
Analysis of Pneumonia Occurrence in Relation to Climate Change in Tanga, Tanzania



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.1.1. Study Site
2.1.2. Sampling
2.2. Variables
2.2.1. Outcome Variable
2.2.2. Exposure Variables
2.2.3. Other Variables
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
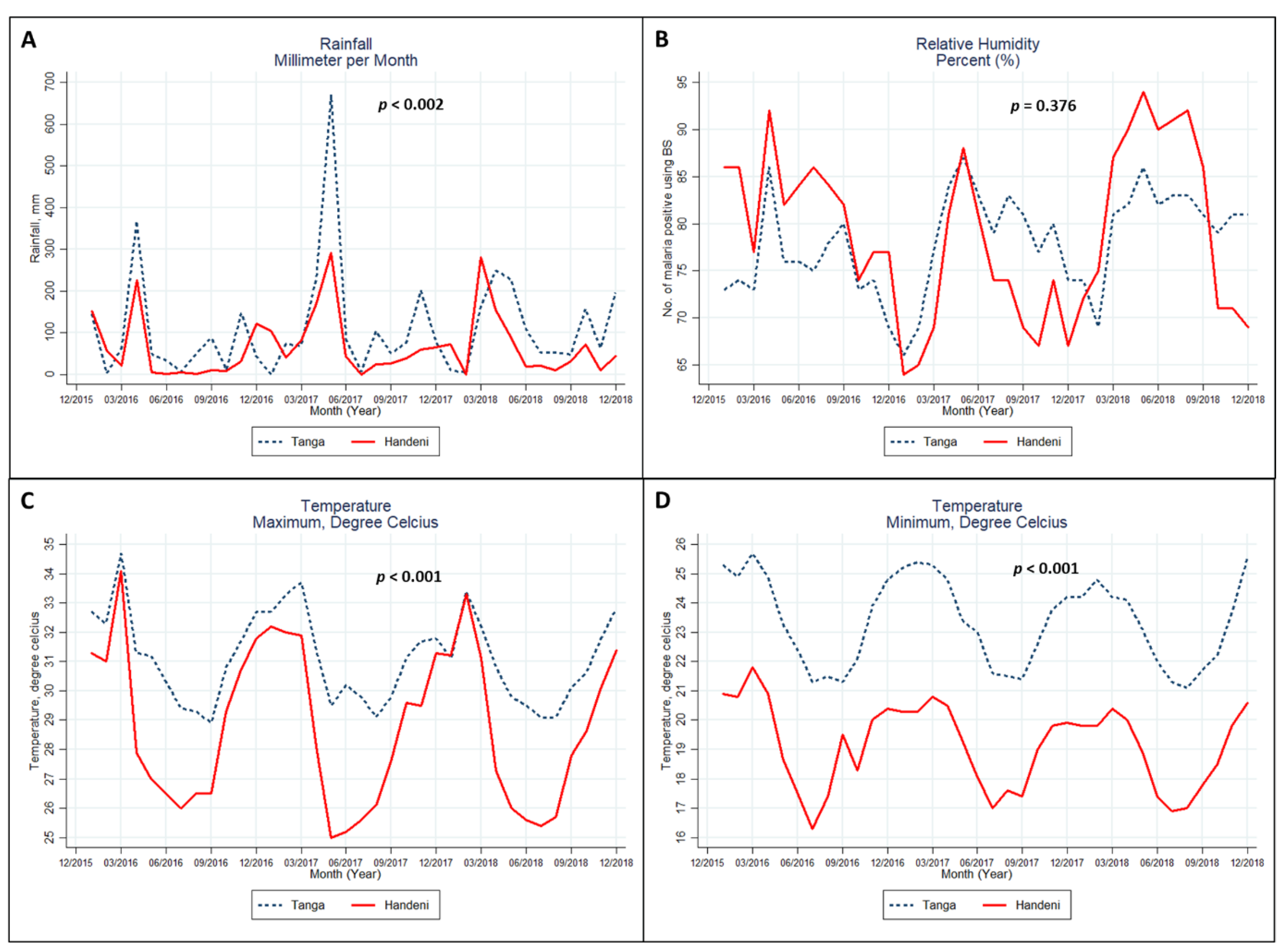
3.1. Trends in the Climate Indicators
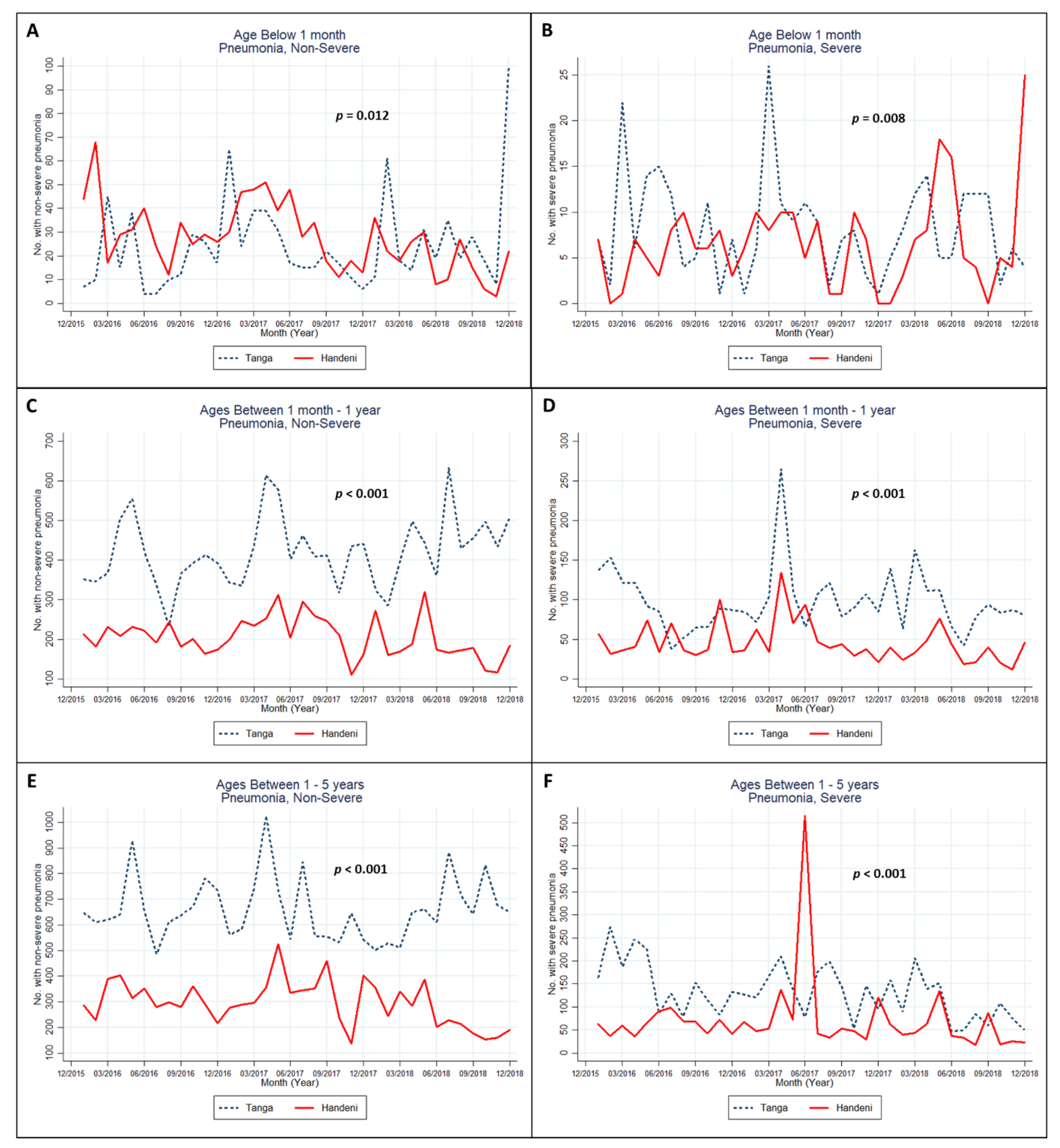
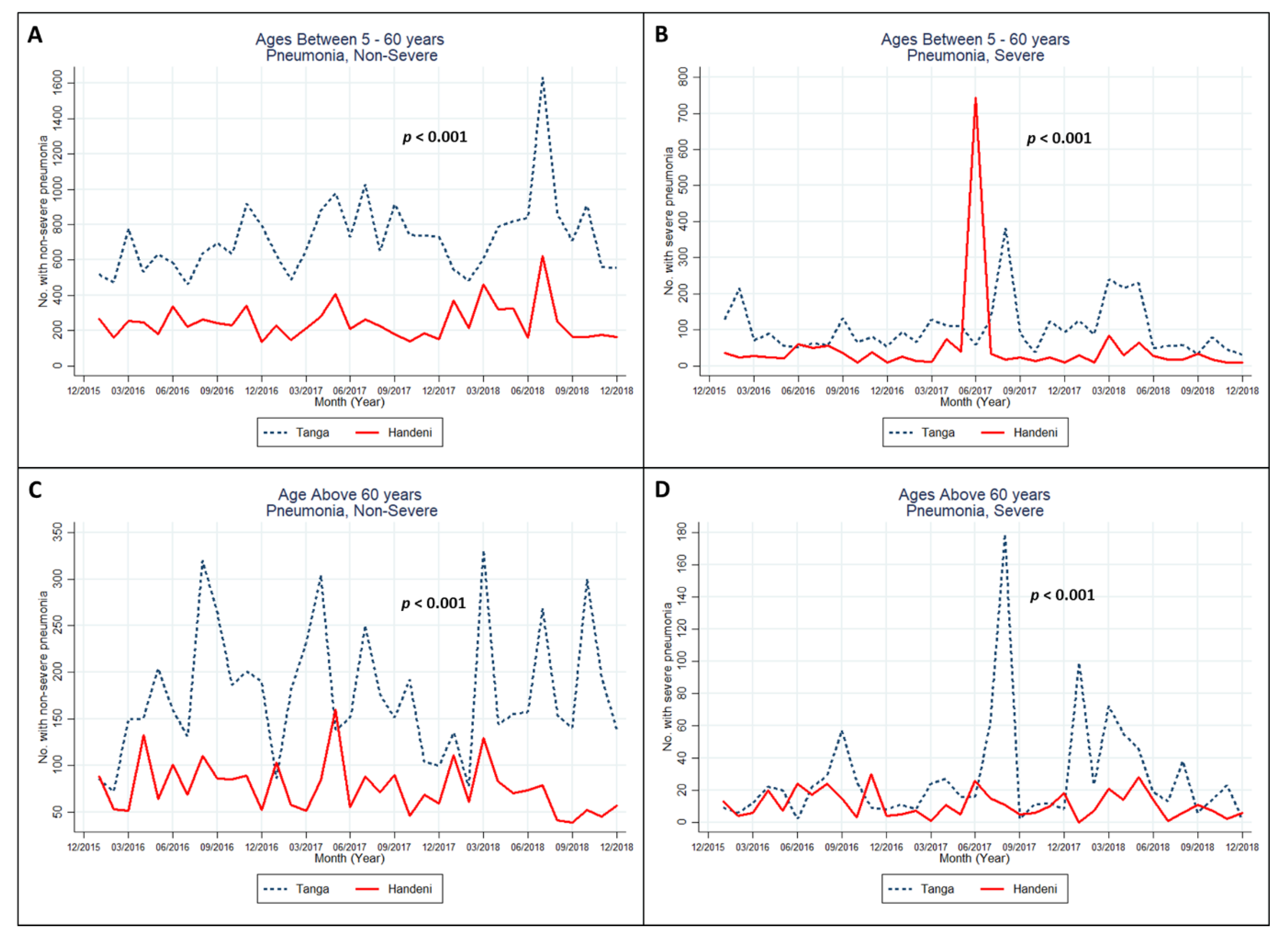
3.2. Trends in the Occurrence of Pneumococcal Infection
3.3. Association between Climate Change and Pneumococcal Infections
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Pneumonia. Available online: https://www.who.int/news-room/fact-sheets/detail/pneumonia (accessed on 5 July 2020).
