
The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wartecki, A.; Rzymski, P. On the Coronaviruses and Their Associations with the Aquatic Environment and Wastewater. Water 2020, 12, 1598. [Google Scholar] [CrossRef]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; De Caro, F. Infection Control in Dental Practice During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. [Google Scholar] [CrossRef] [PubMed]
- Spagnuolo, G.; De Vito, D.; Rengo, S.; Tatullo, M. COVID-19 Outbreak: An Overview on Dentistry. Int. J. Environ. Res. Public Health 2020, 17, 2094. [Google Scholar] [CrossRef] [Green Version]
- Ethics Subcommittee of the Council on Ethics, Bylaws and Judicial Affairs. Ethical Practice during the COVID-19 Pandemic. J. Am. Dent. Assoc. 2020, 151, 377–378. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, P. Dentistry and Coronavirus (COVID-19)—Moral Decision-Making. Br. Dent. J. 2020, 228, 503–505. [Google Scholar] [CrossRef]
- Dacic, S.D.; Miljkovic, M.N.; Jovanovic, M.C. Dental Care during the Covid-19 Pandemic—To Treat or Not to Treat? J. Infect. Dev. Ctries. 2020, 14, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Attia, S.; Howaldt, H.-P. Impact of COVID-19 on the Dental Community: Part I before Vaccine (BV). J. Clin. Med. 2021, 10, 288. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhao, J.; Peng, J.; Li, X.; Deng, X.; Geng, Z.; Shen, Z.; Guo, F.; Zhang, Q.; Jin, Y.; et al. Detection of SARS-CoV-2 in Saliva and Characterization of Oral Symptoms in COVID-19 Patients. Cell Prolif. 2020, 53, e12923. [Google Scholar] [CrossRef]
- Gurgel, B.C.d.V.; Borges, S.B.; Borges, R.E.A.; Calderon, P.D.S. COVID-19: Perspectives for the Management of Dental Care and Education. J. Appl. Oral. Sci. 2020, 28, e20200358. [Google Scholar] [CrossRef] [PubMed]
- Izzetti, R.; Nisi, M.; Gabriele, M.; Graziani, F. COVID-19 Transmission in Dental Practice: Brief Review of Preventive Measures in Italy. J. Dent. Res. 2020, 99, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Vergara-Buenaventura, A.; Castro-Ruiz, C. Use of Mouthwashes against COVID-19 in Dentistry. Br. J. Oral Maxillofac. Surg. 2020, 58, 924–927. [Google Scholar] [CrossRef]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission Routes of 2019-NCoV and Controls in Dental Practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Ali, K.; Raja, M. Coronavirus Disease 2019 (COVID-19): Challenges and Management of Aerosol-Generating Procedures in Dentistry. Evid. Based Dent. 2020, 21, 44–45. