
Processes of a Transformation of Young Drivers’ Responsibility for Health—Carpe Diem

Abstract
:1. Introduction
1.1. Factors Influencing Risky Driving
1.2. Understanding Responsibility for Health
2. Materials and Methods
Description of the Group
- Preliminary analysis of initial data. Preliminary analysis of the results obtained by each of the respondents aims to identify, on the basis of methods (their items) and survey data, categories important for the reconstruction of the characteristics of the respondents, including: manifested health behaviours, recognised criteria of health, and the sense of locus of control. The research used information obtained from three questionnaires: the Inventory of Health Behaviours, the Multidimensional Health Locus of Control, and the Criteria of Health List. The Inventory of Health Behaviours (IHB, Z. Juczyński) consists of 24 items describing various types of behaviour related to health. The tested person responds to each statement on a scale from 1—almost never—to 5—almost always. The second questionnaire used in the study was the Multidimensional Health Locus of Control (MHLC, Z. Juczyński). The scale consists of 18 statements concerning the locus of health control in three aspects: the internal locus, the influence of others, and chance. The examined person responds to the statements on a scale from 1 (I strongly disagree) to 6 (I strongly agree). The last questionnaire used was the Criteria of Health List (LHC, Z. Juczyński), consisting of 24 statements describing various dimensions of physical, mental, and social health.
