
Relationship between Health Counselor Characteristics and Counseling Impact on Individuals at High-Risk for Lifestyle-Related Disease: Sub-Analysis of the J-HARP Cluster-Randomized Controlled Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Characteristics
2.2. Health Counselor Characteristics
2.3. Health Counseling
- (a)
- Mechanisms by which hypertension, hyperglycemia, and high levels of low-density lipoprotein cholesterol contribute to atherosclerosis (large vessel pathology), arteriolosclerosis (small vessel pathology), cardiovascular sclerotic arteriosclerotic diseases, and chronic kidney disease;
- (b)
- Health checkup result assessment skills to explain the pathophysiology of outcomes;
- (c)
- Need for medical treatment of hypertension, diabetes, high low-density lipoprotein cholesterol levels, and chronic kidney disease;
- (d)
- How to use information on health insurance claims;
- (e)
- Methods and implementation of health counseling based on the modified health belief model;
- (f)
- How to deal with negative responses from participants;
- (g)
- How to cooperate with primary care physicians.
2.4. Counseling Time and Mode
2.5. Surveillance for Clinic Visits
2.6. Statistical Analysis
2.7. Ethical Approval and Informed Consent
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- World Health Organization. Global Status Report on Noncommunicable Diseases. World Health Organization. 2014. Available online: https://apps.who.int/iris/handle/10665/148114 (accessed on 1 May 2022).
- Lechner, K.; von Schacky, C.; McKenzie, A.L.; Worm, N.; Nixdorff, U.; Lechner, B.; Kränkel, N.; Halle, M.; Krauss, R.; Scherr, J. Lifestyle factors and high-risk atherosclerosis: Pathways and mechanisms beyond traditional risk factors. Eur. J. Prev. Cardiol. 2020, 27, 394–406. [Google Scholar] [CrossRef] [Green Version]
- Fukuma, S.; Ikenoue, T.; Saito, Y.; Yamada, Y.; Saigusa, Y.; Misumi, T.; Masataka, T. Lack of a bridge between screening and medical management for hypertension: Health screening cohort in Japan. BMC Public Health 2020, 20, 1419. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, A.; Takahashi, Y.; Tsujimura, Y.; Miyazaki, K.; Satoh, T.; Ikeda, S.; Nakayama, T. Predicting failure to follow-up screened high blood pressure in Japan: A cohort study. J. Public Health 2015, 37, 498–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarado, M.; Murphy, M.M.; Guell, C. Brriers and facilitators to physical activity amongst overweight and obese women in an Afro-Caribbean population: A qualitative study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandel, P.; Lim, S.; Pirotta, S.; Skouteris, H.; Moran, L.J.; Hill, B. Enablers and barriers to women’s lifestyle behavior change during the preconception period: A systematic review. Obes. Rev. 2021, 22, e13235. [Google Scholar] [CrossRef]
- Dillon, P.; Smith, S.M.; Gallagher, P.; Cousins, G. Impact of financial burden, resulting from prescription co-payments, on antihypertensive medication adherence in an older publically insured population. BMC Public Health 2018, 18, 1282. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, M.; Kojima, S.; Sairenchi, T.; Kinuta, M.; Yamakawa, M.; Nishizawa, H.; Takahara, M.; Imano, H.; Kitamura, I.; Yoshida, T.; et al. Study profile Japan trial in high-risk individuals to enhance their referral to physicians (J-HARP)—A nurse-led, community-based prevention program of lifestyle-related disease. J. Epidemiol. 2019, 4, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Iso, H. Report of the Comprehensive Research on Strategic Studies for Prevention of Severe Lifestyle-Related Diseases, Funded by the Health, Labour and Welfare Science Research Grants. 2017. Available online: http://www.pbhel.med.osaka-u.ac.jp/common/images/pdf/themes/jharp/sougou_1.pdf (accessed on 1 May 2022). (In Japanese).
