
Listen to Your Heart–Ecological Momentary Assessment of Interoceptive Accuracy, Awareness and Sensibility: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
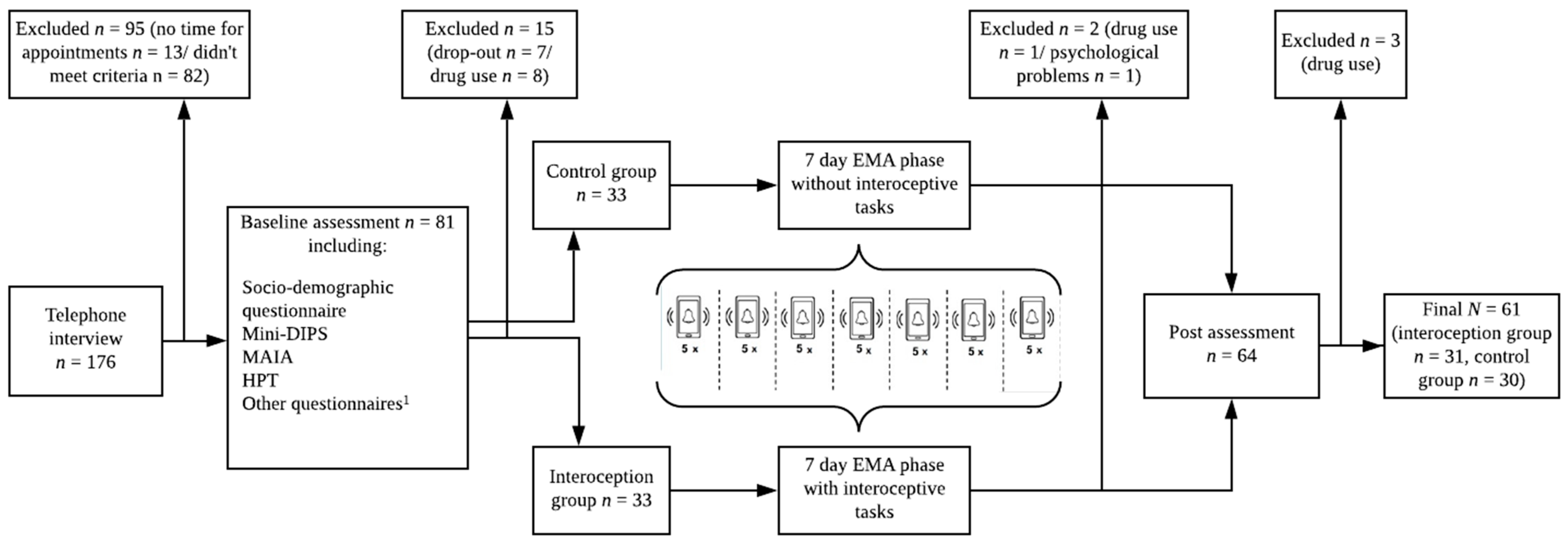
2.1. Participants
2.2. Procedure
2.2.1. Baseline Assessment
2.2.2. 7-Day EMA
2.2.3. Post Assessment
2.3. Measures
2.3.1. Baseline and Post Assessment Measures
Multidimensional Assessment of Interoceptive Awareness (MAIA)
Pre- and Post-Heartbeat Perception Task (HPT)
2.3.2. Items Used during the EMA Phase
EMA-MAIA
EMA-HPT
2.4. Statistical Analyses
2.4.1. EMA-Data (Interoception Group Only)
2.4.2. Baseline and Post Assessment Data
3. Results
3.1. Short-Term Variability of Interoception during EMA
3.2. Practice Effects of Interoception from Baseline to Post Assessment
4. Discussion
4.1. Fluctuations of Interoception during EMA
4.2. Practice Effects of Interoception from Baseline to Post Assessment
4.3. Strengths and Limitations
- (1)
- Zamariola, Maurage, Luminet and Corneille [64] state that interoceptive accuracy measured with the HPT depends on the error of participants’ undercounting of their perceived heartbeats due to their beliefs about their heart rate. Ainley, Tsakiris, Pollatos, Schulz and Herbert [67] counter that participants’ beliefs do not explain why participants would rate their heart rates lower than they are and, thereby, their beliefs would not particularly explain their possible undercounting, which is contradictory to the first criticism.