- Selection of descriptive categories. As a result of the analysis of the content of items from the methods and the questionnaires, characteristics were selected that allowed the authors to describe each of the respondents. Example: Manifestations of concern for one’s own health—health behaviours (IHB, Item 10: “I follow medical recommendations resulting from my medical examination”).
- Collating each individual’s characteristics in an individual database. The record created was a kind of basic report describing a person’s features and functioning in terms of health, health attribution, and attitude to their own health.
3. Results
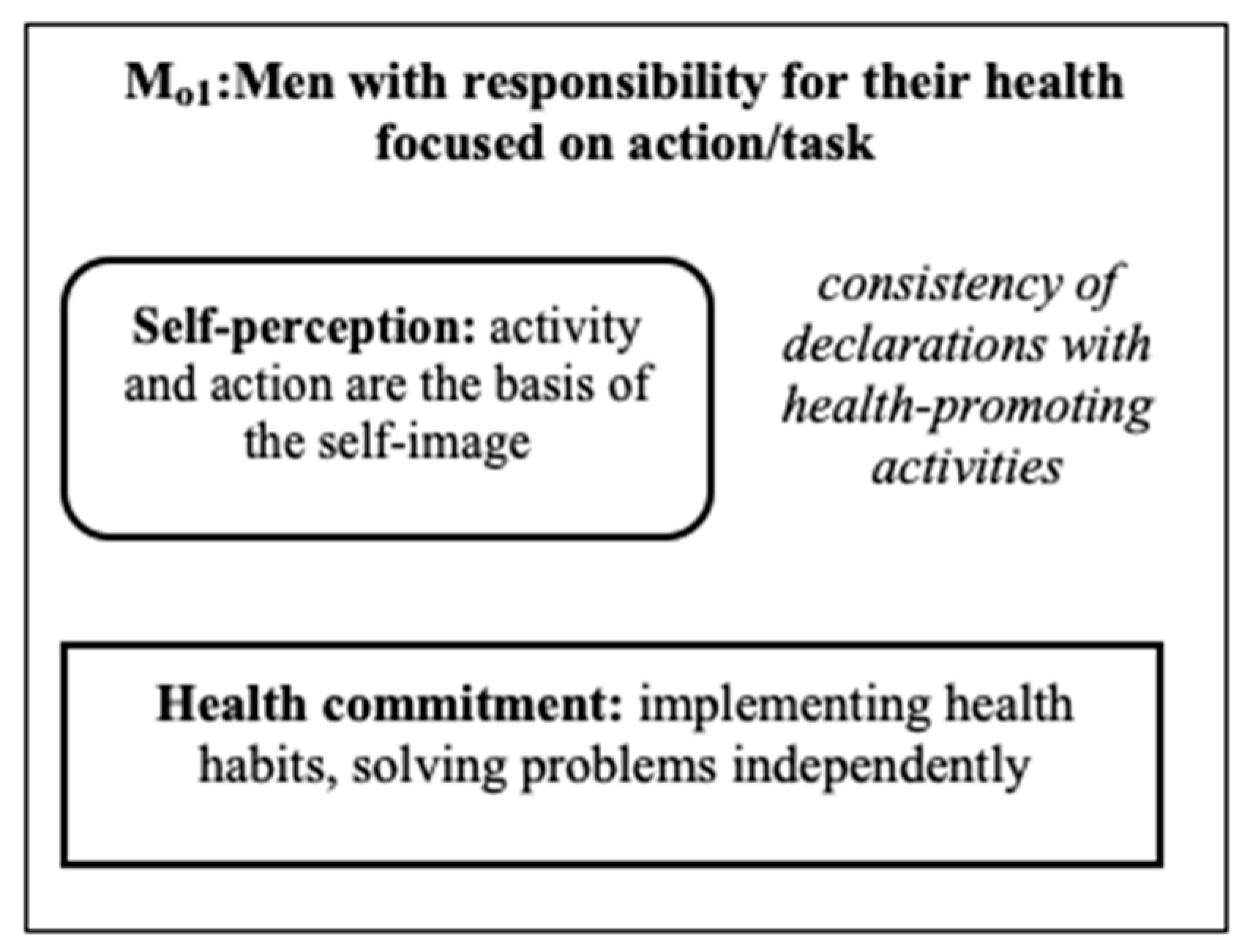
3.1. People Who Refrain from Driving Fast
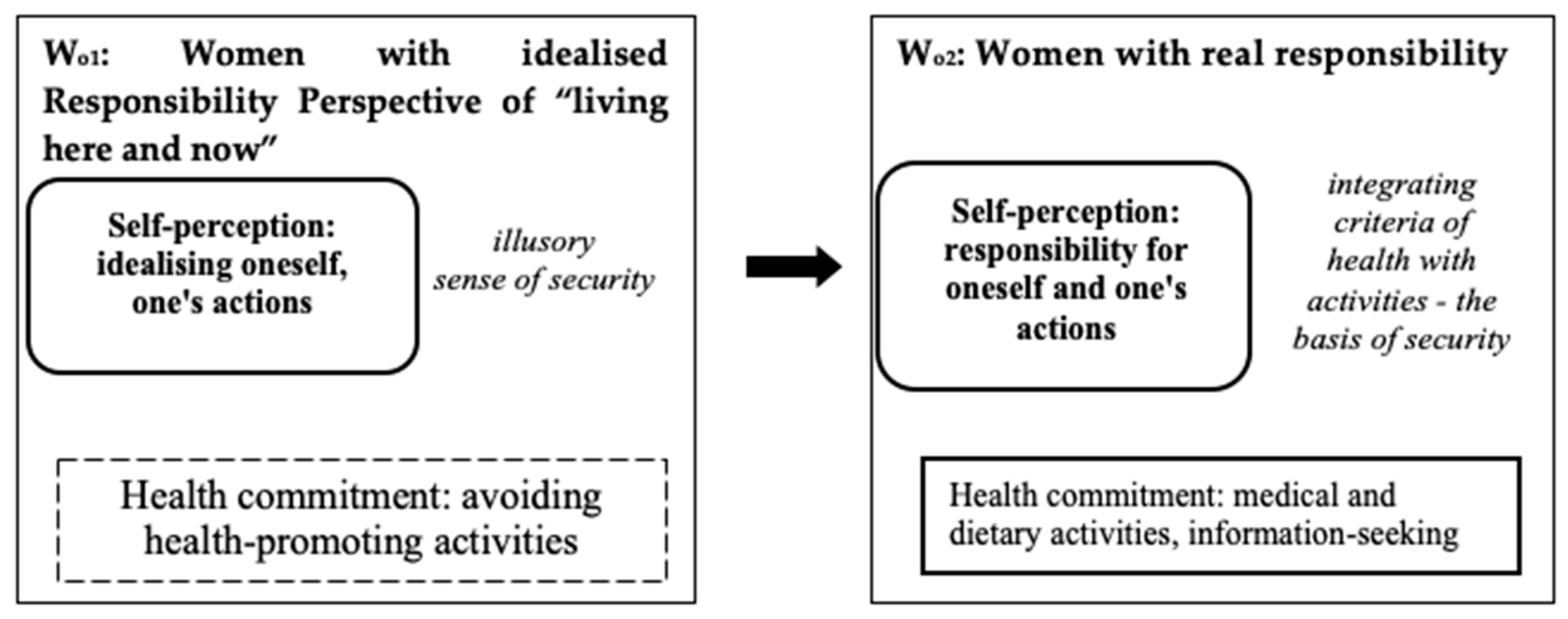
3.2. Wo1: Women with Idealised Responsibility for Their Health
3.3. Wo2: Women with Real Responsibility for Their Health
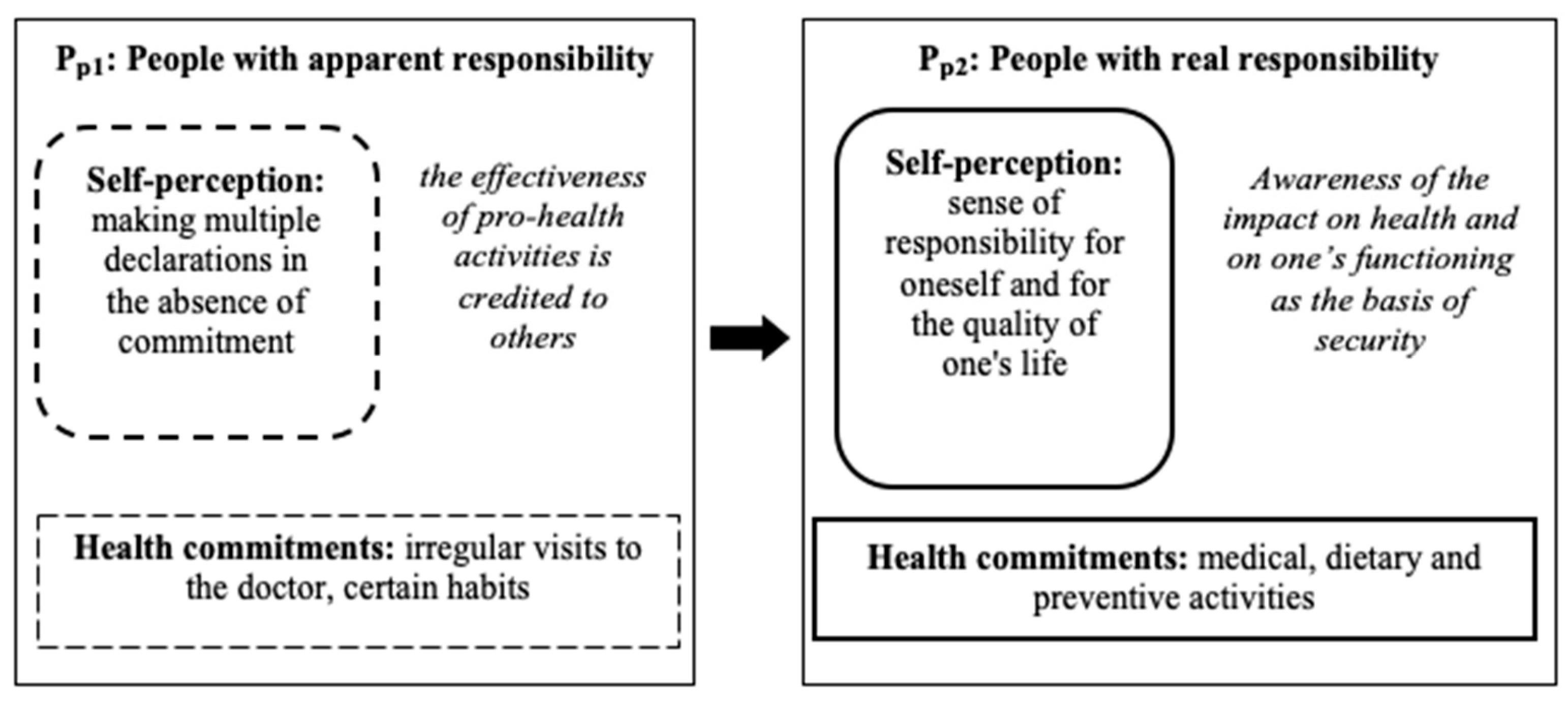
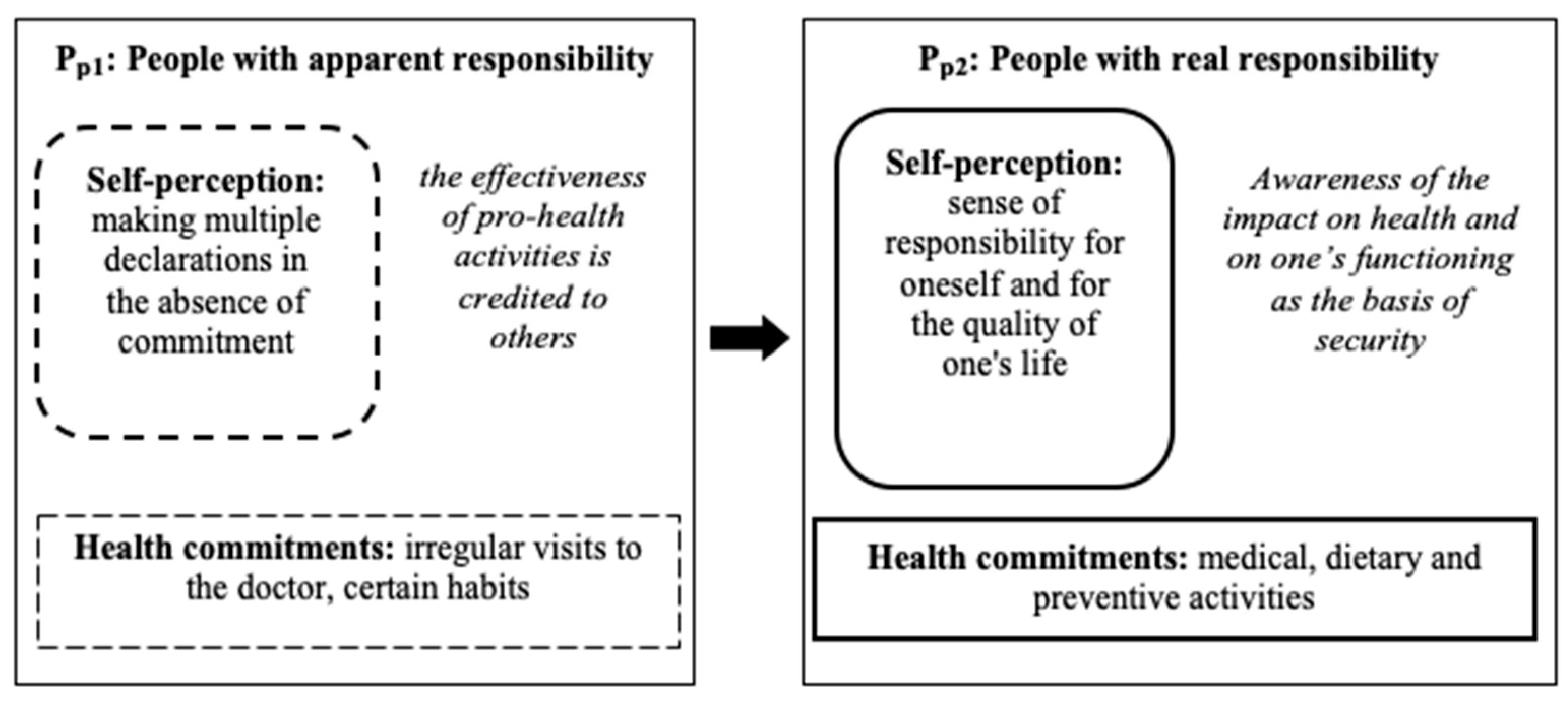
3.4. Pp1: People with Apparent Responsibility for Their Health
3.5. Pp2: People with Real Responsibility for Their Health
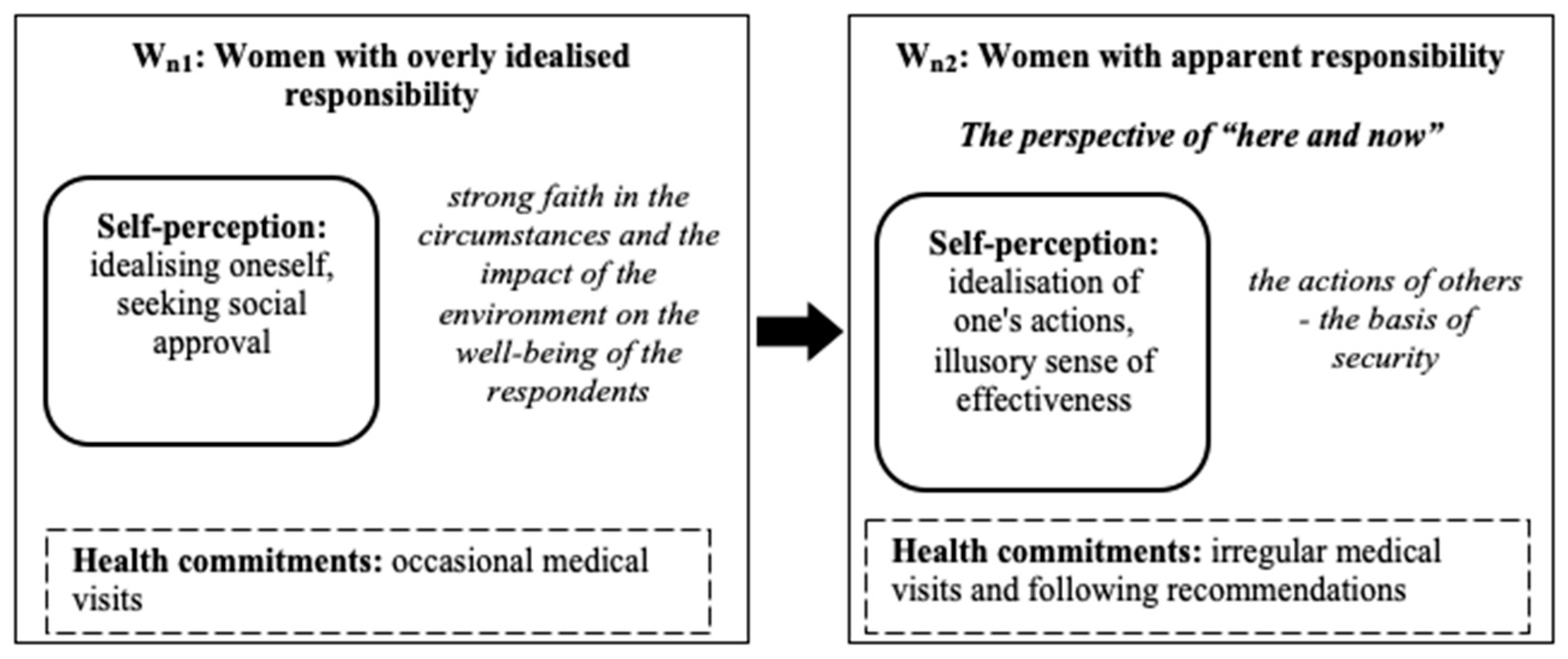
3.6. Wn1: Women with Excessively Idealised Responsibility for Their Health
3.7. Wn2: Women with Apparent Responsibility for Their Health
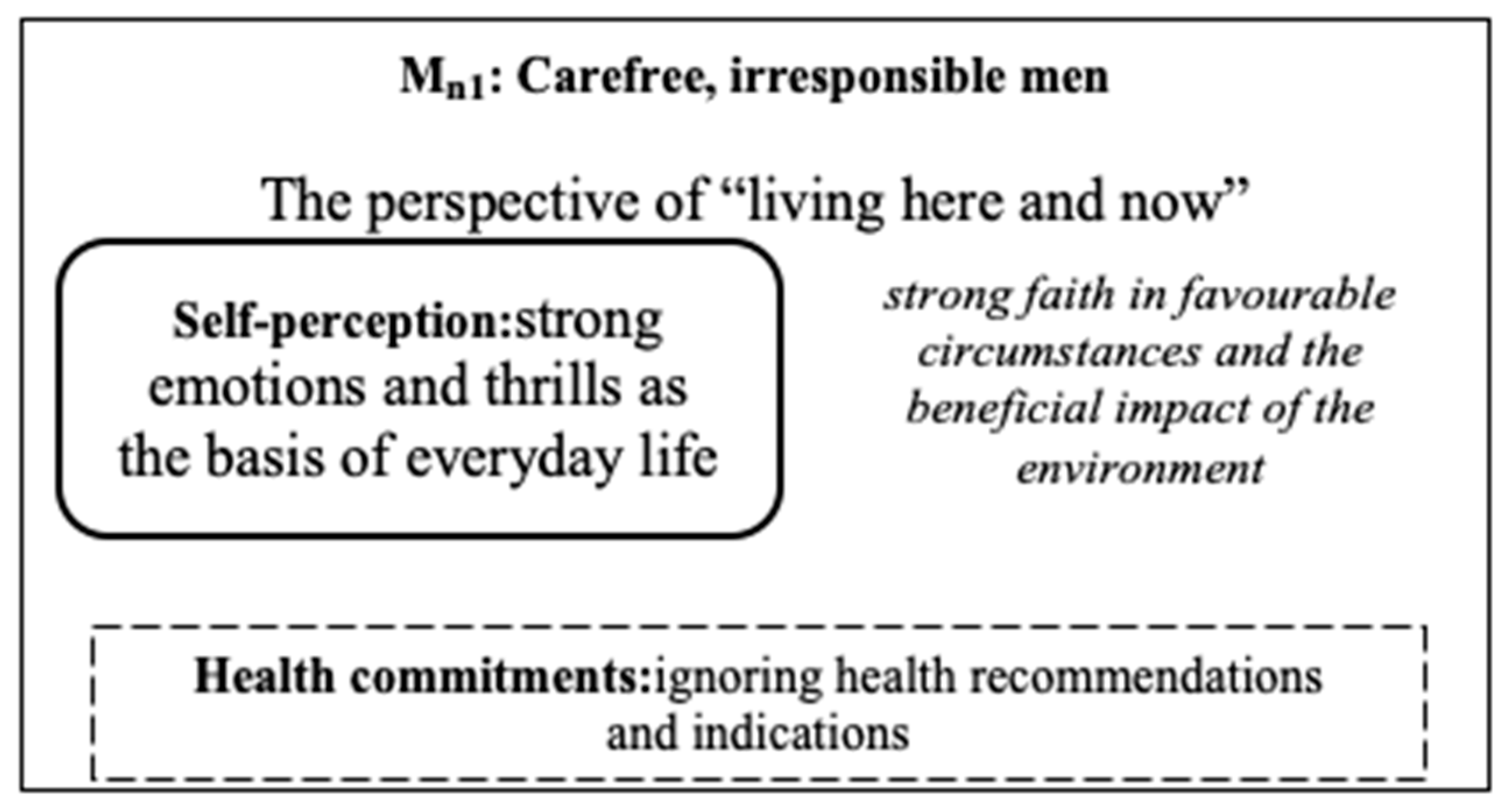
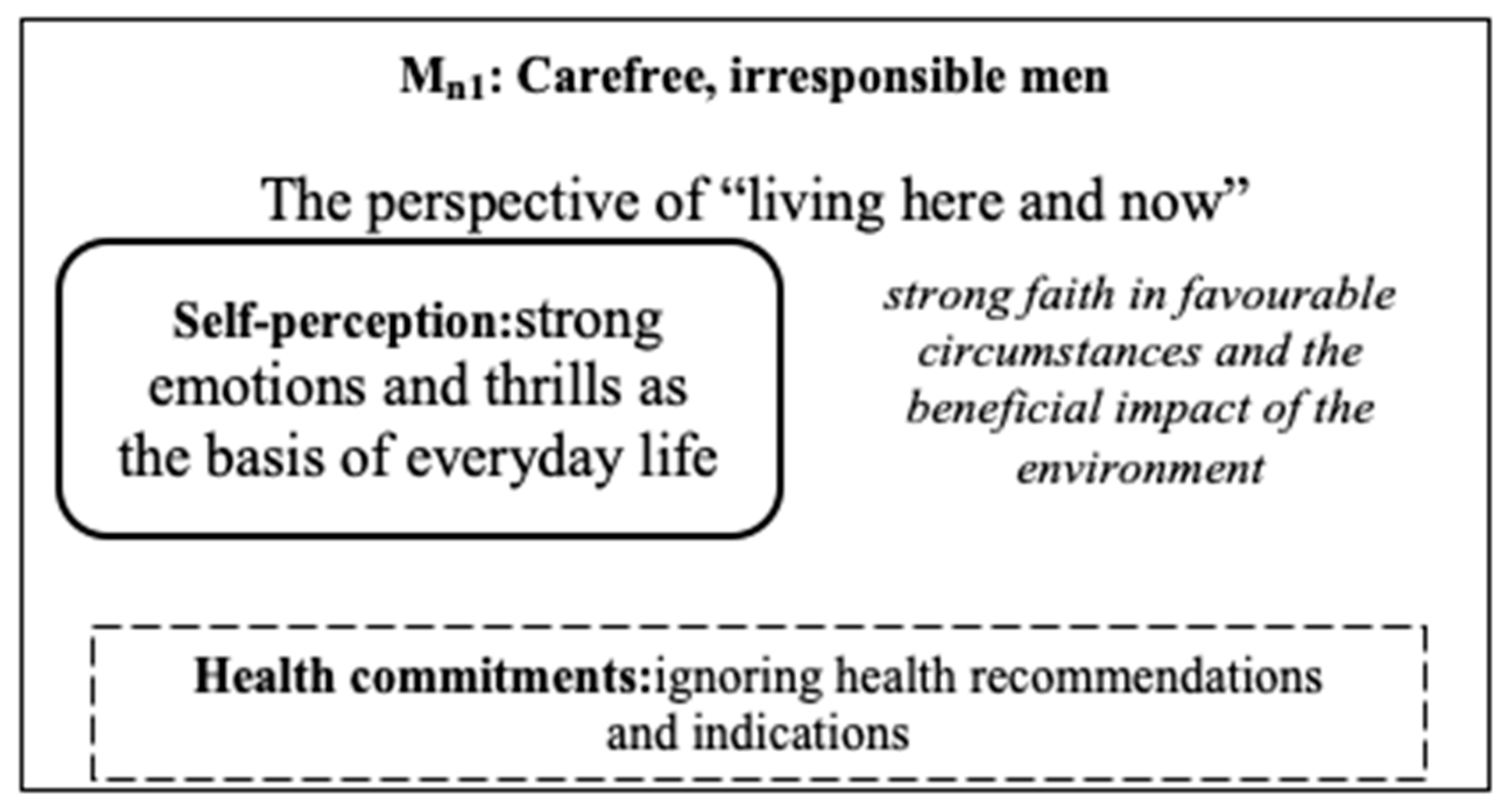
3.8. Mn1: Carefree Men, Irresponsible with Their Health
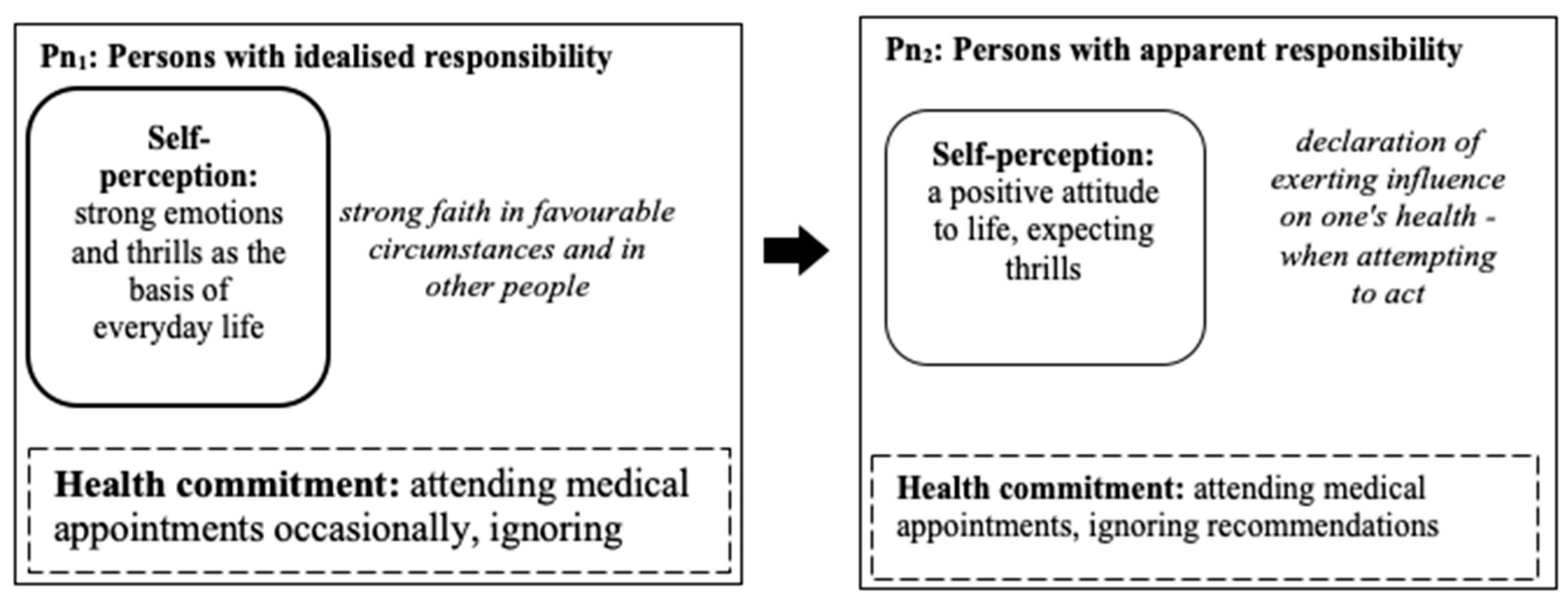
3.9. Pn1: Persons with Idealised Responsibility for Their Health
