
LONG-REMI: An AI-Based Technological Application to Promote Healthy Mental Longevity Grounded in Reminiscence Therapy

 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Reminiscence Therapy
1.2. State of the Art
- AlzhUp: Personal memory bank to which the caregiver and family members can contribute. It also incorporates aerobic, calculation, memory, or relaxation games and exercises [28].
- Memory Box: Aims to stimulate long-term memory by storing photographs and audios of everyday experiences while also encouraging conversations and exchanges between an elderly person and the caregiver or family member [29].
- Refresh My Memory—An application to help remember objects and their location, as well as people in the user’s environment [30].
- YoTeCuido Alzheimer: Support application for caregivers and patients. It provides information about Alzheimer’s disease and allows establishing routines and exercises. The main novelty of its contents compared to other available apps is that they are based on the experience of caregivers and family members, as well as patients and professional caregivers [31].
- Backup Memory: Creates a memory album. The app reminds users of their relationship with each family member by showing them photos and videos of past experiences they shared with their family member [32].
- Imentia: Cognitive stimulation based on a series of interactive exercises that train the different cognitive areas: memory, orientation, language, attention, reasoning, comprehension, etc. Each work area has different levels of complexity [33].
- NoMeOlvides: Application made up of a series of mini-games classified in different categories, such as shapes, colors, addition and subtraction, animals, and objects. It uses an assistant that guides the user through the application [34].
- Andzheimer: Through different graphic exercises divided into their corresponding cognitive areas, it tries to enhance memory, attention, language, executive functions, etc. [35].
- Stimulus: It is based on a series of interactive exercises that train the different cognitive processes, attention, perception, working memory, long-term memory, calculation, reasoning, executive functions, etc. [36].
2. Materials and Methods
2.1. Intangible Cultural Heritage Material
2.2. AI-Based Application Development
- An internal storage structure for the material that makes up the intangible cultural heritage, as well as patient information. With patient information, we refer both to the characteristics of each patient (age, place of birth, place where they live, level of cognitive impairment, can or cannot read) and to the knowledge that the application acquires as the user progresses in RT (what type of activities and cultural heritage causes reminiscence reactions, what type of cultural heritage do they like more, i.e., tongue twisters, songs, proverbs, or dances).
- A specific technique for facial emotion recognition focusing on the analysis of the expression of the mouth and eyes. Our approach is framed in the area of face tracking. On the basis of the identified shape of the mouth and the degree of eye opening, it defines a smile index in the range [0, 1]. This index indicates confidence in the presence of a smile. For example, a value equal to or greater than 0.7 indicates the likelihood that a person is smiling is very high.
- An algorithm for optimal pathfinding maximizing the possibility of reminiscence dynamically, depending on the emotions of the person performing the RT. This algorithm aims to guide the application by the cultural heritage introduced in the internal storage structure considering the person who is using the system, their personal characteristics, and the reminiscences detected throughout the therapy session. Therefore, the program learns from the user’s reactions, in order to provide the best therapeutic stimuli at each moment.
- A large set of activities of the different representations of intangible cultural heritage, i.e., proverbs, tongue twisters, songs, and dances.
2.3. Face Emotion Recognition
2.4. Path Finding Algorithm
2.5. App Activities
- Audio/video is presented showing one or more people singing a traditional song. The user listens to the song.
- Users are asked several questions about the song they have heard: Do you know the song? Do you remember who sang it? Who did you sing it with or listen to it with? Do you usually sing it? The user selects an answer from the displayed list.
- A list of music topics is displayed. Users are asked which topic(s) they like the most. The user selects an answer from the displayed list.