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Nkenke, E. Approaches to the Management of Patients in Oral and Maxillofacial Surgery during COVID-19 Pandemic. J. Craniomaxillofac. Surg. 2020, 48, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Mallineni, S.K.; Innes, N.P.; Raggio, D.P.; Araujo, M.P.; Robertson, M.D.; Jayaraman, J. Coronavirus Disease (COVID-19): Characteristics in Children and Considerations for Dentists Providing Their Care. Int. J. Paediatr. Dent. 2020, 30, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passarelli, P.C.; Rella, E.; Manicone, P.F.; Garcia-Godoy, F.; D’Addona, A. The Impact of the COVID-19 Infection in Dentistry. Exp. Biol. Med. 2020, 245, 940–944. [Google Scholar] [CrossRef] [PubMed]
- Bhumireddy, J.; Mallineni, S.K.; Nuvvula, S. Challenges and Possible Solutions in Dental Practice during and Post COVID-19. Environ. Sci. Pollut. Res. Int. 2021, 28, 1275–1277. [Google Scholar] [CrossRef]
- Bizzoca, M.E.; Campisi, G.; Muzio, L.L. Covid-19 Pandemic: What Changes for Dentists and Oral Medicine Experts? A Narrative Review and Novel Approaches to Infection Containment. Int. J. Environ. Res. Public Health 2020, 17, 3793. [Google Scholar] [CrossRef] [PubMed]
- Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef]
- Dalewski, B.; Palka, L.; Kiczmer, P.; Sobolewska, E. The Impact of SARS-CoV-2 Outbreak on the Polish Dental Community’s Standards of Care—A Six-Month Retrospective Survey-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 1281. [Google Scholar] [CrossRef] [PubMed]
- Sycinska-Dziarnowska, M.; Paradowska-Stankiewicz, I. Dental Challenges and the Needs of the Population during the Covid-19 Pandemic Period. Real-Time Surveillance Using Google Trends. Int. J. Environ. Res. Public Health 2020, 17, 8999. [Google Scholar] [CrossRef]
- Goddard, A.F.; Patel, M. The Changing Face of Medical Professionalism and the Impact of COVID-19. Lancet 2021, 397, 950–952. [Google Scholar] [CrossRef]
- Bahadori, M.; Raadabadi, M.; Ravangard, R.; Baldacchino, D. Factors Affecting Dental Service Quality. Int. J. Health Care Qual. Assur. 2015, 28, 678–689. [Google Scholar] [CrossRef] [PubMed]
- Cieślik, K.; Surdacka, A. Patient Satisfaction with Dental Services. Dent. Forum 2019, 47, 36–40. [Google Scholar] [CrossRef]
- Rocha, J.; Pinto, A.; Batista, M.; de Paula, J.S.; Ambrosano, G. The Importance of the Evaluation of Expectations and Perceptions to Improve the Dental Service Quality. Int. J. Health Care Qual. Assur. 2017, 30, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical Dental Care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef] [PubMed]