3.10. Pn2: Personsw Apparent Responsibility for Their Health
4. Discussion
5. Conclusions
- (1)
- the adopted model of responsibility for health partly explains why young drivers engage in fast driving,
- (2)
- the most important factor in the prediction of these risky behaviours is treating health as a state of pleasure,
- (3)
- the transformation processes of the factors of responsibility for health are differentiated by gender:
- (a)
- the group that does not refrain from driving fast: for women they range from attitudes of idealising themselves and their abilities to have hedonistic attitudes, for men these are individuals with immediately hedonistic attitudes; a mixed group also emerged in which the initial attitudes are immediately characterised by pleasure tendencies that turn into a hedonistic attitude to life and thrill-seeking;
- (b)
- the group refraining from driving fast: for women transformations from avoidance attitudes to health-promoting behaviours, for men manifestations of responsibility for health, in the mixed group (from empty declarations to the integration of declarations with pro-health activities).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Komenda Główna Policji Biuro Ruchu Drogowego. Road Accidents in Poland in 2015–2018; Agencja Wydawnicza ARGIsc: Warsaw, Poland.
- Stawiarska-Lietzau, M. Ryzykanci—Bohaterowie czy ofiary? Kulturowe uwarunkowania ryzykownej jazdy młodych mężczyzn. Prace Naukowe Akademii im. Jana Długosza Częstochowie Seria Pedagog. 2011, 20, 211–220. [Google Scholar]
