1. Introduction
The COVID-19 pandemic challenged our healthcare systems tremendously and had major consequences for people’s lives and their mental health [
1,
2,
3]. Emergency healthcare workers directly involved in dealing with the COVID-19 pandemic experienced depression (22.8%), anxiety (23.2%), and insomnia (38.9%) [
4,
5], threatening the continuity of care delivered by them and their teams [
6,
7,
8,
9]. To safeguard employee wellbeing and continuity of care, healthcare organizations should encourage individual and team resilience, referring to the ability to “bounce back” from stressful situations [
10,
11]. Resilience has been studied as a personality trait, referring to psychological resilience, as a process of structuring feedback and adaptation, and as a capacity that could be developed [
11,
12,
13,
14]. From a management science perspective, the capacity view is most suitable for the purpose of this study, because resilience as a capacity can be enhanced with intervention or training in an organizational context [
11,
15]. In addition to the types of resilience, research defines resilience at the individual, team, and organizational level. In the healthcare hospital context, even on the smallest scale, the care of a patient does not solely rely on one resilient healthcare worker [
7]. Teams need to respond and adjust as a unity to overcome the unprecedented challenges the healthcare sector has witnessed and will continue to face [
16], indicating the importance of understanding team resilience in addition to individual resilience. Team resilience can be defined as: “the capacity of a team to withstand and overcome stressors in a manner that enables sustained performance; it helps teams handle and bounce back from challenges that can endanger their cohesiveness and performance” [
17] (p. 177). A highly resilient emergency healthcare team is able to manage trade-offs between competing goals, collaborate across specialists, and use collective sensemaking [
18]. Although recent research suggests that lower-level processes facilitate the development of resilience at higher levels [
19,
20], the relationship between individual resilience and team resilience is not that obvious. For example, synergetic teams can elevate team resilience above and beyond individual levels. Research is needed to empirically test the interplay between individual and team resilience, as well as their antecedents; for example, to show whether stimuli of individual resilience cumulate in team resilience or whether separate stimuli are required [
11,
16,
19,
20].
Literature argues that individual, team-level, and contextual factors play a role in the development of team resilience [
11,
16,
21,
22]. This study investigates two main predictors of team resilience, namely the team-level factor, team familiarity, and the contextual factor, transformational leadership, as these conditions are within the circle of influence of an organization to intervene on. First, team familiarity is defined as: “the extent to which team members have personal knowledge of each other’s strengths, weaknesses, preferences, styles’’ [
21] (p. 9), thus, as a capacity that could be developed or stimulated, rather than just ‘the duration of work experience’. Team familiarity is associated with individual resilience [
23] by creating psychological safety [
24], lowering barriers to ask for help [
25], and enabling individuals to learn from each other [
26,
27]. In addition, team familiarity is related to team resilience [
21], as team members who are more familiar with each other are more likely to cooperate well by integrating their expertise, resulting in collective action [
24,
25]. Second, transformational leadership is defined as: “The leader elevates the follower’s level of maturity and ideals as well as concerns for achievement, self-actualization, and the wellbeing of others, the organization, and society” [
28] (p. 11). At the individual level, transformational leaders are able to take care of the psychological safety of their team members by creating an environment of openness and trust [
24], lowering barriers to ask for help and support, and encouraging feelings of belonging to a team [
24,
29,
30], thereby increasing individual resilience [
31]. Transformational leadership is also associated with team resilience [
32] by clarifying objectives, showing initiative, and encouraging creative thinking and flexibility to adjust to adversity [
33,
34]. Both conditions of team familiarity and transformational leadership became salient in the context of emergency healthcare delivery during the COVID-19 pandemic. Many healthcare teams were forced to mix up their team members and reorganize their work responsibilities [
35], making unfamiliarity with team members’ expertise inevitable [
36]. In addition, team leaders were pressured to simultaneously ensure the psychological safety of their employees [
24], convince their team that the crisis situation was surmountable [
29], and deal with staff shortages, possibly even taking over care duties themselves [
37], requiring them to set priorities.
