
Interprofessional and Intraprofessional Communication about Older People’s Medications across Transitions of Care

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting and Sample
2.2. Ethical Considerations
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Transferring Setting: Interprofessional and Intraprofessional Medication Information Dissemination
3.1.1. Health Professionals’ Proactive Stance in Conveying Medication Information across Communication Channels
…we always ring to make sure the faxes have gone through (to the community pharmacist), that the information is there, and that they’re (community pharmacist) able to supply what we want. (Pharm5_GeriRehab3)
- Pharm4:
- Hello, I am just checking to see if my fax came through.
- Pharm4:
- OK. Thank you. (She waits for them to check).
- Pharm4:
- Wonderful! Now, I haven’t sent the script through yet. Because I just am waiting for the script from the doctors. So, I’ll do for one prazosin, BioMag® (magnesium) and then Nexium® (esomeprazole) 20 s.
- Pharm4:
- OK? Wonderful! Thank you so much. Bye. (Pharm4_Obs_Acute2)
We’d photocopied the medication chart for them (receiving hospital) but he’d (older patient) had some diarrhoea for about five days and we’d stopped giving him Coloxyl (docusate sodium) and senna and it was working a treat. I was a bit concerned that when he went there (other hospital), they’d just copy off the medication chart and start giving it to him again because no one looks at a photocopy once he gets back into the hospital. I mentioned that one in the verbal handover to XXX (receiving hospital) … “You could just stop it altogether because if it’s on the chart someone’s going to give it to him. He’s not constipated so he doesn’t need it.” Again if I hadn’t given that handover, that wouldn’t have happened. (RN14_Acute3)
RN7: We will either fax it to you or either a hard copy. … He is still the same… not much changes. Medications still crushed with puree … He is seen by the speech (speech pathologist) here and they put him on level 400. Otherwise, he is OK, saturating well in room air. (She was being asked some questions by the nursing home staff on the phone). Yes, yes. … So, I’ll copy the OBS (observations) chart, drug chart, discharge summary. (RN7_Obs_Acute2)
3.1.2. Health Professionals’ Lack of Familiarity with Unknown Settings
I try and include everything in my discharge summary, but whether or not the GP (general practitioner) is actually reading that and, I guess, understands fully about why we’ve done stuff. (Med1_Acute1)
I feel like it would be good to give the GP or the doctor who is looking after them, maybe a bit more information. But I think what happens is the discharge summary is faxed to the GP or someone, but I’m not entirely sure. (Pharm1_Acute1)
“If there’s something you really want checked on yeah, you call the GP and be like, “We’re looking at this, this is the story that’s happened,” if there’s something that you really don’t want to go wrong, you call the GP, but not every patient. So, that kind of hand over, which, I mean, maybe they should, but there’s maybe not time.” (Med3_GeriRehab3)
3.2. Receiving Setting: Interprofessional and Intraprofessional Communication for Safe Continuation of Medications
3.2.1. Surveillance and Investigation of Medication Incidents
The medication chart—it was from another ward—their midday dose, I think it was of their frusemide (furosemide) wasn’t given, well it wasn’t signed for, so we followed that exact process. Couldn’t chase up the nurse, because by the time we found it in the transfer it was the AM, and it was an agency nurse or something; it was not going to be followed up any time soon, anyway. So we did page the team. They came to review the patient clinically, ‘yes, looks overloaded, give the dose, it’s fine if we give extra’. (RN5_Acute1)
If they have come from another facility, it can be really hard to fix that. … If they have come from another hospital in a different city, out of state, out of country, then it’s much harder to call, because you have got to call the hospital, hopefully get put through to the ward that they were on, but because they are discharged from their hospital now, the switchboard can’t necessarily direct you to where they were, so you can’t necessarily find the right nurse to ask, it might not be their shift, they may not have any idea whether that medication was given. The doctors won’t know, because they don’t give the medication so chasing it up is really, really hard. (RN10_Acute2)
- RN6 (on phone to emergency nurse):
- It’s just that her NGT (nasogastric tube) is in, but there’s no proper documentation so we can’t use it [for medication administration]. Do you know who put the NGT in?
- RN6:
- Yeah so we can’t really use that in the ward. So it needs to be properly documented on the NGT form. By the nurse who inserted it, at what centimetre [for positioning] and all that stuff.