- Riskfactors. Available online: https://www.obserwatoriumbrd.pl/pl/analizy_brd/problemy_brd/mlodzi_kierowcy/czynniki_ryzyka/ (accessed on 30 January 2021).
- The Characteristics of the Group. Available online: https://www.obserwatoriumbrd.pl/pl/analizy_brd/problemy_brd/mlodzi_kierowcy/charakterystyka_grupy/ (accessed on 30 January 2021).
- Who and Why Does Exceed the Speed Limits. Available online: https://www.obserwatoriumbrd.pl/pl/analizy_brd/problemy_brd/predkosc/kto-i-dlaczego-przekracza-predkosc/ (accessed on 30 January 2021).
- Oviedo-Trespalacios, O.; Scott-Parker, B. Fast and furious: A neglected issue in health promotion among young drivers. Health Promot. J. Aust. Off. J. Aust. Assoc. Health Promot. Prof. 2019, 30, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Jackowska, B.; Wycinka, E. The influence of generation on the risk of road accidents. Statistical News. Pol. Stat. 2019, 64, 64–82. [Google Scholar]
- Wontorczyk, A. Dangerous Behavior of Drivers. Psychological Model of Behavior Regulation in Road Traffic; Wydawnictwo Uniwersytetu Jagiellońskiego: Kraków, Poland, 2011. [Google Scholar]
- Znajmiecka-Sikora, M.; Sałagacka, M. Personal determinators of risk and aggressive behavior in the motorcycle group. Zesz. Nauk. Politech. Śląskiej. Seria Organ. Zarządzanie 2018, 132, 731–747. [Google Scholar]
- Suchocka, L. A Sense of Responsibility in Health and Disease. Noo-Theoretical Perspective; Difin: Warsaw, Poland, 2010. [Google Scholar]
