
Development of a Digital Lifestyle Modification Intervention for Use after Transient Ischaemic Attack or Minor Stroke: A Person-Based Approach

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
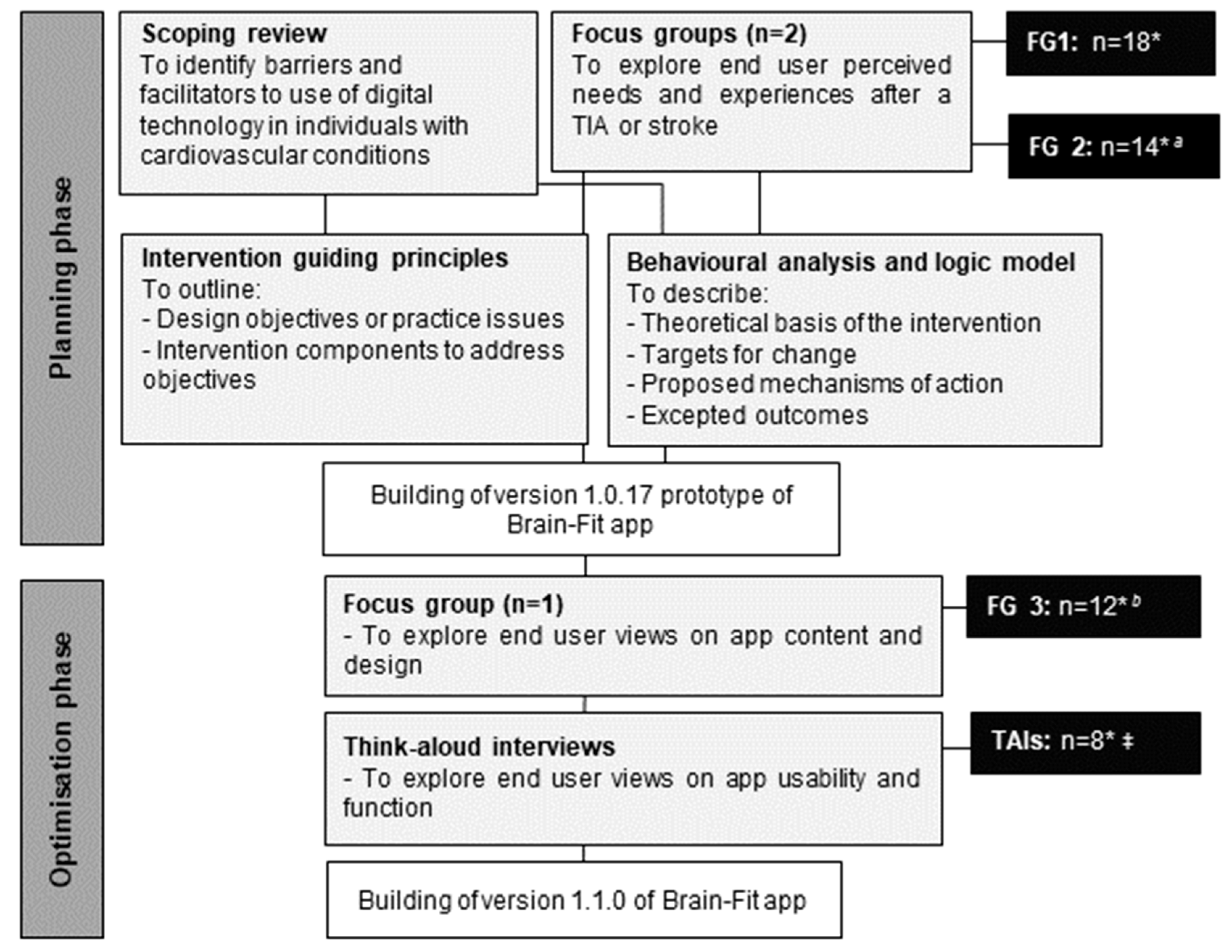
2.1. Study Design
- A scoping review of qualitative evidence to identify perceived barriers and facilitators to use of digital health interventions in individuals with cardiovascular disease (CVD).