In sum, previous research has provided arguments for team familiarity effects and transformational leadership effects on either individual resilience [
23,
31] or team resilience [
21,
32]. However, there is scant empirical evidence on these effects and their interplay, particularly at times of crises such as the COVID-19 pandemic [
16,
19]. This study aims to show (I) whether team resilience is a standalone concept, more than the cumulative resilience of team members; (II) whether team familiarity and transformational leadership influence team resilience; and (III) whether these effects are mediated by individual resilience, ensuring team members’ psychological safety, or enhance team resilience directly (synergy effects). The study also accounts for psychological characteristics and social support. Self-efficacy and optimism have been identified as antecedents of individual resilience, helping to adapt to and anticipate different and tense circumstances [
31,
38]. Moreover, social support from family and friends might facilitate healthcare employees’ ability to bounce back from adversity or stress [
39], by providing opportunities to express their emotions and needs and enhancing their psychological safety [
24]. Thus, this article aims to investigate to what extent transformational leadership and team familiarity influence the level of team resilience in the context of emergency healthcare teams, and to what extent these relationships are mediated by the level of individual resilience, accounting for psychological characteristics and social support.
4. Discussion
This study empirically investigated whether ‘team resilience is the sum of individual resilience, or more than the sum of its parts’ and how it can be influenced. Previous literature reviews have conceptualized individual and team resilience and identified their conceptual differences [
16,
19]. However, empirical research, such as this study, is urgently needed to empirically test the conceptualization presented in the aforementioned literature reviews [
16,
19]. Testing this conceptualization highlights the necessity of interventions at different levels within an organization to enhance both individual and team resilience. Findings show that individual and team resilience are two different constructs. The principal component analysis shows that respondents unconsciously identified the two variables when filling out the questionnaire. This demonstrates that resilience scales validated at the individual level are not necessarily valid to use at the team level, confirming the expectations of recent prior research [
13,
22]. This implies that studying individual resilience is not sufficient to develop an understanding of resilience at higher levels in the organization; team resilience must be studied in its own right. Moreover, the results show a positive relation between individual and team resilience, suggesting that individuals who have the capacity to react and overcome adversity will create a team environment that positively impacts the resilience of their teams as a whole. However, only 12.4% of the variance in team resilience can be explained by individual resilience, leaving 87.6% of the variance to be explained by other individual, contextual, and team-level factors. This implies that team resilience is a standalone concept that could not be fully explained through individual resilience and that research must identify distinct predictors of team resilience.
