
Pain in Multiple Sites and Clusters of Cause-Specific Work Disability Development among Midlife Municipal Employees

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Ethics
2.3. Measures: Diagnostic Specific Work Disability
2.4. Predictors: Pain in Multiple Sites
2.5. Other Predictors
2.6. Statistical Analysis
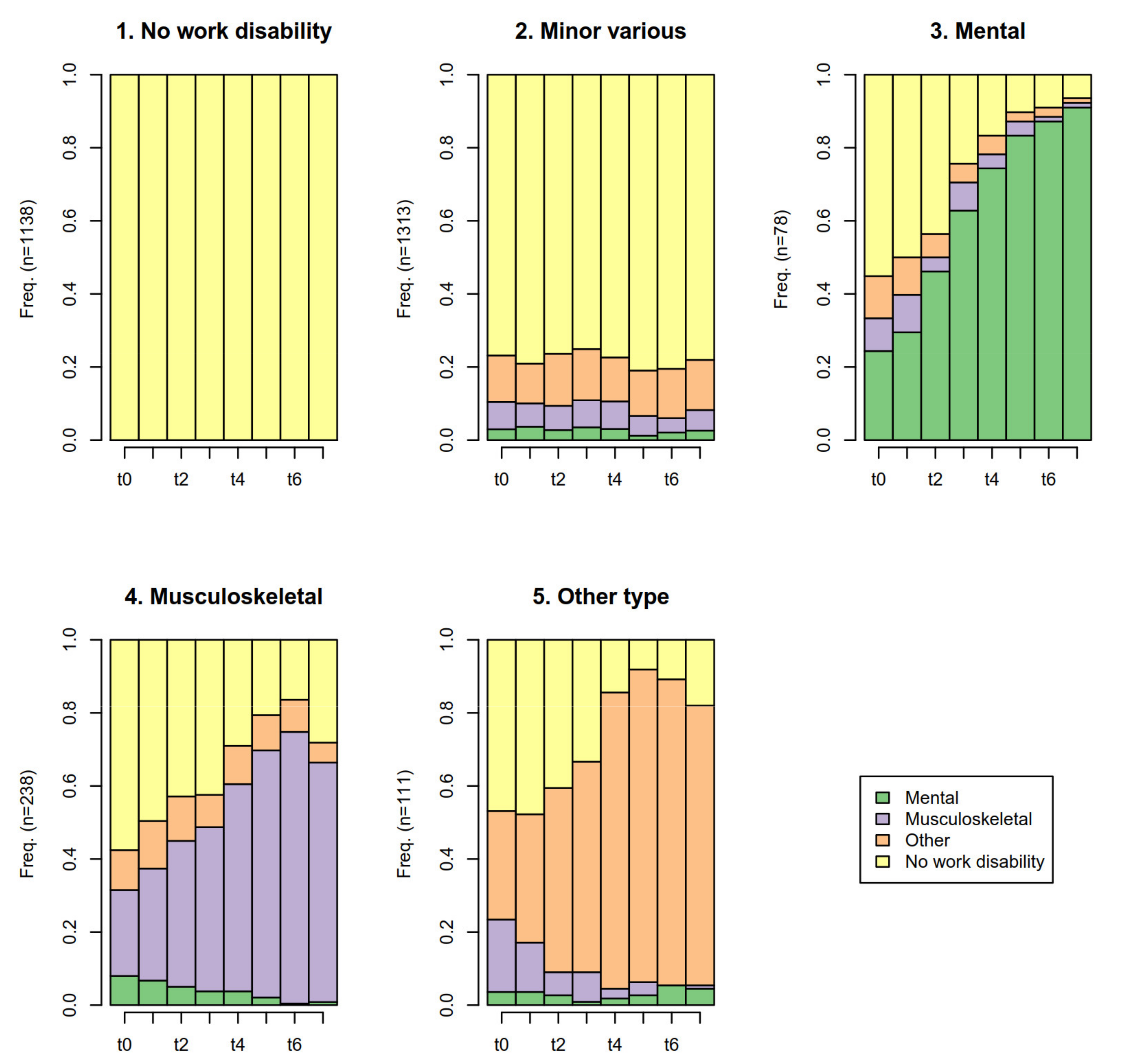
3. Results
4. Discussion
Methodological Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haukka, E.; Kaila-Kangas, L.; Ojajärvi, A.; Saastamoinen, P.; Holtermann, A.; Jørgensen, M.B.; Karppinen, J.; Heliövaara, M.; Leino-Arjas, P. Multisite musculoskeletal pain predicts medically certified disability retirement among Finns. Eur. J. Pain 2015, 19, 1119–1128. [Google Scholar] [CrossRef]
- Øverland, S.; Harvey, S.B.; Knudsen, A.K.; Mykletun, A.; Hotopf, M. Widespread pain and medically certified disability pension in the Hordaland Health Study. Eur. J. Pain 2012, 16, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Ropponen, A.; Narusyte, J.; Mittendorfer-Rutz, E.; Svedberg, P. Number of Pain Locations as a Predictor of Cause-Specific Disability Pension in Sweden-Do Common Mental Disorders Play a Role? J. Occup. Environ. Med. 2019, 61, 646–652. [Google Scholar] [CrossRef]
- Finnish Centre for Pensions. Statistical Yearbook of Pensioners in Finland 2016; Finnish Centre for Pensions: Helsinki, Finland, 2017. [Google Scholar]
- Mose, S.; Christiansen, D.H.; Jensen, J.J.; Andersen, J.H. Widespread pain–do pain intensity and care-seeking influence sickness absence?—A population-based cohort study. BMC Musculoskelet. Disord. 2016, 17, 197. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.D.C.P.; Burdorf, A. Erratum to: Associations of multisite pain with healthcare utilization, sickness absence and restrictions at work. Int. Arch. Occup. Environ. Health 2016, 89, 1047. [Google Scholar] [CrossRef] [PubMed]
- Eckhoff, C.; Straume, B.; Kvernmo, S. Multisite musculoskeletal pain in adolescence as a predictor of medical and social welfare benefits in young adulthood: The Norwegian Arctic Adolescent Health Cohort Study. Eur. J. Pain 2017, 21, 1697–1706. [Google Scholar] [CrossRef]
- Kamaleri, Y.; Natvig, B.; Ihlebaek, C.M.; Bruusgaard, D. Does the number of musculoskeletal pain sites predict work disability? A 14-year prospective study. Eur. J. Pain 2009, 13, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Piccarreta, R.; Studer, M. Holistic analysis of the life course: Methodological challenges and new perspectives. Adv. Life Course Res. 2019, 41, 100251. [Google Scholar] [CrossRef]