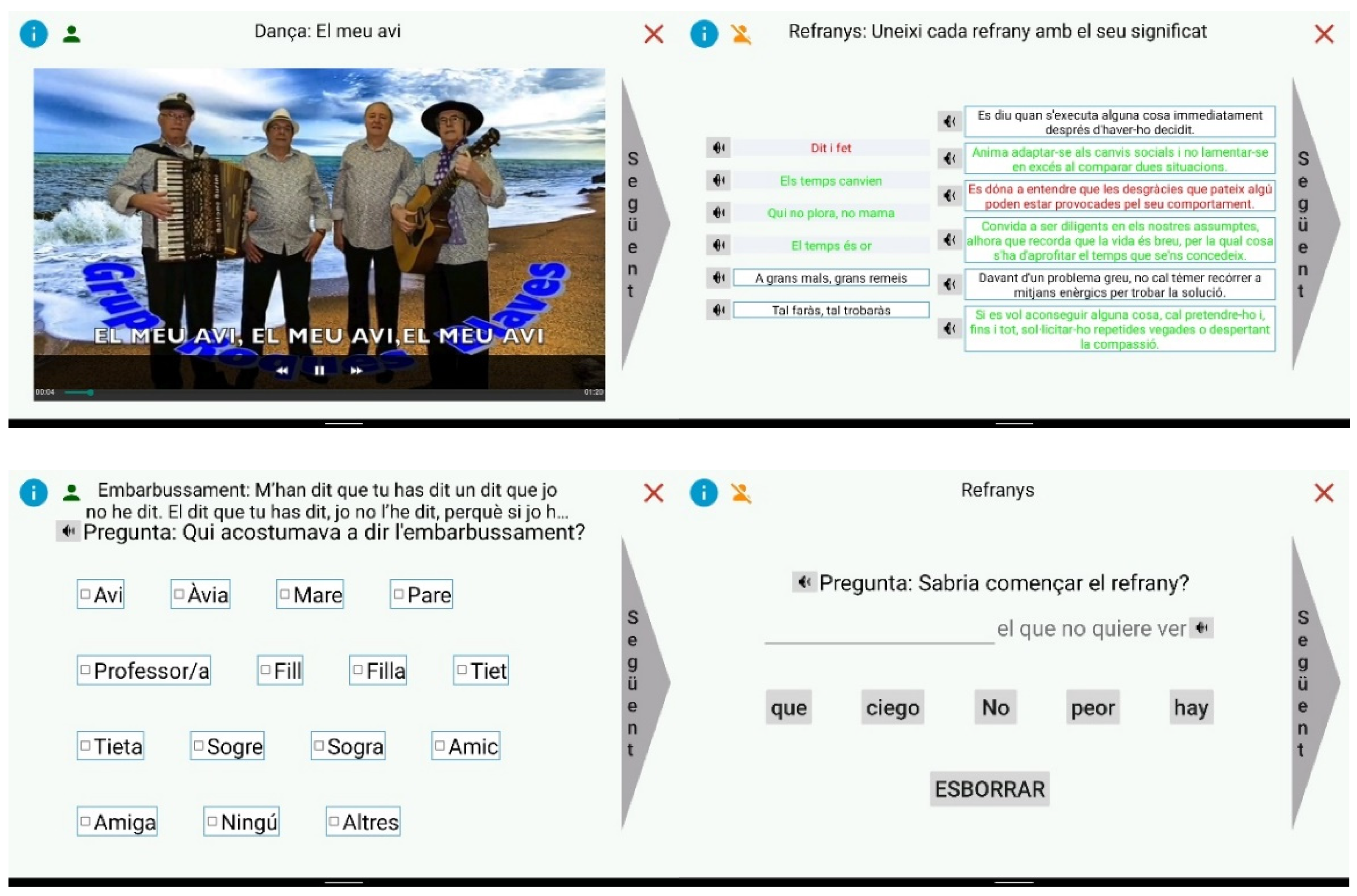
- The activities associated with the dances are the same as those discussed for the songs, adapting the questions to be consistent.
- The activities associated with tongue twisters are the same as those listed for songs. These activities are presented by voice and also by text that appears on the screen.
- The whole proverb is shown. The user is asked several questions: Have you heard it before? Do you remember who said it? Do you usually use it?. The user selects an answer from the displayed list.
- The first part of the proverb is shown. The user must finish the proverb by selecting the words that appear unordered on the screen or by typing the text from a keyboard.
- The second part of the proverb is displayed. The user must complete the proverb by selecting the words that appear unordered on the screen or by typing the text from a keyboard.
