
Burnout and Its Relationship with Demographic and Job-Related Variables among Dentists in Lithuania: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Participants and Data Collection
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Demographic and Job-Related Characteristics
3.2. Job Satisfaction
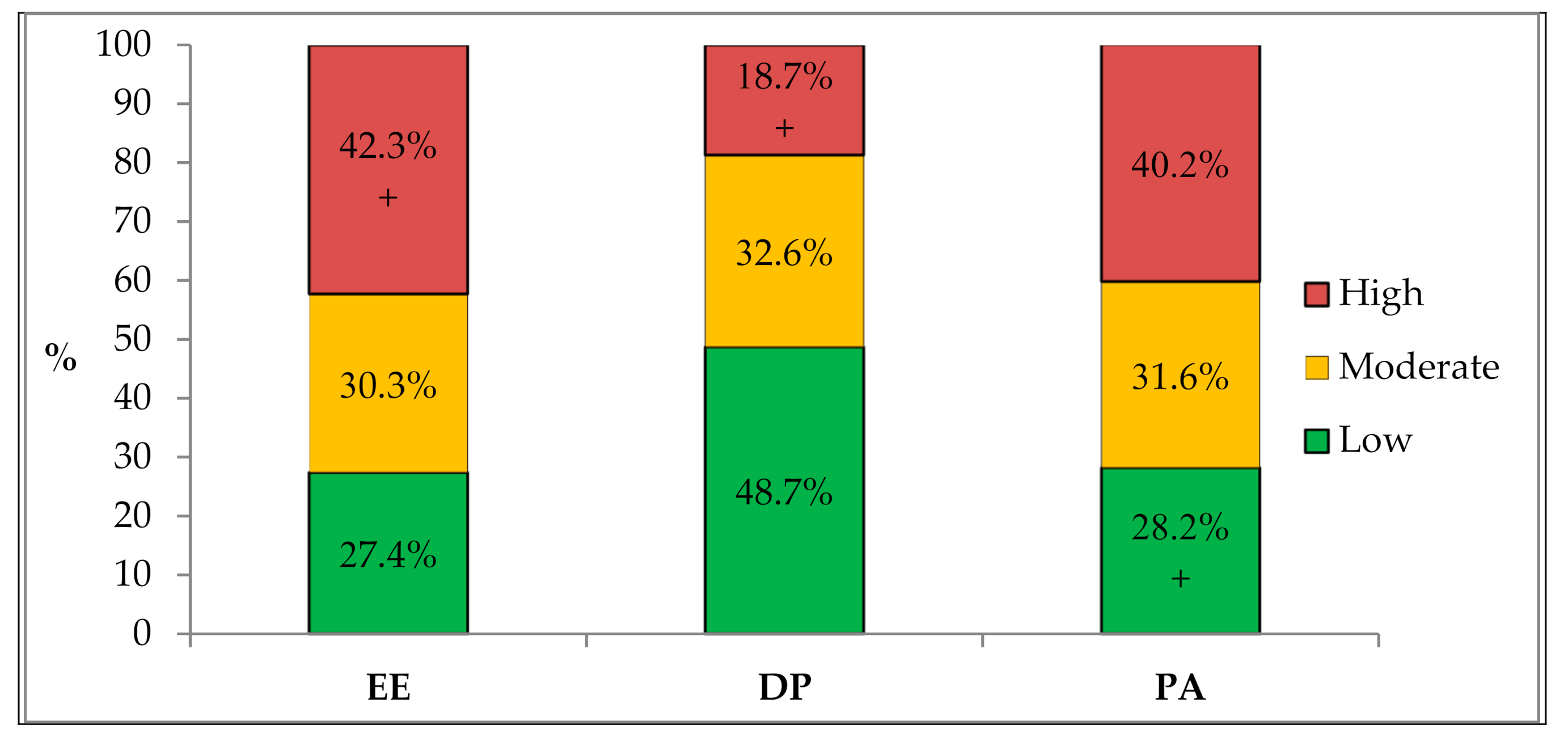
3.3. Maslach Burnout Inventory and Level of Burnout
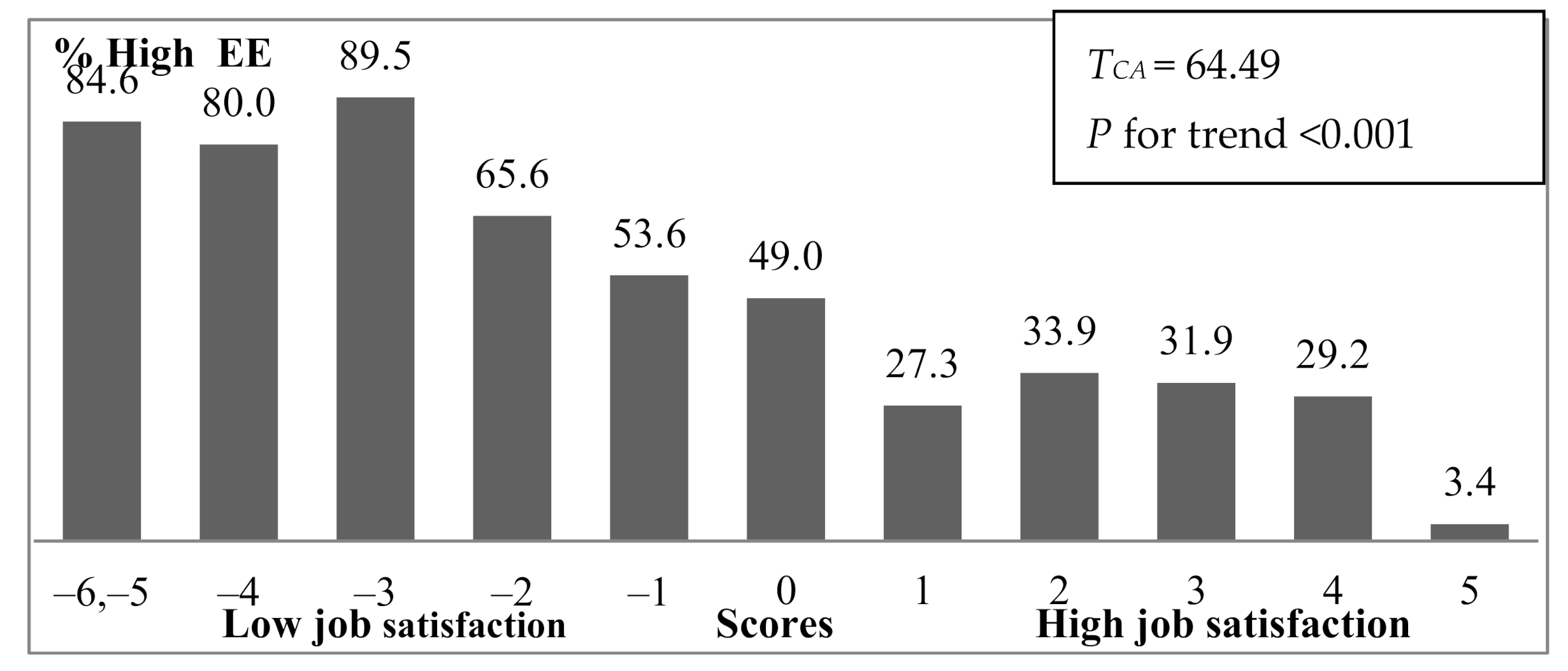
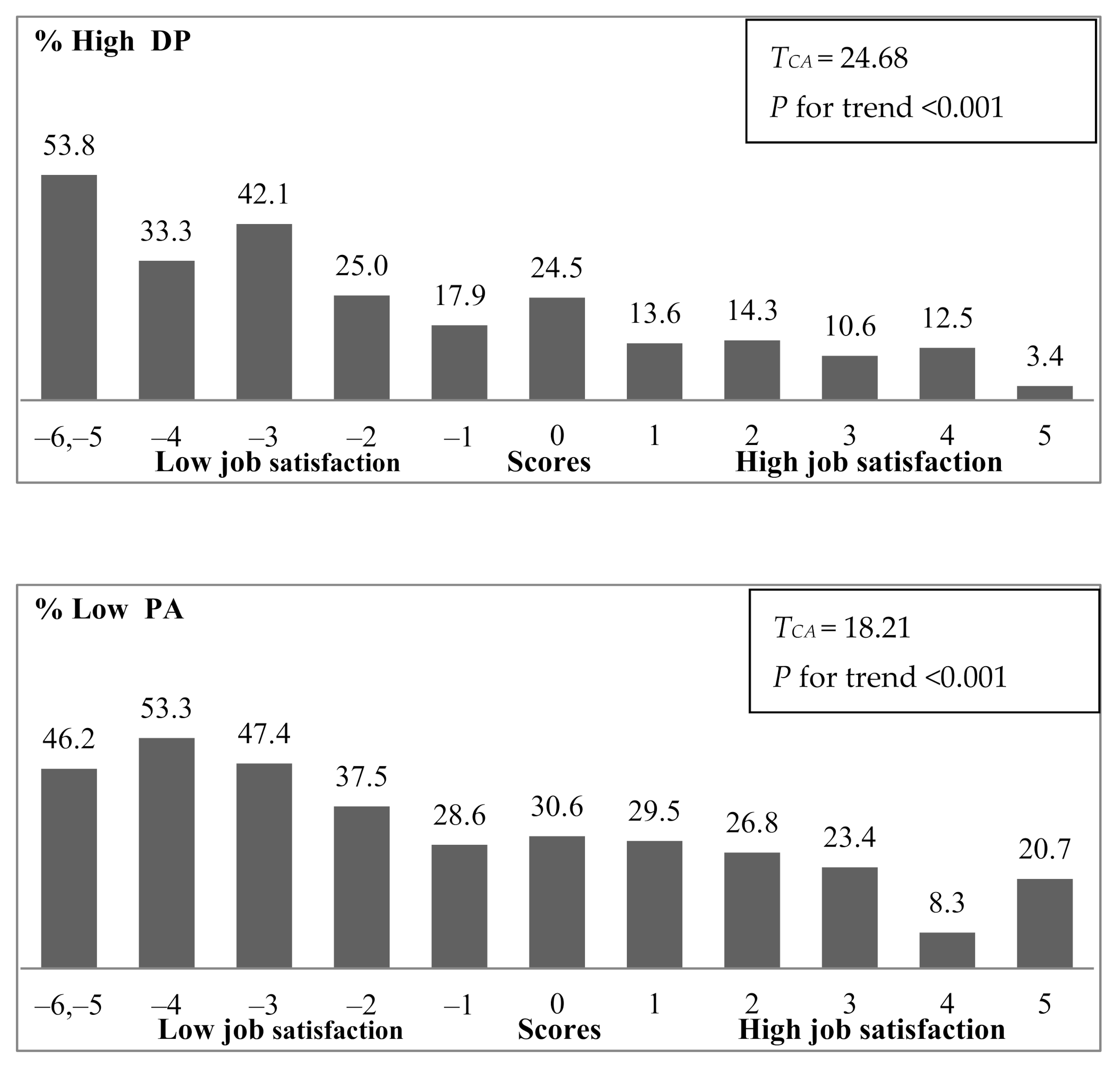
3.4. Maslach Burnout Inventory and Job Satisfaction
3.5. Relationship of Burnout Level with Demographic and Job-Related Variables