- (2)
- The number of recorded heartbeats and the number of perceived heartbeats does not correlate (in Zamariola, Maurage, Luminet and Corneille’s data [64]). However, Ainley, Tsakiris, Pollatos, Schulz and Herbert [67] found that Zamariola, Maurage, Luminet and Corneille [64] made this assumption due to arithmetic misunderstanding, which disproves this second criticism.
- (3)
- Zamariola, Maurage, Luminet and Corneille [64] state that a measure for interoceptive accuracy should not depend on heart condition. However, this should actually be treated in favor of the HPT’s construct validity, since it is clear that the perception of interoceptive signals is depending on one’s specific physiology [67].
- (4)
- Last but not least, there seems to be a tendency to poorer performance on the longer trials of the HPT. This statement is rejected by Ainley, Tsakiris, Pollatos, Schulz and Herbert [67] arguing that mean recorded heart rates significantly differed between the three lengths of the trials in the data of Zamariola, Maurage, Luminet and Corneille [64], which is in contrast to their assumption that the heart rate is constant across intervals and the poorer performance for longer trials is traced to participants’ undercounting.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Craig, A.D. Interoception: The sense of the physiological condition of the body. Curr. Opin. Neurobiol. 2003, 13, 500–505. [Google Scholar] [CrossRef]
- Dunn, B.D.; Galton, H.C.; Morgan, R.; Evans, D.; Oliver, C.; Meyer, M.; Cusack, R.; Lawrence, A.D.; Dalgleish, T. Listening to your heart: How interoception shapes emotion experience and intuitive decision making. Psychol. Sci. 2010, 21, 1835–1844. [Google Scholar] [CrossRef] [Green Version]
- Yoris, A.; Esteves, S.; Couto, B.; Melloni, M.; Kichic, R.; Cetkovich, M.; Favaloro, R.; Moser, J.; Manes, F.; Ibanez, A.; et al. The roles of interoceptive sensitivity and metacognitive interoception in panic. Behav. Brain Funct. 2015, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Garfinkel, S.N.; Seth, A.K.; Barrett, A.B.; Suzuki, K.; Critchley, H.D. Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biol. Psychol. 2015, 104, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012, 7, e48230. [Google Scholar]
- Meessen, J.; Mainz, V.; Gauggel, S.; Volz-Sidiropoulou, E.; Sütterlin, S.; Forkmann, T. The relationship between interoception and metacognition: A pilot study. J. Psychophysiol. 2016, 30, 76–86. [Google Scholar] [CrossRef]
- Forkmann, T.; Scherer, A.; Meessen, J.; Michal, M.; Schachinger, H.; Vogele, C.; Schulz, A. Making sense of what you sense: Disentangling interoceptive awareness, sensibility and accuracy. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2016, 109, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Schandry, R. Heart beat perception and emotional experience. Psychophysiology 1981, 18, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Quadt, L.; Critchley, H.D.; Garfinkel, S.N. The neurobiology of interoception in health and disease. Ann. N. Y. Acad. Sci. 2018, 1428, 112–128. [Google Scholar] [CrossRef]
- Paulus, M.P.; Stein, M.B. Interoception in anxiety and depression. Brain Struct. Funct. 2010, 214, 451–463. [Google Scholar] [CrossRef] [Green Version]
