COVID-19 pandemic in spain. Int. J. Environ. Res. Public Health 2020, 17, 3947. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Diseas; Cambridge Scholars Publishing: Newcastle upon Tyne, UK, 2019. [Google Scholar]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacioppo, J.T.; Cacioppo, S.; Capitanio, J.P.; Cole, S.W. The neuroendocrinology of social isolation. Annu. Rev. Psychol. 2015, 66, 733–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, T.; Danese, A.; Wertz, J.; Odgers, C.L.; Ambler, A.; Moffitt, T.E.; Arseneault, L. Social isolation, loneliness and depression in young adulthood: A behavioural genetic analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Shankar, A.; Hamer, M.; McMunn, A.; Steptoe, A. Social isolation and loneliness: Relationships with cognitive function during 4 years of follow-up in the english longitudinal study of ageing. Psychosomat. Med. 2013, 75, 161–170. [Google Scholar] [CrossRef]
- Fernandes, N. Economic Effects of Coronavirus Outbreak (COVID-19) on the World Economy. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3557504 (accessed on 15 July 2020).
- Davalos, M.E.; French, M.T. This recession is wearing me out! Health-related quality of life and economic downturns. J. Ment. Health Policy Econ. 2011, 14, 61–72. [Google Scholar] [PubMed]
- Leung, G.; Ho, L.; Lam, T.; Hedley, A. Epidemiology of sars in the 2003 Hong Kong epidemic. Hong Kong Med. J. 2009, 15, 12–16. [Google Scholar] [PubMed]
- Algahtani, F.D.; Hassan, S.-u.-N.; Alsaif, B.; Zrieq, R. Assessment of the quality of life during COVID-19 pandemic: A cross-sectional survey from the kingdom of saudi arabia. Int. J. Environ. Res. Public Health 2021, 18, 847. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Group, W. Development of the world health organization whoqol-bref quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Gholami, A.; Jahromi, L.M.; Zarei, E.; Dehghan, A. Application of whoqol-bref in measuring quality of life in health-care staff. Int. J. Prev. Med. 2013, 4, 809. [Google Scholar]
- Choi, E.P.; Wong, J.Y.; Fong, D.Y. Mental health and health-related quality of life of chinese college students who were the victims of dating violence. Qual. Life Res. 2017, 26, 945–957. [Google Scholar] [CrossRef]
- Chew, B.-H.; Mohd-Sidik, S.; Shariff-Ghazali, S. Negative effects of diabetes–related distress on health-related quality of life: An evaluation among the adult patients with type 2 diabetes mellitus in three primary healthcare clinics in malaysia. Health Qual. Life Outcomes 2015, 13, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, K.; Wong, W.; Tay, M.; Chu, M.; Ng, S. Development and validation of the interview version of the hong kong chinese whoqol-bref. Qual. Life Res. 2005, 14, 1413–1419. [Google Scholar] [CrossRef] [PubMed]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and anovas. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Heymann, D.L. Data sharing and outbreaks: Best practice exemplified. Lancet 2020, 395, 469–470. [Google Scholar] [CrossRef] [Green Version]
- Kowalski, K.C.; Crocker, P.R. Development and validation of the coping function questionnaire for adolescents in sport. J. Sport Exerc. Psychol. 2001, 23, 136–155. [Google Scholar] [CrossRef] [Green Version]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The impact of stress on body function: A review. EXCLI J. 2017, 16, 1057. [Google Scholar]
- Cohen, S.; Janicki-Deverts, D.; Miller, G.E. Psychological stress and disease. JAMA 2007, 298, 1685–1687. [Google Scholar] [CrossRef] [PubMed]
- Porges, S.W. Cardiac vagal tone: A physiological index of stress. Neurosci. Biobehav. Rev. 1995, 19, 225–233. [Google Scholar] [CrossRef]
- Pressman, S.D.; Cohen, S.; Miller, G.E.; Barkin, A.; Rabin, B.S.; Treanor, J.J. Loneliness, social network size, and immune response to influenza vaccination in college freshmen. Health Psychol. 2005, 24, 297. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C. Clinical characteristics of COVID-19 patients with digestive symptoms in hubei, china: A descriptive, cross-sectional, multicenter study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef]
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Barsky, A.J.; Wyshak, G.; Klerman, G.L. The somatosensory amplification scale and its relationship to hypochondriasis. J. Psychiatr. Res. 1990, 24, 323–334. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in china. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Rief, W.; Broadbent, E. Explaining medically unexplained symptoms-models and mechanisms. Clin. Psychol. Rev. 2007, 27, 821–841. [Google Scholar] [CrossRef]
- Cuan-Baltazar, J.Y.; Muñoz-Perez, M.J.; Robledo-Vega, C.; Pérez-Zepeda, M.F.; Soto-Vega, E. Misinformation of COVID-19 on the internet: Infodemiology study. JMIR Public Health Surveill. 2020, 6, e18444. [Google Scholar] [CrossRef] [Green Version]
- Hernández-García, I.; Giménez-Júlvez, T. Assessment of health information about covid-19 prevention on the internet: Infodemiological study. JMIR Public Health Surveill. 2020, 6, e18717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 0020764020915212. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- Census and Statistics Department The HKSAR. Labour Force. Available online: https://www.censtatd.gov.hk/hkstat/sub/sp200.jsp?tableID=006&ID=0&productType=8 (accessed on 15 July 2020).
