
Trends of the Prevalence of Pre-gestational Diabetes in 2030 and 2050 in Belgrade Cohort



 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Egan, A.M.; Dunne, F.P. Epidemiology of Gestational and Pregestational Diabetes Mellitus. In Gestational Diabetes; Karger Publishers: Basel, Switzerland, 2019; Volume 28, pp. 1–10. [Google Scholar]
- Gualdani, E.; Di Cianni, G.; Seghieri, M.; Francesconi, P.; Seghieri, G. Pregnancy outcomes and maternal characteristics in women with pregestational and gestational diabetes: A retrospective study on 206,917 singleton live births. Acta Diabetol. 2021, 58, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Khalifeh, A.; Breathnach, F.; Coulter-Smith, S.; Robson, M.; Fitzpatrick, C.; Malone, F. Changing trends in diabetes mellitus in pregnancy. J. Obstet. Gynaecol. 2014, 34, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Xodo, S.; Londero, A.P.; D’agostin, M.; Novak, A.; Galasso, S.; Pittini, C.; Baccarini, G.; Grimaldi, F.; Driul, L. Is glycated hemoglobin a1c level associated with adverse pregnancy outcomes of women affected by pre-gestational diabetes? Medicina 2021, 57, 461. [Google Scholar] [CrossRef] [PubMed]
- Mackin, S.T.; Nelson, S.M.; Kerssens, J.J.; Wood, R.; Wild, S.; Colhoun, H.M.; Leese, G.P.; Philip, S.; Lindsay, R.S. Diabetes and pregnancy: National trends over a 15 year period. Diabetologia 2018, 61, 1081–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maahs, D.M.; Snively, B.M.; Bell, R.A.; Dolan, L.; Hirsch, I.; Imperatore, G.; Linder, B.; Marcovina, S.M.; Mayer-Davis, E.J.; Pettitt, D.J.; et al. Higher prevalence of elevated albumin excretion in youth with type 2 than type 1 diabetes: The SEARCH for Diabetes in Youth study. Diabetes Care 2007, 30, 2593–2598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morampudi, S.; Balasubramanian, G.; Gowda, A.; Zomorodi, B.; Patil, A.S. The challenges and recommendations for gestational diabetes mellitus care in India: A review. Front. Endocrinol. 2017, 8, 56. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, K.K.; De Courten, M.; Kapur, A. Health system and societal barriers for gestational diabetes mellitus (GDM) services—Lessons from World Diabetes Foundation supported GDM projects. BMC Int. Health Hum. Rights 2012, 12, 1. [Google Scholar] [CrossRef] [Green Version]
- City Institute of Public Health Belgrade. City Institute of Public Health of Belgrade Statistical Report of Health Care in Belgrade for 2020; City Institute of Public Health of Belgrade: Belgrade, Serbia, 2021. [Google Scholar]
