
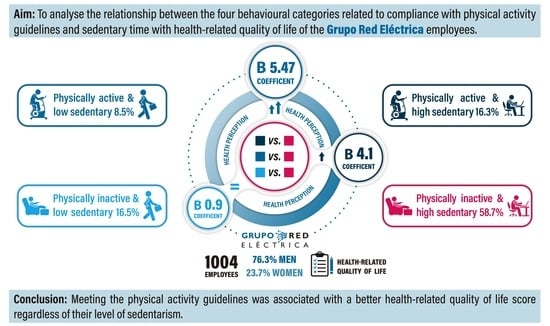
Association between Physical Activity Guidelines and Sedentary Time with Workers’ Health-Related Quality of Life in a Spanish Multinational Company

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Procedure
2.2. Measures
2.2.1. Health-Related Quality of Life
2.2.2. WHO Physical Activity Guidelines
2.2.3. Sedentary Time
2.2.4. Determination of Physical Behaviour Categories
2.2.5. Covariates
2.3. Statistical Analysis
2.3.1. Continuous Analysis
2.3.2. Categorical Analysis
2.3.3. Minimal Clinically Important Difference (MCID)
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tudor-Locke, C.; Leonardi, C.; Johnson, W.D.; Katzmarzyk, P.T. Time spent in physical activity and sedentary behaviors on the working day: The American time use survey. J. Occup. Environ. Med. 2011, 53, 1382–1387. [Google Scholar] [CrossRef]
- McCrady, S.K.; Levine, J.A. Sedentariness at work: How much do we really sit? Obesity 2009, 17, 2103–2105. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, N.; Kitabayashi, M.; Kikuchi, H.; Sasai, H.; Oka, K.; Nakata, Y.; Tanaka, S.; Inoue, S. Comparison of accelerometer-measured sedentary behavior, and light- and moderate-to-vigorous-intensity physical activity in white- and blue-collar workers in a Japanese manufacturing plant. J. Occup. Health 2018, 60, 246–253. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- European Union. Special Eurobarometer 472: Sport and Physical Activity; European Union: Brussels, Belgium, 2017. [Google Scholar]
- Bennie, J.A.; De Cocker, K.; Smith, J.J.; Wiesner, G.H. The epidemiology of muscle-strengthening exercise in Europe: A 28-country comparison including 280,605 adults. PloS ONE 2020, 15, e0242220. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Martel, J.-P.; Dupuis, G. Quality of Work Life: Theoretical and Methodological Problems, and Presentation of a New Model and Measuring Instrument. Soc. Indic. Res. 2006, 77, 333–368. [Google Scholar] [CrossRef]
- Barranco-Ruiz, Y.; Paz-Viteri, S.; Villa-González, E. Dance Fitness Classes Improve the Health-Related Quality of Life in Sedentary Women. Int. J. Environ. Res. Public Health 2020, 17, 3771. [Google Scholar] [CrossRef]
- Fang, Y.Y.; Huang, C.Y.; Hsu, M.C. Effectiveness of a physical activity program on weight, physical fitness, occupational stress, job satisfaction and quality of life of overweight employees in high-tech industries: A randomized controlled study. Int. J. Occup. Saf. Ergon. JOSE 2019, 25, 621–629. [Google Scholar] [CrossRef]
- Nguyen, T.M.; Nguyen, V.H.; Kim, J.H. Physical Exercise and Health-Related Quality of Life in Office Workers: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3791. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Television time and continuous metabolic risk in physically active adults. Med. Sci. Sports Exerc. 2008, 40, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Bakrania, K.; Edwardson, C.L.; Bodicoat, D.H.; Esliger, D.W.; Gill, J.M.; Kazi, A.; Velayudhan, L.; Sinclair, A.J.; Sattar, N.; Biddle, S.J.; et al. Associations of mutually exclusive categories of physical activity and sedentary time with markers of cardiometabolic health in English adults: A cross-sectional analysis of the Health Survey for England. BMC Public Health 2016, 16, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mañas, A.; Del Pozo-Cruz, B.; Rodríguez-Gómez, I.; Leal-Martín, J.; Losa-Reyna, J.; Rodríguez-Mañas, L.; García-García, F.J.; Ara, I. Dose-response association between physical activity and sedentary time categories on ageing biomarkers. BMC Geriatr. 2019, 19, 270. [Google Scholar] [CrossRef] [PubMed]
- Henson, J.; Edwardson, C.L.; Morgan, B.; Horsfield, M.A.; Khunti, K.; Davies, M.J.; Yates, T. Sedentary Time and MRI-Derived Measures of Adiposity in Active Versus Inactive Individuals. Obesity 2018, 26, 29–36. [Google Scholar] [CrossRef]