- De Almeida Barros Mourão, C.F.; Javid, K.; Bastos Barbosa, I. How Can We Reduce the Risks of SARS-CoV-2 (COVID-19) for Dentists and Their Patients? Evid. Based Dent. 2020, 21, 50–51. [Google Scholar] [CrossRef]
- Spicciarelli, V.; Marruganti, C.; Viviano, M.; Baldini, N.; Franciosi, G.; Tortoriello, M.; Ferrari, M.; Grandini, S. A New Framework to Identify Dental Emergencies in the COVID-19 Era. J. Oral Sci. 2020, 62, 344–347. [Google Scholar] [CrossRef]
- Ayub, K.; Alani, A. Acute Endodontic and Dental Trauma Provision during the COVID-19 Crisis. Br. Dent. J. 2020, 229, 169–175. [Google Scholar] [CrossRef]
- Peditto, M.; Scapellato, S.; Marcianò, A.; Costa, P.; Oteri, G. Dentistry during the COVID-19 Epidemic: An Italian Workflow for the Management of Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3325. [Google Scholar] [CrossRef]
- Banakar, M.; Bagheri Lankarani, K.; Jafarpour, D.; Moayedi, S.; Banakar, M.H.; MohammadSadeghi, A. COVID-19 Transmission Risk and Protective Protocols in Dentistry: A Systematic Review. BMC Oral Health 2020, 20, 275. [Google Scholar] [CrossRef] [PubMed]
- Dave, M.; Seoudi, N.; Coulthard, P. Urgent Dental Care for Patients during the COVID-19 Pandemic. Lancet 2020, 395, 1257. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Halabi, M.; Salami, A.; Alnuaimi, E.; Kowash, M.; Hussein, I. Assessment of Paediatric Dental Guidelines and Caries Management Alternatives in the Post COVID-19 Period. A Critical Review and Clinical Recommendations. Eur. Arch. Paediatr. Dent. 2020, 21, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Czajkowska, S.; Rupa-Matysek, J.; Gil, L.; Surdacka, A. Practical Recommendations for Treatment of Dental Patients with Congenital Bleeding Disorders during the Covid-19 Pandemic: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7245. [Google Scholar] [CrossRef]
- Chamorro-Petronacci, C.; Carreras-Presas, M.C.; Sanz-Marchena, A.; A Rodríguez-Fernández, M.; Suárez-Quintanilla, M.J.; Rivas-Mundiña, B.; Suárez-Quintanilla, J.; Pérez-Sayáns, M. Assessment of the Economic and Health-Care Impact of COVID-19 (SARS-CoV-2) on Public and Private Dental Surgeries in Spain: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 5139. [Google Scholar] [CrossRef]
- Schwendicke, F.; Krois, J.; Gomez, J. Impact of SARS-CoV2 (Covid-19) on Dental Practices: Economic Analysis. J. Dent. 2020, 99, 103387. [Google Scholar] [CrossRef] [PubMed]