- Ruuskanen, O.; Lahti, E.; Jennings, L.C.; Murdoch, D.R. Viral pneumonia. Lancet 2011, 377, 1264–1275. [Google Scholar] [CrossRef]
- Anthony, J.; Scott, G.; Adegbola, R.; Gordon, S.B. Pneumonia in adults. In Principles of Medicine in Africa, 4th ed.; Whitty, C.J.M., Mabey, D., Parry, E., Gill, G., Weber, M.W., Eds.; Cambridge University Press: Cambridge, UK, 2013; pp. 254–265. [Google Scholar]
- Muro, F.; Mtove, G.; Mosha, N.; Wangai, H.; Harrison, N.; Hildenwall, H.; Schellenberg, D.; Todd, J.; Olomi, R.; Reyburn, H. Effect of context on respiratory rate measurement in identifying non-severe pneumonia in African children. Trop. Med. Int. Health 2015, 20, 757–765. [Google Scholar] [CrossRef] [Green Version]
- Lugangira, K.; Kalokola, F. Morbidity and mortality of children aged 2–59 months admitted in the Tanzania Lake Zone’s public hospitals: A cross-sectional study. BMC Res. Notes 2017, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Forsberg, P. Pneumonia Among Hospitalized Children Aged 1–9 Years: A Prospective and Retrospective Study at a Referral Hospital in Northern Tanzania; Sahlgrenska Academy, Gothenburg University: Gothenburg, Sweden, 2012. [Google Scholar]
- Caggiano, S.; Ullmann, N.; De Vitis, E.; Trivelli, M.; Mariani, C.; Podagrosi, M.; Ursitti, F.; Bertolaso, C.; Putotto, C.; Unolt, M. Factors that negatively affect the prognosis of pediatric community-acquired pneumonia in district hospital in Tanzania. Int. J. Mol. Sci. 2017, 18, 623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Vaccine Access Center (IVAC); Johns Hopkins Bloomberg School of Public Health. Pneumonia and Diarrhea Progress Report. 2018. Available online: https://stoppneumonia.org/wp-content/uploads/2018/11/Pneumonia-and-Diarrhea-Progress-Report-2018.pdf (accessed on 6 July 2020).
- Rudan, I.; Boschi-Pinto, C.; Biloglav, Z.; Mulholland, K.; Campbell, H. Epidemiology and etiology of childhood pneumonia. Bull. World Health Organ. 2008, 86, 408–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Poon, R.; Chen, L.; Frescura, A.-M.; Montuschi, P.; Ciabattoni, G.; Wheeler, A.; Dales, R. Acute effects of air pollution on pulmonary function, airway inflammation, and oxidative stress in asthmatic children. Environ. Health Perspect. 2009, 117, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Sun, S.; Tang, R.; Chan, K.-P.; Tian, L. Pneumonia hospitalization risk in the elderly attributable to cold and hot temperatures in Hong Kong, China. Am. J. Epidemiol. 2016, 184, 570–578. [Google Scholar] [CrossRef] [Green Version]
- Mirsaeidi, M.; Motahari, H.; Taghizadeh Khamesi, M.; Sharifi, A.; Campos, M.; Schraufnagel, D.E. Climate change and respiratory infections. Ann. Am. Thorac. Soc. 2016, 13, 1223–1230. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Labori, M.; Viasus, D.; Simonetti, A.; Garcia-Somoza, D.; Dorca, J.; Gudiol, F.; Carratalà, J. Rainfall is a risk factor for sporadic cases of Legionella pneumophila pneumonia. PLoS ONE 2013, 8, e61036. [Google Scholar]
- Murdoch, D.R.; Jennings, L.C. Association of respiratory virus activity and environmental factors with the incidence of invasive pneumococcal disease. J. Infect. 2009, 58, 37–46. [Google Scholar] [CrossRef]