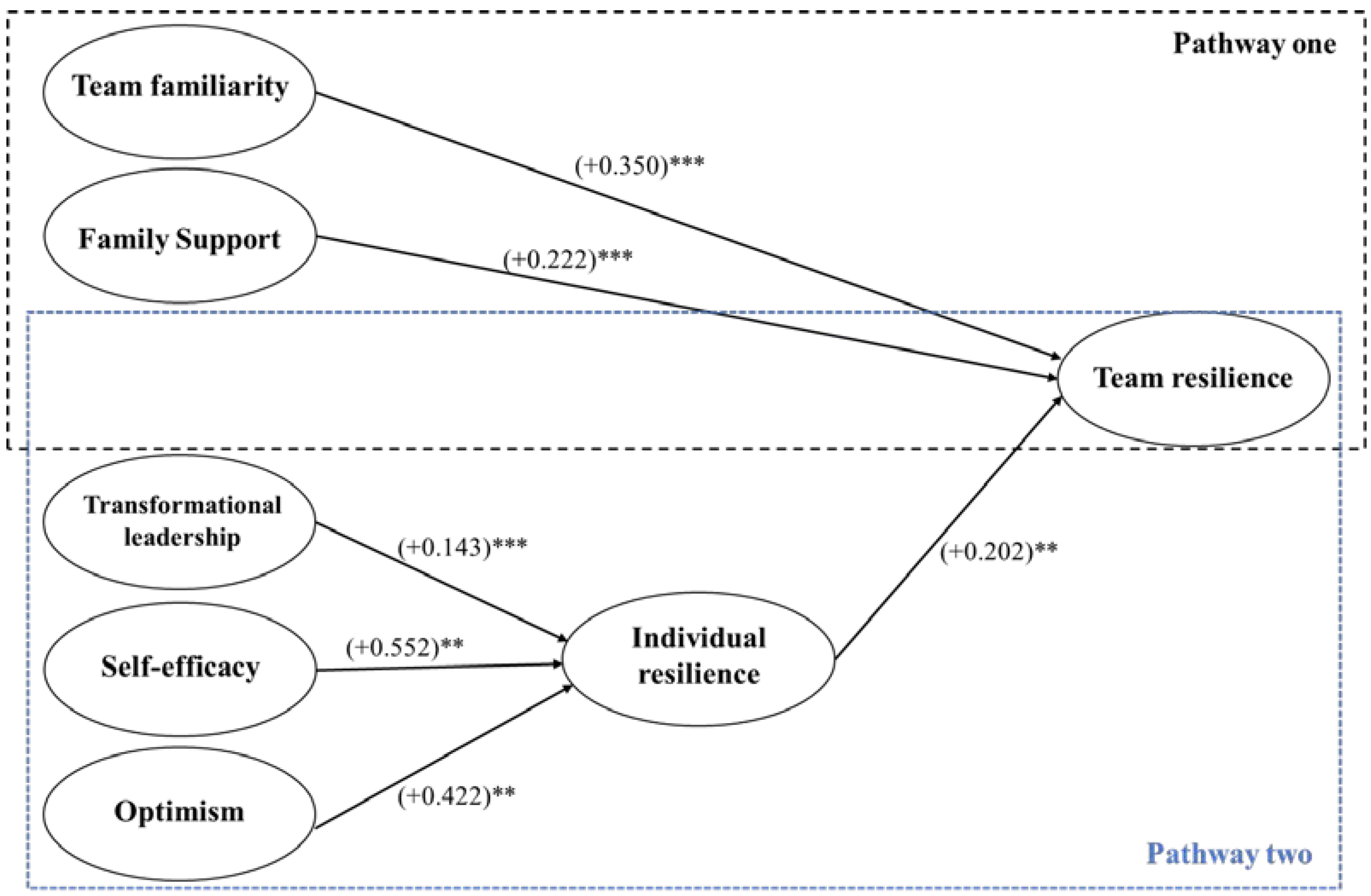
When looking at the predictors, this article identifies two distinct pathways to encourage team resilience or individual resilience. On the one hand, familiarizing team members with each other and mobilizing family support stimulates team resilience directly. On the other hand, transformational leadership, and staffing optimistic team members with high levels of self-efficacy stimulates individual resilience, which contributes indirectly but limitedly to the level of team resilience. This is important since team resilience is essential for the continuity of care, while individual resilience is essential for the mental health and wellbeing of healthcare professionals. The findings validate prior conceptual work that distinguished team resilience predictors from individual resilience predictors and called for empirically testing both in a variety of research contexts [
16,
19]. In the following sections, these two pathways are discussed in more detail.
The first pathway indicates that interventions to enhance team resilience directly should focus on familiarizing team members with each other and mobilizing family support. The results show that team familiarity has a positive significant effect on team resilience but not on individual resilience, meaning that being familiar with other team members does not so much increase one’s own resilience but only that of the team as a whole. The findings correspond to prior research in the context of elite sports [
48], but deviate from a study in the healthcare context [
23]. The latter study associated individual resilience with a team intervention that enhanced team familiarity and simultaneously provided space for caring and mindfulness. Comparing the findings of both studies leads us to conclude that it must have been the caring and mindfulness elements that contributed to employee psychological safety, while team familiarity only enhances the resilience of the team. A plausible explanation for the latter could be drawn from transactive memory theory. Knowing each other’s strengths, weaknesses, preferences, and styles is a source of synergy, achieving more together than one could possibly have achieved alone [
26,
49], but it is not a source of mental health and self-protection. On the contrary, team members have a higher level of commitment to collaborate together when they are familiar with each other [
44]. The emergency healthcare context is characterized by a lack of slack resources and work that ‘has to be done’. High team familiarity might increase healthcare workers’ tendency to take over work from each other to unburden colleagues. The results demonstrate the importance of differentiating between predictors for individual and team resilience, considering the research context.