- A list of n proverbs (default n = 3) is displayed on the left-hand side of the screen, and a list of their unordered meanings is displayed on the right-hand side. The user has to match each proverb with its meaning.
- A list of the first part of n proverbs (default n = 3) is displayed on the left-hand side of the screen, and a list of the second part of the previous n proverbs is displayed unordered on the right-hand side of the screen. The user must join the two parts of each proverb.
- A proverb and a list of categories are displayed. The user must select the category to which the proverb belongs.
- A proverb is shown leaving one or more empty words. A list of words is also displayed. The user must complete the proverb by selecting the correct words.
- A proverb is displayed, and the system asks the user to read it. The user’s voice is recorded and used in case the proverb comes up again in any of the subsequent RT sessions.
2.6. Pilot Study and Participants
2.7. Intervention Program
2.8. Clinical Evaluation and Outcome Variables
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eurostat. Increase in the Share of the Population Aged 65 Years or over between 2011 and 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed on 25 January 2022).
- Woods, B.; Thorgrimsen, L.; Spector, A.; Royan, L.; Orrell, M. Improved quality of life and cognitive stimulation therapy in dementia. Aging Ment. Health 2006, 10, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Daviglus, M.L.; Bell, C.C.; Berrettini, W.; Bowen, P.E.; Connolly, E.S., Jr.; Cox, N.J.; Dunbar-Jacob, J.M.; Granieri, E.C.; Hunt, G.; McGarry, K.; et al. National Institutes of Health State-of the-Science Conference statement: Preventing alzheimer disease and cognitive decline. Ann. Intern. Med. 2010, 153, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Bahar-Fuchs, A.; Martyr, A.; Goh, A.; Sabates, J.; Clare, L. Cognitive training for people with mild to moderate dementia. Cochrane Database Syst. Rev. 2019, 3, CD013069. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; O’Philbin, L.; Farrell, E.M.; Spector, A.E.; Orrell, M. Reminiscence therapy for dementia. Cochrane Database Syst. Rev. 2018, 3, CD001120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuevas, P.E.G.; Davidson, P.M.; Mejilla, J.L.; Rodney, T.W. Reminiscence therapy for older adults with Alzheimer’s disease: A literature review. Int. J. Ment. Health Nurs. 2020, 29, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Westerhof, G.J.; Bohlmeijer, E.T. Celebrating fifty years of research and applications in reminiscence and life review: State of the art and new directions. J. Aging Stud. 2014, 29, 107–114. [Google Scholar] [CrossRef]
- Ryan, A.A.; McCauley, C.O.; Laird, E.A.; Gibson, A.; Mulvenna, M.D.; Bond, R.; Bunting, B.; Curran, K.; Ferry, F. ‘There is still so much in-side’: The impact of personalised reminiscence, facilitated by a tablet device, on people living with mild to moderate dementia and their family carers. Dementia 2020, 19, 1131–1150. [Google Scholar] [CrossRef]
- Robertson, L.T. Memory and the brain. J. Dent. Educ. 2002, 66, 30–42. [Google Scholar] [CrossRef]
- Dementia: Supporting People with Dementia and Their Carers in Health and Social Care: Guidance, NICE. Available online: http://www.nice.org.uk/guidance/cg42 (accessed on 30 January 2022).
