
Acute Effects of a High Volume vs. High Intensity Bench Press Protocol on Electromechanical Delay and Muscle Morphology in Recreationally Trained Women

 , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
2. Material and Methods
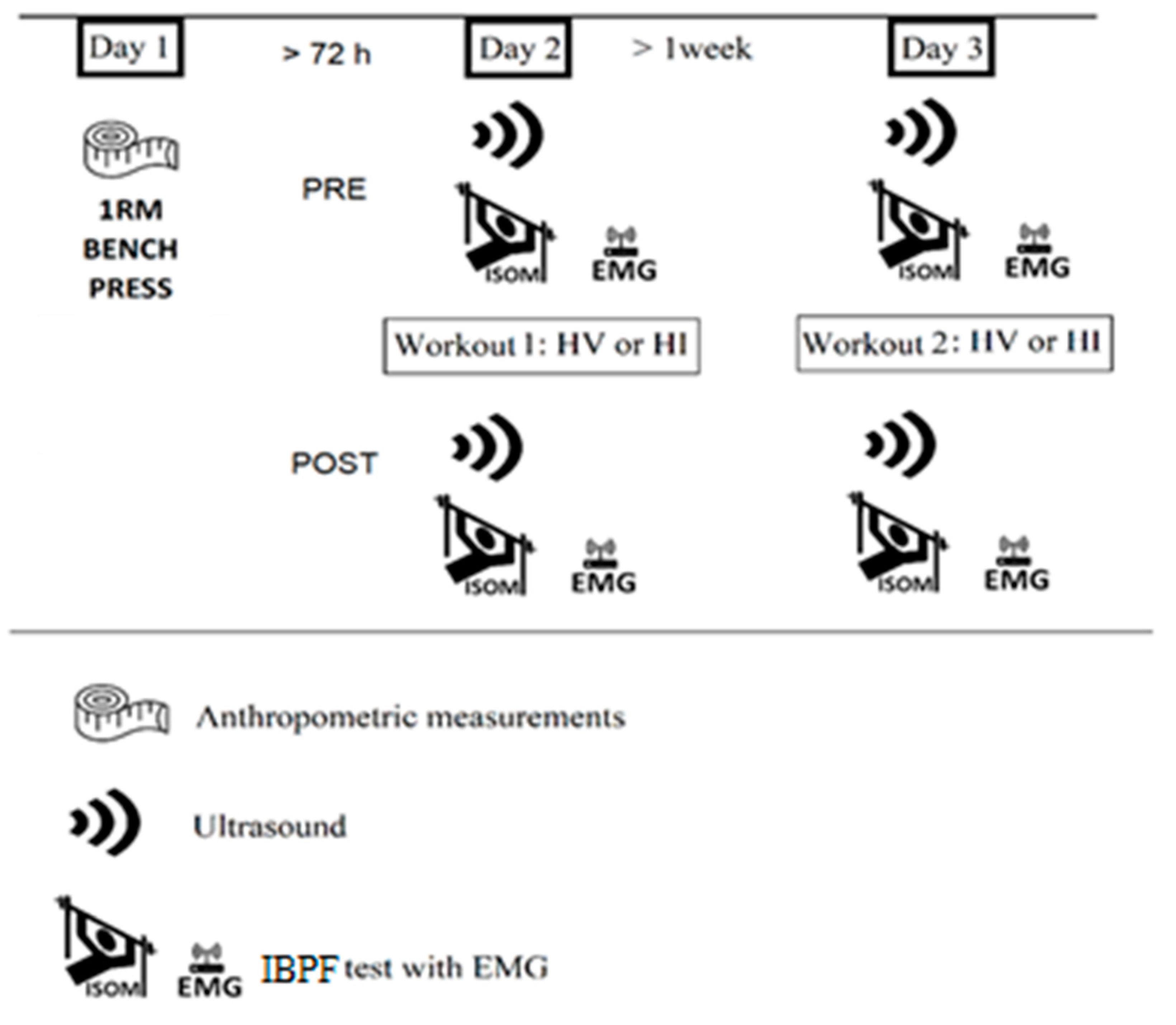
2.1. Experimental Design
2.2. Subjects
2.3. Strength Testing
2.4. Ultrasound Measurements
2.5. Electromyographic Measurements
2.6. Statistical Analysis
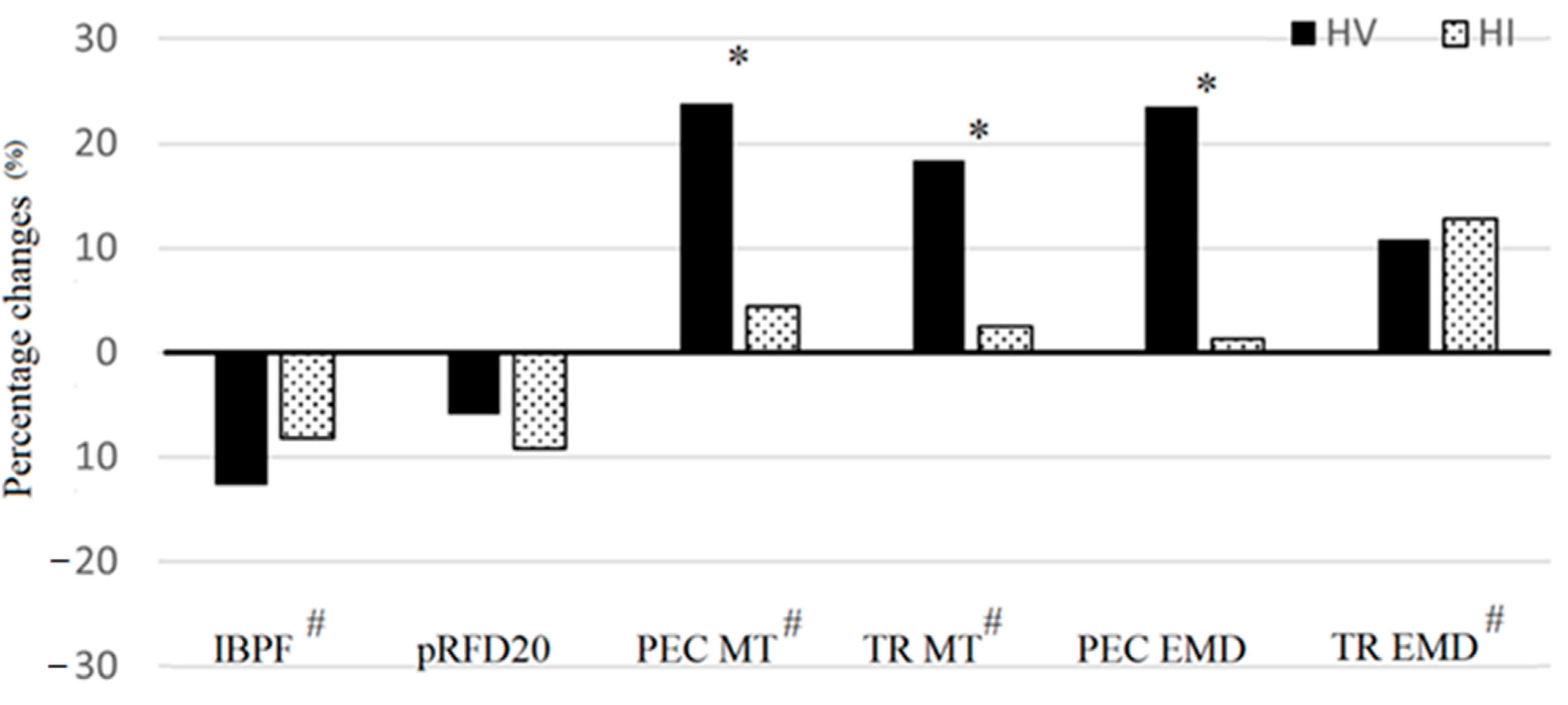
3. Results
3.1. Strength Testing
3.2. Ultrasound Measurements
3.3. Electromyographic Measurements
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gonzalez, A.M.; Hoffman, J.R.; Townsend, J.R.; Jajtner, A.R.; Boone, C.H.; Beyer, K.S.; Baker, K.M.; Wells, A.J.; Mangine, G.T.; Robinson IV, E.H.; et al. Intramuscular anabolic signaling and endocrine response following high volume and high intensity resistance exercise protocols in trained men. Physiol. Rep. 2015, 3, e12466. [Google Scholar] [CrossRef] [Green Version]
- Bartolomei, S.; Sadres, E.; Church, D.D.; Arroyo, E.; Gordon, J.A., III; Varanoske, A.N.; Wang, R.; Beyer, K.S.; Oliveira, L.P.; Stout, J.R.; et al. Comparison of the recovery response from high-intensity and high-volume resistance exercise in trained men. Eur. J. Appl. Physiol. 2017, 117, 1287–1298. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, P.R.; Komi, P.V. Electromechanical delay in human skeletal muscle under concentric and eccentric contractions. Graefe’s Arch. Clin. Exp. Ophthalmol. 1979, 42, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, J.T.; Feland, J.B.; Hunter, I. A comparison of voluntary and involuntary measures of electromechanical delay. Int. J. Neurosci. 2007, 117, 597–604. [Google Scholar] [CrossRef]
- Howatson, G.; Glaister, M.; Brouner, J.; Van Someren, K.A. The reliability of electromechanical delay and torque during isometric and concentric isokinetic contractions. J. Electromyogr. Kinesiol. 2009, 19, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.B.; Herda, T.J.; Walter, A.A.; Valdez, A.M.; Cramer, J.T. Effects of short-term resistance training and subsequent detraining on the electromechanical delay. Muscle Nerve 2013, 48, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Stock, M.S.; Olinghouse, K.D.; Mota, J.A.; Drusch, A.S.; Thompson, B.J.; Information, P.E.K.F.C. Muscle group specific changes in the electromechanical delay following short-term resistance training. J. Sci. Med. Sport 2016, 19, 761–765. [Google Scholar] [CrossRef]