- RN6:
- We do have the forms here, if you could get the nurse who looked after her just to come up and fill out the forms, is that alright? (RN6_Obs_Acute2)
The pharmacist is sitting at a satellite station on the ward at the computer. She is reviewing the patient’s medication reconciliation form (MRF). (…) The pharmacist [then] stands up and opens the patient’s locked medication cupboard at the back of the satellite station. She takes out the patient’s medication bucket, which contains the patient’s regular medications in a red bag (hospital supplied to store patient’s own medications). The pharmacist opens the bag and looks at the medication containers and bottles. She opens some of the containers and appears to look at how many tablets are inside. The pharmacist replaces the medications and closes the cupboard. She collects the patient’s medication chart and walks to the next satellite station to find the intern [to discuss a medication issue identified]. (Pharm1_Acute1_FieldNotes)
So the medication was rivaroxaban, it’s used for AF (atrial fibrillation)—prevention of stroke. This patient came in with a stroke. So potentially, we could have prevented the stroke if the dose was appropriate. So apparently, it had been adjusted for their renal function in the past, which had been poor, but now their renal function was pretty much fine and they could have had their full dose. (Pharm1_Acute1)
So the one I’ve had is that the pack said that it should be metoprolol 50 mg BD, but what was being packed was actually 100 mg BD (two times daily), so it was double the dose. So then looking at first of all is the patient’s safety kind of thing, is that why the patient’s come into hospital and what can we do to fix that? And in this case, she was bradycardic and it potentially could have been why she was admitted. (Pharm2_Acute2)
Ahh, no that [prednisolone] shouldn’t be seven days. That’s wrong, so we don’t [want] them to stop it in seven days. No. No duration, thank you! (Pharm5_Obs_GeriRehab2)
3.2.2. Continuity of Medications from Transferring Settings
…when patients transfer, what we always do is we call them for a handover and we always say, “Could you please put in all the non-imprest (non-ward stocked) medication when they come here.” Because we’re not a major hospital … the pharmacy department don’t open 24/7. They probably close roughly about 5:30 so, we’ve got to make sure that all of that comes over with [the patient so]… on arrival to us, that it’s there. (RN20_GeriRehab4)
“We’re very lucky here that our pharmacists do a lot … for us so they will liaise with the actual chemist in the community to see what’s being dispensed to the patient and they will check the patient’s physical medications if they’ve got them” (Med2_FG_Acute).
So with the medical staff being so time-poor, they would chart whatever they felt were the most necessary medications at the time and not chart anything else, whereas as part of our credentialing process, we have to think about all the medications. … But even still, I would feel that the patients sort of arrive up on the ward and they’d still have a handful of medications still not charted. So it’s up to us to sort of follow-up on that and say ‘I know, it’s just magnesium (laugh) or Vitamin D. But for consistency, we need to carry on with these’. (Pharm3_Acute2)
We’ve had a few times where things (medications) have been left for a really long time. It’s simple things like eye drops and things that are really important to them (older patients) and things like that. We’re not getting them ordered and things so I just feel like we take a really more laid back approach. (RN11_Acute2)
RN17 (to nurse in charge): Ah! I forgot to tell the doctors. I’ll tell them to order him up some normal [eye] lubrication. I don’t think he’s got conjunctivitis. He’s just got the upturned eyelids, it looks irritated and dry. (RN17_Obs_GeriRehab4)
3.3. Real Time Communication: Barriers to Collaborative Interprofessional and Intraprofessional Communication
3.3.1. Discontinuous Nursing Handover Responsibilities
I guess if I’m not really familiar with that patient so if I’ve just come on to the shift and then I get handed the phone to hand over this patient that I’ve only just met and things. I guess I can look at the medication chart and things but if they (receiving nurse) ask specific questions then the answer might not 100% be correct. I feel sometimes when we ask that from other places as well you get the same sort of thing. A lot of time you say, “I’ve only just got handover on them. I’ve only just met them.” So I feel like that’s a really big barrier in some ways. (RN11_Acute2)
- The afternoon nurse:
- So, I’ve only just started my shift by the way.
