
Physical Rehabilitation Programs for Bedridden Patients with Prolonged Immobility: A Scoping Review

 ,
,  , , , , , , , , ,
, , , , , , , , ,  , and
, and
Abstract
:1. Introduction
- What are the physical rehabilitation programs for bedridden patients (e.g., neurological, orthopedic, and cardiorespiratory) with prolonged immobility?
- What is the context where the physical rehabilitation programs are implemented (e.g., institutions, community care, and outpatient)?
- What are the rehabilitation domains of the physical rehabilitation programs (motor, respiratory, and cardiorespiratory)?
- What kind of devices are used for bedridden patients with prolonged immobility (e.g., elastics, weights, crankset, and EMS)?
- What are the parameters assessed during the implementation of physical rehabilitation programs (e.g., muscle mass and oxygen saturation)?
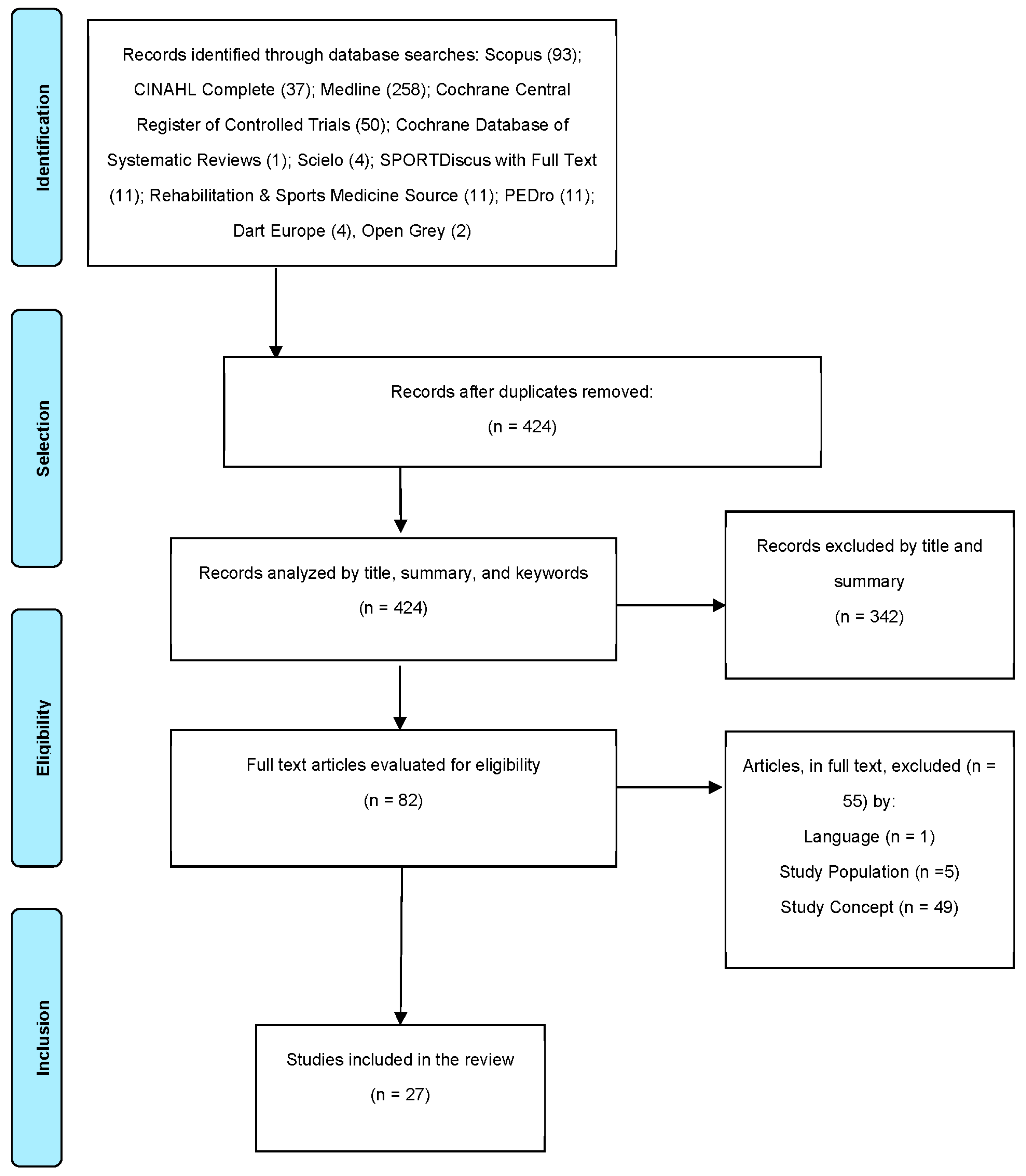
2. Materials and Methods
2.1. Search Strategy
2.2. Data Extraction
3. Results
3.1. Study Characteristics, Settings, and Sample
3.2. Context
3.3. Programs and Domains
3.4. Devices
3.5. Clinical Parameters
4. Discussion
4.1. Context
4.2. Domains
4.3. Devices
4.4. Parameters
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Pereira, F.; Carvalho, V.; Soares, F.; Machado, J.; Bezerra, K.; Silva, R.; Matos, D. Development of a mechatronic system for bedridden people support. In Advances in Engineering Research; Nova Science Publisher: Hauppauge, NY, USA, 2013; pp. 138–144. [Google Scholar]
- Andone, I.; Popescu, C.; Spinu, A.; Daia, C.; Stoica, S.; Onose, L.; Anghel, I.; Onose, G. Current aspects regarding “smart homes”/ambient assisted living (AAL) including rehabilitation specific devices, for people with disabilities/special needs. Balneo Res. J. 2020, 444–449. [Google Scholar] [CrossRef]
- Orun, B.; Roesler, C.; Martins, D. Review of Assistive Technologies for Bedridden Persons. ResearchGate. 2016. Available online: https://www.researchgate.net/profile/Bilal-Orun/publication/283459329_Review_of_assistive_technologies_for_bedridden_persons/links/5638bbda08ae78d01d39fa44/Review-of-assistive-technologies-for-bedridden-persons.pdf (accessed on 11 February 2022).