- Elsangedy, H.M.; Oliveira, G.T.A.; Machado, D.; Tavares, M.P.M.; Araújo, A.O.; Krinski, K.; Browne, R.A.V.; Gregório da Silva, S. Effects of Self-selected Resistance Training on Physical Fitness and Psychophysiological Responses in Physically Inactive Older Women: A Randomized Controlled Study. Percept. Mot. Skills 2021, 128, 467–491. [Google Scholar] [CrossRef]
- Hernández Sánchez, S.; Carrero, J.J.; Morales, J.S.; Ruiz, J.R. Effects of a resistance training program in kidney transplant recipients: A randomized controlled trial. Scand. J. Med. Sci. Sports 2021, 31, 473–479. [Google Scholar] [CrossRef]
- Oliveira-Dantas, F.F.; Browne, R.A.V.; Oliveira, R.S.; Cabral, L.L.P.; de Farias Junior, L.F.; Costa, E.C. Effect of High-velocity Resistance Exercise on 24-h Blood Pressure in Hypertensive Older Women. Int. J. Sports Med. 2021, 42, 41–47. [Google Scholar] [CrossRef]
- Cheema, B.S.; Chan, D.; Fahey, P.; Atlantis, E. Effect of progressive resistance training on measures of skeletal muscle hypertrophy, muscular strength and health-related quality of life in patients with chronic kidney disease: A systematic review and meta-analysis. Sports Med. 2014, 44, 1125–1138. [Google Scholar] [CrossRef]
- Hart, P.D.; Buck, D.J. The effect of resistance training on health-related quality of life in older adults: Systematic review and meta-analysis. Health Promot. Perspect. 2019, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- INE. Encuesta Europea de Salud en España (EESE). Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/EncuestaEuropea/Enc_Eur_Salud_en_Esp_2014.htm (accessed on 20 January 2018).
- Chau, J.Y.; Van Der Ploeg, H.P.; Dunn, S.; Kurko, J.; Bauman, A.E. Validity of the occupational sitting and physical activity questionnaire. Med. Sci. Sports Exerc. 2012, 44, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.K.; Lynch, B.M.; Winkler, E.A.; Gardiner, P.A.; Healy, G.N.; Dunstan, D.W.; Owen, N. Validity of a multi-context sitting questionnaire across demographically diverse population groups: AusDiab3. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, A.G.; van Lanschot, J.J.; Stalmeier, P.F.; van Sandick, J.W.; Hulscher, J.B.; de Haes, J.C.; Sprangers, M.A. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2004, 13, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Maes, I.; Ketels, M.; Van Dyck, D.; Clays, E. The occupational sitting and physical activity questionnaire (OSPAQ): A validation study with accelerometer-assessed measures. BMC Public Health 2020, 20, 1072. [Google Scholar] [CrossRef] [PubMed]
- Jancey, J.; Tye, M.; McGann, S.; Blackford, K.; Lee, A.H. Application of the Occupational Sitting and Physical Activity Questionnaire (OSPAQ) to office based workers. BMC Public Health 2014, 14, 762. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Liu, B.; Sun, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in Adherence to the Physical Activity Guidelines for Americans for Aerobic Activity and Time Spent on Sedentary Behavior Among US Adults, 2007 to 2016. JAMA Netw. Open 2019, 2, e197597. [Google Scholar] [CrossRef] [Green Version]
- Loyen, A.; Clarke-Cornwell, A.M.; Anderssen, S.A.; Hagströmer, M.; Sardinha, L.B.; Sundquist, K.; Ekelund, U.; Steene-Johannessen, J.; Baptista, F.; Hansen, B.H.; et al. Sedentary Time and Physical Activity Surveillance Through Accelerometer Pooling in Four European Countries. Sports Med. 2017, 47, 1421–1435. [Google Scholar] [CrossRef] [Green Version]
- Spittaels, H.; Van Cauwenberghe, E.; Verbestel, V.; De Meester, F.; Van Dyck, D.; Verloigne, M.; Haerens, L.; Deforche, B.; Cardon, G.; De Bourdeaudhuij, I. Objectively measured sedentary time and physical activity time across the lifespan: A cross-sectional study in four age groups. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 149. [Google Scholar] [CrossRef] [Green Version]
- ILO. International Standard Classification of Occupations: ISCO-08. Available online: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_172572.pdf (accessed on 15 January 2018).