- Kózka, M.; Sega, A.; Wojnar-Gruszka, K.; Tarnawska, A.; Gniadek, A. Risk factors of pneumonia associated with mechanical ventilation. Int. J. Environ. Res. Public Health 2020, 17, 656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.L.; Seon, S.H.; Rhee, D.K. Pneumonia and Streptococcus pneumoniae vaccine. Arch. Pharm. Res. 2017, 40, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Zou, Q.; Zheng, S.; Wang, X.; Liu, S.; Bao, J.; Yu, F.; Wu, W.; Wang, X.; Shen, B.; Zhou, T.; et al. Influenza A-associated severe pneumonia in hospitalized patients: Risk factors and NAI treatments. Int. J. Infect. Dis. 2020, 92, 208–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, B.B.; Singh, V. Pneumonia bugs and determinants of their occurrence. Lung India Off. Organ Indian Chest Soc. 2018, 35, 95. [Google Scholar]
- Herrera-Lara, S.; Fernández-Fabrellas, E.; Cervera-Juan, Á.; Blanquer-Olivas, R. Do seasonal changes and climate influence the etiology of community acquired pneumonia? Arch. Bronconeumol. Engl. Ed. 2013, 49, 140–145. [Google Scholar] [CrossRef]
- Liu, Y.; Kan, H.; Xu, J.; Rogers, D.; Peng, L.; Ye, X.; Chen, R.; Zhang, Y.; Wang, W. Temporal relationship between hospital admissions for pneumonia and weather conditions in Shanghai, China: A time-series analysis. BMJ Open 2014, 4, e004961. [Google Scholar] [CrossRef]
- Kayembe, J.-M.N.; Kayembe, H.-C.N. Pneumonia: A Challenging Health Concern with the Climate Change. In Contemporary Topics of Pneumonia; IntechOpen: Rijeka, Croatia, 2017. [Google Scholar]
- Onozuka, D.; Hashizume, M.; Hagihara, A. Impact of weather factors on Mycoplasma pneumoniae pneumonia. Thorax 2009, 64, 507–511. [Google Scholar] [CrossRef] [Green Version]
- Makinen, T.M.; Juvonen, R.; Jokelainen, J.; Harju, T.H.; Peitso, A.; Bloigu, A.; Silvennoinen-Kassinen, S.; Leinonen, M.; Hassi, J. Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections. Respir. Med. 2009, 103, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Lam, H.C.-Y.; Chan, E.Y.-Y.; Goggins, W.B. Comparison of short-term associations with meteorological variables between COPD and pneumonia hospitalization among the elderly in Hong Kong—A time-series study. Int. J. Biometeorol. 2018, 62, 1447–1460. [Google Scholar] [CrossRef]
- Champatiray, J.; Satapathy, J.; Kashyap, B.; Mondal, D. Clinico-aetiological study of severe and very severe pneumonia in two months to five years children in a Tertiary Health Care Centre in Odisha, India. J. Clin. Diagn. Res. JCDR 2017, 11, SC06. [Google Scholar] [CrossRef]
- Chen, K.; Jia, R.; Li, L.; Yang, C.; Shi, Y. The aetiology of community associated pneumonia in children in Nanjing, China and aetiological patterns associated with age and season. BMC Public Health 2015, 15, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ota, K.; Sasabuchi, Y.; Matsui, H.; Jo, T.; Fushimi, K.; Yasunaga, H. Age distribution and seasonality in acute eosinophilic pneumonia: Analysis using a national inpatient database. BMC Pulm. Med. 2019, 19, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inostroza, J.; Vinet, A.M.; Retamal, G.; Lorca, P.; Ossa, G.; Facklam, R.R.; Sorensen, R.U. Influence of patient age on Streptococcus pneumoniae serotypes causing invasive disease. Clin. Diagn. Lab. Immunol. 