- Jiang, C.; Xiang, Z. A Novel Gait Training Device for Bedridden Patients’ Rehabilitation. J. Mech. Med. Biol. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Zongxing, L.; Xiangwen, W.; Shengxian, Y. The effect of sitting position changes from pedaling rehabilitation on muscle activity. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Wang, T.; Li, Z.; Liu, G.; Liu, Y.; Zhu, C.; Jiao, J.; Li, J.; Li, F.; Liu, H.; et al. Factors associated with death in bedridden patients in China: A longitudinal study. PLoS ONE 2020, 15, e0228423. [Google Scholar] [CrossRef] [PubMed]
- Salz, I.W.; Carmeli, Y.; Levin, A.; Fallach, N.; Braun, T.; Amit, S. Elderly bedridden patients with dementia use over one-quarter of resources in internal medicine wards in an Israeli hospital. Isr. J. Health Policy Res. 2020, 9, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wu, X.; Li, Z.; Zhou, X.; Cao, J.; Jia, Z.; Wan, X.; Jiao, J.; Liu, G.; Liu, Y.; et al. Nursing resources and major immobility complications among bedridden patients: A multicenter descriptive study in China. J. Nurs. Manag. 2019, 27, 930–938. [Google Scholar] [CrossRef]
- Campos, A.; Cortés, E.; Martins, D.; Ferre, M.; Contreras, A. Development of a flexible rehabilitation system for bedridden patients. J. Braz. Soc. Mech. Sci. Eng. 2021, 43, 361. [Google Scholar] [CrossRef]
- Guedes, L.P.C.M.; De Oliveira, M.L.C.; Carvalho, G.D.A. Deleterious effects of prolonged bed rest on the body systems of the elderly. Rev. Bras. Geriatr. Gerontol. 2018, 21, 499–506. [Google Scholar] [CrossRef]
- Marshall, R.N.; Smeuninx, B.; Morgan, P.T.; Breen, L. Nutritional Strategies to Offset Disuse-Induced Skeletal Muscle Atrophy and Anabolic Resistance in Older Adults: From Whole-Foods to Isolated Ingredients. Nutrition 2020, 12, 1533. [Google Scholar] [CrossRef]
- Arai, H.; Ikegawa, N.; Nozoe, M.; Kamiya, K.; Matsumoto, S. Association between Skeletal Muscle Mass Index and Convalescent Rehabilitation Ward Achievement Index in Older Patients. Prog. Rehabil. Med. 2022, 7, 20220003. [Google Scholar] [CrossRef]
- Wu, X.; Li, Z.; Cao, J.; Jiao, J.; Wang, Y.; Liu, G.; Liu, Y.; Li, F.; Song, B.; Jin, J.; et al. The association between major complications of immobility during hospitalization and quality of life among bedridden patients: A 3 month prospective multi-center study. PLoS ONE 2018, 13, e0205729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiao, J.; Li, Z.; Wu, X.; Cao, J.; Liu, G.; Liu, Y.; Li, F.; Zhu, C.; Song, B.; Jin, J.; et al. Risk factors for 3-month mortality in bedridden patients with hospital-acquired pneumonia: A multicentre prospective study. PLoS ONE 2021, 16, e0249198. [Google Scholar] [CrossRef] [PubMed]
- Tousignant-Laflamme, Y.; Beaudoin, A.-M.; Renaud, A.-M.; Lauzon, S.; Charest-Bossé, M.-C.; Leblanc, L.; Grégoire, M. Adding physical therapy services in the emergency department to prevent immobilization syndrome—A feasibility study in a university hospital. BMC Emerg. Med. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, R.; Watanabe, H.; Tsutsumi, M.; Kanamori, T.; Maeno, T.; Yanagi, H. Factors associated with the recovery of activities of daily living after hospitalization for acute medical illness: A prospective cohort study. J. Phys. Ther. Sci. 2016, 28, 2763–2768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha, A.M.; Martinez, B.; da Silva, V.M.; Junior, L.F. Early mobilization: Why, what for and how? Med. Intensiv. 2017, 41, 429–436. [Google Scholar] [CrossRef] [PubMed]
- McGlinchey, M.P.; James, J.; McKevitt, C.; Douiri, A.; Sackley, C. The effect of rehabilitation interventions on physical function and immobility-related complications in severe stroke: A systematic review. BMJ Open 2020, 10, e033642. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-León, J.F.; Chaparro-Rico, B.D.M.; Russo, M.; Cafolla, D. An Autotuning Cable-Driven Device for Home Rehabilitation. J. Healthc. Eng. 2021, 2021, 6680762. [Google Scholar] [CrossRef]
- Gilmore, B.; MacLachlan, M.; McVeigh, J.; McClean, C.; Carr, S.; Duttine, A.; Mannan, H.; McAuliffe, E.; Mji, G.; Eide, A.H.; et al. A study of human resource competencies required to implement community rehabilitation in less resourced settings. Hum. Resour. Health 2017, 15, 70. [Google Scholar] [CrossRef] [Green Version]
- Dunaj, J.; Klimasara, W.J.; Pilat, Z.; Rycerski, W. Human-Robot Communication in Rehabilitation Devices. J. Autom. Mob. Robot. Intell. Syst. 2015, 9, 9–19. [Google Scholar] [CrossRef]
- Gonzalez, A.; Garcia, L.; Kilby, J.; McNair, P. Robotic devices for pediatric rehabilitation: A review of design features. Biomed. Eng. Online 2021, 20, 1–33. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; Mcinerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Khalil, H.; Peters, M.; Godfrey, C.M.; McInerney, P.; Soares, C.B.; Parker, D. An Evidence-Based Approach to Scoping Reviews. Worldviews Evid.-Based Nurs. 2016, 13, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Évid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parola, V.; Neves, H.; Duque, F.M.; Bernardes, R.A.; Cardoso, R.; Mendes, C.A.; Sousa, L.B.; Santos-Costa, P.; Malça, C.; Durães, R.; et al. Rehabilitation Programs for Bedridden Patients with Prolonged Immobility: A Scoping Review Protocol. Int. J. Environ. Res. Public Health 2021, 18, 12033. [Google Scholar] [CrossRef] [PubMed]
- Alkner, B.A.; Tesch, P.A. Efficacy of a gravity-independent resistance exercise device as a countermeasure to muscle atrophy during 29-day bed rest. Acta Physiol. Scand. 2004, 181, 345–357. [Google Scholar] [CrossRef]
- Benjamin, B.S. Regulating artificial gravity forces in space exploration. In Proceedings of the 47th AIAA Aerospace Sciences Meeting including the New Horizons Forum and Aerospace Exposition, Orlando, FL, USA, 5–8 January 2009; American Institute of Aeronautics and Astronautics Inc.: Reston, VA, USA; School of Architecture, Marvin Hall, University of Kansas: Lawrence, KS, USA, 2009. [Google Scholar]