- The ambulance attendant:
- Ok
- The afternoon nurse:
- So I’ve barely laid eyes on her (older patient). So she had this left intraparenchymal haemorrhage, which I’m not really that familiar with to be honest. She has got a history of AF (atrial fibrillation) there. Which I think she is on metoprolol for… (RN3_Obs_Acute1)
3.3.2. Missed Opportunities for Inclusive Communication to Manage Medications
I would say occasionally you might get the other pharmacist from the other team giving you a handover especially if there’s something to follow up. But that doesn’t happen all that often. Especially if it’s a surgical patient, they’re just like turfed to XXX (medical unit) and you might find out later on, ‘oh I’ve got a transfer of care’. You might be looking at your medication list on [electronic system] and then all of sudden there’s someone new and you think ‘Ugh! Where did they come from?!’ A lot of the pharmacists are in their medical teams WhatsApp groups, and so they’ll get notification often from that perspective, like take over of care from… (Pharm1_FG_Acute1)
- Pharm5 to doctor:
- Hi. He (older patient) is alright. He is not happy that he is not going home today. But I just said that the doctor will come and tell him that it is definitely tomorrow. I think if he gets that it’s definitely tomorrow then he’ll probably be ok.
- Doctor:
- It depends; he can go to home today to be honest.
- Pharm5:
- Really?
- Doctor:
- If Endo (endocrinology team) are happy with him.
- Pharm5:
- Oh. Ok. But the daughter?
- Doctor:
- The daughter is happy for him-
- Pharm5:
- Today?
- Doctor:
- Yeah, yeah, yeah.
- Pharm5:
- Oh.
- Doctor:
- She’s happy for him to go home today. She was happy for him to going yesterday.
- Pharm5:
- Oh, ok. Well then I should-
- Doctor:
- [Today or tomorrow]
- Pharm5:
- Alright. So, we are just waiting for Endo then..
- Doctor:
- Yeah.
- Pharm5:
- I’ll get some meds ready.
- Doctor:
- Yeah. Well-yeah.
- Pharm5:
- Well, I don’t know the- yeah. Ok. (Pharm5 to herself): (sighs) You wonder why patients get annoyed, I don’t know even know what’s going on. It says tomorrow. … Well (sighs)… anyway. … I’m going to get some scripts ready. (Pharm5_Obs_GeriRehab2)
Pharmacist asks question to the nurse what happen to him (older patient) and where he went. Nurse tells that the older patient was already discharged and was picked up by transfer staff minutes ago. Pharmacist becomes very upset and frustrated as she missed the opportunity to explain to the older patient about his medications. She decides that she will call the rehabilitation hospital where the patient was discharged (and contact pharmacists working there) and gives a handover to them over the phone. (Pharm4_Acute2_FieldNotes)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Commission on Safety and Quality in Health Care. Medication Reconciliation. 2019. Available online: https://www.safetyandquality.gov.au/our-work/medication-safety/medication-reconciliation (accessed on 30 November 2020).
- World Health Organisation. Medication Safety in Transitions of Care; World Health Organisation: Geneva, Switzerland, 2019. [Google Scholar]
- Sinvani, L.D.; Beizer, J.; Akerman, M.; Pekmezaris, R.; Nouryan, C.; Lutsky, L.; Cal, C.; Dlugacz, Y.; Masick, K.; Wolf-Klein, G. Medication reconciliation in continuum of care transitions: A moving target. J. Am. Med. Dir. Assoc. 2013, 14, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Tam, V.C.; Knowles, S.R.; Cornish, P.L.; Fine, N.; Marchesano, R.; Etchells, E.E. Frequency, type and clinical importance of medication history errors at admission to hospital: A systematic review. CMAJ 2005, 173, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.E.; Roane, T.E.; McLin, K.D. Reduction of 30-Day Hospital Readmissions After Patient-centric Telephonic Medication Therapy Management Services. Hosp. Pharm. 2016, 51, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Jamjoom, O.; Marupuru, S.; Taylor, A.M.; Warholak, T.; Scovis, N.; Bingham, J.M. Evaluating provider acceptance of pharmacist interventions in the Discharge Companion Program and its association with readmission reduction. J. Am. Pharm. Assoc. (2003) 2020, 60, e47–e51. [Google Scholar] [CrossRef]