- Peloso, R.M.; Pini, N.I.P.; Sundfeld Neto, D.; Mori, A.A.; de Oliveira, R.C.G.; Valarelli, F.P.; Freitas, K.M.S. How Does the Quarantine Resulting from COVID-19 Impact Dental Appointments and Patient Anxiety Levels? Braz. Oral Res. 2020, 34, e84. [Google Scholar] [CrossRef]
- Consolo, U.; Bellini, P.; Bencivenni, D.; Iani, C.; Checchi, V. Epidemiological Aspects and Psychological Reactions to COVID-19 of Dental Practitioners in the Northern Italy Districts of Modena and Reggio Emilia. Int. J. Environ. Res. Public Health 2020, 17, 3459. [Google Scholar] [CrossRef]
- Maffia, F.; Fontanari, M.; Vellone, V.; Cascone, P.; Mercuri, L.G. Impact of COVID-19 on Maxillofacial Surgery Practice: A Worldwide Survey. Int. J. Oral. Maxillofac. Surg. 2020, 49, 827–835. [Google Scholar] [CrossRef]
- Barca, I.; Cordaro, R.; Kallaverja, E.; Ferragina, F.; Cristofaro, M.G. Management in Oral and Maxillofacial Surgery during the COVID-19 Pandemic: Our Experience. Br. J. Oral Maxillofac. Surg. 2020, 58, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, P.; Thomson, P.; Dave, M.; Coulthard, F.P.; Seoudi, N.; Hill, M. The COVID-19 Pandemic and Dentistry: The Clinical, Legal and Economic Consequences—Part 1: Clinical. Br. Dent. J. 2020, 229, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Telles-Araujo, G.d.T.; Caminha, R.D.G.; Kallás, M.S.; da Silva Santos, P.S. Teledentistry Support in COVID-19 Oral Care. Clinics 2020, 75, e2030. [Google Scholar] [CrossRef]
- Machado, R.A.; de Souza, N.L.; Oliveira, R.M.; Martelli, H., Jr.; Bonan, P.R.F. Social Media and Telemedicine for Oral Diagnosis and Counselling in the COVID-19 Era. Oral Oncol. 2020, 105, 104685. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Pandemic | During Pandemic | ||
|---|---|---|---|
| Procedure | M (Q1–Q3) | M (Q1–Q3) | p-Value |
| dental examination | 0.171 (0.167–0.177) | 0.172 (0.160–0.188) | 0.840 |
| periapical X-ray | 0.043 (0.040–0.050) | 0.044 (0.039–0.050) | 0.977 |
| panoramic X-ray | 0.029 (0.025–0.030) | 0.027 (0.024–0.031) | 0.795 |
| Conservative dentistry | |||
| temporary filling | 0.019 (0.019–0.022) | 0.018 (0.016–0.022) | 0.260 |
| single-surface filling | 0.042 (0.038–0.047) | 0.038 (0.019–0.043) | 0.141 |
| two-surface filling | 0.040 (0.033–0.043) | 0.032 (0.021–0.037) | 0.019 * |
| multi-surface filling | 0.009 (0.007–0.011) | 0.007 (0.006–0.008) | 0.061 |
| refunded restoration | 0.075 (0.066–0.078) | 0.068 (0.038–0.076) | 0.285 |
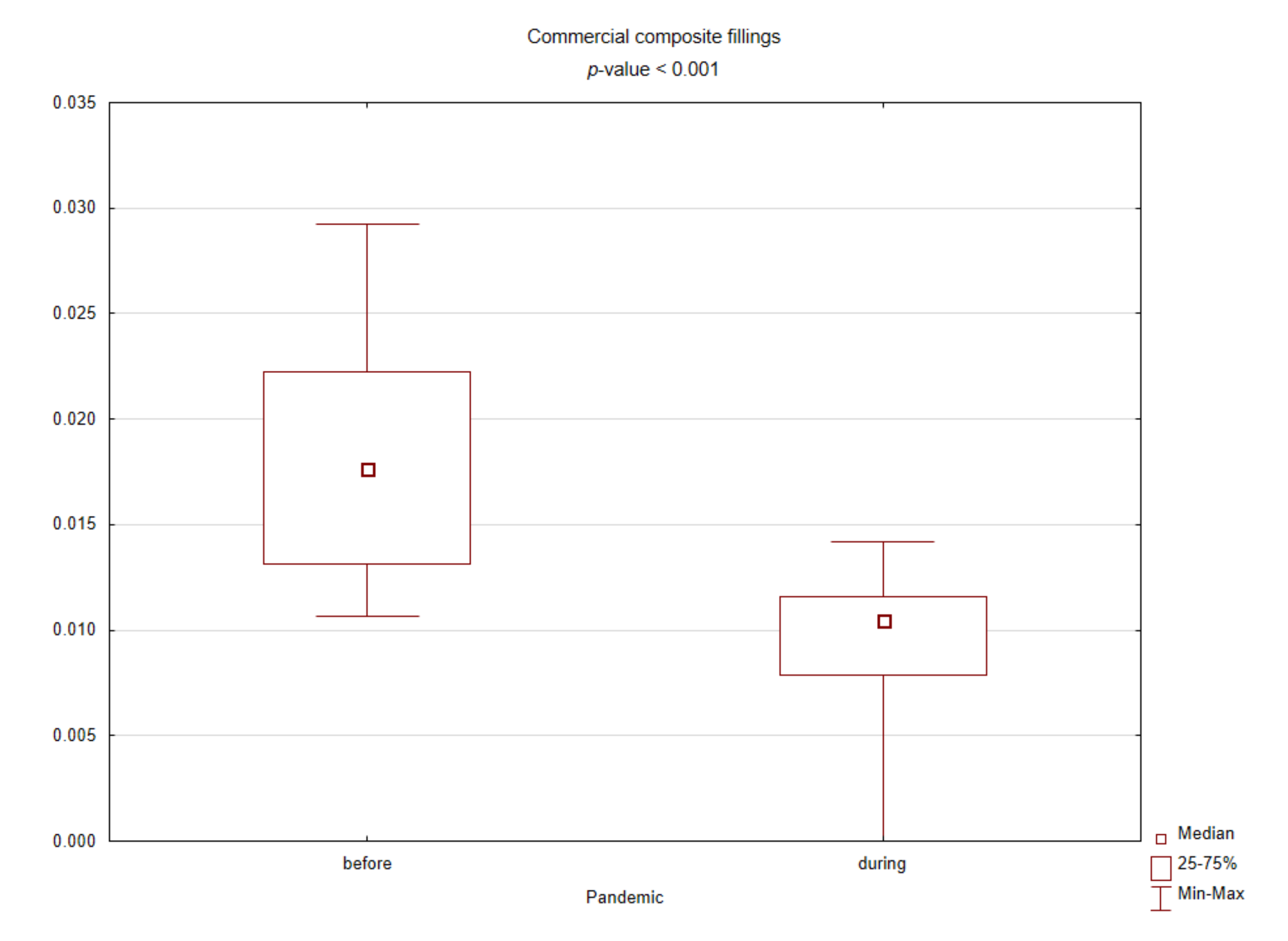
| commercial restoration | 0.018 (0.013–0.022) | 0.010 (0.008–0.012) | <0.001 * |
| filled deciduous teeth | 0.022 (0.019–0.023) | 0.020 (0.017–0.022) | 0.312 |