- Rosenstock, I.M. The health belief model and preventive health behavior. Health Educ. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Campbell, L.A.; Harmon, M.J.; Joyce, B.L.; Little, S.H. Quad Council Coalition community/public health nursing competencies: Building consensus through collaboration. Public Health Nurs. 2020, 37, 96–112. [Google Scholar] [CrossRef] [Green Version]
- Colley, S.K.; Kane, P.K.M.; Gibson, J.M. Risk Communication and Factors Influencing Private Well Testing Behavior: A Systematic Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 4333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, M.; Miyaji, F.; Akimoto, R. The public health nursing role in rural Japan. Public Health Nurs. 2005, 22, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Meretoja, R.; Eriksson, E.; Leino-Kilpi, H. Indicators for competent nursing practice. J. Nurs. Manag. 2002, 10, 95–102. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Adherence to Long-Term Therapies: Evidence for Action. 2003. Available online: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf (accessed on 1 May 2022).
- Calonge Pascual, S.; Casajús Mallén, J.A.; González-Gross, M. Adherence Factors Related to Exercise Prescriptions in Healthcare Settings: A Review of the Scientific Literature. Res. Q. Exerc. Sport 2022, 93, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Glavin, K.; Schaffer, M.A.; Halvorsrud, L.; Kvarme, L.G. A comparison of the cornerstones of public health nursing in Norway and in the United States. Public Health Nurs. 2014, 31, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Nigenda, G.; Magaña-Valladares, L.; Cooper, K.; Ruiz-Larios, J.A. Recent developments in public health nursing in the Americas. Int. J. Environ. Res. Public Health 2010, 7, 729–750. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Overview of the Year 2020. Health Administration Report (Employment Medical Professionals). Available online: https://www.mhlw.go.jp/toukei/saikin/hw/eisei/20/dl/gaikyo.pdf (accessed on 1 May 2022).

{kind=link}
| Profession | Public Health Nurse | Clinical Nurse | Nutritionist | |||