2001, 8, 556–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, A.; Edwards, K.M.; Grijalva, C.G.; Self, W.H.; Zhu, Y.; Chappell, J.D.; Arnold, S.R.; McCullers, J.A.; Ampofo, K.; Pavia, A.T.; et al. Secondhand Smoke Exposure and Illness Severity among Children Hospitalized with Pneumonia. J. Pediatr. 2015, 167, 869–874.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grijalva, C.G.; Poehling, K.A.; Nuorti, J.P.; Zhu, Y.; Martin, S.W.; Edwards, K.M.; Griffin, M.R. National impact of universal childhood immunization with pneumococcal conjugate vaccine on outpatient medical care visits in the United States. Pediatrics 2006, 118, 865–873. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Amouzou, A.; Velez, L.C.; Tarekegn, H.; Young, M. One Is Too Many: Ending Child Deaths from Pneumonia and Diarrhoea; UNICEF: New York, NY, USA, 2016. [Google Scholar]
- Tasci, S.S.; Kavalci, C.; Kayipmaz, A.E. Relationship of Meteorological and Air Pollution Parameters with Pneumonia in Elderly Patients. Emerg. Med. Int. 2018, 2018, 4183203. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.E.; Dougherty, E.; McArthur, C.; Huang, Q.S.; Baker, M.G. Cold, dry air is associated with influenza and pneumonia mortality in Auckland, New Zealand. Influenza Other Respir. Viruses 2016, 10, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Zhang, Y.; Xu, Y.; Xu, X.; Liu, T.; Luo, Y.; Xiao, J.; Wu, W.; Ma, W. Temperature changes between neighboring days and mortality in summer: A distributed lag non-linear time series analysis. PLoS ONE 2013, 8, e66403. [Google Scholar] [CrossRef] [PubMed]
- Watson, M.; Gilmour, R.; Menzies, R.; Ferson, M.; McIntyre, P.; New South Wales Pneumococcal, N. The association of respiratory viruses, temperature, and other climatic parameters with the incidence of invasive pneumococcal disease in Sydney, Australia. Clin. Infect. Dis. 2006, 42, 211–215. [Google Scholar] [CrossRef] [Green Version]
- Saso, A.; Kampmann, B. Vaccine Responses in Newborns. In Seminars in Immunopathology; Springer: Berlin/Heidelberg, Germany, 2017; pp. 627–642. [Google Scholar]
- Don, M. Risk factors of paediatric community-acquired pneumonia. Eur. Respir. J. 2011, 37, 724–725. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| 2016, Annual µ (SD) a | 2017, Annual µ (SD) a | 2018, Annual µ (SD) a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Tanga | Handeni | p-Value | Tanga | Handeni | p-Value | Tanga | Handeni | p-Value | |
| Nonsevere Pneumonia | |||||||||
| <1 month | 18.1 (13.5) | 31.6 (14.5) | 0.027 | 25.1 (16.3) | 32.1 (14.7) | 0.281 | 30.1 (25.9) | 18.6 (10.4) | 0.168 |
| 1 month–1 year | 389.8 (81.6) | 203.9 (25.8) | <0.001 | 431.8 (89.7) | 227.7 (55.6) | <0.001 | 438.8 (92.5) | 185.0 (57.1) | <0.001 |
| 1–5 years | 668.4 (108.8) | 308.2 (59.1) | <0.001 | 655.3 (154.1) | 334.1 (101.3) | <0.001 | 655.0 (116.9) | 244.5 (79.5) | <0.001 |
| 5–60 years | 638.2 (139.2) | 239.9 (62.1) | <0.001 | 763.8(158.0) | 219.7 (73.9) | <0.001 | 775.8 (306.7) | 283.3 (145.7) | <0.001 |
| ≥61 years | 176.2 (69.4) | 81.7 (25.1) | <0.001 | 172.1 (65.2) | 77.8 (31.3) | <0.001 | 182.8 (76.3) | 70.0 (27.7) | <0.001 |
| Severe Pneumonia | |||||||||
| <1 month | 8.8 (6.1) | 5.3 (3.0) | 0.090 | 7.8 (6.8) | 6.4 (3.8) | 0.536 | 8.1 (4.1) | 7.9 (7.7) | 0.948 |
| 1 month–1 year | 92.2 (34.9) | 48.4 (22.1) | 0.001 | 107.5 (52.3) | 54.1 (32.2) | 0.006 | 93.3 (33.6) | 35.3 (17.7) | <0.001 |