| filled permanent teeth | 0.091 (0.084–0.095) | 0.078 (0.046–0.088) | 0.046 * |
| total filled teeth | 0.112 (0.107–0.118) | 0.098 (0.067–0.110) | 0.026 * |
| Endodontics | |||
| intervention procedure | 0.008 (0.007–0.010) | 0.010 (0.009–0.011) | 0.078 |
| intracanal dressing | 0.003 (0.003–0.004) | 0.003 (0.003–0.004) | 0.564 |
| root canal filling | 0.008 (0.007–0.009) | 0.004 (0.002–0.005) | <0.001 * |
| Periodontology | |||
| scaling (quadrant) | 0.111 (0.104–0.118) | 0.105 (0.070–0.123) | 0.507 |
| curettage (quadrant) | 0.006 (0.006–0.007) | 0.005 (0.003–0.007) | 0.194 |
| gingival pocket rinsing | 0.012 (0.010–0.013) | 0.011 (0.008–0.015) | 0.885 |
| oral lesions application | 0.004 (0.003–0.005) | 0.004 (0.002–0.004) | 0.341 |
| Dental surgery | |||
| abscess drainage | 0.001 (0.001–0.002) | 0.002 (0.002–0.003) | 0.002 * |
| intra-alveolar dressing | 0.023 (0.019–0.027) | 0.031 (0.025–0.034) | 0.005 * |
| single-rooted tooth extraction | 0.010 (0.009–0.010) | 0.011 (0.010–0.011) | 0.089 |
| multi-rooted tooth extraction | 0.012 (0.011–0.013) | 0.014 (0.013–0.018) | 0.006 * |
| intra-alveolar extraction | 0.023 (0.020–0.027) | 0.029 (0.027–0.034) | 0.002 * |
| extra-alveolar extraction | 0.003 (0.002–0.003) | 0.005 (0.004–0.009) | 0.002 * |
| impacted tooth extraction | 0.003 (0.003–0.004) | 0.007 (0.005–0.008) | 0.003 * |
| total extracted teeth | 0.051 (0.048–0.054) | 0.064 (0.061–0.077) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nijakowski, K.; Cieślik, K.; Łaganowski, K.; Gruszczyński, D.; Surdacka, A. The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures. Int. J. Environ. Res. Public Health 2021, 18, 3421. https://doi.org/10.3390/ijerph18073421
Nijakowski K, Cieślik K, Łaganowski K, Gruszczyński D, Surdacka A. The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures. International Journal of Environmental Research and Public Health. 2021; 18(7):3421. https://doi.org/10.3390/ijerph18073421
Chicago/Turabian StyleNijakowski, Kacper, Kornela Cieślik, Kacper Łaganowski, Dawid Gruszczyński, and Anna Surdacka. 2021. "The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures" International Journal of Environmental Research and Public Health 18, no. 7: 3421. https://doi.org/10.3390/ijerph18073421
APA StyleNijakowski, K., Cieślik, K., Łaganowski, K., Gruszczyński, D., & Surdacka, A. (2021). The Impact of the COVID-19 Pandemic on the Spectrum of Performed Dental Procedures. International Journal of Environmental Research and Public Health, 18(7), 3421. https://doi.org/10.3390/ijerph18073421