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| DP | Depersonalization |
| EE | Emotional exhaustion |
| MBI | Maslach Burnout Inventory |
| PA | Personal accomplishment |
| RSSM | Ration of sum score means |
| SD | Standard deviation |
References
- O’Dowd, A. Doctors’ leaders call for warning system for GP burnout. BMJ 2015, 351, h4152. [Google Scholar] [CrossRef] [PubMed]
- Rothenberger, D.A. Physician burnout and well-being: A systematic review and framework for action. Dis. Colon. Rectum 2017, 60, 567–576. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ireland, E.J. Dental practice burnout. Compend. Contin. Educ. Dent. 1983, 4, 367–369. [Google Scholar] [PubMed]
- Willey, J.L. Dental burnout. J. Dent. Pract. Adm. 1987, 4, 108–111. [Google Scholar]
- Deshmukh, S.V. Burnout in dentistry: A myth or reality. J. Int. Clin. Dent. Res. Organ. 2019, 11, 1–2. Available online: https://www.jicdro.org/temp/JIntClinDentResOrgan1111-8065239_222412.pdf (accessed on 26 January 2021). [CrossRef]
- Puriene, A.; Janulyte, V.; Musteikyte, M.; Bendinskaite, R. General health of dentists. Literature review. Stomatologija 2007, 9, 10–20. Available online: https://pubmed.ncbi.nlm.nih.gov/17449973/ (accessed on 26 January 2021).