- Pollatos, O.; Traut-Mattausch, E.; Schandry, R. Differential effects of anxiety and depression on interoceptive accuracy. Depress. Anxiety 2009, 26, 167–173. [Google Scholar] [CrossRef]
- Domschke, K.; Stevens, S.; Pfleiderer, B.; Gerlach, A.L. Interoceptive sensitivity in anxiety and anxiety disorders: An overview and integration of neurobiological findings. Clin. Psychol. Rev 2010, 30, 1–11. [Google Scholar] [CrossRef]
- Garfinkel, S.N.; Tiley, C.; O’Keeffe, S.; Harrison, N.A.; Seth, A.K.; Critchley, H.D. Discrepancies between dimensions of interoception in autism: Implications for emotion and anxiety. Biol. Psychol. 2016, 114, 117–126. [Google Scholar] [CrossRef]
- Dunn, B.D.; Stefanovitch, I.; Evans, D.; Oliver, C.; Hawkins, A.; Dalgleish, T. Can you feel the beat? Interoceptive awareness is an interactive function of anxiety- and depression-specific symptom dimensions. Behav. Res. Ther. 2010, 48, 1133–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Does, A.J.; Van, D.R.; Spinhoven, P. Accurate heartbeat perception in panic disorder: Fact and artefact. J. Affect. Disord. 1997, 43, 121–130. [Google Scholar] [CrossRef]
- Ehlers, A.; Breuer, P. Increased cardiac awareness in panic disorder. J Abnorm. Psychol. 1992, 101, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Pollatos, O.; Traut-Mattausch, E.; Schroeder, H.; Schandry, R. Interoceptive awareness mediates the relationship between anxiety and the intensity of unpleasant feelings. J. Anxiety Disord. 2007, 21, 931–943. [Google Scholar] [CrossRef]
- Dunn, B.D.; Dalgleish, T.; Ogilvie, A.D.; Lawrence, A.D. Heartbeat perception in depression. Behav. Res. Ther. 2007, 45, 1921–1930. [Google Scholar] [CrossRef]
- Eggart, M.; Lange, A.; Binser, M.J.; Queri, S.; Müller-Oerlinghausen, B. Major depressive disorder is associated with impaired interoceptive accuracy: A systematic review. Brain Sci. 2019, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- Forrest, L.N.; Smith, A.R.; White, R.D.; Joiner, T.E. (Dis)connected: An examination of interoception in individuals with suicidality. J. Abnorm. Psychol. 2015, 124, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M. EDI-3, Eating Disorder Inventory-3: Professional Manual; Psychological Assessment Resources Incorporated: Lutz, FL, USA, 2004. [Google Scholar]
- Duffy, M.E.; Rogers, M.L.; Gallyer, A.J.; Joiner, T.E. Body Trust and Agitation: Pathways to Suicidal Thoughts and Behaviors. Arch. Suicide Res. 2019, S230–S250. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.L.; Hagan, C.R.; Joiner, T.E. Examination of interoception along the suicidality continuum. J. Clin. Psychol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Brausch, A.M.; Woods, S.E. Emotion Regulation Deficits and Nonsuicidal Self-Injury Prospectively Predict Suicide Ideation in Adolescents. Suicide Life Threat. Behav. 2019, 49, 868–880. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.R.; Dodd, D.R.; Ortiz, S.; Forrest, L.N.; Witte, T.K. Interoceptive deficits differentiate suicide groups and associate with self-injurious thoughts and behaviors in a military sample. Suicide Life Threat. 2019. [Google Scholar] [CrossRef]
- Hagan, C.R.; Rogers, M.L.; Brausch, A.M.; Muehlenkamp, J.J.; Joiner, T.E. Interoceptive deficits, non-suicidal self-injury, and suicide risk: A multi-sample study of indirect effects. Psychol. Med. 2019, 49, 2789–2800. [Google Scholar] [CrossRef]