|---|---|---|---|---|---|---|
| Characteristics of participants | ||||||
| Number of participants | 6219 | 596 | 892 | |||
| Age, years, mean ± SD | 63.1 | ±8.5 | 63.8 | ±8.2 | 64.4 | ±7.9 |
| Men, n (%) | 4139 | (66.6) | 352 | (59.1) | 583 | (65.4) |
| Grade II or higher hypertension, n (%) | 3619 | (58.2) | 338 | (56.7) | 520 | (58.3) |
| Diabetes mellitus, n (%) | 1184 | (19.0) | 119 | (20.0) | 161 | (18.1) |
| Dyslipidemia among men, n (%) | 1410 | (34.3) | 107 | (30.6) | 220 | (38.1) |
| Proteinuria, n (%) | 606 | (9.8) | 91 | (15.4) | 92 | (10.3) |
| Characteristics of counselors | ||||||
| Women, n (%) | 6142 | (98.8) | 596 | (100.0) | 881 | (98.8) |
| Men, n (%) | 77 | (1.2) | 0 | (0.0) | 11 | (1.2) |
| Age, years, mean ± SD | 39.5 | ±9.6 | 51.7 | ±6.4 | 39.4 | ±9.4 |
| Years of experience in general counseling, mean ± SD | 12.2 | ±10.1 | 9.9 | ±6.6 | 6.5 | ±8.3 |
| <3, n (%) | 1511 | (24.3) | 92 | (15.4) | 456 | (51.1) |
| 3–9, n (%) | 1629 | (26.2) | 251 | (42.1) | 274 | (30.7) |
| 10–19, n (%) | 1466 | (23.6) | 224 | (37.6) | 87 | (9.8) |
| ≥20, n (%) | 1611 | (25.9) | 29 | (4.9) | 75 | (8.4) |
| Years of experience for lifestyle-related disease counseling, mean ± SD | 4.3 | ±5.3 | 8.7 | ±6.1 | 3.4 | ±3.6 |
| <3, n (%) | 3418 | (55.0) | 111 | (18.6) | 503 | (56.4) |
| 3–5, n (%) | 1493 | (24.0) | 87 | (14.6) | 311 | (34.9) |
| ≥6, n (%) | 1303 | (21.0) | 398 | (66.8) | 78 | (8.7) |
| Counseling mode, n (%) | ||||||
| Home visit | 3375 | (54.3) | 418 | (70.1) | 402 | (45.1) |
| Face-to-face in a public place | 1694 | (27.2) | 33 | (5.5) | 281 | (31.5) |
| Telephone | 307 | (4.9) | 33 | (5.5) | 36 | (4.0) |
| Incomplete | 845 | (13.6) | 112 | (18.8) | 173 | (19.4) |
| Initial timing, n (%) | ||||||
| ≤45 days | 2489 | (40.0) | 42 | (7.1) | 287 | (32.2) |
| 46–90 days | 1688 | (27.1) | 109 | (18.3) | 257 | (28.8) |
| ≥91 days | 1335 | (21.5) | 337 | (56.5) | 189 | (21.2) |
| Incomplete | 707 | (11.4) | 108 | (18.1) | 159 | (17.8) |
| Number of counseling sessions, n (%) | ||||||
| 1 | 2566 | (41.3) | 250 | (42.0) | 332 | (37.2) |
| 2 | 1753 | (28.2) | 205 | (34.4) | 223 | (25.0) |
| 3 | 1250 | (20.1) | 47 | (7.9) | 182 | (20.4) |