- Choy, H.B.; Wong, M.C. Occupational stress and burnout among Hong Kong dentists. Hong Kong Med. J. 2017, 23, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Toon, M.; Collin, V.; Whitehead, P.; Reynold, L. An analysis of stress and burnout in UK general dental practitioners: Subdimensions and causes. Br. Dent. J. 2019, 226, 125–130. [Google Scholar] [CrossRef]
- Rada, R.E.; Johnson-Leong, C. Stress, burnout, anxiety and depression among dentists. J. Am. Dent. Assoc. 2004, 135, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Wu, J.-H.; Du, L.-K. Work stress and occupational burnout among dental staff in a medical center. J. Dent. Sci. 2019, 14, 295–301. [Google Scholar] [CrossRef]
- Dwivedi, A.; Purohit, B.M.; Bhambal, A. Is dentistry turning into weary profession? Dimensionality of experienced professional burnout among dentists in Central India. J. Dent. Oro. Surg. 2016, 1, 122. Available online: https://www.elynspublishing.com/journal/article/is-dentistry-turning-into-weary-profession-dimensionality-of-experienced-professional-burnout-among-dentists-in-central-india (accessed on 26 January 2021). [CrossRef] [Green Version]
- Strange, M. Burnout and Patient Safety. 2020. Available online: https://www.airtechniques.com/en/burnout-and-patient-safety/ (accessed on 26 January 2021).
- Panagioti, M.; Geraghty, K.; Johnson, J.; Zhou, A.; Panagopoulou, E.; Chew-Graham, C.; Peters, D.; Hodkinson, A.; Riley, R.; Esmail, A. Association between physician burnout and patient safety, professionalism, and patient satisfaction: A systematic review and meta-analysis. JAMA Intern. Med. 2018, 178, 1317–1331. [Google Scholar] [CrossRef]
- Denton, D.A.; Newton, J.T.; Bower, E.J. Occupational burnout and work engagement: A national survey of dentists in the United Kingdom. Br. Dent. J. 2008, 205, E13; discussion 382–383. [Google Scholar] [CrossRef] [Green Version]
- Jin, M.U.; Jeong, S.H.; Kim, E.K.; Choi, Y.H.; Song, K.B. Burnout and its related factors in Korean dentists. Int. Dent. J. 2015, 65, 22–31. [Google Scholar] [CrossRef]
- Jugale, P.V.; Mallaiah, P.; Krishnamurthy, A.; Sangha, R. Burnout and work engagement among dental practitioners in Bangalore city: A cross-sectional study. J. Clin. Diagn. Res. 2016, 10, ZC63–ZC67. [Google Scholar] [CrossRef]
- Calvo, J.M.; Kwatra, J.; Yansane, A.; Tokede, O.; Gorter, R.C.; Kalenderian, E. Burnout and work engagement among US dentists. J. Patient Saf. 2017. [Google Scholar] [CrossRef]
- Carneiro, S.D.R.M.; Tourinho, C.C.; Pedrosa do Vale, T.A.; Campêlo, Y.S.G.; Gomes, F.A.; Lima, D.L.F. Burnout syndrome: Evaluation in dentists in the city of Fortaleza, Brazil. RSBO Online 2013, 10, 266–271. Available online: http://revodonto.bvsalud.org/pdf/rsbo/v10n3/a12v10n3.pdf (accessed on 26 January 2021).
- Janulyte, V.; Aleksejuniene, J.; Puriene, A.; Peciuliene, V.; Benzian, H. Current employment characteristics and career intentions of Lithuanian dentists. Hum. Resour Health 2014, 12, 74. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Occupational. Behav. 1981, 2, 99–113. Available online: https://onlinelibrary.wiley.com/doi/epdf/10.1002/job.4030020205 (accessed on 26 January 2021). [CrossRef]
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of burnout among physicians: A systematic review. JAMA 2018, 320, 1131–1150. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Jackson, S.; Leiter, M. The Maslach Burnout Inventory Manual, 4th ed.; Ming Garden, Inc.: Menio Park, CA, USA, 2016. [Google Scholar]
- García-Arroyo, J.A.; y Osca, A. Effect sizes and cut-off points: A meta-analytical review on burnout in latin American countries. Psychol. Health Med. 2018, 23, 1079–1093. [Google Scholar] [CrossRef]
- Huri, M.; Bağış, N.; Şahin, S.; Eren, H.; Orhan, K. Factors associated with burnout in dentistry from occupational therapy perspective: A systematic review. J. ARSA Actual Res. Sci. Acad. 2017, 2, 10–15. Available online: https://www.researchgate.net/publication/315743851_Factors_Associated_with_Burnout_in_Dentistry_from_Occupational_Therapy_Perspective_A_Systematic_Review (accessed on 26 March 2021).