- Forkmann, T.; Volz-Sidiropoulou, E.; Helbing, T.; Drüke, B.; Mainz, V.; Rath, D.; Gauggel, S.; Teismann, T. Sense it and use it: Interoceptive accuracy and sensibility in suicide ideators. BMC Psychiatry 2019, 19. [Google Scholar] [CrossRef] [Green Version]
- DeVille, D.C.; Kuplicki, R.; Stewart, J.L.; Paulus, M.P.; Khalsa, S.S.; Investigators, T. Diminished responses to bodily threat and blunted interoception in suicide attempters. eLife 2020, 9, e51593. [Google Scholar] [CrossRef]
- Hielscher, E.; Zopf, R. Interoceptive abnormalities and suicidality: A systematic review. Behav. Ther. 2020. [Google Scholar] [CrossRef]
- Ebner-Priemer, U.W.; Trull, T.J. Ecological momentary assessment of mood disorders and mood dysregulation. Psychol. Assess. 2009, 21, 463–475. [Google Scholar] [CrossRef]
- Wittkamp, M.F.; Bertsch, K.; Vögele, C.; Schulz, A. A latent state-trait analysis of interoceptive accuracy. Psychophysiology 2018, 55, e13055. [Google Scholar] [CrossRef]
- Bornemann, B.; Herbert, B.M.; Mehling, W.E.; Singer, T. Differential changes in self-reported aspects of interoceptive awareness through 3 months of contemplative training. Front. Psychol. 2015, 5, 1504. [Google Scholar] [CrossRef] [Green Version]
- Fischer, D.; Messner, M.; Pollatos, O. Improvement of interoceptive processes after an 8-week body scan intervention. Front. Hum. Neurosci. 2017, 11, 452. [Google Scholar] [CrossRef] [Green Version]
- Meyerholz, L.; Irzinger, J.; Witthöft, M.; Gerlach, A.L.; Pohl, A. Contingent biofeedback outperforms other methods to enhance the accuracy of cardiac interoception: A comparison of short interventions. J. Behav. Ther. Exp. Psychiatry 2019, 63, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Trull, T.J.; Ebner-Priemer, U. The role of ambulatory assessment in psychological science. Curr. Dir. Psychol. Sci. 2014, 23, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Trull, T.J.; Ebner-Priemer, U.W. Using experience sampling methods/ecological momentary assessment (ESM/EMA) in clinical assessment and clinical research: Introduction to the special section. Psychol. Assess. 2009, 21, 457–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czyz, E.K.; King, C.A.; Nahum-Shani, I. Ecological assessment of daily suicidal thoughts and attempts among suicidal teens after psychiatric hospitalization: Lessons about feasibility and acceptability. Psychiatry Res. 2018, 267, 566–574. [Google Scholar] [CrossRef]
- Hallensleben, N.; Spangenberg, L.; Forkmann, T.; Rath, D.; Hegerl, U.; Kersting, A.; Kallert, T.W.; Glaesmer, H. Investigating the Dynamics of Suicidal Ideation. Crisis 2017, 65–69. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Turner, B.J.; Fedor, S.; Beale, E.E.; Huffman, J.C.; Nock, M.K. Examination of Real-Time Fluctuations in Suicidal Ideation and Its Risk Factors: Results From Two Ecological Momentary Assessment Studies. J. Abnorm. Psychol. 2017. [Google Scholar] [CrossRef]