- Calero, M.D.; Navarro, E. Cognitive plasticity as a modulating variable on the effects of memory training in elderly persons. Arch. Clin. Neuropsychol. 2007, 22, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Arroyo-Anlló, E.M. Estimulación psicocognoscitiva en las demencias: Programas de talleres de estimulación. Prous Sci. 2002, 128, 405–422. [Google Scholar]
- Woods, B.; Spector, A.E.; Jones, C.A.; Orrell, M.; Davies, S.P. Reminiscence therapy for dementia. Cochrane Database Syst. Rev. 2005, 2, CD001120. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Cleary, S.J.; Hopper, T.; Bayles, K.A.; Mahendra, N.; Azuma, T.; Rackley, A. Evidence-based practice recommendations for working with individuals with dementia. J. Med. Speech-Lang. Pathol. 2006, 14, xxiii. [Google Scholar]
- Chiang, K.J.; Chu, H.; Chang, H.J.; Chung, M.H.; Chen, C.H.; Chion, H.Y.; Chou, K.R. The effects of reminiscence therapy on phychosocial well being, depression, and loneliness among the institutionalized aged. Int. J. Geriatr. Psychiatry 2010, 25, 380–388. [Google Scholar] [CrossRef]
- Coll-Planas, L.; Watchman, K.; Doménech, S.; McGillivray, D.; O’Donnell, H.; Tolson, D. Developing Evidence for Football (Soccer) Reminiscence Interventions Within Long-term Care: A Cooperative Approach Applied in Scotland and Spain. J. Am. Med. Dir. Assoc. 2017, 18, 355–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Shea, E.; Devane, D.; Cooney, A.; Casey, D.; Jordan, F.; Hunter, E.M.; Newell, J.; Connolly, S.; Murphy, K. The impact of reminiscence on the quality of life of residents with dementia in longstay care. Int. J. Geriatr. Psychiatry 2014, 29, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Cotelli, M.; Manenti, R.; Zanetti, O. Reminiscence therapy in dementia: A review. Maturitas 2012, 72, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.C.; Chen, Y.T.; Chen, P.Y.; Huey-Lan Hu, S.; Liu, F.; Kuo, Y.L.; Chiu, H.Y. Reminiscence Therapy Improves Cognitive Functions and Reduces Depressive Symptoms in Elderly People with Dementia: A Meta-Analysis of Randomized Controlled Trials. J. Am. Med. Dir. Assoc. 2015, 16, 1087–1094. [Google Scholar] [CrossRef]
- Satorres, E.; Viguer, P.; Fortuna, F.B.; Meléndez, J.C. Effectiveness of instrumental reminiscence intervention on improving coping in healthy older adults. Stress and Health 2018, 34, 227–234. [Google Scholar] [CrossRef]
- Alzheimer’s Association Report. 2020 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2020, 16, 391–460. [Google Scholar] [CrossRef]
- Guo, Y.; Yang, F.; Hu, F.; Li, W.; Ruggiano, N.; Lee, H.Y. Existing Mobile Phone Apps for Self-Care Management of People with Alzheimer Disease and Related Dementias: Systematic Analysis. JMIR Aging 2020, 3, e15290. [Google Scholar] [CrossRef] [Green Version]
- Klimova, B. Mobile Phone Apps in the Management and Assessment of Mild Cognitive Impairment and/or Mild-to-Moderate Dementia: An Opinion Article on Recent Findings. Front. Hum. Neurosci. 2017, 11, 461. [Google Scholar] [CrossRef] [PubMed]
- Lazar, A.; Thompson, H.; Demiris, G. A systematic review of the use of technology for reminiscence therapy. Health Educ. Behav. 2014, 41, 51–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarne-Fleischmann, V.; Tractinsky, N.Y.; Dwolatzky, T.; Rief, I. Personalized reminiscence therapy for patients with Alzheimer’s disease using a computerized system. In Proceedings of the 4th International Conference on PErvasive Technologies Related to Assistive Environments, Heraklion, Greece; 2011; pp. 1–4. [Google Scholar]
- Yu, F.; Mathiason, M.A.; Johnson, K.; Gaugler, J.E.; Klassen, D. Memory matters in dementia: Efficacy of a mobile reminiscing therapy app. Alzheimer’s Dement. 2019, 5, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, S.; Brill, M.; Whalley, J.H.; Read, R.; Anderson, G.; Edwards, S.; Picking, R. Assessing Wellbeing in People Living with Dementia Using Reminiscence Music with a Mobile App (Memory Tracks): A Mixed Methods Cohort Study. J. Healthc. Eng. 2019, 2019, 8924273. [Google Scholar] [CrossRef] [Green Version]
- Guia de Mayores. Alzhup una App para Intentar Combatir el Alzheimer. Available online: https://guiademayores.com/2016/10/13/alzhup-una-app-intentar-combatir-alzheimer/ (accessed on 25 January 2022).