- Wagner, S.; Banaszkiewicz, M.; Andruszkiewicz, A.; Strahl, A.; Miler, A.; Kubica, A. Healthbehaviors and place of health in the hierarchy of youthvalues. Med. Ogólnai Nauk. Zdrowiu 2015, 21, 278–281. [Google Scholar] [CrossRef]
- Kulik, A.; Frańczyk, E. Wisdom in the Hierarchy of Student Values in the Light of Empirical Research. In Mądrość Jako Sprawność Moralna w Wychowaniu; Jazukiewicz, I., Ed.; Wydawnictwo Naukowe Uniwersytetu Szczecińskiego: Szczecin, Poland, 2018; pp. 187–205. [Google Scholar]
- Jaworski, M.; Adamus, M.; Bojar, J. The Sense of Responsibility for the Health as an Important Element of Health Education. DEStech Trans. Soc. Sci. Educ. Hum. Sci. 2017. [Google Scholar] [CrossRef]
- Stawarz, B.; Lewicka, M.; Sulima, M.; Wiktor, M. Health as a value as assessed by students from the Podkarpackie Province. Ann. Acad. Med. Silesiensis 2014, 4, 226–227. [Google Scholar]
- Juczynski, Z. Measurementtools in Healthpromotion and Psychology; Warszawa Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warsaw, Poland, 2012. [Google Scholar]
- Sukys, S.; Cesnaitiene, V.J.; Ossowsky, P.Z.W. Is Health Education at University Associated with Students’ Health Literacy? BioMed Res. Int. 2017, 2017, 8516843. [Google Scholar] [CrossRef] [PubMed]
- Mazur, J. Subjective health assessment. In Health of Students in 2018 Against the Background of the New HBSC Research Model; Mazur, J., Małkowska-Szkutnik, A., Eds.; Instytut Matkii Dziecka: Warsaw, Poland, 2018; pp. 59–69. [Google Scholar]