- Blanc-Bisson, C.; Dechamps, A.; Gouspillou, G.; Dehail, P.; Bourdel-Marchasson, I. A randomized controlled trial on early physiotherapy intervention versus usual care in acute car unit for elderly: Potential benefits in light of dietary intakes. J. Nutr. Health Aging 2008, 12, 395–399. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Leo, A.; Balletta, T.; Saccá, I.; De Luca, R.; Bramanti, P.; RS, C.; Naro, A.; et al. Do post-stroke patients benefit from robotic verticalization? A pilot-study focusing on a novel neurophysiological approach. Restor. Neurol. Neurosci. 2015, 33, 671–681. [Google Scholar] [CrossRef] [Green Version]
- English, K.L.; Loehr, J.A.; Lee, S.M.C.; Smith, S.M. Early-phase musculoskeletal adaptations to different levels of eccentric resistance after 8 weeks of lower body training. Eur. J. Appl. Physiol. 2014, 114, 2263–2280. [Google Scholar] [CrossRef]
- Golčić, M.; Dobrila-Dintinjana, R.; Golčić, G.; Gović-Golčić, L.; Čubranić, A. Physical Exercise: An Evaluation of a New Clinical Biomarker of Survival in Hospice Patients. Am. J. Hosp. Palliat. Med. 2018, 35, 1377–1383. [Google Scholar] [CrossRef]
- Ino, S.; Hosono, M.; Sato, M.; Nakajima, S.; Yamashita, K.; Izumi, T. A Preliminary Study of a Power Assist System for Toe Exercise Using a Metal Hydride Actuator; Springer: Tsukuba, Japan, 2009; Volume 25, pp. 287–290. [Google Scholar]
- Maimaiti, P.; Sen, L.F.; Aisilahong, G.; Maimaiti, R.; Yun, W.Y. Retracted: Statistical analysis with Kruskal Wallis test for patients with joint contracture. Futur. Gener. Comput. Syst. 2019, 92, 419–423. [Google Scholar] [CrossRef]
- Pittaccio, S.; Garavaglia, L.; Molteni, E.; Guanziroli, E.; Zappasodi, F.; Beretta, E.; Strazzer, S.; Molteni, F.; Villa, E.; Passaretti, F. Can passive mobilization provide clinically-relevant brain stimulation? A pilot EEG and NIRS study on healthy subjects. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. IEEE Eng. Med. Biol. Soc. Annu. Int. Conf. 2013, 2013, 3547–3550. [Google Scholar] [CrossRef]
- Shimizu, Y.; Kamada, H.; Sakane, M.; Aikawa, S.; Mutsuzaki, H.; Tanaka, K.; Mishima, H.; Kanamori, A.; Nishino, T.; Ochiai, N.; et al. A novel exercise device for venous thromboembolism prophylaxis improves venous flow in bed versus ankle movement exercises in healthy volunteers. J. Orthop. Surg. 2017, 25, 2309499017739477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talar, J. Rehabilitation outcome in a patient awakened from prolonged coma. Med. Sci. Monit. 2002, 8, CS31–CS38. [Google Scholar] [PubMed]
- Tseng, C.-N.; Chen, C.-H.; Wu, S.-C.; Lin, L.-C. Effects of a range-of-motion exercise programme. J. Adv. Nurs. 2007, 57, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Vinstrup, J.; Skals, S.; Calatayud, J.; Jakobsen, M.D.; Sundstrup, E.; Pinto, M.D.; Izquierdo, M.; Wang, Y.; Zebis, M.K.; Andersen, L.L. Electromyographic evaluation of high-intensity elastic resistance exercises for lower extremity muscles during bed rest. Eur. J. Appl. Physiol. Occup. Physiol. 2017, 178, 261–1338. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, H.; Nakashima, S.; Aoki, H.; Goto, K.; Yamashita, J.; Honda, Y.; Kondo, Y.; Hirase, T.; Sakamoto, J.; Okita, M. Electrical Stimulation in Addition to Passive Exercise Has a Small Effect on Spasticity and Range of Motion in Bedridden Elderly Patients: A Pilot Randomized Crossover Study. Health 2019, 11, 1072–1086. [Google Scholar] [CrossRef] [Green Version]
- Akar, O.; Günay, E.; Sarinc Ulasli, S.; Ulasli, A.M.; Kacar, E.; Sariaydin, M.; Solak, Ö.; Celik, S.; Ünlü, M. Efficacy of neuromuscular electrical stimulation in patients with COPD followed in intensive care unit. Clin. Respir. J. 2017, 11, 743–750. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Lin, H.-L.; Hsiao, H.-F.; Chou, L.-T.; Kao, K.-C.; Huang, C.-C.; Tsai, Y.-H. Effects of Exercise Training on Pulmonary Mechanics and Functional Status in Patients with Prolonged Mechanical Ventilation. Respir. Care 2012, 57, 727–734. [Google Scholar] [CrossRef] [Green Version]
- Gosselink, R.; Kovacs, L.; Ketelaer, P.; Carton, H.; Decramer, M. Respiratory muscle weakness and respiratory muscle training in severely disabled multiple sclerosis patients. Arch. Phys. Med. Rehabil. 2000, 81, 747–751. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.; Gao, C.; Xin, H.; Li, J.; Li, B.; Wei, Z.; Yue, Y. The application of “upper-body yoga” in elderly patients with acute hip fracture: A prospective, randomized, and single-blind study. J. Orthop. Surg. Res. 2019, 14, 250. [Google Scholar] [CrossRef]
- Tafreshi, A.S.; Okle, J.; Klamroth-Marganska, V.; Riener, R. Modeling the effect of tilting, passive leg exercise, and functional electrical stimulation on the human cardiovascular system. Med. Biol. Eng. Comput. 2017, 55, 1693–1708. [Google Scholar] [CrossRef] [PubMed]
- Friedl-Werner, A.; Brauns, K.; Gunga, H.-C.; Kühn, S.; Stahn, A.C. Exercise-induced changes in brain activity during memory encoding and retrieval after long-term bed rest. NeuroImage 2020, 223, 117359. [Google Scholar] [CrossRef] [PubMed]
- Medrinal, C.; Combret, Y.; Prieur, G.; Quesada, A.R.; Bonnevie, T.; Gravier, F.E.; Frenoy, É.; Contal, O.; Lamia, B. Effects of different early rehabilitation techniques on haemodynamic and metabolic parameters in sedated patients: Protocol for a randomised, single-bind, cross-over trial. BMJ Open Respir. Res. 2017, 4, e000173. [Google Scholar] [CrossRef]
- Boccignone, A.; Abelli, S.; Ortolani, L.; Ortolani, M. Functional outcomes following the rehabilitation of hospitalized patients with immobilization syndromes. Eura. Medicophys. 1999, 35, 185–193. [Google Scholar]
- Hirakawa, Y.; Masuda, Y.; Kimata, T.; Uemura, K.; Kuzuya, M.; Iguchi, A. Effects of home massage rehabilitation therapy for the bed-ridden elderly: A pilot trial with a three-month follow-up. Clin. Rehabil. 2005, 19, 20–27. [Google Scholar] [CrossRef]
- Leite, M.A.; Osaku, E.F.; Albert, J.; Costa, C.R.L.D.M.; Garcia, A.M.; Czapiesvski, F.D.N.; Ogasawara, S.M.; Bertolini, G.R.F.; Jorge, A.C.; Duarte, P.A.D. Effects of Neuromuscular Electrical Stimulation of the Quadriceps and Diaphragm in Critically Ill Patients: A Pilot Study. Crit. Care Res. Pract. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- Mendt, S.; Gunga, H.-C.; Felsenberg, D.; Belavy, D.L.; Steinach, M.; Stahn, A.C. Regular exercise counteracts circadian shifts in core body temperature during long-duration bed rest. Npj Microgravity 2021, 7, 1–6. [Google Scholar] [CrossRef]