| Incomplete | 650 | (10.5) | 94 | (15.8) | 155 | (17.4) |
| Ages of Health Counselors, Years | 20–29 | 30–39 | 40–49 | ≥50 | ||||
|---|---|---|---|---|---|---|---|---|
| Characteristics participants | ||||||||
| Number of participants | 1336 | 2385 | 2327 | 1643 | ||||
| Age, years, mean ± SD | 63.3 | ±8.2 | 63.6 | ±8.3 | 63.1 | ±8.5 | 63.1 | ±8.5 |
| Men, n (%) | 873 | (65.3) | 1563 | (65.5) | 1553 | (66.7) | 1077 | (65.6) |
| Grade II or higher hypertension, n (%) | 788 | (58.9) | 1391 | (58.3) | 1346 | (57.8) | 942 | (57.3) |
| Diabetes mellitus, n (%) | 239 | (17.9) | 450 | (18.9) | 457 | (19.7) | 314 | (19.1) |
| Dyslipidemia among men, (%) | 310 | (35.6) | 533 | (34.4) | 531 | (34.5) | 363 | (33.9) |
| Proteinuria, n (%) | 143 | (10.7) | 241 | (10.1) | 215 | (9.3) | 184 | (11.2) |
| Characteristics of counselors | ||||||||
| Women, n (%) | 1321 | (98.9) | 2335 | (97.9) | 2315 | (99.5) | 1632 | (99.3) |
| Profession | ||||||||
| Public health, n (%) | 1171 | (87.7) | 2021 | (84.7) | 1996 | (85.8) | 1031 | (62.8) |
| Clinical nurse, n (%) | 0 | (0.0) | 37 | (1.6) | 157 | (6.8) | 386 | (23.5) |
| Nutritionist, n (%) | 165 | (12.3) | 327 | (13.7) | 174 | (7.5) | 226 | (13.8) |
| Years of experience in general counseling, mean ± SD | 2.9 | ±2.1 | 7.5 | ±4.8 | 14.9 | ±9.0 | 18.9 | ±12.1 |
| <3, n (%) | 791 | (59.2) | 561 | (23.5) | 432 | (18.6) | 275 | (16.8) |
| 3–9, n (%) | 545 | (40.8) | 1055 | (44.2) | 310 | (13.3) | 244 | (14.9) |
| 10–19, n (%) | 0 | (0.0) | 769 | (32.2) | 695 | (29.9) | 297 | (18.1) |
| ≥20, n (%) | 0 | (0.0) | 0 | (0.0) | 890 | (38.3) | 825 | (50.3) |
| Years of experience for lifestyle-related disease counseling, mean ± SD | 2.1 | ±1.5 | 3.7 | ±3.2 | 4.9 | ±5.6 | 7.1 | ±7.8 |
| <3, n (%) | 981 | (73.7) | 1285 | (53.9) | 1092 | (47.0) | 674 | (41.0) |
| 3–5, n (%) | 326 | (24.5) | 647 | (27.1) | 652 | (28.0) | 266 | (16.2) |
| ≥6, n (%) | 25 | (1.9) | 453 | (19.0) | 582 | (25.0) | 703 | (42.8) |
| Counseling mode, n (%) | ||||||||
| Home visit | 641 | (48.0) | 1144 | (48.0) | 1411 | (60.6) | 988 | (60.1) |
| Face-to-face in a public place | 421 | (31.5) | 679 | (28.5) | 513 | (22.1) | 394 | (24.0) |