- Schoevers, R.; van Borkulo, C.; Lamers, F.; Servaas, M.; Bastiaansen, J.; Beekman, A.; van Hemert, A.; Smit, J.; Penninx, B.; Riese, H. Affect fluctuations examined with ecological momentary assessment in patients with current or remitted depression and anxiety disorders. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Forkmann, T.; Spangenberg, L.; Rath, D.; Hallensleben, N.; Hegerl, U.; Kersting, A.; Glaesmer, H. Assessing suicidality in real time: A psychometric evaluation of self-report items for the assessment of suicidal ideation and its proximal risk factors using ecological momentary assessments. J. Abnorm. Psychol. 2018, 127, 758–769. [Google Scholar] [CrossRef]
- Ferri, F.; Ardizzi, M.; Ambrosecchia, M.; Gallese, V. Closing the gap between the inside and the outside: Interoceptive sensitivity and social distances. PLoS ONE 2013, 8, e75758. [Google Scholar] [CrossRef]
- Herbert, B.M.; Muth, E.R.; Pollatos, O.; Herbert, C. Interoception across modalities: On the relationship between cardiac awareness and the sensitivity for gastric functions. PLoS ONE 2012, 7, e36646. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, W.A.; Jones, G.E. Laterality, emotionality, and heartbeat perception. Psychophysiology 1984, 21, 459–465. [Google Scholar] [CrossRef]
- Margraf, J.; Cwik, J.C.; Pflug, V.; Schneider, S. Structured clinical interviews for mental disorders across the lifespan: Psychometric quality and further developments of the DIPS Open Access interviews. [Strukturierte klinische Interviews zur Erfassung psychischer Störungen über die Lebensspanne: Gütekriterien und Weiterentwicklungen der DIPS-Verfahren.]. Z. Klin. Psychol. Psychother. 2017, 46, 176–186. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373. [Google Scholar]
- World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders: Clinical Descriptions and Diagnostic GuideLines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Stenzel, J.-S.; Höller, I.; Rath, D.; Hallensleben, N.; Spangenberg, L.; Glaesmer, H.; Forkmann, T. Do Feelings of Defeat and Entrapment Change over Time? An Investigation of the Integrated Motivational—Volitional Model of Suicidal Behaviour Using Ecological Momentary Assessments. Int. J. Environ. Res. Public Health 2020, 17, 4685. [Google Scholar] [CrossRef] [PubMed]
- Bornemann, B.; Mehling, W. Multidimensional Assessment of Interoceptive Awareness (MAIA); Sage Publications Sage CA: Los Angeles, CA, USA, 2012. (In German) [Google Scholar]
- Brown, T.A.; Berner, L.A.; Jones, M.D.; Reilly, E.E.; Cusack, A.; Anderson, L.K.; Kaye, W.H.; Wierenga, C.E. Psychometric evaluation and norms for the Multidimensional Assessment of Interoceptive Awareness (MAIA) in a clinical eating disorders sample. Eur. Eat. Disord. Rev. 2017, 25, 411–416. [Google Scholar] [CrossRef]
- Nunan, D.; Jakovljevic, D.G.; Donovan, G.; Hodges, L.D.; Sandercock, G.R.; Brodie, D.A. Levels of agreement for RR intervals and short-term heart rate variability obtained from the Polar S810 and an alternative system. Eur. J. Appl. Physiol. 2008, 103, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Quintana, D.S.; Heathers, J.A.; Kemp, A.H. On the validity of using the Polar RS800 heart rate monitor for heart rate variability research. Eur. J. Appl. Physiol. 2012, 112, 4179–4180. [Google Scholar] [CrossRef]
- Weippert, M.; Kumar, M.; Kreuzfeld, S.; Arndt, D.; Rieger, A.; Stoll, R. Comparison of three mobile devices for measuring R–R intervals and heart rate variability: Polar S810i, Suunto t6 and an ambulatory ECG system. Eur. J. Appl. Physiol. 2010, 109, 779–786. [Google Scholar] [CrossRef]