- Tatsumi, M.; Kumagai, S.; Abe, T.; Murakami, S.; Takeda, H.; Shichinohe, T.; Watanabe, Y.; Katayama, S.; Hirai, S.; Honda, A.; et al. Sarcopenia in a patient with most serious complications after highly invasive surgeries treated with nutrition, rehabilitation, and pharmacotherapy: A case report. J. Pharm. Health Care Sci. 2021, 7, 1–7. [Google Scholar] [CrossRef]
- Bouman, A.I.E.; Hemmen, B.; Evers, S.M.A.A.; Van De Meent, H.; Ambergen, T.; Vos, P.E.; Brink, P.R.G.; Seelen, H.A.M. Effects of an Integrated ‘Fast Track’ Rehabilitation Service for Multi-Trauma Patients: A Non-Randomized Clinical Trial in the Netherlands. PLoS ONE 2017, 12, e0170047. [Google Scholar] [CrossRef]
- Dresser, R. First-in-Human Trial Participants: Not a Vulnerable Population, but Vulnerable Nonetheless. J. Law Med. Ethic 2009, 37, 38–50. [Google Scholar] [CrossRef] [Green Version]
- Karakunnel, J.J.; Bui, N.; Palaniappan, L.; Schmidt, K.T.; Mahaffey, K.W.; Morrison, B.; Figg, W.D.; Kummar, S. Reviewing the role of healthy volunteer studies in drug development. J. Transl. Med. 2018, 16, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiq, M.A.B.; Rathore, F.A.; Clegg, D.; Rasker, J.J. Pulmonary Rehabilitation in COVID-19 patients: A scoping review of current practice and its application during the pandemic. Turk. J. Phys. Med. Rehabil. 2021, 66, 480–494. [Google Scholar] [CrossRef] [PubMed]
- Stam, H.J.; Stucki, G.; Bickenbach, J. COVID-19 and Post Intensive Care Syndrome: A Call for Action. J. Rehabil. Med. 2020, 52, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Gagin, R.; Hagani, N.; Levy, I.; Norman, D. There Is No Place Like Home: A Survey on Satisfaction and Reported Outcomes of a Home-Based Rehabilitation Program Among Orthopedic Surgery Patients. J. Patient Exp. 2019, 7, 1715–1723. [Google Scholar] [CrossRef]
- Palazzo, C.; Klinger, E.; Dorner, V.; Kadri, A.; Thierry, O.; Boumenir, Y.; Martin, W.; Poiraudeau, S.; Ville, I. Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies. Ann. Phys. Rehabil. Med. 2016, 59, 107–113. [Google Scholar] [CrossRef]
- Van Der Veen, D.J.; Döpp, C.M.E.; Siemonsma, P.C.; Der Sanden, M.W.G.N.-V.; De Swart, B.J.M.; Steultjens, E.M. Factors Influencing the Implementation of Home-Based Stroke Rehabilitation: Professionals’ Perspective. PLoS ONE 2019, 14, e0220226. [Google Scholar] [CrossRef]
- Kim, C.S.; Gong, W.; Kim, S.G. The Effects of Lower Extremitiy Muscle Strengthening Exercise and Treadmill Walking Exercise on the Gait and Balance of Stroke Patients. J. Phys. Ther. Sci. 2011, 23, 405–408. [Google Scholar] [CrossRef] [Green Version]
- Muscedere, J.; Sinuff, T.; Heyland, D.K.; Dodek, P.M.; Keenan, S.P.; Wood, G.; Jiang, X.; Day, A.G.; Laporta, D.; Klompas, M.; et al. The Clinical Impact and Preventability of Ventilator-Associated Conditions in Critically Ill Patients Who Are Mechanically Ventilated. Chest 2013, 144, 1453–1460. [Google Scholar] [CrossRef]
- Bernardes, R.A.; Santos-Costa, P.; Sousa, L.B.; Graveto, J.; Salgueiro-Oliveira, A.; Serambeque, B.; Marques, I.; Cruz, A.; Parreira, P. Innovative devices for bedridden older adults upper and lower limb rehabilitation: Key characteristics and features. Int. Workshop Gerontechnol. 2020, 1185 CCIS, 25–35. [Google Scholar]
- Peters, M.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.; Khalil, H. Chapter 3: Systematic Reviews of Effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Chapter 12—Regional Complications in Joint Hypermobility Syndrome. In Grahame Fibromyalgia and Chronic Pain; Hakim, A.J.; Keer, R. (Eds.) Churchill Livingstone: Edinburgh, UK, 2010; pp. 197–280. ISBN 978-0-7020-3005-5. [Google Scholar]


{kind=link}
| Medline (via PubMed)—searched on 8th July 2021: 258 results ((((rehabilitation [MeSH Terms]) OR (rehabilitation [Title/Abstract])) OR (((((exercise*[Title/Abstract]) OR (Exercise Movement Techniques[MeSH Terms])) OR (Rehabilitation Exercise[MeSH Terms])) OR (Exercise[MeSH Terms])) AND ((bedridden[Title/Abstract]) OR (bedridden persons[MeSH Terms])) Filters: English, Portuguese, Spanish, MEDLINE |
| CINAHL Complete—searched on 8th July 2021: 37 results (TI rehab* OR AB rehab* OR TI exercise* OR AB exercise* OR ((TI physical OR AB physical) N1 (TI activit* OR AB activit*)) OR (MH “Therapeutic Exercise”) OR (MH “Physical Activity”) OR (MH “Exercise”) OR (MH “Rehabilitation”)) AND (TI bedridden OR AB bedridden OR (MH “Bedridden Persons”)) Limiters—Exclude MEDLINE records; Language: English, Portuguese, Spanish |
| Cochrane Central Register of Controlled Trials—searched on 8th July 2021: 50 results (TI rehab* OR AB rehab* OR TI exercise* OR AB exercise* OR ((TI physical OR AB physical) N1 (TI activit* OR AB activit*))) AND (TI bedridden OR AB bedridden) |
| Cochrane Database of Systematic Reviews—searched on 8th July 2021: 1 result (TI rehab* OR AB rehab* OR TI exercise* OR AB exercise* OR ((TI physical OR AB physical) N1 (TI activit* OR AB activit*))) AND (TI bedridden OR AB bedridden) Scopus—searched on 8th July 2021: 93 results ((TITLE-ABS (rehabilitation) OR TITLE-ABS (exercise*)) AND (TITLE-ABS (bedridden))) AND NOT ((PMID (1*) OR PMID (2*) OR PMID (3*) OR PMID (4*) OR PMID (5*) OR PMID (6*) OR PMID (7*) OR PMID (8*) OR PMID (9*))) AND (LIMIT-TO (LANGUAGE, “English”) OR LIMIT-TO (LANGUAGE, “Portuguese”) OR LIMIT-TO (LANGUAGE, “Spanish”)) |
| Scielo—searched on 8th July 2021: 4 results (ti:(rehabilitation OR exercise*)) OR (ab:(rehabilitation OR exercise*)) AND (ti:(bedridden)) OR (ab:(bedridden)) |
| SPORTDiscus with Full Text—searched on 8th July 2021: 11 results (ti:(rehabilitation OR exercise)) OR (ab:(rehabilitation OR exercise)) AND (ti:(bedridden)) OR (ab:(bedridden)) Filters: English, Portuguese, Spanish |
| Rehabilitation & Sports Medicine Source- searched on 8th July 2021: 11 results (ti:(rehabilitation OR exercise)) OR (ab:(rehabilitation OR exercise)) AND (ti:(bedridden)) OR (ab:(bedridden)) Filters: English, Portuguese, Spanish |
| DART-Europe—searched on 27th November 2019: 4 results (rehabilitation OR exercise*) AND bedridden Filters: English; Portuguese; Spanish; |
| Open Grey- searched on 8th July 2021: 2 Results bedridden |