- Madsen, A. Årnes Return to work after first incidence of long-term sickness absence: A 10-year prospective follow-up study identifying labour-market trajectories using sequence analysis. Scand. J. Public Health 2019, 48, 134–143. [Google Scholar] [CrossRef] [PubMed]
- McLeod, C.B.; Reiff, E.; Maas, E.; Bültmann, U. Identifying return-to-work trajectories using sequence analysis in a cohort of workers with work-related musculoskeletal disorders. Scand. J. Work. Environ. Health 2018, 44, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Pirkola, S.; Nevalainen, J.; Laaksonen, M.; Fröjd, S.; Nurmela, K.; Näppilä, T.; Tuulio-Henriksson, A.; Autio, R.; Blomgren, J. The importance of clinical and labour market histories in psychiatric disability retirement: Analysis of the comprehensive Finnish national-level RETIRE data. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Lallukka, T.; Hiilamo, A.; Oakman, J.; Mänty, M.; Pietiläinen, O.; Rahkonen, O.; Kouvonen, A.; Halonen, J.I. Recurrent pain and work disability: A record linkage study. Int. Arch. Occup. Environ. Health 2019, 93, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Lahelma, E.; Aittomäki, A.; Laaksonen, M.; Lallukka, T.; Martikainen, P.; Piha, K.; Rahkonen, O.; Saastamoinen, P. Cohort Profile: The Helsinki Health Study. Int. J. Epidemiol. 2013, 42, 722–730. [Google Scholar] [CrossRef]
- Haukka, E.; Kaila-Kangas, L.; Ojajärvi, A.; Miranda, H.; Karppinen, J.; Viikari-Juntura, E.; Heliövaara, M.; Leino-Arjas, P. Pain in multiple sites and sickness absence trajectories: A prospective study among Finns. Pain 2013, 154, 306–312. [Google Scholar] [CrossRef]
- Goldberg, D.P. The Detection of Psychiatric Illness by Questionnaire. Maudsley Monograph; Oxford University Press: London, UK, 1972. [Google Scholar]
- Lahelma, E.; Pietiläinen, O.; Rahkonen, O.; Lallukka, T. Common mental disorders and cause-specific disability retirement. Occup. Environ. Med. 2014, 72, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Studer, M. WeightedCluster Library Manual: A Practical Guide to Creating Typologies of Trajectories in the Social Sciences with R; University of Geneva, Institute for Demographic and Life Course Studies: Geneva, Switzerland, 2013. [Google Scholar]
- Elzinga, C.H. Sequence Analysis: Metric Representations of Categorical Time Series. Sociological Methods and Research. 2006. Available online: https://www.researchgate.net/profile/Cees-Elzinga/publication/228982046_Sequence_analysis_Metric_representations_of_categorical_time_series/links/5464a15e0cf2c0c6aec64294/Sequence-analysis-Metric-representations-of-categorical-time-series.pdf (accessed on 21 February 2021).