- Leiter, M.P.; Maslach, C. Latent burnout profiles: A new approach to understanding the burnout experience. Burn Res. 2016, 3, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Stewart, M.T.; Reed, S.; Reese, J.; Galligan, M.M.; Mahan, J.D. Conceptual models for understanding physician burnout, professional fulfillment, and well-being. Curr. Probl. Pediatr. Adolesc. Health Care 2019, 49, 100658. [Google Scholar] [CrossRef]
- Zhang, X.J.; Song, Y.; Jiang, T.; Ding, N.; Shi, T.Y. Interventions to reduce burnout of physicians and nurses: An overview of systematic reviews and meta-analyses. Med. Baltim. 2020, 26, e20992. [Google Scholar] [CrossRef]
- Guthier, C.; Dormann, C.; Voelkle, M.C. Reciprocal effects between job stressors and burnout: A continuous time meta-analysis of longitudinal studies. Psychol Bull. 2020, 146, 1146–1173. [Google Scholar] [CrossRef]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [Green Version]
- Žutautienė, R.; Radišauskas, R.; Kalinienė, G.; Ustinavičienė, R. The prevalence of burnout and its associations with psychosocial work environment among Kaunas region (Lithuania) hospitals’ physicians. Int. J. Environ. Res. Public Health 2020, 17, 3739. [Google Scholar] [CrossRef]
- Skorobogatova, N.; Žemaitienė, N.; Šmigelskas, K.; Tamelienė, R. Professional burnout and concurrent health complaints in neonatal nursing. Open Med. 2017, 12, 328–334. [Google Scholar] [CrossRef] [Green Version]
- Mikalauskas, A. Burnout among Lithuanian Anesthetists and Intensive Care Physiciants. Ph.D. Thesis, Lithuanian University of Health Sciences, Kaunas, Lithuania, 2018. [Google Scholar]
- Gorter, R.C.; Eijkman, M.A.; Hoogstraten, J. Burnout and health among Dutch dentists. Eur. J. Oral. Sci 2000, 108, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinval, J.; Marôco, J. Short index of job satisfaction: Validity evidence from Portugal and Brazil. PLoS ONE 2020, 15, e0231474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiredo-Ferraz, H.; Grau-Alberola, E.; Gil-Monte, P.R.; García-Juesas, J.A. Burnout and job satisfaction among nursing professionals. Psicothema 2012, 24, 271–276. Available online: https://pubmed.ncbi.nlm.nih.gov/22420356/ (accessed on 26 January 2021). [PubMed]
- Mijakoski, D.; Karadzinska-Bislimovska, J.; Basarovska, V.; Stoleski, S.; Minov, J. Burnout and work demands predict reduced job satisfaction in health professionals working in a surgery clinic. Open Access Maced. J. Med. Sci. 2015, 3, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Gorter, R.C.; Freeman, R. Burnout and engagement in relation with job demands and resources among dental staff in Northern Ireland. Community Dent. Oral. Epidemiol. 2011, 39, 87–95. [Google Scholar] [CrossRef]
- Karanika-Murray, M.; Duncan, N.; Pontes, H.M.; Griffiths, M.D. Organizational identification, work engagement, and job satisfaction. J. Manag. Psychol. 2015, 30, 1019–1033. [Google Scholar] [CrossRef]
- Rosales, R.A.; Labrague, L.J.; Rosales, G.L. Nurses’ job satisfaction and burnout: Is there a connection? Int. J. Adv. Nurs. Stud. 2013, 2, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Puriene, A.; Petrauskiene, J.; Janulyte, V.; Balciuniene, I. Factors related to job satisfaction among Lithuanian dentists. Stomatologija 2007, 9, 109–113. Available online: http://europepmc.org/article/med/18303275 (accessed on 26 January 2021).
- G* Power 3.1 Manual. 1 March 2017. Available online: https://www.psychologie.hhu.de/fileadmin/redaktion/Fakultaeten/Mathematisch-Naturwissenschaftliche_Fakultaet/Psychologie/AAP/gpower/GPower3-BRM-Paper.pdf (accessed on 21 February 2021).