- Kubo, K.; Kanehisa, H.; Ito, M.; Fukunaga, T. Effects of isometric training on the elasticity of human tendon structures in vivo. J. Appl. Physiol. 2001, 91, 26–32. [Google Scholar] [CrossRef]
- Häkkinen, K.; Komi, P.V. Changes in Neuromuscular Performance in Voluntary and Reflex Contraction during Strength Training in Man. Int. J. Sports Med. 1983, 4, 282–288. [Google Scholar] [CrossRef]
- Yavuz, Ş.U.; Şendemir-Ürkmez, A.; Türker, K.S. Effect of gender, age, fatigue and contraction level on electromechanical delay. Clin. Neurophysiol. 2010, 121, 1700–1706. [Google Scholar] [CrossRef]
- Minshull, C.; Gleeson, N.; Walters-Edwards, M.; Eston, R.; Rees, D. Effects of acute fatigue on the volitional and magnetically-evoked electromechanical delay of the knee flexors in males and females. Graefe’s Arch. Clin. Exp. Ophthalmol. 2007, 100, 469–478. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Huston, L.J.; Lindenfeld, T.N.; Hewett, T.E.; Greenfield, M.L.V.H. Association Between the Menstrual Cycle and Anterior Cruciate Ligament Injuries in Female Athletes. Am. J. Sports Med. 1998, 26, 614–619. [Google Scholar] [CrossRef]
- Zhou, S.; Carey, M.F.; Snow, R.J.; Lawson, D.L.; Morrison, W. Effects of muscle fatigue and temperature on electromechanical delay. Electromyogr. Clin. Neurophysiol. 1998, 38, 67–74. [Google Scholar]
- Evans, E.M.; Rowe, D.A.; Misic, M.M.; Prior, B.M.; Arngrímsson, S.Á. Skinfold Prediction Equation for Athletes Developed Using a Four-Component Model. Med. Sci. Sports Exerc. 2005, 37, 2006–2011. [Google Scholar] [CrossRef] [PubMed]
- Bartolomei, S.; Hoffman, J.R.; Stout, J.R.; Merni, F. Effect of Lower-Body Resistance Training on Upper-Body Strength Adaptation in Trained Men. J. Strength Cond. Res. 2018, 32, 13–18. [Google Scholar] [CrossRef]