- Gojnic, M.; Todorovic, J.; Stanisavljevic, D.; Jotic, A.; Lukic, L.; Milicic, T.; Dugalic, S. Maternal and Fetal Outcomes among Pregnant Women with Diabetes. Int. J. Environ. Res. Public Health 2022, 19, 3684. [Google Scholar] [CrossRef]
- Pineda, E.; Sanchez-Romero, L.M.; Brown, M.; Jaccard, A.; Jewell, J.; Galea, G.; Webber, L.; Breda, J. Forecasting Future Trends in Obesity across Europe: The Value of Improving Surveillance. Obes. Facts 2018, 11, 360–371. [Google Scholar] [CrossRef]
- Dall, T.M.; Yang, W.; Gillespie, K.; Mocarski, M.; Byrne, E.; Cintina, I.; Beronja, K.; Semilla, A.P.; Iacobucci, W.; Hogan, P.F. The economic burden of elevated blood glucose levels in 2017: Diagnosed and undiagnosed diabetes, gestational diabetes mellitus, and prediabetes. Diabetes Care 2019, 42, 1661–1668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coton, S.J.; Nazareth, I.; Petersen, I. A cohort study of trends in the prevalence of pregestational diabetes in pregnancy recorded in UK general practice between 1995 and 2012. BMJ Open 2016, 6, e009494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yefet, E.; Jeda, E.; Tzur, A.; Nachum, Z. Markers for undiagnosed type 2 diabetes mellitus during pregnancy—A population-based retrospective cohort study. J. Diabetes 2020, 12, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Isabey, E.P.; Pylypjuk, C.L. The Relationship between Fetal Abdominal Wall Thickness and Intrapartum Complications amongst Mothers with Pregestational Type 2 Diabetes. J. Diabetes Res. 2021, 2021, 5544599. [Google Scholar] [CrossRef] [PubMed]
- Van Otterloo, L.; Connelly, C.; Gould, J.; Abreo, A.; Main, E. Mothers at Risk: Factors Affecting Maternal Postpartum Length of Stay. J. Perinat. Neonatal Nurs. 2018, 32, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.N.; Choi, D.W.; Kim, D.S.; Park, E.C.; Kwon, J.Y. Maternal age and risk of early neonatal mortality: A national cohort study. Sci. Rep. 2021, 11, 814. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ren, X.; He, L.; Li, J.; Zhang, S.; Chen, W. Maternal age and the risk of gestational diabetes mellitus: A systematic review and meta-analysis of over 120 million participants. Diabetes Res. Clin. Pract. 2020, 162, 108044. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Number of Women with Pregestational Diabetes | Prevalence of Pregestational Diabetes among DM in Pregnancy (%) | Prevalence of Pregestational Diabetes among All Pregnancies (%) | Number of Women with GDM | Prevalence of GDM among DM in Pregnancy (%) | Prevalence of GDM among All Pregnancies (%) |