| Telephone | 78 | (5.8) | 133 | (5.6) | 90 | (3.9) | 72 | (4.4) |
| Incomplete | 196 | (14.7) | 429 | (18.0) | 313 | (13.5) | 189 | (11.5) |
| Initial timing, n (%) | ||||||||
| ≤45 days | 474 | (35.5) | 840 | (35.2) | 974 | (41.9) | 529 | (32.2) |
| 46–90 days | 416 | (31.1) | 672 | (28.2) | 542 | (23.3) | 420 | (25.6) |
| ≥91 days | 278 | (20.8) | 484 | (20.3) | 550 | (23.6) | 541 | (32.9) |
| Incomplete | 168 | (12.6) | 389 | (16.3) | 261 | (11.2) | 153 | (9.3) |
| Number of counseling sessions, n (%) | ||||||||
| 1 | 556 | (41.6) | 1024 | (42.9) | 979 | (42.1) | 583 | (35.5) |
| 2 | 323 | (24.2) | 603 | (25.3) | 714 | (30.7) | 534 | (32.5) |
| 3 | 289 | (21.6) | 404 | (16.9) | 400 | (17.2) | 386 | (23.5) |
| Incomplete | 168 | (12.6) | 354 | (14.8) | 234 | (10.1) | 140 | (8.5) |
| Years of Experience | <3 | 3–9 | 10–19 | ≥20 | ||||
|---|---|---|---|---|---|---|---|---|
| Characteristics of participants | ||||||||
| Number of participants | 2059 | 2154 | 1777 | 1715 | ||||
| Age, years, mean ± SD | 64.1 | ±8.1 | 63.3 | ±8.5 | 63.3 | ±8.2 | 62.4 | ±8.7 |
| Men, n (%) | 1331 | (64.6) | 1431 | (66.4) | 1167 | (65.7) | 1144 | (66.7) |
| Grade II or higher hypertension, n (%) | 1237 | (60.1) | 1225 | (56.9) | 1002 | (56.4) | 1012 | (59.0) |
| Diabetes mellitus, n (%) | 367 | (17.8) | 394 | (18.3) | 396 | (22.3) | 307 | (17.9) |
| Dyslipidemia among men, n (%) | 463 | (34.9) | 520 | (36.5) | 368 | (31.7) | 385 | (34.0) |
| Proteinuria, n (%) | 199 | (9.7) | 236 | (11.0) | 197 | (11.1) | 157 | (9.2) |
| Characteristics of counselors | ||||||||
| Women, n (%) | 2005 | (97.4) | 2154 | (100.0) | 1743 | (98.1) | 1715 | (100.0) |
| Profession | ||||||||
| Public health, n (%) | 1511 | (73.4) | 1629 | (75.6) | 1466 | (82.5) | 1611 | (93.9) |
| Clinical nurse, n (%) | 92 | (4.5) | 251 | (11.7) | 224 | (12.6) | 29 | (1.7) |
| Nutritionist, n (%) | 456 | (22.2) | 274 | (12.7) | 87 | (4.9) | 75 | (4.4) |
| Years of experience for lifestyle-related disease counseling, mean ± SD | 1.3 | ±0.8 | 4.5 | ±2.3 | 6.1 | ±5.0 | 6.9 | ±8.6 |
| <3, n (%) | 2050 | (99.8) | 559 | (26.0) | 674 | (38.0) | 747 | (43.6) |