- Müller, A.M.; Wang, N.X.; Yao, J.; Tan, C.S.; Low, I.C.C.; Lim, N.; Tan, J.; Tan, A.; Müller-Riemenschneider, F. Heart rate measures from wrist-worn activity trackers in a laboratory and free-living setting: Validation study. JMIR mHealth uHealth 2019, 7, e14120. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Use R!); Springer: New York, NY, USA, 2009; Volume 10, pp. 978–970. [Google Scholar]
- Hox, J.H. Multilevel Analysis: Techniques and Application; Routledge: New York, NY, USA, 2010; Volume 2. [Google Scholar]
- Woyshville, M.J.; Lackamp, J.M.; Eisengart, J.A.; Gilliland, J.A. On the meaning and measurement of affective instability: Clues from chaos theory. Biol. Psychiatry 1999, 45, 261–269. [Google Scholar] [CrossRef]
- Fissler, M.; Winnebeck, E.; Schroeter, T.; Gummersbach, M.; Huntenburg, J.M.; Gaertner, M.; Barnhofer, T. An investigation of the effects of brief mindfulness training on self-reported interoceptive awareness, the ability to decenter, and their role in the reduction of depressive symptoms. Mindfulness 2016, 7, 1170–1181. [Google Scholar] [CrossRef]
- Delgado-Pastor, L.C.; Ciria, L.F.; Blanca, B.; Mata, J.L.; Vera, M.N.; Vila, J. Dissociation between the cognitive and interoceptive components of mindfulness in the treatment of chronic worry. J. Behav. Ther. Exp. Psychiatry 2015, 48, 192–199. [Google Scholar] [CrossRef]
- Knapp-Kline, K.; Kline, J.P. Heart rate, heart rate variability, and heartbeat detection with the method of constant stimuli: Slow and steady wins the race. Biol. Psychol. 2005, 69, 387–396. [Google Scholar] [CrossRef]
- Khalsa, S.S.; Rudrauf, D.; Sandesara, C.; Olshansky, B.; Tranel, D. Bolus isoproterenol infusions provide a reliable method for assessing interoceptive awareness. Int. J. Psychophysiol. 2009, 72, 34–45. [Google Scholar] [CrossRef] [Green Version]
- Desmedt, O.; Luminet, O.; Corneille, O. The heartbeat counting task largely involves non-interoceptive processes: Evidence from both the original and an adapted counting task. Biol. Psychol. 2018, 138, 185–188. [Google Scholar] [CrossRef]
- Zamariola, G.; Maurage, P.; Luminet, O.; Corneille, O. Interoceptive accuracy scores from the heartbeat counting task are problematic: Evidence from simple bivariate correlations. Biol. Psychol. 2018, 137, 12–17. [Google Scholar] [CrossRef]
- Füstös, J.; Gramann, K.; Herbert, B.M.; Pollatos, O. On the embodiment of emotion regulation: Interoceptive awareness facilitates reappraisal. Soc. Cogn. Affect. Neurosci. 2013, 8, 911–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werner, N.S.; Jung, K.; Duschek, S.; Schandry, R. Enhanced cardiac perception is associated with benefits in decision-making. Psychophysiology 2009, 46, 1123–1129. [Google Scholar] [CrossRef]
- Ainley, V.; Tsakiris, M.; Pollatos, O.; Schulz, A.; Herbert, B.M. Comment on “Zamariola et al. (2018), Interoceptive Accuracy Scores are Problematic: Evidence from Simple Bivariate Correlations”—The empirical data base, the conceptual reasoning and the analysis behind this statement are misconceived and do not support the authors’ conclusions. Biol. Psychol. 2020, 152, 107870. [Google Scholar] [PubMed]