| PEDro—Physiotherapy Evidence Database—searched on 8th July 2021: 11 Results bedridden exercise* = 10 OR bedridden activit* = 5 Filters: English; Portuguese; Spanish |
| Author, Year, Country | Population | Physical Rehabilitation Programs | Parameters | Context | Devices |
|---|---|---|---|---|---|
| Musculoskeletal Domain (n = 15) | |||||
| Alkner et al. [28] 2004, Sweden | Seventeen healthy subjects (26–41 years). Study subjects were divided into two groups: with (8) or without (9) resistance exercise | The training was performed in the 6° head-down tilt position. Study subjects performed four sets of 7 repetitions of supine squat and 14 repetitions of calf press every third day using a gravity-independent flywheel ergometer for 29 days; 2 min of rest was allowed between sets and 5 min between exercises | Quadriceps and triceps muscle volume using MRI (before and after bed rest). EMG, Peak force, power, work velocity, and minimum joint angle (for each repetition) | Research institute | Gravity-independent flywheel ergometer, |
| Benjamin et al. [29] 2009, USA | One healthy man (69 years) | The study subject used a newly designed bodysuit that applied precise loads to specific body parts | Artificial gravity force | Research institute | Bodysuit |
| Blanc-Bisson et al. [30] 2008, France | Seventy-six acute bedridden patients or with reduced mobility. (55F; 21M), 85.4 ± 6.6 years. Patients were divided into two groups: usual care and early physiotherapy program | Besides usual care, patients started on day 1 to 2: 10 repetitions of dynamic work against the foot of the bed (for triceps). When the subject was able to stand, exercises of plantar flexors and extensors were performed in the upright position. Extended leg, hip flexion at 45°/s alternatively for each leg; each repetition was maintained for 3 to 5 s, 10 repetitions with 10 s rest period between each (both legs). Knee flexed at 30°, moving pelvis to the left and the right, 10 repetitions (For the pelvis). | History of weight loss, weight, BMI, calf and arm circumference, triceps skinfold, day dietary records, serum albumin, and CRP. Katz index, handgrip strength, and change in ADL autonomy | Hospital (Acute-care geriatric medicine unit.) | Unspecified |
| Calabro et al. [31] 2015, Italy | Twenty bedridden patients due to ischemic stroke; 10 patients were randomly allocated in (G1) and 10 patients control group (G2) | Each G1—patient underwent 30 sessions of robotic verticalization procedures using the robotic tilt-table ERIGO. During the first 3 training sessions, patients were gradually verticalized from 10 to 30° over 15 min at a rate of 3° in 5 s. By session 5, verticalization was increased to 60° and reached 90° by session 10. During verticalization, each patient received a functional electrical stimulation treatment (30 mA of intensity). In G2, physiotherapy-assisted verticalization was performed through a simple tilt-table, with similar verticalization procedures to the G1. | The measure of the mean BP, HR, and SpO2. Lower limb’s paresis using the MRC scale, Patient’s postural control using the Postural Assessment Scale for Stroke patients | Rehabilitation clinic (neurorehabilitation) | ERIGO (Hocoma AG, Volketswil, Switzerland) Six-channel stimulator (Motionstim-8, Medel GmbH, Hamburg, Germany) |
| English et al. [32], 2014, USA | Forty healthy subjects (males) 34.9 ± 7 years. Study subjects were divided into six groups (8 per group according to concentric load) | Exercise testing and training were conducted using supine leg press and supine calf press exercise; Intensity (eccentric): 0% (concentric-only training), 33, 66, 100, or 138% of the concentric load. The program was performed 3 days per week over 12 weeks: 3 weeks of pre-testing, 8 weeks of training, and 1 week of post-testing, | Pre- and post-training whole body, lumbar spine, and hip bone mineral density. Whole-body lean tissue mass. Urine and blood markers of bone metabolism. | Research institute | Agaton Fitness System (Agaton Fitness AB, Boden, Sweden) |
| Golčić et al. [33] 2018, Croatia | Five hundred and thirty-six palliative patients with a life expectancy of fewer than 3 months (mainly cancer diagnosis), 71.77 ± 11.13 years. An approximate number of females (50.56%) and males. | The program consisted of active, actively assisted, and passive positioning exercises. Active exercises included the ability to move at least one of the arms or the legs against gravity. The exercises were considered actively assisted if the patients could start and perform the motion but were unable to complete the normal range of motion. Passive exercises consisted of stretching (5 to 10 repetitions) and performing ROM in at least all large joints of the extremities. | Manual-muscle test and performance score. | Hospice | Unspecified |
| Ino et al. [34] 2009, Japan | Ten healthy subjects (20 to 80 years) | Subjects’ toe joints were subjected to bending and stretching motions for 2 min, keeping the subjects in a supine position for 5 to 10 min | Lower limb blood flow | Research institute | Device for passive mobilization of toe joints |
| Maimati et al. [35] 2019, China | Eighty bedridden patients with disuse syndrome (50M; 30F), 69.25 ± 7.80 years were divided into experimental (40) and a control group (40) | Comprehensive rehabilitation nursing intervention was employed as follows: once a day, 50 min, 5 times a week and consisted of: Uyghur medicine; hand micro-vibration therapy, and training combined with education through a 20 min video once per week. | ROM of the hip joint, knee joint, and ankle joint. | Welfare home | Unspecified |
| Pittaccio et al. [36] 2013, Italy | Four healthy subjects (2 male; 2 female) | This program consisted of rest, active, passive, and assisted conditions for 5 min. Rest: the subject laid with the leg positioned on the leg rest of the mobilizer. Active: the subject performed a voluntary movement of the ankle, alternating 7 s of dorsiflexion hold to 30 s of relaxation. Passive and assisted conditions were performed with the Toe-Up! The device was set to produce cycles of 30° dorsiflexion (7 s) and relaxation towards plantar flexion in 30 s. In the passive condition: Toe-Up performed a continuous passive motion (CPM) to the subject’s ankle, whereas in the assisted condition, the subject was instructed to follow the CPM, collaborating actively in the dorsiflexion promoted by the device | Brain activity (EEG and NIRS in 4 different conditions: rest, active dorsiflexion of the ankle, passive mobilization of the ankle, and assisted motion of the same joint | Research institute | Toe-Up! An electro-mechanical mobilizer for the ankle joint |