- Ward, J.H., Jr. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Gabadinho, A.; Ritschard, G.; Mueller, N.S.; Studer, M. Analyzing and visualizing state sequences in R with TraMineR. J. Stat. Softw. 2011, 40, 1–37. [Google Scholar] [CrossRef]
- Virtanen, M.; Ervasti, J.; Head, J.; Oksanen, T.; Salo, P.; Pentti, J.; Kouvonen, A.; Väänänen, A.; Suominen, S.; Koskenvuo, M.; et al. Lifestyle factors and risk of sickness absence from work: A multicohort study. Lancet Public Health 2018, 3, e545–e554. [Google Scholar] [CrossRef]
- Melchior, M.; Krieger, N.; Kawachi, I.; Berkman, L.F.; Niedhammer, I.; Goldberg, M. Work Factors and Occupational Class Disparities in Sickness Absence: Findings From the GAZEL Cohort Study. Am. J. Public Health 2005, 95, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Polvinen, A.; Laaksonen, M.; Gould, R.; Lahelma, E.; Martikainen, P. The contribution of major diagnostic causes to socioeconomic differences in disability retirement. Scand. J. Work. Environ. Health 2013, 40, 353–360. [Google Scholar] [CrossRef]
- Croft, P.; Blyth, F.M.; Van Der Windt, D. Chronic pain as a topic for epidemiology and public health. In Chronic Pain Epidemiology; Oxford University Press (OUP): London, UK, 2010. [Google Scholar]
- Oakman, J.; Keegel, T.; Kinsman, N.; Briggs, A.M. Persistent musculoskeletal pain and productive employment; a systematic review of interventions. Occup. Environ. Med. 2016, 73, 206–214. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Work Disability Clusters | ||||||
|---|---|---|---|---|---|---|
| N | 1. No Work Disability | 2. Minor Various | 3. Mental | 4. Musculoskeletal | 5. Other Type | |
| Row N/% | Row N/% | Row N/% | Row N/% | Row N/% | ||
| N | 2878 | 1138 | 1313 | 78 | 238 | 111 |
| Total | - | 40 | 46 | 3 | 8 | 4 |
| Gender | ||||||
| Men | 510 | 45 | 45 | 2 | 4 | 4 |
| Women | 2368 | 38 | 46 | 3 | 9 | 4 |
| Age group | ||||||
| 45–49 | 947 | 44 | 45 | 2 | 7 | 3 |
| 50–54 | 1023 | 37 | 47 | 3 | 8 | 4 |
| 55–57 | 908 | 37 | 45 | 3 | 10 | 4 |
| Occupational class | ||||||
| Managers or professionals | 915 | 51 | 42 | 2 | 3 | 2 |
| Semi-professionals | 693 | 42 | 46 | 4 | 5 | 3 |
| Routine non-manual workers | 903 | 31 | 48 | 3 | 14 | 4 |
| Manual workers | 316 | 26 | 49 | 3 | 14 | 8 |
| Missing | 51 | 33 | 53 | 2 | 6 | 6 |
| Work Disability Clusters | ||||||