- Bartolomei, S.; Nigro, F.; Ruggeri, S.; Lanzoni, I.M.; Ciacci, S.; Merni, F.; Sadres, E.; Hoffman, J.R.; Semprini, G. Comparison Between Bench Press Throw and Ballistic Push-up Tests to Assess Upper-Body Power in Trained Individuals. J. Strength Cond. Res. 2018, 32, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Haff, G.G.; Ruben, R.P.; Lider, J.; Twine, C.; Cormie, P. A Comparison of Methods for Determining the Rate of Force Development During Isometric Midthigh Clean Pulls. J. Strength Cond. Res. 2015, 29, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Kondo, M.; Kawakami, Y.; Fukunaga, T. Prediction equations for body composition of Japanese adults by B-mode ultrasound. Am. J. Hum. Biol. 1994, 6, 161–170. [Google Scholar] [CrossRef]
- Yasuda, T.; Fujita, S.; Ogasawara, R.; Sato, Y.; Abe, T. Effects of low-intensity bench press training with restricted arm muscle blood flow on chest muscle hypertrophy: A pilot study. Clin. Physiol. Funct. Imaging 2010, 30, 338–343. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Stevens, J.P. Applied Multivariate Statistics for the Social Sciences; Routledge: London, UK, 2012. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Bartolomei, S.; Totti, V.; Griggio, F.; Malerba, C.; Ciacci, S.; Semprini, G.; Di Michele, R. Upper-Body Resistance Exercise Reduces Time to Recover After a High-Volume Bench Press Protocol in Resistance-Trained Men. J. Strength Cond. Res. 2021, 35, S180–S187. [Google Scholar] [CrossRef] [PubMed]
- Aben, H.G.J.; Hills, S.P.; Higgins, D.; Cooke, C.B.; Davis, D.; Jones, B.; Russell, M. The Reliability of Neuromuscular and Perceptual Measures Used to Profile Recovery, and the Time-Course of Such Responses Following Academy Rugby League Match-Play. Sports 2020, 8, 73. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.A.; Drake, D. Dissociated Time Course of Recovery Between Strength and Power After Isoinertial Resistance Loading in Rugby Union Players. J. Strength Cond. Res. 2018, 32, 748–755. [Google Scholar] [CrossRef]
- Raeder, C.; Wiewelhove, T.; Westphal-Martinez, M.P.; Fernandez-Fernandez, J.; Simola, R.A.D.P.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Neuromuscular Fatigue and Physiological Responses After Five Dynamic Squat Exercise Protocols. J. Strength Cond. Res. 2016, 30, 953–965. [Google Scholar] [CrossRef] [Green Version]