| Shimizu et al. [37] 2017, Japan | Eight healthy subjects (5M; 3F); 21.6 ± 2.3 years, (19–25 years), Patients had no history (or risk factors) for deep vein thrombosis or lower limb operation | The participants performed 1-min leg exercise apparatus (LEX) exercises in three modes: (1) rapid single ankle motion (maximum active ankle dorsiflexion/plantarflexion at a rate of 60 cycles/min); (2) slow single ankle motion (maximum active ankle dorsiflexion/plantarflexion at a rate of 30 cycles/min); and (3) slow combined leg motion (active ankle dorsiflexion/plantarflexion and subtalar eversion/inversion at a rate of 30 cycles/min, with natural knee extension/flexion, hip/extension, and hip internal/external rotation). | Venous flow volume and velocity in the femoral vein at 1, 10, 20, and 30 min postexercise. These measurements were repeated three times for each participant, | Research institute | The LEX is a portable apparatus that enables patients to move their legs while supine. |
| Talar et al. [38] 2002, Poland | Twenty-eight-year-old male bedridden who suffered severe closed head injuries in an automobile accident and was in a comatose state for more than two months (GCS score of 5). | Physiotherapy was started with the patient still in comatose as follows: hydrotherapy, physical stimulation, including interference current (0.10 and 0.100 amps for 10 min, 6 times daily), low-power magnetic stimulation (15 min, 6 times daily), scanning laser (trunk and limbs, power 2J, 10 min, 6 times daily); manual massage of the trunk and limbs (30 min, 4–5 times per week). Kinesitherapy was initiated to restore locomotion after the patient awakened from the coma. | Clinical observation and family interviews. Wechsler Adult Intelligence, Vignos and Archibald scale. Rivermead Behavioural Memory, and FIM tests. Western Aphasia Battery; Frontal Behaviour Inventory and Boston Test of Praxis, | Rehabilitation clinic | Unspecified |
| Tseng et al. [39] 2007, Twain | Fifty-nine bedridden older stroke survivors: 17 in the usual care group, 21 in intervention group I, and 21 in intervention group II | Intervention group 1 involved a nurse supervising participants performing and completing the ROM protocol by themselves. Participants in intervention group 2 carried out the same ROM protocol with the nurse’s presence to help them physically achieve maximum ROM within or beyond their present ability; both intervention groups completed the ROM exercise protocol. This protocol was performed five times per joint, twice per day, and 6 days per week for 4 weeks, with each session lasting approximately 10–20 min. | 17 joint angle measures in six joints (shoulder; elbow; wrist; hip; knee; dorsal ankle and plantar) and self-perception of pain using three ratings. | Long-term care facilities | Unspecified |
| Vinstrup et al. [40] 2017, Denmark | Twenty-two healthy subjects (15M/7F), 34.2 ± 14.7 years, | Elastic bands with a very low to very high resistance were attached to a standard-issued hospital bed. Total of 14 exercises: femoris muscle setting, prone knee extension, hip flexion with the leg bent, hip flexion with the leg straight, hip adduction, sideways hip abduction, prone hip abduction, supine knee flexion, hip thrust, dorsal flexion, plantar flexion, hip extension with the leg bent, and prone knee flexion performed with and without TheraBand Kinesiology Tape. The training session of 2.5 h and consisted of 3 repetitions of each exercise with 2 min of rest between exercises | Electromyographic signals were recorded from 13 lower extremity muscles. Borg CR-10 scale | Research Centre | Elastic bands (TheraBand CLX Consecutive Loops, TheraBand, Akron, OH, USA) |
| Kataoka et al. [41] 2017, Japan | Thirty bedridden disabled elderly patients | In addition to rehabilitation, the intervention mainly consisted of ROMex and sitting or standing; Belt electrode skeletal muscle electrical stimulation (B-SES) was applied on bilateral lower limbs 3 times per week for 3 months. | ROM of lower limbs at baseline and 1, 2, and 3 months after starting treatment, Muscle tone and pain | Hospital | B-SES |
| Cardiorespiratory domain (n = 8) | |||||
| Akar et al. [42] 2017, Turkey | Thirty COPD patients (15M) treated with Invasive mechanical ventilation were divided (blinded) into 3 groups (10 each): (1) active extremity exercise and NMES (2) NMES alone; and (3) active extremity ‘exercise alone | NMES was performed transcutaneously on the deltoid and quadriceps muscles using a four-channel neuromuscular electrical stimulator. The amplitude was switched between 20 mA and 25 mA (according to each patient). Symmetrical biphasic square waves with 6 s duration of contraction, 1.5 s of increase, and 0.75 s of decrease were applied. The wave frequency was 50 Hz. Patients were given a pulmonary rehabilitation program 5 days per week for 20 sessions. | Lower extremity and upper extremity muscle strength (scale of 5), mobilization duration, and weaning situation. Serum CRP, IL-6, IL-8, IL-10 and TNF-a, HR, RR. | Hospital (ICU) | Four-channel portable neuromuscular electrical stimulator, COMPEX device (MI Theta PRO, Switzerland) |
| Chen et al. [43] 2012, Twain | Twenty-seven prolonged mechanical ventilation patients | The cardiopulmonary exercise was performed on a cycle ergometer with a training intensity targeted at 60–80% of age-predicted maximal intermittent and short-term periods. Muscle-strengthening exercises included respiratory muscle and arm muscle strengthening exercises. Stretching exercises consisted of cervical, upper limb, and upper chest stretching. Respiratory muscle training was performed by putting a weight (0.5–2 kg sandbag) on the subject’s abdomen while he or she lay on the bed. The train lasted 30–40 min/session, 4–6 sessions/week for 10 sessions. | Vital signs and electrocardiogram. Physical functional status, pulmonary mechanics, ADL, BI, tidal volume, minute volume, respiratory muscle strength (maximal inspiratory pressure), and RR | Hospital | Ergometer (APT-5, Tzora, Kibbutz Tzora, Israel) |