| 3–5, n (%) | 5 | (0.2) | 1021 | (47.4) | 416 | (23.4) | 449 | (26.2) |
| ≥6, n (%) | 0 | (0.0) | 574 | (26.7) | 686 | (38.6) | 519 | (30.3) |
| Counseling mode, n (%) | ||||||||
| Home visit | 1045 | (50.8) | 1110 | (51.5) | 1019 | (57.3) | 1021 | (59.5) |
| Face-to-face in a public place | 510 | (24.8) | 539 | (25.0) | 468 | (26.3) | 490 | (28.6) |
| Telephone | 120 | (5.8) | 142 | (6.6) | 53 | (3.0) | 59 | (3.4) |
| Incomplete | 384 | (18.7) | 363 | (16.9) | 237 | (13.3) | 145 | (8.5) |
| Initial timing, n (%) | ||||||||
| ≤45 days | 620 | (30.1) | 609 | (28.3) | 724 | (40.7) | 865 | (50.4) |
| 46–90 days | 574 | (27.9) | 613 | (28.5) | 418 | (23.5) | 449 | (26.2) |
| ≥91 days | 538 | (26.1) | 602 | (28.0) | 427 | (24.0) | 293 | (17.1) |
| Incomplete | 327 | (15.9) | 330 | (15.3) | 208 | (11.7) | 108 | (6.3) |
| Number of counseling sessions, n (%) | ||||||||
| 1 | 829 | (40.3) | 991 | (46.0) | 638 | (35.9) | 689 | (40.2) |
| 2 | 554 | (26.9) | 554 | (25.7) | 561 | (31.6) | 512 | (29.9) |
| 3 | 352 | (17.1) | 317 | (14.7) | 393 | (22.1) | 417 | (24.3) |
| Incomplete | 324 | (15.7) | 292 | (13.6) | 185 | (10.4) | 97 | (5.7) |
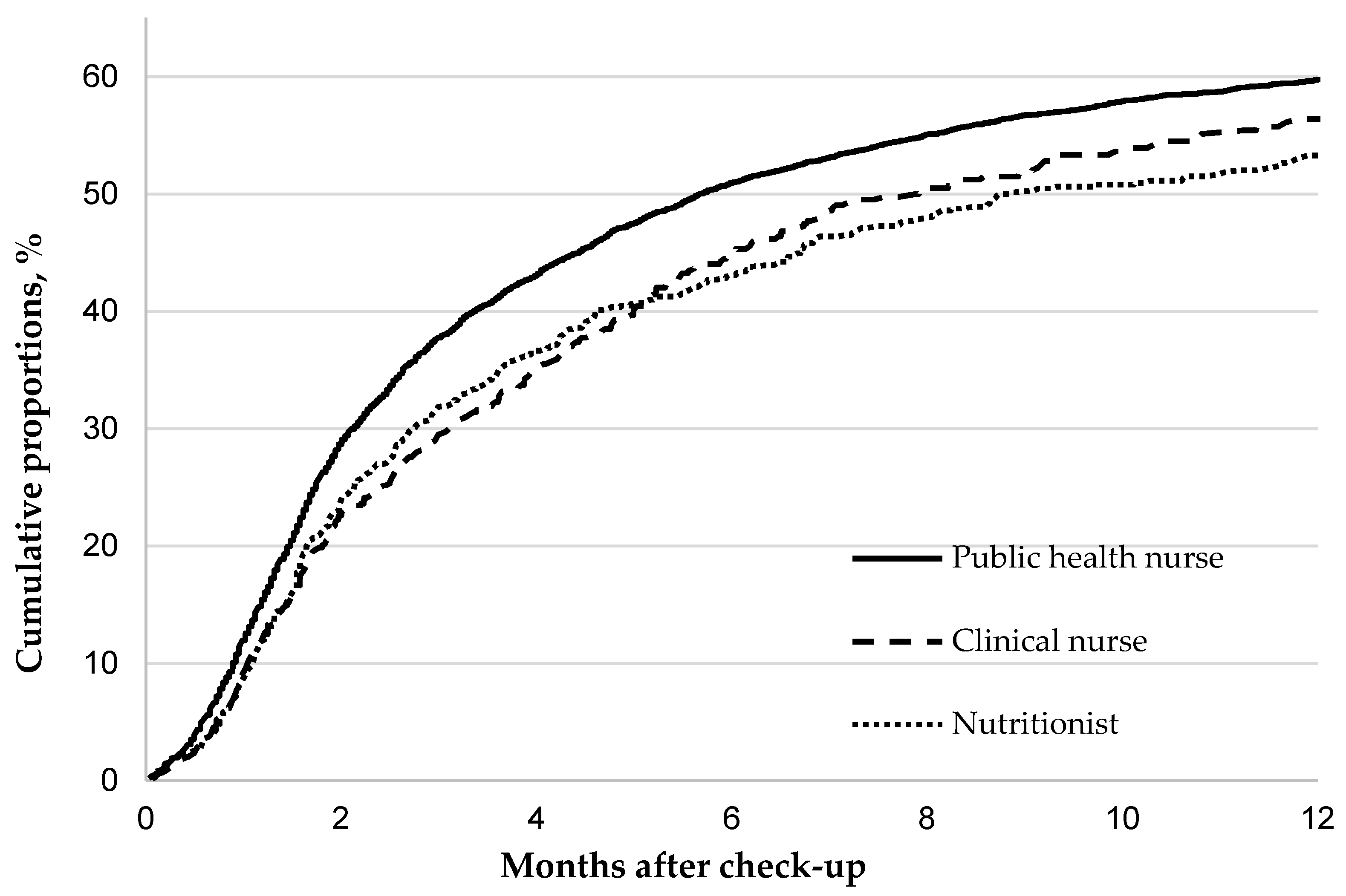
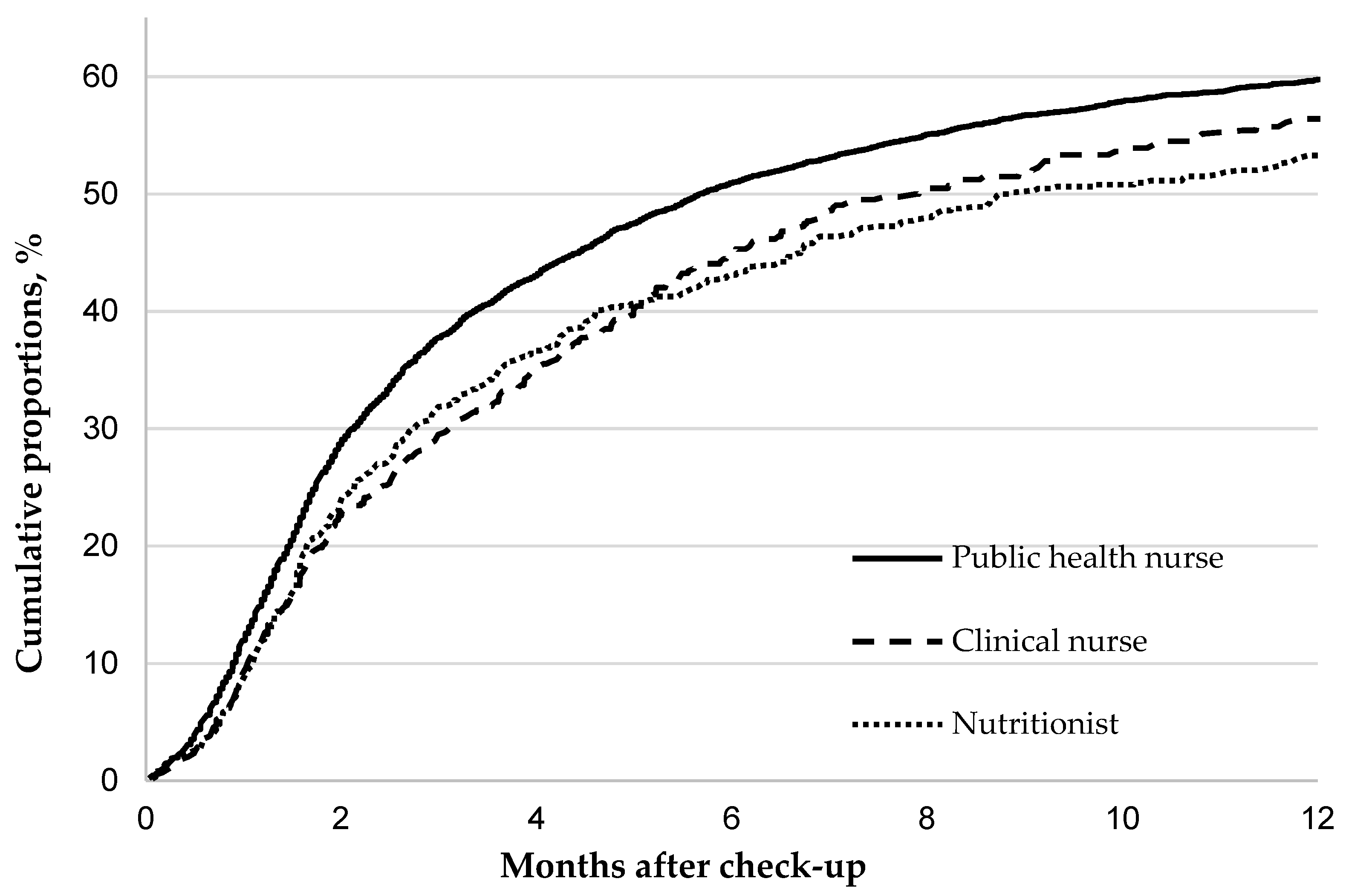
| Profession | Public Health Nurse | Clinical Nurse | Nutritionist | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| No. at risk | 6219 | 596 | 892 | ||||||
| No. of clinic visits | 3439 | 302 | 438 | ||||||
| Cumulative proportion of clinic visits (95% CI) | |||||||||
| 3 months | 37.8 | (36.6–39.0) | 29.5 | (26.0–33.4) | 31.9 | (28.9–35.0) | <0.001 | ||
| 6 months | 50.9 | (49.7–52.2) | 45.1 | (41.1–49.3) | 43.1 | (39.9–46.5) | <0.001 | ||
| 12 months | 59.8 | (58.4–61.1) | 56.4 | (52.0–60.9) | 53.3 | (49.8–56.9) | <0.001 | ||
| Probability ratio (95% Cl) | 1.22 | (1.11–1.35) | 1.04 | (0.90–1.20) | 1.00 | ||||
| Multivariable probability ratio (95% Cl) | |||||||||
| Model 1 a | 1.18 | (1.07–1.31) | 0.99 | (0.85–1.16) | 1.00 | ||||
| Model 2 b | 1.16 | (1.05–1.29) | 1.12 | (0.95–1.31) | 1.00 | ||||
| Ages of counselors | 20–29 | 30–39 | 40–49 | ≥50 | p-value | ||||