- Primary qualitative evidence from two focus group meetings to explore end users’ perceived needs and experiences after a TIA or stroke.
- Development of intervention guiding principles.
- Behavioural analysis and logic modelling.
- Primary qualitative evidence from an additional focus group to explore end user perspectives on the content and structure of the prototype, ‘Brain-Fit’ app.
- Qualitative think-aloud interviews to explore end users’ in-depth views on the prototype and its content, functionality and usability.
2.2. Phase I: Intervention Planning
2.2.1. Scoping Review
2.2.2. Primary Qualitative Evidence
2.2.3. Development of Intervention Guiding Principles
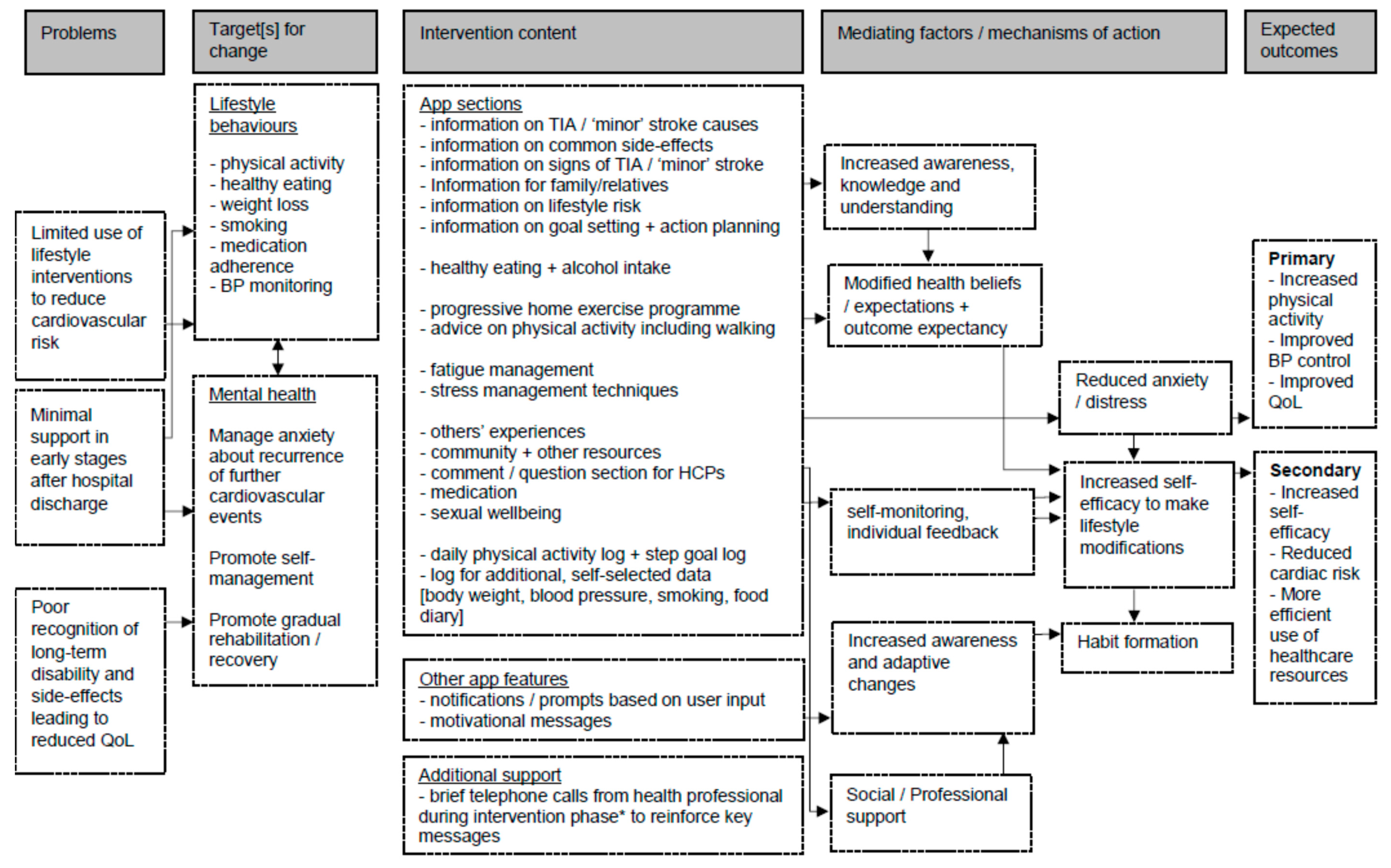
2.2.4. Behavioural Analysis and Logic Modelling
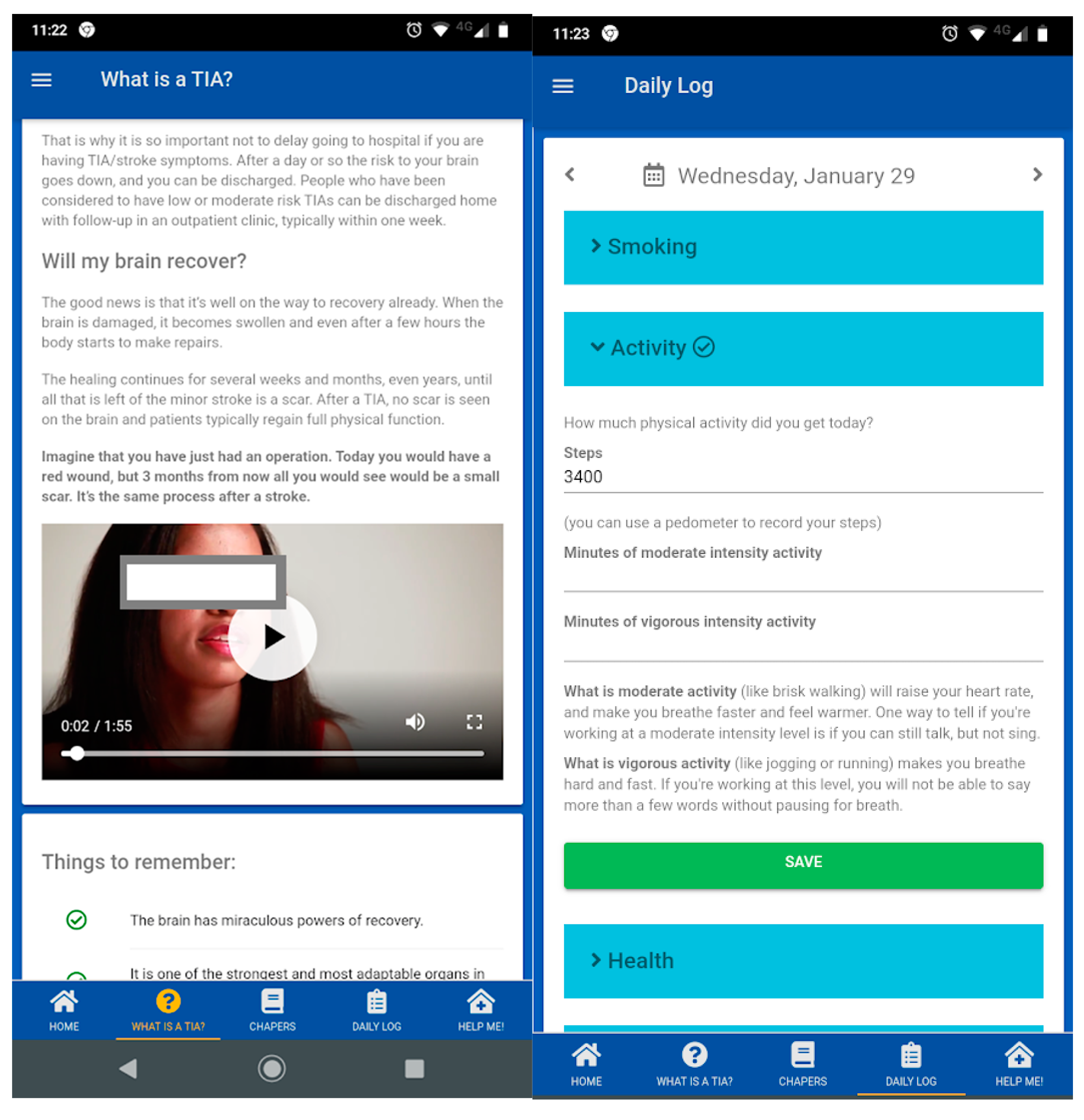
2.2.5. Prototype Intervention Building
2.3. Phase II. Intervention Optimisation
2.3.1. Primary Qualitative Evidence from Additional Focus Group Meeting
2.3.2. Qualitative Think-Aloud Interviews
3. Results
3.1. Scoping Review
3.2. Primary Qualitative Evidence from Focus Group 1 and 2
3.3. Intervention Guiding Principles
3.4. Behavioural Analysis and Logic Modelling
3.5. Phase II. Intervention Optimisation
Primary Qualitative Evidence from Focus Group 3 and Think-Aloud Interviews
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Flach, C.; Muruet, W.; Wolfe, C.D.A.; Bhalla, A.; Douiri, A. Risk and Secondary Prevention of Stroke Recurrence: A Population-Base Cohort Study. Stroke 2020, 51, 2435–2444. [Google Scholar] [CrossRef]
- GBD 2016 Neurological Disorders Collaborator Group. Global, regional, and national burden of neurological disorders during 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Giles, M.F.; Rothwell, P.M. Risk of stroke early after transient ischaemic attack: A systematic review and meta-analysis. Lancet Neurol. 2007, 6, 1063–1072. [Google Scholar] [CrossRef]