- Čekanavičius, V.; Murauskas, G. Taikomoji Regresinė Analizė Socialiniuose Tyrimuose [Applied Regression Analysis in Social Sciences]; Vilnius University: Vilnius, Lithuania, 2014; Available online: http://www.statistika.mif.vu.lt/wp-content/uploads/2014/04/regresine-analize.pdf (accessed on 26 January 2021).
- Hayat, M.J.; Higgins, M. Understanding Poisson regression. J. Nurs. Educ. 2014, 53, 207–215. [Google Scholar] [CrossRef]
- Slabšinskienė, E.; Gorelik, A.; Vasiliauskienė, I.; Kavaliauskienė, A.; Zaborskis, A. Factorial validity and variance of the Maslach Burnout Inventory between demographic and workload groups among dentists of Lithuania. Int. J. Environ. Res. Public Health 2020, 17, 9154. [Google Scholar] [CrossRef]
- Zini, A.; Zaken, Y.; Ovadia-Gonen, H.; Mann, J.; Vered, Y. Burnout level among general and specialist dentists: A global manpower concern. Occup. Med. Health Aff. 2013, 1, 5. [Google Scholar] [CrossRef]
- Puriene, A.; Aleksejuniene, J.; Petrauskiene, J.; Balciuniene, I.; Janulyte, V. Self-perceived mental health and job satisfaction among Lithuanian dentists. Ind. Health 2008, 46, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnot Inventory Manual, 3rd ed.; Consulting Psychologists Press, Inc.: Palo Alto, CA, USA, 1996. [Google Scholar]
- Moksony, F.; Hegedus, R. The use of Poisson regression in the sociological study of suicide. Corvinus J. Sociol. Soc. Policy 2014, 5, 97–114. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Aulak, D.S.; Mangat, S.S.; Aulak, M.S. Systematic review: Factors contributing to burnout in dentistry. Occup. Med. Lond. 2016, 66, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Schaufeli, W.B.; Desart, S.; De Witte, H. Burnout Assessment Tool (BAT)—development, validity, and reliability. Int. J. Environ. Res. Public Health 2020, 17, 9495. [Google Scholar] [CrossRef]
- Spagnoli, P.; Buono, C.; Kovalchuk, L.S.; Cordasco, G.; Esposito, A. Perfectionism and burnout during the COVID-19 crisis: A two-wave cross-lagged study. Front. Psychol. 2021, 11, 4087. [Google Scholar] [CrossRef]
- Schaufeli, W.; Leiter, M.; Maslach, C. Burnout: 35 Years of research and practice. Career Dev. Int 2009, 14, 204–220. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Mindgarden. The Problem with Cut-Offs for the Maslach Burnout Inventory. 2018. Available online: https://www.mindgarden.com/documents/MBI-Cutoff-Caveat.pdf (accessed on 26 January 2021).
- Bianchini-Mataramoros, M. El síndrome del Burnout en personal profesional de la salud. Med. Leg Costa Rica 1997, 13–14, 189–192. Available online: http://www.scielo.sa.cr/scielo.php?script=sci_arttext&pid=S1409-00151997000200017&lng=en&nrm=iso (accessed on 26 January 2021).
- Gorter, R.C. Burnout among Dentists: Identification and Prevention. Ph.D. Thesis, University of Amsterdam, Amsterdam, The Netherlands, 2000. [Google Scholar]
- Alzahem, A.M.; Alhaizan, Y.A.; Algudaibi, L.Y.; Albani, R.M.; Aljuraisi, A.M.; Alaqeel, M.K. Stress and burnout among dental staff. Imam J. Appl. Sci. 2020, 5, 9–15. Available online: https://www.e-ijas.org/article.asp?issn=2589-0603;year=2020;volume=5;issue=1;spage=9;epage=15;aulast=Alzahem (accessed on 26 January 2021).