- McGuigan, M.R.; Winchester, J.B. The Relationship Between Isometric and Dynamic Strength in College Football Players. J. sports Sci. Med. 2008, 7, 101–105. [Google Scholar]
- Markus, I.; Constantini, K.; Hoffman, J.R.; Bartolomei, S.; Gepner, Y. Exercise-induced muscle damage: Mechanism, assessment and nutritional factors to accelerate recovery. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 121, 969–992. [Google Scholar] [CrossRef]
- Esposito, F.; Limonta, E.; Cè, E. Passive stretching effects on electromechanical delay and time course of recovery in human skeletal muscle: New insights from an electromyographic and mechanomyographic combined approach. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 111, 485–495. [Google Scholar] [CrossRef]
- Allen, D.G.; Lamb, G.D.; Westerblad, H. Impaired calcium release during fatigue. J. Appl. Physiol. 2008, 104, 296–305. [Google Scholar] [CrossRef]
- Chalchat, E.; Gennisson, J.-L.; Peñailillo, L.; Oger, M.; Malgoyre, A.; Charlot, K.; Bourrilhon, C.; Siracusa, J.; Garcia-Vicencio, S. Changes in the Viscoelastic Properties of the Vastus Lateralis Muscle with Fatigue. Front. Physiol. 2020, 11, 307. [Google Scholar] [CrossRef] [PubMed]
- Morel, B.; Hug, F.; Nordez, A.; Pournot, H.; Besson, T.; Mathevon, L.; Lapole, T. Reduced Active Muscle Stiffness after Intermittent Submaximal Isometric Contractions. Med. Sci. Sports Exerc. 2019, 51, 2603–2609. [Google Scholar] [CrossRef]
- Zhou, S.; Lawson, D.L.; Morrison, W.E.; Fairweather, I. Electromechanical delay in isometric muscle contractions evoked by voluntary, reflex and electrical stimulation. Graefe’s Arch. Clin. Exp. Ophthalmol. 1995, 70, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, Y.; Kubo, K.; Fukunaga, T.; Kanehisa, H. Effects of repeated muscle contractions on the tendon structures in humans. Graefe’s Arch. Clin. Exp. Ophthalmol. 2001, 84, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Kubo, K.; Kanehisa, H.; Kawakami, Y.; Fukunaga, T. Influences of repetitive muscle contractions with different modes on tendon elasticity in vivo. J. Appl. Physiol. 2001, 91, 277–282. [Google Scholar] [CrossRef]