- Deijle, I.A.; Van Schaik, S.M.; Van Wegen, E.E.; Weinstein, H.C.; Kwakkel, G.; Van den Berg-Vos, R.M. Lifestyle interventions to prevent cardiovascular events after stroke and transient ischemic attack: Systematic review and meta-analysis. Stroke 2017, 48, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, M.; Laumeier, I.; Ihl, T.; Steinicke, M.; Ferse, C.; Endres, M.; Grau, A.; Hastrup, S.; Poppert, H.; Palm, F.; et al. A support programme for secondary prevention in patients with transient ischaemic attack and minor stroke (INSPiRE-TMS): An open-label, randomised controlled trial. Lancet Neurol. 2020, 19, 49–60. [Google Scholar] [CrossRef]
- Lee, Y.M.; Kim, R.B.; Lee, H.J.; Kim, K.; Shin, M.H.; Park, H.K.; Ahn, S.K.; Kim, S.Y.; Lee, Y.H.; Kim, B.G.; et al. Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: A cross-sectional study. Health Qual. Life Outcomes 2018, 16, 100. [Google Scholar] [CrossRef] [PubMed]
- Willeit, P.; Toell, T.; Boehme, C.; Krebs, S.; Mayer, L.; Lang, C.; Seekircher, L.; Tschiderer, L.; Willeit, K.; Rumpold, G.; et al. STROKE-CARD care to prevent cardiovascular events and improve quality of life after acute ischaemic stroke or TIA: A randomised clinical trial. EClinicalMedicine 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Sammut, M.; Fini, N.; Haracz, K.; Nilsson, M.; English, C.; Janssen, H. Increasing time spent engaging in moderate-to vigorous physical activity by community-dwelling adults following a transient ischemic attack or non-disabling stroke: A systematic review. Disabil. Rehabil. 