- Lally, K.; Nathan-V, Y.; Dunne, S.; McGrath, D.; Cullen, W.; Meagher, D.; Coffey, J.C.; Dunne, C. Awareness of sexually transmitted infection and protection methods among university students in Ireland. Ir. J. Med. Sci. 2015, 184, 135–142. [Google Scholar] [CrossRef]
- Burnett, A.J.; Sabato, T.M.; Walter, K.O.; Kerr, D.; Wagner, L.; Smith, A. The Influence of Attributional Style on Substance Use and Risky Sexual Behavior Among College Students. Coll. Stud. J. 2014, 1, 122–137. [Google Scholar]
- Kawczyńska-Butrym, Z.; Butrym, M.; Czapka, E. Students of Lublin universities. Health Risk Behaviors 20 Years Later; UMCS: Lublin, Poland, 2015. [Google Scholar]
- Andruszkiewicz, A.; Basińska, M.; Kubica, A. Factorsinfluencing the level of motivation to quit smoking in the group of peopleaddicted to nicotine. Folia Cardiol. Excerpta 2010, 5, 49–53. [Google Scholar]
- Ahmed, F.M.; Badawy, R.E. Health Locus of Control and Health Promoting Behaviors among Nursing and Non-Nursing Students in Zagazig University. IOSR J. Nurs. Health Sci. 2016, 5, 28–35. [Google Scholar] [CrossRef]
- Pirzadeh, A.; Moghaddam, E.S.; Araghinezhad, Z.E.; Ardakani, T.; Torkian, S. Health Locus of Control among Students of Isfahan University of Medical Sciences (2018). Health Educ. Health Promot. 2019, 7, 133–137. [Google Scholar] [CrossRef]
- Cohen, M.; Azaiza, F. Health-promoting behaviors and health locus of control from a multicultural perspective. Ethn. Dis. 2007, 17, 636–642. [Google Scholar] [PubMed]