|---|---|---|---|---|---|---|
| 1. No Work Disability | 2. Minor Various | 3. Mental | 4. Musculoskeletal | 5. Other Type | Chi2 | |
| Col % | Col % | Col % | Col % | Col % | p-value | |
| Number of pain locations | ||||||
| No pain | 67 | 54 | 47 | 29 | 36 | |
| Single location pain | 15 | 19 | 14 | 21 | 20 | <0.001 |
| 2 locations | 9 | 13 | 6 | 22 | 20 | |
| 3–7 locations | 7 | 12 | 31 | 26 | 23 | |
| Pain locations | ||||||
| Pain in head or face | 4 | 5 | 13 | 9 | 13 | <0.001 |
| Pain in neck or shoulder | 17 | 25 | 35 | 41 | 37 | <0.001 |
| Pain in low back | 12 | 17 | 35 | 34 | 25 | <0.001 |
| Pain in upper limbs | 10 | 16 | 19 | 24 | 25 | <0.001 |
| Pain in lower limbs | 11 | 18 | 26 | 39 | 31 | <0.001 |
| Pain in stomach location | 3 | 5 | 9 | 5 | 7 | 0.018 |
| Pain in some other location | 2 | 4 | 4 | 8 | 12 | <0.001 |
| Mentally strenuous working environment | 11 | 13 | 27 | 13 | 19 | 0.003 |
| Physically strenuous working environment | 23 | 29 | 27 | 55 | 42 | <0.001 |
| Smoking | ||||||
| No | 64 | 56 | 58 | 47 | 41 | |
| Past smoking | 22 | 23 | 19 | 22 | 21 | <0.001 |
| Smoking | 13 | 21 | 23 | 30 | 36 | |
| Binge drinking | ||||||
| Binge drinking (once a month or more) | 23 | 28 | 22 | 24 | 33 | <0.001 |
| Obesity | ||||||
| Healthy weight | 55 | 47 | 35 | 39 | 34 | |
| Overweight | 32 | 35 | 37 | 38 | 44 | <0.001 |
| Obesity | 12 | 17 | 28 | 21 | 21 | |
| Common mental disorders | ||||||
| Common mental disorders | 20 | 24 | 49 | 34 | 39 | <0.001 |
| Helsinki Health Study, Finland. Missing categories omitted (1–3%). | ||||||
| Work Disability Clusters | |||||
|---|---|---|---|---|---|
| 1. No Work Disability | 2. Minor Various | 3. Mental | 4. Musculoskeletal | 5. Other Type | |
| AMEs [95% CI] | AMEs [95% CI] | AMEs [95% CI] | AMEs [95% CI] | AMEs [95% CI] | |
| Pain (ref. no pain) | |||||
| Single location pain | −9.9 *** [−14.6–−5.1] | 4.2 [−0.9–9.2] | −0.6 [−2.1–0.8] | 4.9 *** [2.1–7.7] | 1.5 [−0.5–3.4] |
| 2 locations | −13.7 *** [−19.1–−8.3] | 4.5 [−1.2–10.3] | −1.5 * [−2.9–−0.1] | 8.1 *** [4.6–11.5] | 2.6 * [0.2–5.0] |
| 3–7 locations | −17.1 *** [−22.7–−11.5] | 3.7 [−2.3–9.8] | 2.4 * [0.0–4.7] | 8.1 *** [4.7–11.6] | 2.9 * [0.4–5.3] |
| Common mental disorders (Ref. no) | |||||
| Yes | −4.5 * [−8.7–−0.3] | −2.0 [−6.4–2.5] | 2.7 ** [1.0–4.5] | 1.9 [−0.5–4.3] | 1.8 * [0.0–3.6] |
| Gender (ref. men) | |||||
| Women | −4.7 + [−9.6–0.3] | 2.5 [−2.7–7.6] | 0.3 [−1.3–2.0] | 2.6 + [−0.1–5.4] | −0.7 [−2.9–1.4] |
| Age in 2007 (ref. 45–49) | |||||