2020, 1, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Redgrave, J.; Shafizadeh, M.; Majid, A.; Kilner, K.; Ali, A.N. Aerobic exercise interventions reduce blood pressure in patients after stroke or transient ischaemic attack: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 1515–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flint, K.; Kennedy, K.; Arnold, S.V.; Dodson, J.A.; Cresci, S.; Alexander, K.P. Slow Gait Speed and Cardiac Rehabilitation Participation in Older Adults After Acute Myocardial Infarction. J. Am. Heart Assoc. 2018, 7, e008296. [Google Scholar] [CrossRef]
- Aggarwal, M.; Ornish, D.; Josephson, R.; Brown, T.M.; Ostfeld, R.J.; Gordon, N.; Madan, S.; Allen, K.; Khetan, A.; Mahmoud, A.; et al. Closing Gaps in Lifestyle Adherence for Secondary Prevention of Coronary Heart Disease. Am. J. Cardiol. 2021, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Borg, S.; Öberg, B.; Nilsson, L.; Söderlund, A.; Bäck, M. The Added Value of a Behavioral Medicine Intervention in Physiotherapy on Adherence and Physical Fitness in Exercise-Based Cardiac Rehabilitation (ECRA): A Randomised, Controlled Trial. Patient Prefer. Adherence 2020, 14, 2517–2529. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.; Auinger, A.; Riedl, R.; Kindermann, H.; Helfert, M.; Ocenasek, H. Digitally enhanced recovery: Investigating the use of digital self-tracking for monitoring leisure time physical activity of cardiovascular disease (CVD) patients undergoing cardiac rehabilitation. PLoS ONE 2017, 12, e0186261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GOV.UK. Coronavirus (COVID-19): Guidance and Support. Available online: https://www.gov.uk/coronavirus (accessed on 21 January 2021).