|---|---|---|---|---|---|---|
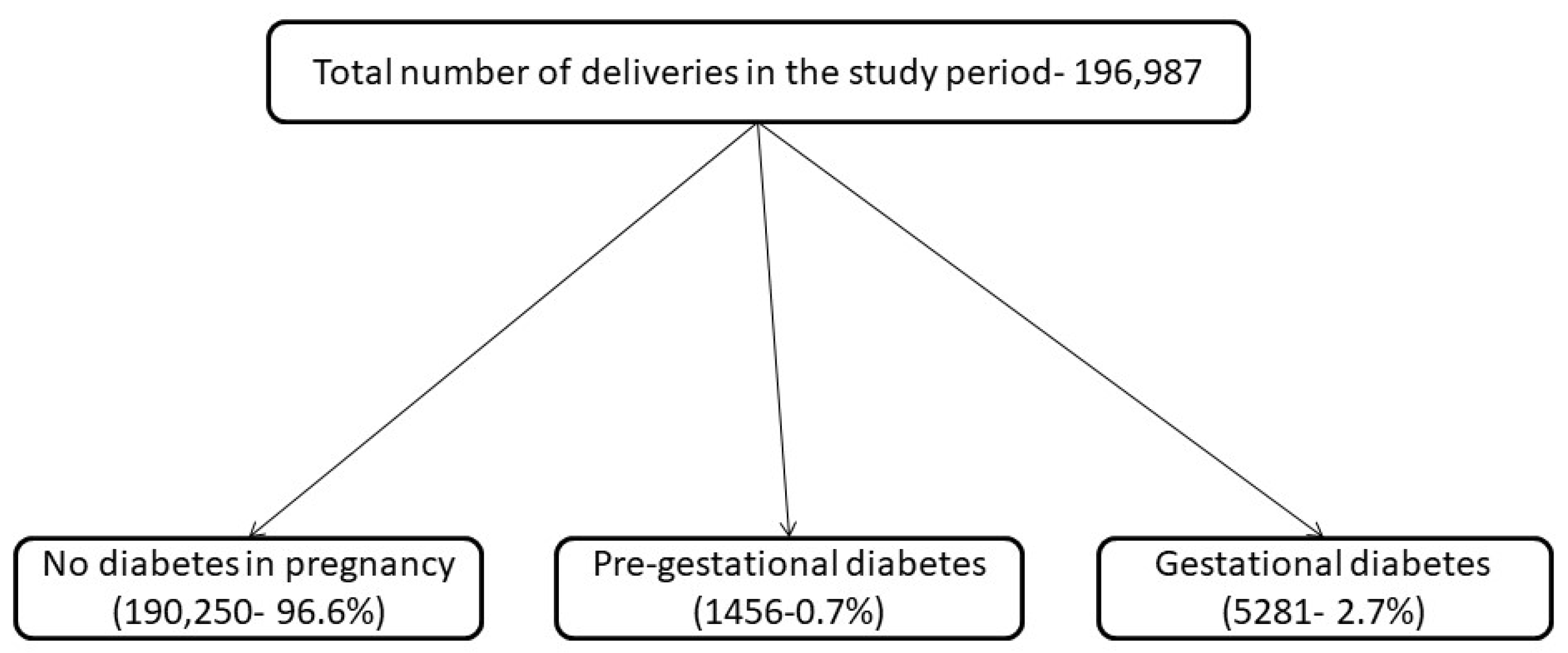
| 2010 | 111 | 15.30 | 0.6 | 614 | 84.7 | 3.4 |
| 2011 | 111 | 14.90 | 0.6 | 633 | 85.1 | 3.6 |
| 2012 | 77 | 8.50 | 0.4 | 831 | 91.5 | 4.5 |
| 2013 | 89 | 8.70 | 0.4 | 933 | 91.3 | 5.2 |
| 2014 | 68 | 11.70 | 0.4 | 513 | 88.3 | 2.8 |
| 2015 | 99 | 22.70 | 0.5 | 338 | 77.3 | 1.8 |
| 2016 | 90 | 19.70 | 0.5 | 367 | 80.3 | 2.0 |
| 2017 | 67 | 16.80 | 0.4 | 333 | 83.2 | 1.8 |
| 2018 | 261 | 36.70 | 1.4 | 450 | 63.3 | 2.5 |
| 2019 | 260 | 59.10 | 1.4 | 180 | 40.9 | 1.0 |
| 2020 | 223 | 71.50 | 1.4 | 89 | 28.5 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dugalic, S.; Petronijevic, M.; Vasiljevic, B.; Todorovic, J.; Stanisavljevic, D.; Jotic, A.; Lukic, L.; Milicic, T.; Lalić, N.; Lalic, K.; et al. Trends of the Prevalence of Pre-gestational Diabetes in 2030 and 2050 in Belgrade Cohort. Int. J. Environ. Res. Public Health 2022, 19, 6517. https://doi.org/10.3390/ijerph19116517
Dugalic S, Petronijevic M, Vasiljevic B, Todorovic J, Stanisavljevic D, Jotic A, Lukic L, Milicic T, Lalić N, Lalic K, et al. Trends of the Prevalence of Pre-gestational Diabetes in 2030 and 2050 in Belgrade Cohort. International Journal of Environmental Research and Public Health. 2022; 19(11):6517. https://doi.org/10.3390/ijerph19116517
Chicago/Turabian StyleDugalic, Stefan, Milos Petronijevic, Brankica Vasiljevic, Jovana Todorovic, Dejana Stanisavljevic, Aleksandra Jotic, Ljiljana Lukic, Tanja Milicic, Nebojsa Lalić, Katarina Lalic, and et al. 2022. "Trends of the Prevalence of Pre-gestational Diabetes in 2030 and 2050 in Belgrade Cohort" International Journal of Environmental Research and Public Health 19, no. 11: 6517. https://doi.org/10.3390/ijerph19116517
APA StyleDugalic, S., Petronijevic, M., Vasiljevic, B., Todorovic, J., Stanisavljevic, D., Jotic, A., Lukic, L., Milicic, T., Lalić, N., Lalic, K., Stoiljkovic, M., Terzic-Supic, Z., Stanisavljevic, T., Stefanovic, A., Stefanovic, K., Vrzic-Petronijevic, S., Macura, M., Pantic, I., Piperac, P., ... Gojnic, M. (2022). Trends of the Prevalence of Pre-gestational Diabetes in 2030 and 2050 in Belgrade Cohort. International Journal of Environmental Research and Public Health, 19(11), 6517. https://doi.org/10.3390/ijerph19116517