- Leotsakos, A.; Zheng, H.; Croteau, R.; Loeb, J.M.; Sherman, H.; Hoffman, C.; Morganstein, L.; O’Leary, D.; Bruneau, C.; Lee, P.; et al. Standardization in patient safety: The WHO High 5s project. Int. J. Qual. Health Care 2014, 26, 109–116. [Google Scholar] [CrossRef]
- Dickinson, D.T.; Rashid, S.; Weiland, A.; Tjoa, T.; Kim, D.S.; Huang, S.S. Errors in antibiotic transitions between hospital and nursing home: How often do they occur? Infect. Control Hosp. Epidemiol. 2019, 40, 1416–1419. [Google Scholar] [CrossRef]
- Achilleos, M.; McEwen, J.; Hoesly, M.; DeAngelo, M.; Jennings, T. Pharmacist-led program to improve transitions from acute care to skilled nursing facility care. Am. J. Health Syst. Pharm. 2020, 77, 979–984. [Google Scholar] [CrossRef]
- Martirosov, A.L.; Smith, Z.R.; Hencken, L.; MacDonald, N.C.; Griebe, K.; Fantuz, P.; Grafton, G.; Hegab, S.; Ismail, R.; Jackson, B.; et al. Improving transitions of care for critically ill adult patients on pulmonary arterial hypertension medications. Am. J. Health Syst. Pharm. 2020, 77, 958–965. [Google Scholar] [CrossRef]
- Evans, D.; Usery, J. Implementation and Assessment of a Pharmacy-Led Inpatient Transitions of Care Program. South Med. J. 2020, 113, 320–324. [Google Scholar] [CrossRef]
- Guilcher, S.J.T.; Fernandes, O.; Luke, M.J.; Wong, G.; Lui, P.; Cameron, K.; Pariser, P.; Raco, V.; Kak, K.; Varghese, S.; et al. A developmental evaluation of an intraprofessional Pharmacy Communication Partnership (PROMPT) to improve transitions in care from hospital to community: A mixed-methods study. BMC Health Serv. Res. 2020, 20, 99. [Google Scholar] [CrossRef]
- Ozavci, G.; Bucknall, T.; Woodward-Kron, R.; Hughes, C.; Jorm, C.; Joseph, K.; Manias, E. A systematic review of older patients’ experiences and perceptions of communication about managing medication across transitions of care. Res. Soc. Adm. Pharm. 2020. [Google Scholar] [CrossRef]
- Manias, E.; Bucknall, T.; Hughes, C.; Jorm, C.; Woodward-Kron, R. Family involvement in managing medications of older patients across transitions of care: A systematic review. BMC Geriatr. 2019, 19, 95. [Google Scholar] [CrossRef]
- Glintborg, B.; Andersen, S.E.; Dalhoff, K. Insufficient communication about medication use at the interface between hospital and primary care. Qual. Saf. Health Care 2007, 16, 34–39. [Google Scholar] [CrossRef]
- Patterson, M.E.; Foust, J.B.; Bollinger, S.; Coleman, C.; Nguyen, D. Inter-facility communication barriers delay resolving medication discrepancies during transitions of care. Res. Soc. Adm. Pharm. 2019, 15, 366–369. [Google Scholar] [CrossRef]
- Manias, E.; Gerdtz, M.; Williams, A.; Dooley, M. Complexities of medicines safety: Communicating about managing medicines at transition points of care across emergency departments and medical wards. J. Clin. Nurs. 2015, 24, 69–80. [Google Scholar] [CrossRef]
- Redmond, P.; Munir, K.; Alabi, O.; Grimes, T.; Clyne, B.; Hughes, C.; Fahey, T. Barriers and facilitators of medicines reconciliation at transitions of care in Ireland—A qualitative study. BMC Fam. Pract. 2020, 21, 116. [Google Scholar] [CrossRef]
- Manias, E.; Gerdtz, M.; Williams, A.; McGuiness, J.; Dooley, M. Communicating about the management of medications as patients move across transition points of care: An observation and interview study. J. Eval. Clin. Pract. 2016, 22, 635–643. [Google Scholar] [CrossRef]
- Liu, W.; Manias, E.; Gerdtz, M. Medication communication through documentation in medical wards: Knowledge and power relations. Nurs. Inq. 2014, 21, 246–258. [Google Scholar] [CrossRef]
- Rixon, S.; Braaf, S.; Williams, A.; Liew, D.; Manias, E. Pharmacists’ Interprofessional Communication About Medications in Specialty Hospital Settings. Health Commun. 2015, 30, 1065–1075. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care. Medication Reconciliation Resources and Tools. 2019. Available online: https://www.safetyandquality.gov.au/our-work/medication-safety/medication-reconciliation/medication-reconciliation-resources-and-tools (accessed on 20 November 2020).