- Gallagher, R.; Chow, C.; Parker, H.; Neubeck, L.; Celermajer, D.; Redfern, J.; Tofler, G.; Buckley, T.; Schumacher, T.; Ferry, C. Design and rationale of the MyHeartMate study: A randomised controlled trial of a game-based app to promote behaviour change in patients with cardiovascular disease. BMJ Open 2019, 9, e024269. [Google Scholar] [CrossRef]
- Dithmer, M.; Rasmussen, J.O.; Grönvall, E.; Spindler, H.; Hansen, J.; Nielsen, G.; Sørensen, S.B.; Dinesen, B. “The Heart Game” Using Gamification as Part of a Telerehabilitation Program for Heart Patients. Games Health J. 2016, 5, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Radhakrishnan, K.; Toprac, P.; O’Hair, M.; Bias, R.; Kim, M.T.; Bradley, P.; Mackert, M. Interactive Digital e-Health Game for Heart Failure Self-Management: A Feasibility Study. Games Health J. 2016, 5, 366–374. [Google Scholar] [CrossRef]
- Wei, K.S.; Ibrahim, N.E.; Kumar, A.A.; Jena, S.; Chew, V.; Depa, M.; Mayanil, N.; Kvedar, J.C.; Gaggin, H.K. Habits Heart App for Patient Engagement in Heart Failure Management: Pilot Feasibility Randomized Trial. JMIR Mhealth Uhealth 2021, 9, e19465. [Google Scholar] [CrossRef]
- Duscha, B.D.; Piner, L.W.; Patel, M.P.; Craig, K.P.; Brady, M.; McGarrah, R.W., 3rd; Chen, C.; Kraus, W.E. Effects of a 12-week mHealth program on peak VO2 and physical activity patterns after completing cardiac rehabilitation: A randomized controlled trial. Am. Heart J. 2018, 199, 105–114. [Google Scholar] [CrossRef]
- Persell, S.D.; Peprah, Y.A.; Lipiszko, D.; Lee, J.Y.; Li, J.J.; Ciolino, J.D.; Karmali, K.N.; Sato, H. Effect of Home Blood Pressure Monitoring via a Smartphone Hypertension Coaching Application or Tracking Application on Adults With Uncontrolled Hypertension: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e200255. [Google Scholar] [CrossRef] [Green Version]
- Setiawan, I.M.A.; Zhou, L.; Alfikri, Z.; Saptono, A.; Fairman, A.D.; Dicianno, B.E.; Parmanto, B. An adaptive mobile health system to support self-management for persons with chronic conditions and disabilities: Usability and feasibility studies. JMIR Form Res. 2019, 3, e12982. [Google Scholar] [CrossRef]
- Liao, P.; Dempsey, W.; Sarker, H.; Hossain, S.M.; Al’absi, M.; Klasnja, P.; Murphy, S. Just-in-time but not too much: Determining treatment timing in mobile health. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2018, 2, 179. [Google Scholar] [CrossRef] [PubMed]
- Forman, E.M.; Goldstein, S.P.; Crochiere, R.J.; Butryn, M.L.; Juarascio, A.S.; Zhang, F.; Foster, G.D. Randomized controlled trial of OnTrack, a just-in-time adaptive intervention designed to enhance weight loss. Transl. Behav. Med. 2019, 9, 989–1001. [Google Scholar] [CrossRef] [PubMed]