- Samsa, G.; Edelman, D.; Rothman, M.L.; Williams, G.R.; Lipscomb, J.; Matchar, D. Determining clinically important differences in health status measures: A general approach with illustration to the Health Utilities Index Mark II. Pharmacoeconomics 1999, 15, 141–155. [Google Scholar] [CrossRef]
- Copay, A.G.; Subach, B.R.; Glassman, S.D.; Polly, D.W., Jr.; Schuler, T.C. Understanding the minimum clinically important difference: A review of concepts and methods. Spine J. 2007, 7, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Elliott, C.G.; Scott, K.; Visintini, S.; Reed, J.L. Device-measured physical activity, sedentary behaviour and cardiometabolic health and fitness across occupational groups: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 30. [Google Scholar] [CrossRef] [PubMed]
- Kniffin, K.M.; Narayanan, J.; Anseel, F.; Antonakis, J.; Ashford, S.P.; Bakker, A.B.; Bamberger, P.; Bapuji, H.; Bhave, D.P.; Choi, V.K.; et al. COVID-19 and the workplace: Implications, issues, and insights for future research and action. Am. Psychol. 2021, 76, 63–77. [Google Scholar] [CrossRef]
- Wang, Y.; Nie, J.; Ferrari, G.; Rey-Lopez, J.P.; Rezende, L.F.M. Association of Physical Activity Intensity with Mortality: A National Cohort Study of 403 681 US Adults. JAMA Intern. Med. 2021, 181, 203–211. [Google Scholar] [CrossRef]
- Rollo, S.; Prapavessis, H. A combined health action process approach and mHealth intervention to reduce workplace sitting time in office-working adults: A secondary analysis examining health-related quality of life and work performance outcomes. Psychol. Health 2020, 36, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Lee, H.; Cardinal, B.J. Daily movement patterns and biological markers among adults in the United States. Prev. Med. 2014, 60, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; De Craemer, M.; De Cocker, K.; Powell, L.; Van Cauwenberg, J.; Dall, P.; Hamer, M.; Stamatakis, E. How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br. J. Sports Med. 2019, 53, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Hupin, D.; Raffin, J.; Barth, N.; Berger, M.; Garet, M.; Stampone, K.; Celle, S.; Pichot, V.; Bongue, B.; Barthelemy, J.C.; et al. Even a Previous Light-Active Physical Activity at Work Still Reduces Late Myocardial Infarction and Stroke in Retired Adults Aged>65 Years by 32%: The PROOF Cohort Study. Front. Public Health 2019, 7, 51. [Google Scholar] [CrossRef]
- Tarro, L.; Llauradó, E.; Ulldemolins, G.; Hermoso, P.; Solà, R. Effectiveness of Workplace Interventions for Improving Absenteeism, Productivity, and Work Ability of Employees: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2020, 17, 1901. [Google Scholar] [CrossRef] [Green Version]
- Arslan, S.S.; Alemdaroğlu, İ.; Karaduman, A.A.; Yilmaz, Ö.T. The effects of physical activity on sleep quality, job satisfaction, and quality of life in office workers. Work 2019, 63, 3–7. [Google Scholar] [CrossRef]
- Torbeyns, T.; de Geus, B.; Bailey, S.; De Pauw, K.; Decroix, L.; Van Cutsem, J.; Meeusen, R. Cycling on a Bike Desk Positively Influences Cognitive Performance. PloS ONE 2016, 11, e0165510. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Sample | “Physically Active & Low Sedentary” | “Physically Active & High Sedentary” | “Physically Inactive & Low Sedentary” | “Physically Inactive & High Sedentary” |
|---|---|---|---|---|---|
| N = 1004 | N = 85; 8.5% | N = 164; 16.3% | N = 166; 16.5% | N = 589; 58.7% | |
| Age (years) | |||||
| Less than 25 years | 7 (0.7) | 0 (0.0) | 3 (1.8) | 0 (0.0) | 4 (0.7) |