- Burawoy, M. Revisits: An outline of a theory of reflexive ethnography. Am. Sociol. Rev. 2003, 68, 645–679. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- QSR International. NVivo Qualitative Data Analysis Software; QSR International: Chadstone, VIC, Australia, 2018. [Google Scholar]
- Coiera, E. Communication systems in healthcare. Clin. Biochem. Rev. 2006, 27, 89–98. [Google Scholar]
- Riley, R.; Forsyth, R.; Manias, E.; Iedema, R. Whiteboards: Mediating professional tensions in clinical practice. Commun. Med. 2007, 4, 165–175. [Google Scholar] [CrossRef]
- Pantilat, S.Z.; Lindenauer, P.K.; Katz, P.P.; Wachter, R.M. Primary care physician attitudes regarding communication with hospitalists. Am. J. Med. 2001, 111, 15–20. [Google Scholar] [CrossRef]
- Van Walraven, C.; Seth, R.; Laupacis, A. Dissemination of discharge summaries. Can. Fam. Physician 2002, 48, 737–742. [Google Scholar]
- Jones, C.D.; Vu, M.B.; O’Donnell, C.M.; Anderson, M.E.; Patel, S.; Wald, H.L.; Coleman, E.A.; DeWalt, D.A. A failure to communicate: A qualitative exploration of care coordination between hospitalists and primary care providers around patient hospitalizations. J. Gen. Intern. Med. 2015, 30, 417–424. [Google Scholar] [CrossRef]
- Pham, H.H.; Grossman, J.M.; Cohen, G.; Bodenheimer, T. Hospitalists and care transitions: The divorce of inpatient and outpatient care. Health Aff. (Millwood) 2008, 27, 1315–1327. [Google Scholar] [CrossRef]
- Pinelli, V.; Stuckey, H.L.; Gonzalo, J.D. Exploring challenges in the patient’s discharge process from the internal medicine service: A qualitative study of patients’ and providers’ perceptions. J. Interprof. Care 2017, 31, 566–574. [Google Scholar] [CrossRef]
- Tobiano, G.; Ting, C.; Ryan, C.; Jenkinson, K.; Scott, L.; Marshall, A.P. Front-line nurses’ perceptions of intra-hospital handover. J. Clin. Nurs. 2020, 29, 2231–2238. [Google Scholar] [CrossRef]
- Hilligoss, B.; Cohen, M.D. The unappreciated challenges of between-unit handoffs: Negotiating and coordinating across boundaries. Ann. Emerg. Med. 2013, 61, 155–160. [Google Scholar] [CrossRef]
- Slawomirski, L.; Klazinga, N. The Economics of Patient Safety, from Analysis to Action; OECD: Paris, France, 2020. [Google Scholar]
- Wilson, A.J.; Palmer, L.; Levett-Jones, T.; Gilligan, C.; Outram, S. Interprofessional collaborative practice for medication safety: Nursing, pharmacy, and medical graduates’ experiences and perspectives. J. Interprof. Care 2016, 30, 649–654. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Semi-Structured Health Professional Interview Schedule |