- Caroli, E.; Godard, M. Does job insecurity deteriorate health? Health Econ. 2016, 25, 131–147. [Google Scholar] [CrossRef] [Green Version]
- Bünnings, C.; Kleibrink, J.; Weßling, J. Fear of unemployment and its effect on the mental health of spouses. Health Econ. 2017, 26, 104–117. [Google Scholar] [CrossRef] [PubMed]
- McDonough, P. Job insecurity and health. Int. J. Health Serv. 2000, 30, 453–476. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Mean Age (SD) | 47.26 (15.82) |
| n (%) | |
| Gender | |
| Male | 226 (45.20) |
| Female | 274 (54.80) |
| Marital status | |
| Not currently married | 164 (32.80) |
| Currently married | 336 (67.20) |
| Education status | |
| Below bachelor’s degree | 341 (68.20) |
| Bachelor’s degree or above | 159 (31.80) |
| Employment status | |
| Having a full-time job | 281 (56.20) |
| Having a part-time job | 39 (7.80) |
| Students | 22 (4.40) |
| Homemakers | 65 (13.00) |
| Retirement | 64 (12.80) |
| Current not working | 29 (5.80) |
| Monthly personal income | |
| HKD$ 20,000 or below | 339 (67.80) |
| HKD$ 20,001 or above | 161 (32.20) |
| The impacts of COVID-19 ^ | |
| (i) I feel worried that I will be infected with COVID-19. | 348 (69.60) |
| (ii) I feel worried that my family members will be infected with COVID-19. | 371 (74.20) |
| (iii) I feel bothered because I often suspect that I have COVID-19 symptoms. | 207 (41.40) |
| (iv) I feel bothered because I do not have enough surgical masks. | 197 (39.40) |
| (v) I feel bothered because I do not have enough disinfectant supplies at home. | 145 (29.00) |
| (vi) I feel worried that I may lose my job because of COVID-19. | 237 (47.40) |
| Mean HRQOL scores (SD) * | |
| Physical health | 68.09 (15.16) |
| Psychological health | 59.40 (14.95) |
| Social relationships | 62.37 (14.20) |
| Environment | 56.88 (14.20) |
| Physical Health | Psychological Health | |||||
| No | Yes | No | Yes | |||
| Mean (SD) | Mean (SD) | Effect Size 🟂 | Mean (SD) | Mean (SD) | Effect Size 🟂 | |
| (i) I feel worried that I will be infected with COVID-19. ^ | 72.70 (14.39) | 66.07 (15.06) ** | 0.45 | 62.36 (14.95) | 58.11 (14.79) ** | 0.29 |
| (ii) I feel worried that my family members will be infected with COVID-19. ^ | 71.46 (13.81) | 66.91 (15.44) ** | 0.31 | 61.11 (15.07) | 58.81 (14.88) | 0.15 |
| (iii) I feel bothered because I often suspect that I have COVID-19 symptoms. ^ | 72.77 (13.52) | 61.46 (14.91) ** | 0.79 | 62.57 (14.99) | 54.91 (13.72) ** | 0.53 |
| (iv) I feel bothered because I do not have enough surgical masks. ^ | 71.25 (14.93) | 63.22 (14.22) ** | 0.55 | 61.58 (15.78) | 56.05 (12.91) ** | 0.38 |
| (v) I feel bothered because I do not have enough disinfectant supplies at home. ^ | 71.34 (14.74) | 60.12 (13.12) ** | 0.80 | 61.61 (15.27) | 53.99 (12.65) ** | 0.54 |
| (vi) I feel worried that I may lose my job because of COVID-19. ^ | 69.09 (15.83) | 66.97 (14.32) | 0.14 | 62.21 (14.82) | 56.28 (14.50) ** | 0.40 |
| Social Relationships | Environment | |||||
| No | Yes | No | Yes | |||
| Mean (SD) | Mean (SD) | Effect Size 🟂 | Mean (SD) | Mean (SD) | Effect Size 🟂 | |