- Te Brake, H.J.H.M. Burnout and Job Engagement in Dentistry. PhD Thesis, University of Amsterdam, Amsterdam, The Netherlands, 2005. [Google Scholar]
- Gorter, R.C.; Eijkman, M.A.; Hoogstraten, J. A career counselling program for dentists: Effects on burnout. Patient Educ. Couns. 2001, 43, 23–30. [Google Scholar] [CrossRef]
- Molina-Hernández, J.; Fernández-Estevan, L.; Montero, J.; González-García, L. Work environment, job satisfaction and burnout among Spanish dentists: A cross-sectional study. BMC Oral. Health 2021, 21, 156. [Google Scholar] [CrossRef] [PubMed]
- Levin, K.A. Study design III: Cross-sectional studies. Evid. Based Dent. 2006, 7, 24–25. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. (%) or Mean (SD) of Respondents | |
|---|---|---|
| Gender (n = 380) | ||
| Male | 58 | (15.3) |
| Female | 322 | (84.7) |
| Age (years) (n = 374) | ||
| Mean and standard deviation | 37.3 | (12.9) |
| < 40 | 248 | (66.3) |
| ≥ 40 | 126 | (33.7) |
| Marital status (n = 376) | ||
| Married | 223 | (59.3) |
| Never married | 119 | (31.6) |
| Divorced / widow | 34 | (9.0) |
| Number of children (n = 377) | ||
| No children | 177 | (46.9) |
| Have children | 200 | (52.6) |
| Work practice experience (n = 365) | ||
| Mean and standard deviation | 12.8 | (12.3) |
| <10 | 196 | (53.7) |
| ≥10 | 169 | (46.3) |
| Working in several places (n = 372) | ||
| In one clinic only | 183 | (49.2) |
| In two or more clinics | 189 | (50.8) |
| Type of practice (n = 378) | ||
| Public | 59 | (15.6) |
| Private | 213 | (56.3) |
| Both | 106 | (28.1) |
| Property of the clinic (for private practice only) (n = 329) | ||
| Commercial network | 79 | (24.0) |
| Individual (small) clinics) | 250 | (76.0) |
| Specialist status (n = 380) | ||
| General dental practitioners | 278 | (73.7) |
| Specialists | 102 | (26.3) |
| Number of working hours per week (n = 371) | ||
| Mean and standard deviation | 36.7 | (12.2) |
| ≤40 | 257 | (69.3) |
| >40 | 114 | (30.7) |
| Number of working days per week (n = 376) | ||
| <5 | 83 | (21.8) |
| ≥5 | 293 | (77.1) |
| Characteristics | No. (%) of Respondents | Scores Given | |
|---|---|---|---|
| Do you think you are earning enough given your workload and efforts? (n = 378) | |||
| Really enough | 113 | (29.9) | +1 |
| O.K., though I would like to earn more | 185 | (48.9) | 0 |
| My earning is insufficient / low | 80 | (21.2) | −1 |
| Do you feel sufficiently respected and valued by your colleagues in the clinic or in a professional group? (n = 378) | |||
| Yes | 274 | (72.5) | +1 |
| No | 39 | (10.3) | −1 |
| I never thought about it | 65 | (17.2) | 0 |
| Do you feel sufficiently respected and appreciated by the head of clinic? (n = 374) | |||
| Yes | 209 | (55.9) | +1 |
| No | 70 | (18.7) | −1 |
| I never thought about it | 51 | (13.6) | 0 |
| I myself am the head of the clinic | 44 | (11.8) | 0 |
| How do you assess the microclimate in your workplace? (n = 376) | |||
| I like the atmosphere at work, I don’t feel any stress about it | 167 | (44.4) | +1 |
| The atmosphere at work is quite normal, but of the atmosphere at work I sometimes feel stress | 174 | (46.3) | −1 |
| I don’t like the atmosphere at work because it causes a lot of stress | 25 | (6.6) | −2 |
| The atmosphere at work does not affect my mood and well-being | 10 | (2.7) | 0 |
| Would you recommend the profession of dentist to an undecided young person? (n = 377) | |||
| Yes | 131 | (34.7) | +1 |
| No | 124 | (32.9) | −1 |
| I can’t reply | 122 | (32.4) | 0 |
| No. of Scores | No. (%) of Respondents | |||||