- Byambasuren, O.; Sanders, S.; Beller, E.; Glasziou, P. Prescribable mHealth apps identified from an overview of systematic reviews. NPJ Digit. Med. 2018, 1, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, W.T.; Rivera, D.E.; Atienza, A.A.; Nilsen, W.; Allison, S.M.; Mermelstein, R. Health behavior models in the age of mobile interventions: Are our theories up to the task? Transl. Behav. Med. 2011, 1, 53–71. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Kolt, G.S.; Caperchione, C.M.; Savage, T.N.; Rosenkranz, R.R.; Maeder, A.J.; Van Itallie, A.; Tague, R.; Oldmeadow, C.; Mummery, W.K. Effectiveness of a Web 2.0 Intervention to Increase Physical Activity in Real-World Settings: Randomized Ecological Trial. J. Med. Internet Res. 2017, 19, e390. [Google Scholar] [CrossRef] [Green Version]
- Yardley, L.; Spring, B.J.; Riper, H.; Morrison, L.G.; Crane, D.H.; Curtis, K.; Merchant, G.C.; Naughton, F.; Blandford, A. Understanding and Promoting Effective Engagement with Digital Behavior Change Interventions. Am. J. Prev. Med. 2016, 51, 833–842. [Google Scholar] [CrossRef] [Green Version]
- Yardley, L.; Ainsworth, B.; Arden-Close, E.; Muller, I. The person-based approach to enhancing the acceptability and feasibility of interventions. Pilot Feasibility Stud. 2015, 1, 37. [Google Scholar] [CrossRef] [Green Version]
- Muller, I.; Santer, M.; Morrison, L.; Morton, K.; Roberts, A.; Rice, C.; Williams, M.; Yardley, L. Combining qualitative research with PPI: Reflections on using the person-based approach for developing behavioural interventions. Res. Involv. Engagem. 2019, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Heron, N.; Kee, F.; Mant, J.; Reilly, P.M.; Cupples, M.; Tully, M.; Donnelly, M. Stroke Prevention Rehabilitation Intervention Trial of Exercise (SPRITE)—A randomised feasibility study. BMC Cardiovasc. Disord. 2017, 17, 290. [Google Scholar] [CrossRef] [Green Version]
- Heron, N.; Kee, F.; Mant, J.; Cupples, M.E.; Donnelly, M. Rehabilitation of patients after transient ischaemic attack or minor stroke: Pilot feasibility randomised trial of a home-based prevention programme. Br. J. Gen. Pract. 2019, 69, e706–e714. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Saldaña, J. Qualitative Data Analysis Strategies. In The Oxford Handbook of Qualitative Research, 2nd ed.; Leavy, P., Ed.; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Michie, S.; Wood, C.E.; Johnston, M.; Abraham, C.; Francis, J.J.; Hardeman, W. Behaviour change techniques: The development and evaluation of a taxonomic method for reporting and describing behaviour change interventions (a suite of five studies involving consensus methods, randomised controlled trials and analysis of qualitative data). Health Technol. Assess. 2015, 19, 1–188. [Google Scholar] [PubMed] [Green Version]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.M.; Colquhoun, H.; Grimshaw, J.M. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 7. [Google Scholar] [CrossRef]
- Michie, S.; West, R. The Behaviour Change Wheel: A Guide to Developing Inter-Ventions; Silverback Publishing: London, UK, 2015; Available online: www.behaviour-changewheel.com (accessed on 3 November 2020).