| Gosselink et al. [44] 2000, Belgium | Twenty-eight bedridden (11) or wheelchair-bound (17) MS patients (13M) 58 ± 14 years were assigned to a training group (9) or a control group (n = 9) | The training group performed three series of 15 contractions against an expiratory resistance (60% maximum expiratory pressure (PEmax)) 2 times a day, whereas the control group performed breathing exercises to enhance maximal inspiration. | BMI, inspiratory and expiratory muscle strength (PImax and PEmax), FVC, neck flexion force, cough efficacy (Pulmonary Index); functional status (Extended Disability Status Scale. | Rehabilitation center (for MS) | Unspecified |
| Guo et al. [45] 2019, China | Eighty-four clinically stable patients with hip fractures who were aged above 65 years were randomly divided into either a yoga group (YG) (n = 42) or a control group (CG) (n = 42); 39 subjects in the YG (age, 74.10 ± 6.59 years) and 40 subjects in the CG (age, 75.10 ± 6.96 years) completed this study. | The “upper-body yoga” training was as follows: with closed eyes, the patient concentrated on breathing to inhale slowly and deeply through one’s nostrils, to raise his/her abdomen until the lung was fully expanded. Then, exhale completely through one’s mouth with a sound of “a~~” 10 times. Additionally, the patient rotated all joints of the upper limbs during a 1-min warm-up period. In the following phase, the patients inhaled deeply and raised one of their arms slowly to 180° from the front of the body, breathing quietly 3–5 times and exhaling completely with arms facing backward. Then, lean toward the left or right and breathe quietly 3–5 times before exhaling completely with arms facing backward. Then Inhale and exhale while simultaneously bending the elbows and rotating the shoulder joints as much as possible. In the final phase, the patient closes one’s eyes and breathes in and out quietly with his/her hands placed on the abdomen to relax and meditate for 3 min, followed by two quick and forceful breaths using the sound of “ha~”. The program was performed 2 times/day, 7 days/week | FVC/predicted value (FVC%), peak cough flow, BI, the incidence of pneumonia, rates of right skills, and inclination. Patients were tested in a 30° supine position on the day of admission (T1) after 7 days of training (T2) and 4 weeks after surgery (T3). | Hospital | Unspecified |
| Tafreshi et al. [46] 2017, Switzerland | Ten healthy participants | The study consisted of four different study protocols. (1) subjects were tilted to the maximum tilt angle of 71° and then to 40° with a 3 min supine period in between. In a second step, the same experiment was conducted at 60° instead of 71° (2 and 3) both protocols were conducted at = {20°, 40°, 60°} of tilt (three experiments per protocol) with or without FES, the FES frequency was set to 40 Hz. FES pulse was bipolar and biphasic with a width of 300 μs, and its amplitude could be varied between a minimum and a maximum (between 7 and 30 mA) (4). A 5-min synchronized stepping with minimum FES input was applied (uFES = 0, i.e., IMIN) followed by a 5-min interval of maximum FES input (uFES = 1, i.e., 0.8IMAX) and a 5-min period during which the amplitude was set back to the minimum current strength. The protocol was conducted at four different tilt angles = {0°, 20°, 40°, 60°} (to identify the effect of the change in FES amplitude during the stepping with FES on the cardiovascular variables) | HR, sBP, dBP | Research institute | ERIGO (Hocoma AG, Volketswil, Switzerland) |
| Friedl-Werner et al. [47], 2020, Germany | Twenty-three young, healthy men participants (29 ± 6 years) completed the study; 11 participants were randomly assigned to a high-intensity interval training (TRAIN) | The exercise training was performed in a supine position. Four different training sessions consisting of varying numbers of countermovement jumps and hops were designed and applied to TRAIN 5 to 6 training sessions per week for 60 days. The total training duration of one session did not exceed more than 17 min using an average training load between 80% and 90% of the body weight. | Memory performance and brain regions involved using MRI and functional magnetic resonance imaging (fMRI) | Research institute | Unspecified |
| Medrinal, et al. [48] 2016, France | Twenty participants | Exercises were divided into 10 min of passive ROM for the legs, 10 min of quadriceps electrical stimulation, 10 min of passive cycle-ergometry (MotoMed Letto II®), and 10 min of FES cycling (Reha-Move®) 20 rev/min for the last two exercises. For the exercises involving electrical stimulation, a rectangular, intermittent, bidirectional current with no ramp was used (length 300 μs, frequency 35 Hz). During FES cycling, electrical stimulation was synchronized with knee extension. A 30-min rest period was allowed between each intervention for the cardiorespiratory system to return to its baseline state | Cardiac output, pulmonary artery pressure, tricuspid annular plane systolic excursion (cardiac ultrasonography) Oxygenation of vastus lateralis muscle (NIRS). Expiratory volume and RR | Hospital | MotoMed Letto II® RehaMove®, Hasomed, Germany |
| Others/Mixed domains (n = 6) | |||||
| Boccignone et al. [49] 1999, Italy | Fifty-four patients with disuse syndrome (28M, 26F), mean age 77 years) | Thirty minutes of rehabilitation treatments per session, 6 days per week. Treatment sessions included passive kinesitherapy, active kinesitherapy; early progression to sitting position; gradual progression to an upright position, exercises to restore gait, | FIM scale; Mini-Mental State Examination | Geriatric hospital | Tilt table |