|---|---|---|---|---|---|---|
| Total Sample (n = 374) | Ordinary Dentists (n = 330) | Heads of the Dental Clinic (n = 44) | ||||
| −6 | 3 | (0.8) | 3 | (0.9) | - | |
| −5 | 10 | (2.7) | 8 | (2.4) | 2 | (4.5) |
| −4 | 15 | (4.0) | 15 | (4.5) | 0 | (0.0) |
| −3 | 19 | (5.1) | 16 | (4.8) | 3 | (6.8) |
| −2 | 32 | (8.6) | 30 | (9.1) | 2 | (4.5) |
| −1 | 28 | (7.5) | 22 | (6.7) | 6 | (13.6 |
| 0 | 46 | (12.3) | 40 | (12.1) | 6 | (13.6) |
| +1 | 43 | (11.5) | 37 | (11.2) | 6 | (13.6) |
| +2 | 55 | (14.7) | 47 | (14.2) | 8 | (18.2) |
| +3 | 46 | (12.7) | 40 | (12.1) | 6 | (13.6) |
| +4 | 48 | (12.8) | 43 | (13.0) | 5 | (11.4) |
| +5 | 29 | (7.8) | 29 | (8.8) | - | |
| <0 | 107 | (28.6) | 94 | (28.5) | 13 | (29.5) |
| 0 | 46 | (12.3) | 40 | (12.1) | 6 | (13.6) |
| >0 | 221 | (59.1) | 196 | (59.4) | 25 | (56.8) |
| χ2 = 0.13, df = 2, p = 0.936 | ||||||
| Dimension | Number of Items | Sum Score | Cronbach’s Alpha | ||||
|---|---|---|---|---|---|---|---|
| Mean | Standard Deviation | Average Item Rating a | Mean adjusted to Maximum Sum Score (%) b | Test for Normality c | |||
| Emotional exhaustion | 9 | 24.27 | 11.66 | 2.70 | 44.94 | 0.163 | 0.904 |
| Depersonalization | 5 | 7.78 | 5.94 | 1.56 | 25.93 | <0.001 | 0.737 |
| Personal achievement | 8 | 35.56 | 7.66 | 4.45 | 74.08 | 0.011 | 0.789 |
| Independent Variable | Emotional Exhaustion | Depersonalization | Personal Accomplishment | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RSSM | 95% CI | p Value | RSSM | 95% CI | p Value | RSSM | 95% CI | p Value | |
| Gender | |||||||||
| Females | 1.11 | 1.04–1.19 | 0.001 | ||||||
| Males * | 1.00 | ||||||||
| Age (years) | |||||||||
| ≥40 | 0.74 | 0.65–0.84 | <0.001 | ||||||
| <40 * | 1.00 | ||||||||
| Marital status | |||||||||
| Divorced/widow | 0.98 | 0.92–1.06 | 0.640 | ||||||
| Never married | 0.95 | 0.90–0.99 | 0.017 | ||||||
| Married * | 1.00 | ||||||||
| Work practice experience (years) | |||||||||
| ≥10 | 0.87 | 0.81–0.93 | <0.001 | ||||||
| <10 * | 1.00 | ||||||||
| Specialist status | |||||||||
| Specialists | 0.91 | 0.86–0.97 | 0.003 | 0.87 | 0.78–0.96 | 0.007 | |||
| General dental practitioners * | 1.00 | 1.00 | |||||||
| Number of working hours per week | |||||||||
| >40 | 1.09 | 1.04–1.15 | 0.001 | 1.11 | 1.01–1.21 | 0.026 | |||
| ≤40 * | 1.00 | 1.00 | |||||||
| Number of working days per week | |||||||||
| <5 | 0.92 | 0.88–0.97 | 0.001 | ||||||
| ≥5 * | 1.00 | ||||||||
| Job satisfaction score | |||||||||
| Negative | 1.61 | 1.53–1.69 | <0.001 | 1.67 | 1.54–1.82 | <0.001 | 0.88 | 0.84–0.92 | <0.001 |
| 0 | 1.31 | 1.23–1.40 | <0.001 | 1.24 | 1.10–1.40 | <0.001 | 0.97 | 0.92-1.03 | 0.300 |
| Positive * | 1.00 | 1.00 | 1.00 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Slabšinskienė, E.; Gorelik, A.; Kavaliauskienė, A.; Zaborskis, A. Burnout and Its Relationship with Demographic and Job-Related Variables among Dentists in Lithuania: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 3968. https://doi.org/10.3390/ijerph18083968
Slabšinskienė E, Gorelik A, Kavaliauskienė A, Zaborskis A. Burnout and Its Relationship with Demographic and Job-Related Variables among Dentists in Lithuania: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(8):3968. https://doi.org/10.3390/ijerph18083968
Chicago/Turabian StyleSlabšinskienė, Eglė, Andrej Gorelik, Aistė Kavaliauskienė, and Apolinaras Zaborskis. 2021. "Burnout and Its Relationship with Demographic and Job-Related Variables among Dentists in Lithuania: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 8: 3968. https://doi.org/10.3390/ijerph18083968