|---|
Examples of interview questions:
|
| Observations schedule |
|
| Focus Group interviews |
| Quotation excerpts of communication practices and interactions from interviews and observations were read to participants. Participants were asked to reflect on these existing practices and to consider possible strategies for improvement [23]. |
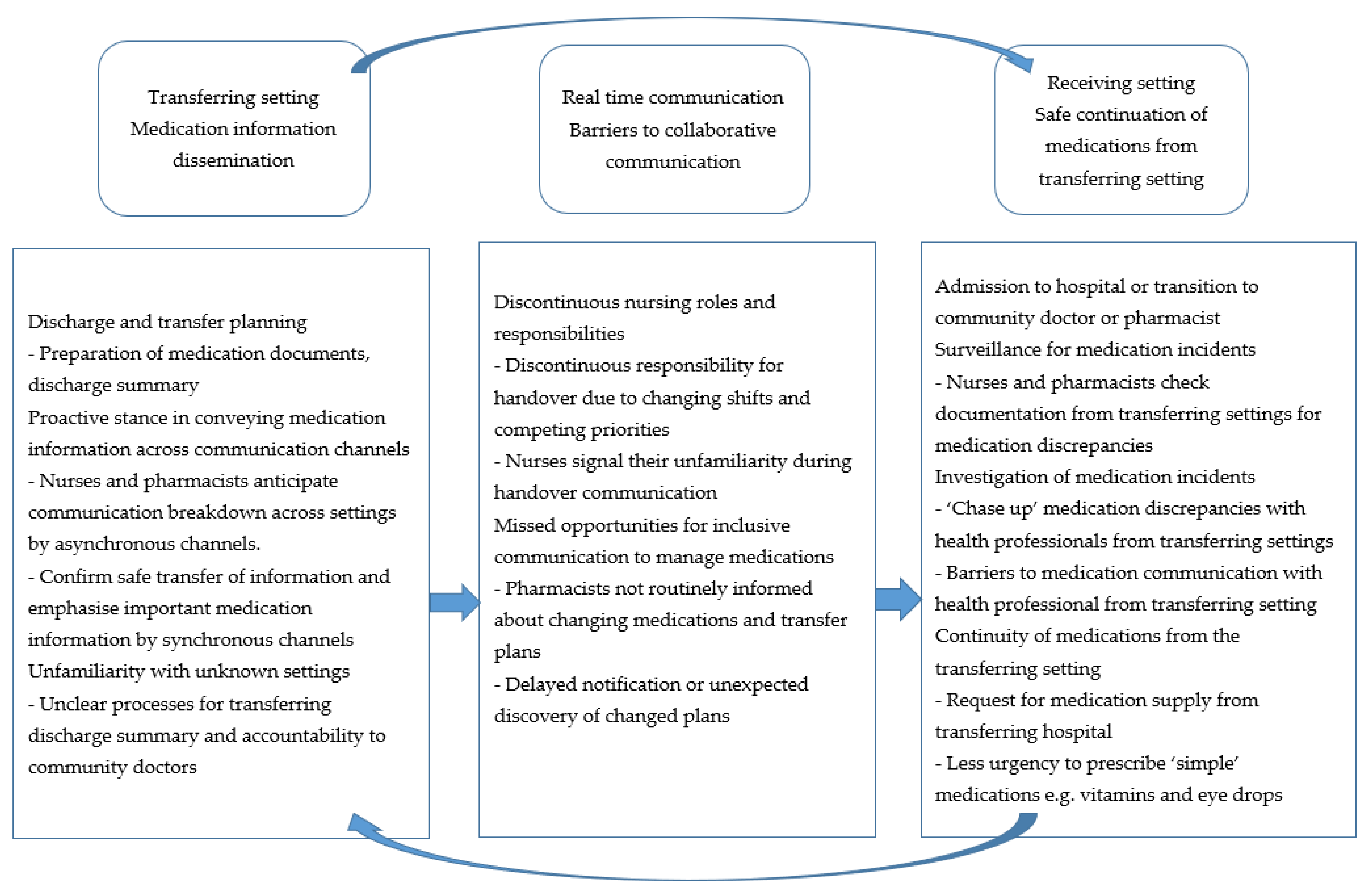
| Themes | Transferring Setting: Medication Information Dissemination | ‘Real-Time’: Barriers to Collaborative Communication | Receiving Setting: Safe Continuation of Medications from Transferring Setting |
|---|---|---|---|
| Sub Themes | 1. Proactive stance in conveying medication information across communication channels 2. Unfamiliarity with unknown settings | 1. Discontinuous nursing roles and responsibilities 2. Missed opportunities for inclusive communication to manage medications | 1. Surveillance and investigation of medication incidents 2. Continuity of medications from transferring settings |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manias, E.; Bucknall, T.; Woodward-Kron, R.; Hughes, C.; Jorm, C.; Ozavci, G.; Joseph, K. Interprofessional and Intraprofessional Communication about Older People’s Medications across Transitions of Care. Int. J. Environ. Res. Public Health 2021, 18, 3925. https://doi.org/10.3390/ijerph18083925
Manias E, Bucknall T, Woodward-Kron R, Hughes C, Jorm C, Ozavci G, Joseph K. Interprofessional and Intraprofessional Communication about Older People’s Medications across Transitions of Care. International Journal of Environmental Research and Public Health. 2021; 18(8):3925. https://doi.org/10.3390/ijerph18083925
Chicago/Turabian StyleManias, Elizabeth, Tracey Bucknall, Robyn Woodward-Kron, Carmel Hughes, Christine Jorm, Guncag Ozavci, and Kathryn Joseph. 2021. "Interprofessional and Intraprofessional Communication about Older People’s Medications across Transitions of Care" International Journal of Environmental Research and Public Health 18, no. 8: 3925. https://doi.org/10.3390/ijerph18083925
APA StyleManias, E., Bucknall, T., Woodward-Kron, R., Hughes, C., Jorm, C., Ozavci, G., & Joseph, K. (2021). Interprofessional and Intraprofessional Communication about Older People’s Medications across Transitions of Care. International Journal of Environmental Research and Public Health, 18(8), 3925. https://doi.org/10.3390/ijerph18083925