| Hirakawa et al. [50] 2005, Japan | Fifty-three bedridden patients (>65 years) were divided into 2 groups: the home massage group (26) and the routine care group without massage (27) | Thirty-minute sessions of home massage rehabilitation therapy and kinesiotherapy by a massage practitioner 2 or 3 days a week for three consecutive months. Kinesitherapy: Sitting balanced exercises, sitting up exercises, Standing up exercises, Gait exercise, ROM exercises. | BI, Subjective Satisfaction and Refreshment Scale, Apathy Scale, and Self-rating Depression Scale at baseline and three months. | 3 home nursing stations, 13 visit care stations, and a one-day service center | Unspecified |
| Leite et al. [51] 2018, Brazil | Sixty-seven subjects in mechanical ventilation were divided into 3 groups: control group (CG, n = 26), stimulation of quadriceps (Quadriceps group (QG), n = 24), and (stimulation of diaphragm (Diaphragm group (DG), n = 17). | The QG and DG patients received conventional physical therapy once a day, plus a daily electrical stimulation session from the first day of randomization until ICU discharge. For the NMES of the quadriceps, the following parameters were used: Aussie current, synchronized impulse at a frequency of 50 Hz, 1 s pulse increase period, 8 s “on” (muscle contraction) period, 1 s pulse decrease period, and 30 s “off” (disconnection) period. For the NMES of the diaphragm, the following parameters were used: Aussie current, synchronized impulse at a frequency of 30 Hz, 1 s pulse increase period, 1 s “on” (muscle contraction) period, 1 s pulse decrease period, and 20 s “off” (disconnection) period. Each session was performed for 45 min at intensities that produced visible contractions. | Length of hospitalization. Peripheral muscle strength (MRC). Respiratory muscle strength using a manovacuometer. BI and. Glasgow Coma Scale | Hospital (ICU) | Neurodyn MulticorrentesTM device (Ibramed, São Paulo, Brazil), |
| Mendt et al. [52] 2021, Germany | Sixteen healthy men (age: 30.5 ± 7.5 years) after 7 days and 49 days of Head-down tilt bed rest (HDBR). Five participants underwent HDBR only (CTR), 5 participants underwent HDBR and performed resistive exercises, and 6 performed HDBR and resistive exercises superimposed with vibrations (RVE). | Exercises were performed 3 times/week with a duration of 45 min. Exercise sessions were structured as follows: (1) short warm-up (bilateral leg press with 50% of pre-bed rest maximum voluntary contraction); (2) bilateral leg press (75–80% of maximum); (3) single-leg heel raises (about 1.3 times of their HDBR1 body weight); (4) double-leg heel raises (about 1.8 times of their HDBR1 body weight); and finally (5) back and forefoot raise (performing hip and lumbar spine extension against gravity with ankle dorsiflexion; a force 1.5 times body weight was applied at the shoulders). The RVE group additionally received vibration with frequencies between 16 and 26 Hz, depending on the exercise. | Core body temperature | Research institute | Tilt bed Galileo Space exercise device. |
| Tatsumi et al. [53] 2021, Japan | Seventy-year-old man bedridden man with sarcopenia developed as a postoperative complication | The patient was treated by initiating a 6- month-long Nutrition Support Team intervention that combined nutrition, exercise therapy, and pharmacotherapy. Priority was given to patient mobilization, the balance of energy intake and expenditure, prevention of complications associated with bed rest, and prevention of the progression of generalized deconditioning. Upper body muscle training was started 5 days a week for 20 min. Lower-limb muscle training was initiated to prevent the loss of skeletal muscle. | Weight, BMI, serum creatinine, eGFR creatinine, cystatin C, eGFR cystatin. Arm and arm muscle circumference | Hospital | Unspecified |
| Bouman et al. [54] 2008, The Netherlands | One hundred and thirty-two multi-trauma patients admitted to one of the Accident and Emergency Departments (A&E) participating hospitals are included. | Intervention group: Phase 1; There were 10 sessions per week of 30 min each. In addition, fitness, gymnastics, table tennis, swimming, bowling, hand bike, wheelchair training, and archery are given. There were 2–3 sessions per week for each treatment modality of 60 min each. Phase 2: new treatment aims were added by the physiotherapist. These might include a gradual individual weight-bearing scheme, coordination training, and functional training. There were 7 therapy sessions per week of 30 min. In addition, fitness, gymnastics, table tennis, swimming, rowing, cycling, and archery are given. This is offered in 2–4 sessions per week for each treatment modality of 60 min each. | Primary outcome measure: Generic quality of life: 36-item Short-Form Health Survey (SF-36); Functional health status: FIM) | Hospital | Unspecified |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardoso, R.; Parola, V.; Neves, H.; Bernardes, R.A.; Duque, F.M.; Mendes, C.A.; Pimentel, M.; Caetano, P.; Petronilho, F.; Albuquerque, C.; et al. Physical Rehabilitation Programs for Bedridden Patients with Prolonged Immobility: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 6420. https://doi.org/10.3390/ijerph19116420
Cardoso R, Parola V, Neves H, Bernardes RA, Duque FM, Mendes CA, Pimentel M, Caetano P, Petronilho F, Albuquerque C, et al. Physical Rehabilitation Programs for Bedridden Patients with Prolonged Immobility: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(11):6420. https://doi.org/10.3390/ijerph19116420
Chicago/Turabian StyleCardoso, Remy, Vitor Parola, Hugo Neves, Rafael A. Bernardes, Filipa Margarida Duque, Carla A. Mendes, Mónica Pimentel, Pedro Caetano, Fernando Petronilho, Carlos Albuquerque, and et al. 2022. "Physical Rehabilitation Programs for Bedridden Patients with Prolonged Immobility: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 11: 6420. https://doi.org/10.3390/ijerph19116420
APA StyleCardoso, R., Parola, V., Neves, H., Bernardes, R. A., Duque, F. M., Mendes, C. A., Pimentel, M., Caetano, P., Petronilho, F., Albuquerque, C., Sousa, L. B., Malça, C., Durães, R., Xavier, W., Parreira, P., Apóstolo, J., & Cruz, A. (2022). Physical Rehabilitation Programs for Bedridden Patients with Prolonged Immobility: A Scoping Review. International Journal of Environmental Research and Public Health, 19(11), 6420. https://doi.org/10.3390/ijerph19116420