| From 26 to 35 years | 150 (14.9) | 20 (23.5) | 29 (17.7) | 26 (15.7) | 75 (12.7) |
| From 36 to 45 years | 488 (48.6) | 44 (51.8) | 80 (48.8) | 80 (48.2) | 284 (48.2) |
| From 46 to 55 years | 207 (20.6) | 13 (15.3) | 29 (17.7) | 29 (17.5) | 136 (23.1) |
| More than 55 years | 152 (15.1) | 8 (9.4) | 23 (14) | 31 (18.7) | 90 (15.3) |
| Sex | |||||
| Male | 766 (76.3) | 82 (96.5) | 128 (78.0) | 142 (85.5) | 414 (70.3) |
| Female | 238 (23.7) | 3 (3.5) | 36 (22.0) | 24 (14.5) | 175 (29.7) |
| Type of occupation | |||||
| Facilities workers | 252 (25.1) | 61 (71.8) | 20 (12.2) | 112 (67.5) | 59 (10.0) |
| Office workers | 752 (74.9) | 24 (28.2) | 144 (87.8) | 54 (32.5) | 530 (90.0) |
| Number of diseases | |||||
| 0 | 430 (42.8) | 50 (58.8) | 76 (46.3) | 80 (48.2) | 224 (38.0) |
| 1 | 370 (36.9) | 22 (25.9) | 64 (39.0) | 59 (35.5) | 225 (38.2) |
| 2 | 148 (14.7) | 12 (14.1) | 19 (11.6) | 17 (10.2) | 100 (17.0) |
| 3 | 45 (4.5) | 1 (1.2) | 4 (2.4) | 7 (4.2) | 33 (5.6) |
| 4 | 10 (1.0) | 0 (0.0) | 1 (0.6) | 3 (1.8) | 6 (1.0) |
| 5 | 1 (0.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.2) |
| ≥6 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Meet WHO aerobic guidelines | |||||
| Yes | 494 (49.2) | 85 (100.0) | 164 (100.0) | 69 (41.6) | 176 (29.9) |
| No | 510 (50.8) | 0 (0.0) | 0 (0.0) | 97 (58.4) | 413 (70.1) |
| Meet WHO strength guidelines | |||||
| Yes | 327 (32.6) | 85 (100.0) | 164 (100.0) | 16 (9.6) | 62 (10.5) |
| No | 677 (67.4) | 0 (0.0) | 0 (0.0) | 150 (90.4) | 527 (89.5) |
| Meet WHO aerobic & strength guidelines | |||||
| Yes | 249 (24.8) | 85 (100.0) | 164 (100.0) | 0 (0.0) | 0 (0.0) |
| No | 755 (75.2) | 0 (0.0) | 0 (0.0) | 166 (100.0) | 589 (100.0) |
| Sedentary time | |||||
| High | 753 (75.0) | 0 (0.0) | 164 (100.0) | 0 (0.0) | 589 (100.0) |
| Low | 251 (25.0) | 85 (100.0) | 0 (0.0) | 166 (100.0) | 0 (0.0) |
| HRQoL score | 77.17 ± 16.11 | 83.60 ± 10.39 | 80.25 ± 15.16 | 78.23 ± 14.32 | 75.08 ± 17.12 |
| Active | Inactive | Low Sedentary | High Sedentary | p-Value | |
|---|---|---|---|---|---|
| MVPA guidelines | N = 494 80.53 ± 14.44 | N = 510 73.91 ± 16.97 | _ | _ | <0.001 * |
| Strength guidelines | N = 327 79.99 ± 15.09 | N = 677 75.8 ± 16.43 | _ | _ | <0.001 * |
| MVPA + Strength guidelines | N = 249 81.39 ± 13.79 | N = 755 75.77 ± 16.58 | _ | _ | <0.001 * |
| Sedentary status | _ | _ | N = 251 80.05 ± 13.34 | N = 753 76.21 ± 16.84 | 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Redondo, P.; Marín, V.; Leal-Martín, J.; Ruiz-Moreno, C.; Giráldez-Costas, V.; Urdiola, P.; Ara, I.; Mañas, A. Association between Physical Activity Guidelines and Sedentary Time with Workers’ Health-Related Quality of Life in a Spanish Multinational Company. Int. J. Environ. Res. Public Health 2022, 19, 6592. https://doi.org/10.3390/ijerph19116592
Gómez-Redondo P, Marín V, Leal-Martín J, Ruiz-Moreno C, Giráldez-Costas V, Urdiola P, Ara I, Mañas A. Association between Physical Activity Guidelines and Sedentary Time with Workers’ Health-Related Quality of Life in a Spanish Multinational Company. International Journal of Environmental Research and Public Health. 2022; 19(11):6592. https://doi.org/10.3390/ijerph19116592
Chicago/Turabian StyleGómez-Redondo, Paola, Victoria Marín, Javier Leal-Martín, Carlos Ruiz-Moreno, Verónica Giráldez-Costas, Pilar Urdiola, Ignacio Ara, and Asier Mañas. 2022. "Association between Physical Activity Guidelines and Sedentary Time with Workers’ Health-Related Quality of Life in a Spanish Multinational Company" International Journal of Environmental Research and Public Health 19, no. 11: 6592. https://doi.org/10.3390/ijerph19116592