- Memory Box Stories, AppAdvice. Available online: https://appadvice.com/app/memory-box-stories/588677432 (accessed on 30 January 2022).
- Refresh My Memory, Wiki Nuevas Tecnologías en el Ámbito Sanitario. Available online: https://nntt-uma.fandom.com/es/wiki/Refresh_My_Memory (accessed on 30 January 2022).
- Yotecuido, YoTeCuido Alzhéimer: La App Para Cuidadores y Afectados de Alzhéimer. Available online: http://www.yotecuidoalzheimer.com/ (accessed on 30 January 2022).
- Samsung Releases Backup Memory App for Alzheimer’s Patients, MobiHealthNews. Available online: https://www.mobihealthnews.com/43023/samsung-releases-backup-memory-app-for-alzheimers-patients (accessed on 30 January 2022).
- Imentia. Available online: https://www.imentia.com/ (accessed on 30 January 2022).
- App De Juegos Para Alzheimer–Nomeolvides. Available online: https://www.accesibles.org/app-de-juegos-para-alzheimer-nomeolvides/ (accessed on 30 January 2022).
- La App Que Ayuda a Mejorar Las Capacidades Cognitivas De Los Pacientes Con Alzhimer., ANDZHEIMER, 1 April 2014. Available online: http://www.arananet.net/andzheimer/ (accessed on 30 January 2022).
- App Profesional de Estimulación Cognitiva, Stimulus. Available online: https://stimuluspro.com/ (accessed on 30 January 2022).
- Caros, M.; Garolera, M.; Radeva, P.; Giro-i-Nieto, X. Automatic Reminiscence Therapy for Dementia. 2019. Available online: http://arxiv.org/abs/1910.11949 (accessed on 11 January 2022).
- Matías Guiu, J.A.; Pérez Martínez, D.A.; Matías Guiu, J. A pilot study of a new method of cognitive stimulation using abacus arithmetic in healthy and cognitively impaired elderly subjects. Neurología 2016, 31, 326–331. [Google Scholar] [CrossRef]
- Mahendran, R.; Rawtaer, I.; Fam, J.; Wong, J.; Kumar, A.P.; Gandhi, M.; Jing, K.X.; Feng, L.; Kua, E.H. Art therapy and music reminiscence activity in the prevention of cognitive decline: Study protocol for a randomized controlled trial. Trials 2017, 18, 324. [Google Scholar] [CrossRef] [Green Version]
- Pöllänen, S.H.; Hirsimäki, R.M. Crafts as memory triggers in reminiscence: A case study of older women with dementia. Occup. Ther. Health Care 2014, 28, 410–430. [Google Scholar] [CrossRef] [Green Version]
- Keating, F.; Cole, L.; Grant, R. An evaluation of group reminiscence arts sessions for people with dementia living in care homes. Dementia 2020, 19, 805–821. [Google Scholar] [CrossRef] [Green Version]
- Viejo-Rose, D. Cultural heritage and memory: Untangling the ties that bind. Cult. Hist. Digit. J. 2015, 4, e018. [Google Scholar] [CrossRef] [Green Version]
- ML Kit SDK, Google Developers. Available online: https://developers.google.com/ml-kit/guides (accessed on 30 January 2022).
- Reisberg, B.; Ferris, S.H.; de Leon, M.J.; Crook, T. The Global Deterioration Scale for Assessments of Primary Degenerative Dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatry Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Watson, D. Intraindividual and interindividual analyses of positive and negative affect: Their relation to health complaints, perceived stress, and daily activities. J. Personal. Soc. Psychol. 1988, 54, 1020–1030. [Google Scholar] [CrossRef]
- Gould, D.; Phil, M.; Kelly, D.; Goldstone, L.; Gammon, J. Visual Analogue Scale (VAS). J. Clin. Nurs. 2001, 10, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Sauro, J.; Lewis, J.R. Quantifying the User Experience: Practical Statistics for User Research; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar] [CrossRef]
- Hedlefs, M.I.; de la Garza, A.; Sánchez, M.P.; Garza, A.A. Adaptación al español del Cuestionario de Usabilidad de Sistemas Informáticos CSUQ. RECI Rev. Iberoam. De Las Cienc. Comput. E Inf. 2015, 4, 84–99. [Google Scholar]
- Robles, R.; Páez, F. Estudio sobre la traducción al español y las propiedades psicométricas de las escalas de afecto positivo y negativo (PANAS). Salud Ment. 2003, 26, 69–75. [Google Scholar]
- SPSS Software, IBM. Available online: https://www.ibm.com/analytics/spss-statistics-software (accessed on 30 January 2022).