- Pollatos, O.; Kirsch, W.; Schandry, R. Brain structures involved in interoceptive awareness and cardioafferent signal processing: A dipole source localization study. Hum. Brain Mapp. 2005, 26, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Pollatos, O.; Schandry, R.; Auer, D.P.; Kaufmann, C. Brain structures mediating cardiovascular arousal and interoceptive awareness. Brain Res. 2007, 1141, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Van der Does, A.W.; Antony, M.M.; Ehlers, A.; Barsky, A.J. Heartbeat perception in panic disorder: A reanalysis. Behav. Res. Ther. 2000, 38, 47–62. [Google Scholar] [CrossRef]
- Suschinsky, K.D.; Lalumiere, M.L. Is sexual concordance related to awareness of physiological states? Arch. Sex. Behav. 2012, 41, 199–208. [Google Scholar] [CrossRef]
- Pennebaker, J.W.; Roberts, T.-A. Toward a his and hers theory of emotion: Gender differences in visceral perception. J. Soc. Clin. Psychol. 1992, 11, 199–212. [Google Scholar] [CrossRef]
- Khalsa, S.S.; Lapidus, R.C. Can interoception improve the pragmatic search for biomarkers in psychiatry? Front. Psychiatry 2016, 7, 121. [Google Scholar] [CrossRef]
- Khalsa, S.S.; Adolphs, R.; Cameron, O.G.; Critchley, H.D.; Davenport, P.W.; Feinstein, J.S.; Feusner, J.D.; Garfinkel, S.N.; Lane, R.D.; Mehling, W.E.; et al. Interoception and Mental Health: A Roadmap. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 501–513. [Google Scholar] [CrossRef]
- Paulus, M.P.; Feinstein, J.S.; Khalsa, S.S. An active inference approach to interoceptive psychopathology. Annu. Rev. Clin. Psychol. 2019, 15, 97–122. [Google Scholar] [CrossRef]
- Critchley, H.; Ewing, D.L.; Gould van Praag, C.; Habash-Bailey, H.; Eccles, J.; Meeten, F.; Garfinkel, S.N. Transdiagnostic Expression of Interoceptive Abnormalities in Psychiatric Conditions. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Construct and Items | T0 1 | T2 1 | EMA 2 | MSSD (EMA Items) | ICC | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | Min. | Max | M | SD | Min | Max | M | SD | Min. | Max | M | SD | Min | Max | ||
| Interoceptive Accuracy (HPT) | 0.58 | 0.10 | 0.26 | 0.79 | 0.60 | 0.11 | 0.24 | 0.82 | 0.72 | 0.18 | 0.12 | 0.90 | 0.05 | 0.05 | 0.01 | 0.27 | 0.42 |
| Interoceptive Awawareness | −7.62 | 23.62 | −52.28 | 50.56 | −7.75 | 23.25 | −58.20 | 56.03 | −21.99 | 28.15 | −62.41 | 69.06 | 720.62 | 493.06 | 79.85 | 2006.43 | 0.63 |
| Interoceptive Sensibility 3 | |||||||||||||||||
| Noticing | 3.28 | 0.79 | 1.50 | 5.00 | 3.52 | 0.72 | 1.00 | 5.00 | 3.49 | 0.73 | 1.97 | 5.00 | 0.72 | 1.08 | 0.00 | 5.82 | 0.56 |
| Not-Distracting | 2.24 | 0.87 | 0.33 | 4.33 | 2.16 | 0.83 | 0.67 | 4.33 | 4.17 | 0.61 | 3.06 | 4.97 | 0.87 | 0.87 | 0.03 | 4.79 | 0.42 |
| Not-Worrying | 2.61 | 0.96 | 0.33 | 5.00 | 2.55 | 0.94 | 0.33 | 5.00 | 4.46 | 0.62 | 2.70 | 5.00 | 0.61 | 0.90 | 0.00 | 4.79 | 0.52 |
| Attention Regulation | 2.96 | 0.75 | 1.14 | 4.43 | 2.95 | 0.84 | 1.14 | 4.71 | 2.60 | 0.69 | 1.29 | 3.95 | 1.26 | 0.91 | 0.06 | 4.39 | 0.38 |
| Emotional Awareness | 3.43 | 0.94 | 1.20 | 5.00 | 3.67 | 0.77 | 1.40 | 5.00 | 3.40 | 0.85 | 1.09 | 4.97 | 0.78 | 0.97 | 0.00 | 5.44 | 0.62 |
| Self-Regulation | 2.72 | 1.07 | 0.25 | 5.00 | 2.77 | 1.14 | 0.00 | 5.00 | 3.07 | 0.92 | 1.20 | 4.85 | 0.76 | 1.07 | 0.00 | 6.11 | 0.62 |
| Body Listening | 2.66 | 0.99 | 0.00 | 5.00 | 2.90 | 1.02 | 0.67 | 5.00 | 3.28 | 0.83 | 1.03 | 4.58 | 0.95 | 1.42 | 0.00 | 7.00 | 0.56 |