- Smith, C.M.; Griffiths, F.; Fothergill, R.T.; Vlaev, I.; Perkins, G.D. Identifying and overcoming barriers to automated external defibrillator use by GoodSAM volunteer first responders in out-of-hospital cardiac arrest using the Theoretical Domains Framework and Behaviour Change Wheel: A qualitative study. BMJ Open 2020, 10, e034908. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Marshall, A.P.; Lin, F. Lessons learnt from the implementation of same-day discharge after percutaneous coronary intervention. Aust. Crit. Care 2019, 32, 458–464. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, K.S.; Ahmad, N.; Tahir, H.; Kahn, S. Fuzzy MoSCoW: A fuzzy based MoSCoW method for the prioritization of software requirements. In Proceedings of the International Conference on Intelligent Computing, Instrumentation and Control Technologies (ICICICT), Kannur, India, 6–7 July 2017; pp. 433–437. [Google Scholar]
- Van Rooij, F.G.; Plaizier, N.O.; Vermeer, S.E.; Góraj, B.M.; Koudstaal, P.J.; Richard, E.; de Leeuw, F.E.; Kessels, R.; van Dijk, E.J. Subjective Cognitive Impairment, Depressive Symptoms, And Fatigue After A Tia Or Transient Neurological Attack: A Prospective Study. Behav. Neurol. 2017, 2017, 5181024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, X.L.; Zuo, L.J.; Zhang, N.; Yang, Y.; Pan, Y.S.; Xiang, X.L.; Chen, L.Y.; Meng, X.; Li, H.; Zhao, X.Q.; et al. Impairment of CognitiON and Sleep quality for patients after acute ischemic stroke or transient ischemic attack (ICONS) Investigators. The occurrence and longitudinal changes of cognitive impairment after acute ischemic stroke. Neuropsychiatr. Dis. Treat. 2020, 16, 807–814. [Google Scholar] [CrossRef] [Green Version]
- Heron, N.; O’Connor, S.R.; Kee, F.; Mant, J.; Cupples, M.E.; Donnelly, M. Usability and Acceptability of a Novel Secondary Prevention Initiative Targeting Physical Activity for Individuals after a Transient Ischaemic Attack or “Minor” Stroke: A Qualitative Study. Int. J. Environ. Res. Public Health 2020, 17, 8788. [Google Scholar] [CrossRef]
- Ramírez-Moreno, J.M.; Muñoz-Vega, P.; Alberca, S.B.; Peral-Pacheco, D. Health-Related Quality of Life and Fatigue after Transient Ischemic Attack and Minor Stroke. Stroke Cerebrovasc. Dis. 2019, 28, 276–284. [Google Scholar] [CrossRef]
- Dang, S.; Karanam, C.; Gómez-Orozco, C.; Gómez-Marín, O. Mobile Phone Intervention for Heart Failure in a Minority Urban County Hospital Population: Usability and Patient Perspectives. Telemed. J. E-Health 2017, 23, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.; Mawson, S.; Mountain, G.; Nasr, N.; Davies, R.; Zheng, H. The provision of feedback through computer-based technology to promote self-managed post-stroke rehabilitation in the home. Disabil. Rehabil. Assist. Technol. 2014, 9, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Pfaeffli, L.; Maddison, R.; Whittaker, R.; Stewart, R.; Kerr, A.; Jiang, Y.; Kira, G.; Carter, K.; Dalleck, L. A mHealth cardiac rehabilitation exercise intervention: Findings from content development studies. BMC Cardiovasc. Disord. 2012, 12, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, D.M.; Moran, K.; Cornelissen, V.; Buys, R.; Cornelis, N.; Woods, C. Electronic Health Physical Activity Behavior Change Intervention to Self-Manage Cardiovascular Disease: Qualitative Exploration of Patient and Health Professional Requirements. J. Med. Internet. Res. 2018, 20, e163. [Google Scholar] [CrossRef] [PubMed]
- Connell, L.E.; Carey, R.N.; de Bruin, M.; Rothman, A.J.; Johnston, M.; Kelly, M.P.; Michie, S. Links between behavior change techniques and mechanisms of action: An expert consensus study. Ann. Behav. Med. 2019, 8, 708–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chudowolska-Kiełkowska, M.; Małek, Ł.A. A nurse-led intervention to promote physical activity in sedentary older adults with cardiovascular risk factors: A randomized clinical trial (STEP-IT-UP study). Eur. J. Cardiovasc. Nurs. 2020, 19, 638–645. [Google Scholar] [CrossRef]