- Cè, E.; Rampichini, S.; Agnello, L.; Limonta, E.; Veicsteinas, A.; Esposito, F. Effects of temperature and fatigue on the electromechanical delay components. Muscle Nerve 2013, 47, 566–576. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Assessment | Time Point | HV (Mean ± SD) | HI (Mean ± SD) | Trial Difference |
|---|---|---|---|---|
| IBPF (N) | PRE | 439.3 ± 108.4 | 446.5 ± 78.3 | F = 1.951 p = 0.196 η2 = 0.178 |
| POST | 383.4 ± 102.1 | 410.8 ± 89.2 | ||
| pRFD (N s−1) | PRE | 3297.0 ± 1205.6 | 3644.5 ± 1197.0 | F = 0.213 p = 0.655 η2 = 0.023 |
| POST | 3102.5 ± 1115.2 | 3307.5 ± 929.2 | ||
| PEC MT (mm) | PRE | 13.2 ± 2.7 | 13.2 ± 2.2 | F = 17.951 p = 0.002 η2 = 0.666 |
| POST | 16.3 ± 3.5 | 13.7 ± 2.1 | ||
| TR MT (mm) | PRE | 17.2 ± 2.4 | 17.1 ± 2.7 | F = 18.632 p < 0.001 η2 = 0.791 |
| POST | 20.3 ± 3.1 | 17.1 ± 2.2 | ||
| PEC EMD (ms) | PRE | 116.4 ± 26.0 | 116.9 ± 39.5 | F = 5.654 p = 0.039 η2 = 0.361 |
| POST | 143.8 ± 26.6 | 118.5 ± 31.5 | ||
| TR EMD (ms) | PRE | 118.7 ± 29.0 | 111.2 ± 22.1 | F = 0.036 p = 0.854 η2 = 0.004 |
| POST | 131.5 ± 16.1 | 125.5 ± 23.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartolomei, S.; Nigro, F.; Malagoli Lanzoni, I.; Mangia, A.L.; Cortesi, M.; Ciacci, S.; Fantozzi, S. Acute Effects of a High Volume vs. High Intensity Bench Press Protocol on Electromechanical Delay and Muscle Morphology in Recreationally Trained Women. Int. J. Environ. Res. Public Health 2021, 18, 4874. https://doi.org/10.3390/ijerph18094874
Bartolomei S, Nigro F, Malagoli Lanzoni I, Mangia AL, Cortesi M, Ciacci S, Fantozzi S. Acute Effects of a High Volume vs. High Intensity Bench Press Protocol on Electromechanical Delay and Muscle Morphology in Recreationally Trained Women. International Journal of Environmental Research and Public Health. 2021; 18(9):4874. https://doi.org/10.3390/ijerph18094874
Chicago/Turabian StyleBartolomei, Sandro, Federico Nigro, Ivan Malagoli Lanzoni, Anna Lisa Mangia, Matteo Cortesi, Simone Ciacci, and Silvia Fantozzi. 2021. "Acute Effects of a High Volume vs. High Intensity Bench Press Protocol on Electromechanical Delay and Muscle Morphology in Recreationally Trained Women" International Journal of Environmental Research and Public Health 18, no. 9: 4874. https://doi.org/10.3390/ijerph18094874