| (i) I feel worried that I will be infected with COVID-19. ^ | 65.52 (12.83) | 60.99 (14.56) ** | 0.33 | 61.10 (13.45) | 55.04 (14.14) ** | 0.44 |
| (ii) I feel worried that my family members will be infected with COVID-19. ^ | 63.89 (14.37) | 61.84 (14.12) | 14.39 | 58.45 (13.83) | 56.33 (14.30) | 0.15 |
| (iii) I feel bothered because I often suspect that I have COVID-19 symptoms. ^ | 63.65 (14.50) | 60.55 (13.60) * | 0.22 | 59.35 (14.87) | 53.38 (12.39) ** | 0.44 |
| (iv) I feel bothered because I do not have enough surgical masks. ^ | 63.17 (14.62) | 61.13 (13.47) | 0.15 | 58.82 (15.45) | 53.90 (11.42) ** | 0.36 |
| (v) I feel bothered because I do not have enough disinfectant supplies at home. ^ | 63.33 (14.33) | 60.00 (13.63) * | 0.24 | 58.42 (15.03) | 53.13 (11.07) ** | 0.40 |
| (vi) I feel worried that I may lose my job because of COVID-19. ^ | 62.99 (13.51) | 61.67 (14.92) | 0.09 | 59.01 (14.20) | 54.52 (13.84) ** | 0.32 |
| Physical Health | Psychological Health | Social Relationships | Environment | |
|---|---|---|---|---|
| β | β | β | β | |
| (i) I feel worried that I will be infected with COVID-19. (ref: no) | −7.42 ** | −5.18 ** | −5.46 ** | −6.88 ** |
| (ii) I feel worried that my family members will be infected with COVID-19. (ref: no) | −4.78 ** | −2.88 | −2.71 | −2.73 |
| (iii) I feel bothered because I often suspect that I have COVID-19 symptoms. (ref: no) | −11.20 ** | −7.74 ** | −3.24 * | −6.00 ** |
| (iv) I feel bothered because I do not have enough surgical masks. (ref: no) | −7.92 ** | −5.88 ** | −2.41 | −5.20 ** |
| (v) I feel bothered because I do not have enough disinfectant supplies at home. (ref: no) | −10.55 ** | −7.58 ** | −3.31 * | −5.27 ** |
| (vi) I feel worried that I may lose my job because of COVID-19. (ref: no) | −4.67 ** | −7.34 ** | −2.14 | −4.97 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F.; Kwok, J.Y.Y.; Tam, T.H.L.; Wu, C. COVID-19 and Health-Related Quality of Life: A Community-Based Online Survey in Hong Kong. Int. J. Environ. Res. Public Health 2021, 18, 3228. https://doi.org/10.3390/ijerph18063228
Choi EPH, Hui BPH, Wan EYF, Kwok JYY, Tam THL, Wu C. COVID-19 and Health-Related Quality of Life: A Community-Based Online Survey in Hong Kong. International Journal of Environmental Research and Public Health. 2021; 18(6):3228. https://doi.org/10.3390/ijerph18063228
Chicago/Turabian StyleChoi, Edmond Pui Hang, Bryant Pui Hung Hui, Eric Yuk Fai Wan, Jojo Yan Yan Kwok, Tiffany Hei Lam Tam, and Chanchan Wu. 2021. "COVID-19 and Health-Related Quality of Life: A Community-Based Online Survey in Hong Kong" International Journal of Environmental Research and Public Health 18, no. 6: 3228. https://doi.org/10.3390/ijerph18063228
APA StyleChoi, E. P. H., Hui, B. P. H., Wan, E. Y. F., Kwok, J. Y. Y., Tam, T. H. L., & Wu, C. (2021). COVID-19 and Health-Related Quality of Life: A Community-Based Online Survey in Hong Kong. International Journal of Environmental Research and Public Health, 18(6), 3228. https://doi.org/10.3390/ijerph18063228