- Beauchamp, T.L.; Childress, J.F. Principles of Biomedical Ethics, 5th ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| People without Cognitive Impairment (n = 21) | People with Cognitive Impairment (n = 21) | |
|---|---|---|
| Age M ± SD (ranges) | 76.67 ± 6.55 (66–87) | 81.76 ± 7.08 (68–94) |
| Gender % women | 66.2 (14 participants) | 76.19 (16 participants) |
| Education level | 100 (21 participants) | |
| Low | 38.1 (8 participants) | |
| Medium | 47.6 (10 participants) | |
| High | 14.3 (3 participants) | |
| MMSE M ± SD (ranges) | 22.60 ± 5.48 (13–30) |
| People without Cognitive Impairment (n = 21) | People with Cognitive Impairment (n = 21) | |
|---|---|---|
| Usability | 8.29 ± 1.59 | 7.43 ± 2.38 |
| Satisfaction | 8.57 ± 1.78 | 8.29 ± 1.42 |
| CSUQ | ||
| Overall score | 6.95 ± 0.22 | 5.64 ± 1.06 |
| System utility | 6.35 ± 0.97 | 5.83 ± 1.02 |
| Information quality | 6.04 ± 1.15 | 6.04 ± 0.72 |
| Interface quality | 6.71 ± 0.67 | 5.74 ± 1.07 |
| PANAS | Pre Intervention | Post Intervention | p-Value |
|---|---|---|---|
| People without cognitive impairment | |||
| Positive affect subscale | 31.81 ± 8.32 | 40.52 ± 10.17 | 0.001 |
| Negative affect subscale | 11.76 ± 2.32 | 11.62 ± 2.54 | 0.775 |
| People with cognitive impairment | |||
| Positive affect subscale | 24.29 ± 8.39 | 34.57 ± 9.12 | 0.000 |
| Negative affect subscale | 12.24 ± 3.42 | 12.33 ± 3.32 | 0.975 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nebot, À.; Domènech, S.; Albino-Pires, N.; Mugica, F.; Benali, A.; Porta, X.; Nebot, O.; Santos, P.M. LONG-REMI: An AI-Based Technological Application to Promote Healthy Mental Longevity Grounded in Reminiscence Therapy. Int. J. Environ. Res. Public Health 2022, 19, 5997. https://doi.org/10.3390/ijerph19105997
Nebot À, Domènech S, Albino-Pires N, Mugica F, Benali A, Porta X, Nebot O, Santos PM. LONG-REMI: An AI-Based Technological Application to Promote Healthy Mental Longevity Grounded in Reminiscence Therapy. International Journal of Environmental Research and Public Health. 2022; 19(10):5997. https://doi.org/10.3390/ijerph19105997
Chicago/Turabian StyleNebot, Àngela, Sara Domènech, Natália Albino-Pires, Francisco Mugica, Anass Benali, Xènia Porta, Oriol Nebot, and Pedro M. Santos. 2022. "LONG-REMI: An AI-Based Technological Application to Promote Healthy Mental Longevity Grounded in Reminiscence Therapy" International Journal of Environmental Research and Public Health 19, no. 10: 5997. https://doi.org/10.3390/ijerph19105997
APA StyleNebot, À., Domènech, S., Albino-Pires, N., Mugica, F., Benali, A., Porta, X., Nebot, O., & Santos, P. M. (2022). LONG-REMI: An AI-Based Technological Application to Promote Healthy Mental Longevity Grounded in Reminiscence Therapy. International Journal of Environmental Research and Public Health, 19(10), 5997. https://doi.org/10.3390/ijerph19105997