- Thorup, C.B.; Grønkjær, M.; Spindler, H.; Andreasen, J.J.; Hansen, J.; Dinesen, B.I.; Nielsen, G.; Sørensen, E.E. Pedometer use and self-determined motivation for walking in a cardiac telerehabilitation program: A qualitative study. BMC Sports Sci. Med. Rehabil. 2016, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Knittle, K.; Heino, M.; Marques, M.M.; Stenius, M.; Beattie, M.; Ehbrecht, F.; Hagger, M.S.; Hardeman, W.; Hankonen, N. The compendium of self-enactable techniques to change and self-manage motivation and behaviour v.1.0. Nat. Hum. Behav. 2020, 4, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Coorey, G.M.; Neubeck, L.; Mulley, J.; Redfern, J. Effectiveness, acceptability and usefulness of mobile applications for cardiovascular disease self-management: Systematic review with meta-synthesis of quantitative and qualitative data. Eur. J. Prev. Cardiol. 2018, 25, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; MacIintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guest, G.; Namey, E.; McKenna, K. How Many Focus Groups Are Enough? Building an Evidence Base for Nonprobability Sample Sizes. Field Methods 2017, 29, 3–22. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Focus Group Methods |
|---|
|
|
|
|
|
| Intervention Components |
|---|
| Chapters Introduction General information on TIA and minor stroke
Managing stress
Sex after a TIA or minor stroke Community resources General information on employment, driving and relevant sources of support. |
Daily log
|
My notes and reminders
|
Other app features [automated]
|
| Total Participants (N= 32) | |
|---|---|
| Age category | |
| 18–49 years 50–69 years 70+ years | 3 (9.4%) 23 (71.8%) 6 (18.7%) |
| Gender | |
| Female Male | 21 (65.6%) 11 (34.4%) |
| Ethnicity | |
| White Black/African/Caribbean/Black British Other | 30 (93.7%) 1 (3.1%) 1 (3.1%) |
| Previous use of mobile technology (smartphone/tablet) | |
| Yes No | 27 (84.4%) 5 (15.6%) |
| Design Objectives | Key Intervention Features | |
|---|---|---|
| 1 | Increase confidence and self-efficacy for making behavioural change and address barriers to lifestyle change Barriers addressed: 1, 2, 3, 4, 5, 6, 7, 8 * |
|
| 2 | Ensure ease of use and good intervention acceptability Barriers addressed: 9, 10, 13 * |
|
| 3 | Provide accessible, brief information and support that can be viewed easily on mobile devices (promoting frequent/daily use) Barriers addressed: 1, 8, 9, 11, 12 * |
|
| 4 | Promote self-management and longer-term behavioural change Barriers addressed: 1, 2, 5, 11 * |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heron, N.; O’Connor, S.R.; Kee, F.; Thompson, D.R.; Anderson, N.; Cutting, D.; Cupples, M.E.; Donnelly, M. Development of a Digital Lifestyle Modification Intervention for Use after Transient Ischaemic Attack or Minor Stroke: A Person-Based Approach. Int. J. Environ. Res. Public Health 2021, 18, 4861. https://doi.org/10.3390/ijerph18094861
Heron N, O’Connor SR, Kee F, Thompson DR, Anderson N, Cutting D, Cupples ME, Donnelly M. Development of a Digital Lifestyle Modification Intervention for Use after Transient Ischaemic Attack or Minor Stroke: A Person-Based Approach. International Journal of Environmental Research and Public Health. 2021; 18(9):4861. https://doi.org/10.3390/ijerph18094861
Chicago/Turabian StyleHeron, Neil, Seán R. O’Connor, Frank Kee, David R. Thompson, Neil Anderson, David Cutting, Margaret E. Cupples, and Michael Donnelly. 2021. "Development of a Digital Lifestyle Modification Intervention for Use after Transient Ischaemic Attack or Minor Stroke: A Person-Based Approach" International Journal of Environmental Research and Public Health 18, no. 9: 4861. https://doi.org/10.3390/ijerph18094861