| No. at risk | 1336 | 2385 | 2327 | 1643 | |||||
| No. of clinic visits | 739 | 1230 | 1290 | 912 | |||||
| Cumulative proportion of clinic visits (95% CI) | |||||||||
| 3 months | 37.1 | (34.6–39.8) | 34.5 | (32.7–36.5) | 38.2 | (36.2–40.2) | 36.3 | (34.1–38.7) | 0.005 |
| 6 months | 49.8 | (47.1–52.6) | 47.5 | (45.5–49.6) | 50.9 | (48.9–53.0) | 50.6 | (48.1–53.1) | <0.001 |
| 12 months | 60.6 | (57.7–63.5) | 56.4 | (54.2–58.6) | 60.0 | (57.8–62.1) | 58.9 | (56.4–61.5) | <0.001 |
| Probability ratio (95% CI) | 1.00 | 0.91 | (0.83–1.00) | 1.01 | (0.92–1.11) | 0.97 | (0.88–1.07) | ||
| Multivariable probability ratio (95% Cl) | |||||||||
| Model 1 a | 1.00 | 0.87 | (0.79–0.96) | 0.89 | (0.80–0.99) | 0.86 | (0.76–0.98) | ||
| Model 2 b | 1.00 | 0.90 | (0.82–0.99) | 0.91 | (0.82–1.02) | 0.88 | (0.77–1.00) | ||
| Years of experience for general counseling | <3 | 3–9 | 10–19 | ≥20 | p-value | ||||
| No at risk | 2059 | 2154 | 1777 | 1715 | |||||
| No. of clinic visits | 1064 | 1106 | 1007 | 1002 | |||||
| Cumulative proportion of clinic visits (95% CI) | |||||||||
| 3 months | 33.2 | (31.2–35.3) | 33.9 | (31.9–35.9) | 38.3 | (36.0–40.6) | 41.6 | (39.3–44.0) | <0.001 |
| 6 months | 46.6 | (44.4–48.8) | 47.2 | (45.0–49.4) | 52.0 | (49.6–54.4) | 53.7 | (51.3–56.1) | <0.001 |
| 12 months | 57.0 | (54.6–59.4) | 56.0 | (53.8–58.4) | 60.9 | (58.4–63.3) | 62.1 | (59.6–64.6) | <0.001 |
| Probability ratio (95% CI) | 1.00 | 0.99 | (0.91–1.08) | 1.13 | (1.04–1.23) | 1.20 | (1.10–1.31) | ||
| Multivariable probability ratio (95% Cl) | |||||||||
| Model 1 a | 1.00 | 0.97 | (0.89–1.06) | 1.09 | (0.99–1.20) | 1.21 | (1.08–1.35) | ||
| Model 2 b | 1.00 | 0.97 | (0.89–1.06) | 1.02 | (0.92–1.12) | 1.07 | (0.96–1.21) | ||
| Years of experience for lifestyle-related disease counseling | <3 | 3–5 | ≥6 | p-value | |||||
| No. at risk | 4032 | 1891 | 1779 | ||||||
| No. of clinic visits | 2198 | 1020 | 958 | ||||||
| Cumulative proportion of clinic visits (95% CI) | |||||||||
| 3 months | 36.1 | (34.6–37.6) | 37.1 | (34.9–39.3) | 36.5 | (34.3–38.8) | 0.037 | ||
| 6 months | 49.4 | (47.9–51.0) | 49.5 | (47.2–51.8) | 50.0 | (47.6–52.4) | <0.001 | ||