- Helmer, S.M.; Krämer, A.; Mikolajczyk, R.T. Health-related locus of control and health behaviour among university students in North Rhine Westphalia, Germany. BMC Res. Notes 2012, 5, 703. [Google Scholar] [CrossRef] [Green Version]
- Figner, B.; Mackinlay, R.J.; Wilkening, F.; Weber, E.U. Affective and deliberative processes in risky choice: Age differences in risk taking in the columbia card task. J. Exp. Psychol. Learn. Mem. Cogn. 2009, 35, 709–730. [Google Scholar] [CrossRef] [Green Version]
- Willoughby, T.; Good, M.; Adachi, P.J.; Hamza, C.; Tavernier, R. Examining the link between adolescent brain development and risk taking from asocial–developmental perspective. Brain Cogn. 2013, 83, 315–324. [Google Scholar] [CrossRef]
- Rzechowska, E. 50+ workers at risk of redundancy, or what counsellors should know: A psychological perspective. J. Couns. 2014, 3, 247–277. [Google Scholar]
- Brandmaier, A.M.; von Oertzen, T.; McArdle, J.J.; Lindenberger, U. Structural equation model trees. Psychol. Methods 2013, 18, 71–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hand, D.; Manilla, H.; Smyth, P. Principles of Data Mining; MIT Press: London, UK, 2001. [Google Scholar]
- Wu, X.; Kumar, V.; Quinlan, J.R.; Ghosh, J.; Yang, Q.; Motoda, H.; McLachlan, G.J.; Ng, A.; Liu, B.; Yu, P.S.; et al. Top 10 algorithms in data mining. Knowl. Inf. Syst. 2008, 14, 1–37. [Google Scholar] [CrossRef] [Green Version]
- An Example of Forecasting Using Data Mining Methods. StatSoft Polska. Available online: https://www.statsoft.pl/Portals/0/Downloads/Przyklad_prognozowania.pdf (accessed on 30 January 2021).