| 1–5 years | 156.3 (65.5) | 61.9 (20.0) | <0.001 | 137.8 (46.9) | 101.8 (134.2) | 0.390 | 101.8 (51.6) | 49.0 (34.0) | 0.007 |
| 5–60 year | 88.8 (48.4) | 32.8 (16.6) | 0.001 | 119.0 (87.8) | 85.9 (208.0) | 0.617 | 104.3 (79.7) | 29.0 (23.1) | 0.005 |
| Climate Indicators | |||||||||
| Rainfall, mm | 83.6 (101.2) | 53.1 (73.5) | 0.406 | 136.6 (180.7) | 78.8 (80.1) | 0.322 | 111.2 (85.1) | 66.9 (80.4) | 0.204 |
| Humidity, % | 75.6 (4.3) | 82.3 (5.2) | 0.002 | 78.3 (6.2) | 72.8 (7.4) | 0.058 | 80.2 (4.5) | 82.3 (9.8) | 0.493 |
| Temperature, Max °C | 31.3 (1.7) | 29.1 (2.7) | 0.024 | 31.2 (1.5) | 28.7 (2.8) | 0.012 | 30.9 (1.4) | 28.6 (2.7) | 0.020 |
| Temperature, Min °C | 23.5 (1.7) | 19.4 (1.7) | <0.001 | 23.5 (1.5) | 19.2 (1.3) | <0.001 | 23.2 (1.5) | 18.9 (1.3) | <0.001 |
| Infectious Disease | Crude IRR (95% CI) | Adjusted IRR (95% CI) |
|---|---|---|
| Nonsevere Pneumonia | ||
| Rainfall, mm | 1.01 (1.01, 1.02) *** | 1.00 (1.00, 1.00) |
| Humidity, % | 1.01 (0.99, 1.02) | 1.01 (1.01, 1.02) ** |
| Temperature, Max °C | 1.07 (1.02, 1.12) *** | 1.00 (0.96, 1.04) |
| Temperature, Min °C | 1.13 (1.10, 1.18) **** | 1.01 (0.96, 1.06) |
| Age group (ref: >60 years) | ||
| <1 month | 0.20 (0.17, 0.24) **** | 0.23 (0.20, 0.27) **** |
| 1 month–1 year | 2.47 (2.08, 2.93) **** | 2.52 (2.22, 2.85) **** |
| 1–5 years | 3.77 (3.17, 4.47) **** | 3.80 (3.35, 4.30) **** |
| 5–60 years | 3.84 (3.23, 4.56) **** | 3.69 (3.26, 4.18) **** |
| District (ref: Tanga) | ||
| Handeni | 0.42 (0.35, 0.51) **** | 0.51 (0.43, 0.60) **** |
| Year (ref: 2016) | ||
| 2017 | 1.07 (0.83, 1.37) | 1.07 (0.96, 1.20) |
| 2018 | 1.05 (0.81, 1.34) | 0.95 (0.86, 1.05) |
| Severe Pneumonia | ||
| Rainfall, mm | 1.01 (1.01, 1.02) ** | 1.00 (1.00, 1.00) |
| Humidity, % | 1.02 (0.99, 1.03) * | 1.02 (1.01, 1.03) ** |
| Temperature, Max °C | 1.02 (0.97, 1.07) | 0.86 (0.80, 0.92) **** |
| Temperature, Min °C | 1.11 (1.07, 1.16) **** | 1.21 (1.11, 1.33) **** |
| Age group (ref: >60 years) | ||
| <1 month | 0.38 (0.29, 0.49) **** | 0.43 (0.34, 0.54) **** |
| 1 month–1 year | 3.67 (2.84, 4.73) **** | 3.80 (3.06, 4.72) **** |
| 1–5 years | 5.18 (4.02, 6.68) **** | 5.37 (4.33, 6.67) **** |
| 5–60 years | 3.91 (3.03, 5.05) **** | 3.71 (2.99, 4.60) **** |
| District (ref: Tanga) | ||
| Handeni | 0.50 (0.40, 0.62) **** | 0.73 (0.54, 0.98) ** |
| Year (ref: 2016) | ||
| 2017 | 1.26 (0.95, 1.66) | 1.26 (1.05, 1.52) ** |
| 2018 | 0.90 (0.68, 1.18) | 0.94 (0.79, 1.11) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyayo, S.F.; Owili, P.O.; Muga, M.A.; Lin, T.-H. Analysis of Pneumonia Occurrence in Relation to Climate Change in Tanga, Tanzania. Int. J. Environ. Res. Public Health 2021, 18, 4731. https://doi.org/10.3390/ijerph18094731
Miyayo SF, Owili PO, Muga MA, Lin T-H. Analysis of Pneumonia Occurrence in Relation to Climate Change in Tanga, Tanzania. International Journal of Environmental Research and Public Health. 2021; 18(9):4731. https://doi.org/10.3390/ijerph18094731
Chicago/Turabian StyleMiyayo, Samweli Faraja, Patrick Opiyo Owili, Miriam Adoyo Muga, and Tang-Huang Lin. 2021. "Analysis of Pneumonia Occurrence in Relation to Climate Change in Tanga, Tanzania" International Journal of Environmental Research and Public Health 18, no. 9: 4731. https://doi.org/10.3390/ijerph18094731