| 12 months | 59.0 | (57.3–60.6) | 58.4 | (56.0–60.8) | 58.6 | (56.1–61.2) | <0.001 | ||
| Probability ratio (95% CI) | 1.00 | 1.00 | (0.93–1.08) | 0.99 | (0.92–1.07) | ||||
| Multivariable probability ratio (95% Cl) | |||||||||
| Model 1 a | 1.00 | 0.98 | (0.91–1.06) | 0.96 | (0.88–1.04) | ||||
| Model 2 b | 1.00 | 0.98 | (0.91–1.06) | 0.95 | (0.88–1.04) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noguchi, M.; Kinuta, M.; Sairenchi, T.; Yamakawa, M.; Koide, K.; Katsura, S.; Matsuo, K.; Omote, S.; Imano, H.; Nishizawa, H.; et al. Relationship between Health Counselor Characteristics and Counseling Impact on Individuals at High-Risk for Lifestyle-Related Disease: Sub-Analysis of the J-HARP Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 6375. https://doi.org/10.3390/ijerph19116375
Noguchi M, Kinuta M, Sairenchi T, Yamakawa M, Koide K, Katsura S, Matsuo K, Omote S, Imano H, Nishizawa H, et al. Relationship between Health Counselor Characteristics and Counseling Impact on Individuals at High-Risk for Lifestyle-Related Disease: Sub-Analysis of the J-HARP Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(11):6375. https://doi.org/10.3390/ijerph19116375
Chicago/Turabian StyleNoguchi, Midori, Minako Kinuta, Toshimi Sairenchi, Miyae Yamakawa, Keiko Koide, Shoko Katsura, Kazue Matsuo, Shizuko Omote, Hironori Imano, Hitoshi Nishizawa, and et al. 2022. "Relationship between Health Counselor Characteristics and Counseling Impact on Individuals at High-Risk for Lifestyle-Related Disease: Sub-Analysis of the J-HARP Cluster-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 11: 6375. https://doi.org/10.3390/ijerph19116375
APA StyleNoguchi, M., Kinuta, M., Sairenchi, T., Yamakawa, M., Koide, K., Katsura, S., Matsuo, K., Omote, S., Imano, H., Nishizawa, H., Shimomura, I., Iso, H., & On behalf of the J-HARP Research Group. (2022). Relationship between Health Counselor Characteristics and Counseling Impact on Individuals at High-Risk for Lifestyle-Related Disease: Sub-Analysis of the J-HARP Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(11), 6375. https://doi.org/10.3390/ijerph19116375