- Quinlan, J.R. C4.5: Programs for Machine Learning; Morgan Kaufmann Publishers: San Mateo, CA, USA, 1993. [Google Scholar]
- Ay, S.; Yanıkkerem, E.; Çalim, S.; Yazici, M. Health-promoting lifestyle behaviour for cancer prevention: A survey of Turkish university students. Asian Pac. J. Cancer Prev. APJCP 2012, 13, 2269–2277. [Google Scholar] [CrossRef] [Green Version]
- Cairns, R.B.; Cairns, B.D. Lifelines and Risks: Pathways of Yout in Our Time; Cambridge University Press: London, UK, 1994. [Google Scholar]
- Henson, J.M.; Carey, M.P.; Carey, K.B.; Maisto, S.A. Associations among health behaviors and time perspective in young adults: Model testing with boot-strapping replication. J. Behav. Med. 2006, 29, 127–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamzah, S.R.; Suandi, T.; Krauss, S.E.; Hamzah, A.; Tamam, E. Youth hedonistic behaviour: Moderating role of peer attachment on the effect of religiosity and worldview. Int. J. Adolesc. Youth 2014, 19, 419–433. [Google Scholar] [CrossRef] [Green Version]
- Kanclerz, B. Life Orien- tations of Youth—Conditions and Changes]. Studia Eduk. 2015, 36, 143–164. [Google Scholar] [CrossRef] [Green Version]
- Thorpe, H. Sex, drugs and snowboarding: Legitimate definitions of taste and lifestyle in a physical youth culture. Leis. Stud. 2012, 31, 33–51. [Google Scholar] [CrossRef]
- Butrym, M. Pleasure or renunciation—Determinants of behaviorrelated to healthrisk. In Students of Lublin Universities. Health Risk Behaviors 20 Years Later; Krawczyńska-Butrym, Z., Butrym, M., Czapska, E., Eds.; UMCS: Lublin, Poland, 2015; pp. 109–119. [Google Scholar]
- Zhu, D.; Sze, N.N.; Bai, L. Roles of personal and environmental factors in the red light running propensity of pedestrian: Case study at the urban crosswalks. Transp. Res. Part F Traffic Psychol. Behav. 2021, 76, 47–58. [Google Scholar] [CrossRef]
- Graham, H.M.; White, R.D. Young people, dangerous driving and car culture. Youth Stud. Aust. 2007, 26, 28–35. [Google Scholar]
- Jessor, R. Risky driving and adolescent problem behaviour: An extension of problem-behavior theory. Alcohol Drugs Driv. 1987, 3, 1–11. [Google Scholar]
- Bauman, Z. Post modern personalpatterns. Studia Socjol. 2011, 1, 435–458. [Google Scholar]
- Bingham, C.R.; Shope, J.T.; Zakrajsek, J.; Raghunathan, T.E. Problem driving behaviour and psychosocial maturation in young adulthood. Accid. Anal. Prev. 2008, 40, 1758–1764. [Google Scholar] [CrossRef] [Green Version]
- Giedd, J.N. Structural magnetic resonance imaging of the adolescent brain. Ann. N. Y. Acad. Sci. 2004, 1021, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Sze, N.N.; Saxena, S.; Pinjari, A.R.; Bhat, C.R.; Bai, L. Evaluation of penalty and enforcement strategies to combat speeding offences among professional drivers: A Hong Kong stated preference experiment. Accid. Anal. Prev. 2020, 135, 105366. [Google Scholar] [CrossRef]
- Nosek, M.A.; Hughes, R.B.; Howland, C.A.; Young, M.E.; Mullen, P.D.; Shelton, M.L. The meaning of health for women with physical disabilities: A qualitative analysis. Fam. Community Health 2004, 27, 6–21. [Google Scholar] [CrossRef] [PubMed]
- Von Ah, D.; Ebert, S.; Ngamvitroj, A.; Park, N.; Kang, D.H. Predictors of health behaviours in college students. J. Adv. Nurs. 2004, 48, 463–474. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Participants | ||
|---|---|---|---|
| N | % | ||
| Age | M | 19.75 | |
| SD | 1.11 | ||
| Min | 18.00 | ||
| Max | 30.00 | ||
| Sex | female | 150.00 | 75.80 |
| male | 48.00 | 24.20 | |
| Place of residence | RA | 71.00 | 35.90 |
| T 50 | 17.00 | 8.60 | |
| C 150 | 28.00 | 14.10 | |
| LC400 | 45.00 | 22.70 | |
| Health condition | 1.00 | 9.00 | 4.50 |
| 2.00 | 12.00 | 6.10 | |
| 3.00 | 34.00 | 17.20 | |
| 4.00 | 100.00 | 50.50 | |
| 5.00 | 43.00 | 21.70 | |
| Awareness of the presence of chronic diseases in the family | Yes | 64.00 | 32.30 |
| No | 96.00 | 48.50 | |
| I do not know | 37.00 | 19.20 | |
| Predictors | B | SE | Wald | Exp (B) | p |
|---|---|---|---|---|---|
| Positive eating habits | −0.362 | 0.225 | 2.577 | 0.696 | n.s. |
| Preventive behaviours | −0.162 | 0.249 | 0.426 | 0.850 | n.s. |
| Positive psychological behaviours | 0.317 | 0.285 | 1.230 | 1.372 | n.s. |
| Health practices | −0.232 | 0.259 | 0.806 | 0.793 | n.s. |
| Understanding health as a state | 0.410 | 0.197 | 4.358 | 1.507 | 0.03 |
| Understanding health as an objective | 0.156 | 0.249 | 0.392 | 1.169 | n.s. |
| Understanding health as a process | 0.168 | 0.321 | 0.275 | 1.183 | n.s. |
| Understanding health as a property | 0.038 | 0.401 | 0.009 | 1.038 | n.s. |
| Understanding health as an outcome | −0.124 | 0.341 | 0.133 | 0.883 | n.s. |
| Internal health control | −0.027 | 0.032 | 0.720 | 0.973 | n.s. |
| The effect of other people on my health | −0.066 | 0.030 | 4.723 | 0.936 | 0.03 |
| The effect of chance on my health | 0.032 | 0.029 | 1.242 | 1.033 | n.s. |
| Gender (M) | −0.070 | 0.379 | 0.034 | 0.932 | n.s. |
| Constant | 1.683 | 1.470 | 1.311 | 5.382 | n.s. |
| Nagelkerke’s R2 = 14.4; Hosmer-Lemeshow χ2 (8) = 4.07; p = 0.851 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulik, A.; Kajka, N.; Dacka, M. Processes of a Transformation of Young Drivers’ Responsibility for Health—Carpe Diem. Int. J. Environ. Res. Public Health 2021, 18, 3634. https://doi.org/10.3390/ijerph18073634
Kulik A, Kajka N, Dacka M. Processes of a Transformation of Young Drivers’ Responsibility for Health—Carpe Diem. International Journal of Environmental Research and Public Health. 2021; 18(7):3634. https://doi.org/10.3390/ijerph18073634
Chicago/Turabian StyleKulik, Agnieszka, Natalia Kajka, and Monika Dacka. 2021. "Processes of a Transformation of Young Drivers’ Responsibility for Health—Carpe Diem" International Journal of Environmental Research and Public Health 18, no. 7: 3634. https://doi.org/10.3390/ijerph18073634
APA StyleKulik, A., Kajka, N., & Dacka, M. (2021). Processes of a Transformation of Young Drivers’ Responsibility for Health—Carpe Diem. International Journal of Environmental Research and Public Health, 18(7), 3634. https://doi.org/10.3390/ijerph18073634