| Trusting | 3.89 | 0.93 | 0.33 | 5.00 | 4.05 | 0.83 | 1.33 | 5.00 | 4.08 | 0.74 | 2.50 | 5.00 | 0.65 | 1.35 | 0.00 | 7.52 | 0.61 |
| Effects | F | p | η2 | |
|---|---|---|---|---|
| Interoceptive Accuracy | ||||
| Interaction effect | Time * Group | 0.26 | 0.614 | .004 |
| Within-subject effect | Time | 1.74 | 0.193 | .029 |
| Between-subject effect | Group | 1.13 | 0.292 | .019 |
| Interoceptive Awawareness | ||||
| Interaction effect | Time * Group | 0.15 | 0.697 | 0.003 |
| Within-subject effect | Time | 0.00 | 0.952 | 0.000 |
| Between-subject effect | Group | 0.05 | 0.828 | 0.001 |
| Interoceptive Sensibility: MAIA scales | ||||
| Interaction effect | Time (Noticing 1) * Group | 0.98 | 0.327 | 0.016 |
| Within-subject effect | Time (Noticing 1) | 5.17 | 0.027 * | 0.081 |
| Between-subject effect | Group | 0.85 | 0.359 | 0.014 |
| Interaction effect | Time (Not-Distracting 1) * Group | 0.01 | 0.937 | 0.000 |
| Within-subject effect | Time (Not-Distracting1) | 0.96 | 0.331 | 0.016 |
| Between-subject effect | Group | 3.42 | 0.070 | 0.90 |
| Interaction effect | Time (Not-Worrying 1) * Group | 0.15 | 0.703 | 0.002 |
| Within-subject effect | Time (Not-Worrying 1) | 0.40 | 0.532 | 0.007 |
| Between-subject effect | Group | 1.81 | 0.184 | 0.030 |
| Interaction effect | Time (Attention Regulation 1) * Group | 3.96 | 0.051 * | 0.063 |
| Within-subject effect | Time (Attention Regulation1) | 0.06 | 0.808 | 0.001 |
| Between-subject effect | Group | 4.13 | 0.047 * | 0.065 |
| Interaction effect | Time (Emotional Awareness 1) * Group | 0.62 | 0.434 | 0.010 |
| Within-subject effect | Time (Emotional Awareness 1) | 5.48 | 0.023 * | 0.085 |
| Between-subject effect | Group | 0.26 | 0.612 | 0.004 |
| Interaction effect | Time (Self-Regulation 1) * Group | 1.98 | 0.165 | 0.032 |
| Within-subject effect | Time (Self-Regulation 1) | 0.23 | 0.636 | 0.004 |
| Between-subject effect | Group | 2.76 | 0.102 | 0.045 |
| Interaction effect | Time (Body Listening 1) * Group | 2.25 | 0.139 | 0.037 |
| Within-subject effect | Time (Body Listening 1) | 4.04 | 0.049 * | 0.064 |
| Between-subject effect | Group | 2.97 | 0.090 | 0.048 |
| Interaction effect | Time (Trusting 1) * Group | 1.29 | 0.261 | 0.021 |
| Within-subject effect | Time (Trusting 1) | 3.09 | 0.084 | 0.050 |
| Between-subject effect | Group | 1.30 | 0.260 | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Höller, I.; Stenzel, J.-S.; Rath, D.; Forkmann, T. Listen to Your Heart–Ecological Momentary Assessment of Interoceptive Accuracy, Awareness and Sensibility: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 4893. https://doi.org/10.3390/ijerph18094893
Höller I, Stenzel J-S, Rath D, Forkmann T. Listen to Your Heart–Ecological Momentary Assessment of Interoceptive Accuracy, Awareness and Sensibility: A Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4893. https://doi.org/10.3390/ijerph18094893
Chicago/Turabian StyleHöller, Inken, Jana-Sophie Stenzel, Dajana Rath, and Thomas Forkmann. 2021. "Listen to Your Heart–Ecological Momentary Assessment of Interoceptive Accuracy, Awareness and Sensibility: A Pilot Study" International Journal of Environmental Research and Public Health 18, no. 9: 4893. https://doi.org/10.3390/ijerph18094893