| 50–54 | −5.1 * [−9.3–−0.9] | 1.3 [−3.1–5.7] | 1.5 * [0.2–2.9] | 0.9 [−1.4–3.2] | 1.4 + [−0.2–3.0] |
| 55–57 | −4.8 * [−9.1–−0.5] | −0.4 [−5.0–4.1] | 1.3 + [−0.1–2.7] | 2.4 + [−0.0–4.9] | 1.5 + [−0.2–3.2] |
| Occupational class (ref. managers or professional) | |||||
| Semi-professionals | −7.6 ** [−12.5–−2.7] | 2.9 [−2.1–7.9] | 2.1 * [0.4–3.8] | 1.3 [−1.1–3.7] | 1.4 [−0.5–3.2] |
| Routine non-manual workers | −14.6 *** [−19.5–−9.7] | 5.7 * [0.6–10.8] | 0.6 [−0.8–2.1] | 6.8 *** [4.1–9.4] | 1.4 [−0.4–3.2] |
| Manual workers | −19.0 *** [−25.7–−12.3] | 8.4 * [1.2–15.5] | 1.1 [−1.3–3.4] | 5.7 ** [2.0–9.4] | 3.8 * [0.8–6.9] |
| Working conditions | |||||
| Physically strenuous work (ref. no) | −2.0 [−6.3–2.4] | −2.7 [−7.2–1.9] | −0.9 [−2.3–0.4] | 4.8 *** [2.4–7.2] | 0.8 [−1.0–2.5] |
| Mentally strenuous work (ref. no) | −4.5 + [−9.8–0.8] | 1.4 [−4.3–7.0] | 2.3 * [0.1–4.5] | −0.6 [−3.5–2.3] | 1.4 [−0.9–3.8] |
| Body weight (ref. BMI < 25) | |||||
| Overweight | −5.8 ** [−9.6–−1.9] | 1.3 [−2.8–5.4] | 0.8 [−0.4–2.1] | 1.8 [−0.4–4.0] | 1.8 * [0.2–3.4] |
| Obesity | −9.0 *** [−14.1–−4.0] | 3.1 [−2.2–8.5] | 2.2 * [0.3–4.1] | 2.4 [−0.5–5.2] | 1.4 [−0.6–3.3] |
| Smoking (ref. never) | |||||
| Past smoking | −3.2 [−7.5–1.2] | 1.7 [−2.8–6.3] | −0.4 [−1.8–1.0] | 1.3 [−1.2–3.8] | 0.5 [−1.2–2.2] |
| Smoking | −10.2 *** [−15.0–−5.5] | 3.6 [−1.5–8.7] | 0.6 [−1.2–2.3] | 3.2 * [0.4–5.9] | 2.9 ** [0.8–5.1] |
| Binge drinking (once a month or more, ref. no) | |||||
| Yes | −4.4 * [−8.6–−0.1] | 5.1 * [0.6–9.6] | −0.8 [−2.1–0.5] | −0.5 [−2.8–1.9] | 0.5 [−1.2–2.2] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiilamo, A.; Huttu, A.; Øverland, S.; Pietiläinen, O.; Rahkonen, O.; Lallukka, T. Pain in Multiple Sites and Clusters of Cause-Specific Work Disability Development among Midlife Municipal Employees. Int. J. Environ. Res. Public Health 2021, 18, 3375. https://doi.org/10.3390/ijerph18073375
Hiilamo A, Huttu A, Øverland S, Pietiläinen O, Rahkonen O, Lallukka T. Pain in Multiple Sites and Clusters of Cause-Specific Work Disability Development among Midlife Municipal Employees. International Journal of Environmental Research and Public Health. 2021; 18(7):3375. https://doi.org/10.3390/ijerph18073375
Chicago/Turabian StyleHiilamo, Aapo, Anna Huttu, Simon Øverland, Olli Pietiläinen, Ossi Rahkonen, and Tea Lallukka. 2021. "Pain in Multiple Sites and Clusters of Cause-Specific Work Disability Development among Midlife Municipal Employees" International Journal of Environmental Research and Public Health 18, no. 7: 3375. https://doi.org/10.3390/ijerph18073375