Next to team familiarity, the results show that family support has a positive significant effect on team resilience, meaning that the more family support team members perceive, the more resilient the team will be. In contrast to prior literature [
39], we did not find a positive family support effect on individual resilience. The reason for these findings could be in the context of this study. The COVID-19 pandemic also highly impacted family life. Hall et al. [
7] showed healthcare workers’ primary concerns about their families’ safety in relation to the risks of viral transmission, as well as their high stress attributed to isolation from family and friends. Due to, e.g., quarantine measures, family members might not have been able to deliver the expected mental buffer to express emotions and needs, causing healthcare workers to feel psychologically safe [
24]. Instead, family support seems to have manifested as a different type of resource, providing healthcare workers with the ability and support to take over more workshifts flexibly or work more hours (as also shown in
Table 2), thus enhancing the team’s capacity to overcome work-demand challenges. This research did not show significant results for friend support, which could be the result of isolation from friends during the COVID-19 pandemic, as a consequence of several lockdowns and social distancing. The results show the importance of developing a contextual understanding of how social support can manifest itself in different forms.
The second pathway to enhance team resilience indirectly is by encouraging individual resilience through transformational leadership, and by staffing optimistic team members with high levels of self-efficacy. In line with prior literature [
31], we find a positive, transformational leadership effect on individual resilience, meaning that transformational leaders create a safe and trustful environment which enhances the resilience of their team members [
24,
30]. Nonetheless, the individual merits of transformational leadership translate into only a weak indirect effect on team resilience. Explanations for the findings may be found in the leaders’ large span of control, which limits their ability to perform leadership tasks or even address the team as a whole [
50], and in the great pressure caused by the COVID-19 pandemic, with shortages of staff and beds for COVID-19 patients [
37], precluding leaders from their duties to instead help in patient care. “The emergency department has 65 nurses, for which there are four team leaders (working supervisors). On top of that, employees work in 24 h shifts, so it is even possible that they do not physically see their leader for two weeks” (expert interview). Given these challenging circumstances, including quarantine measures that curtail social support from family and friends, transformational leaders seem to have prioritized devoting attention to the mental health and wellbeing of individual team members and creating a psychological safe environment, but leaving team resilience to the team. The findings demonstrate the importance of research on priority setting by leaders in crisis situations.
Furthermore, our results show that optimism and self-efficacy have a positive effect on individual resilience. These findings corroborate previous studies claiming that psychological characteristics such as optimism and self-efficacy can enhance the resilience of individuals [
31,
38,
51], because individuals who are optimistic and express self-efficacy are more likely to feel psychologically safe [
24], to be goal oriented, to succeed in handling difficult situations, and to believe in themselves, than those who have less of these characteristics [
52,
53,
54].
In sum, the study demonstrates the importance of examining individual resilience and team resilience as distinct constructs with separate predictors, and the interplay between the two constructs is limited.
4.1. Practical Implications
This study reveals several practical implications for managers who, at times of crisis, want to ensure the continuity of care and service delivery and simultaneously strive to safeguard the health and wellbeing of their employees. The findings are acquired in the context of emergency healthcare at the time of the COVID-19 pandemic but may be informative for other situations as well. The ability to bounce back from adversity, either as an individual or as team, are two distinct, loosely coupled capacities. Of course, both individual and team resilience are of importance for well-functioning organizations, but enhancing the former is hardly sufficient to increase the latter, while direct team-level interventions are available. Accordingly, organizations in pursuit of interventions that enhance individual and team resilience could best opt for an intervention portfolio for both the short-term as well as the long-term. The suggestions on interventions for both pathways are described in more detail below.
First, organizations can encourage team resilience directly by enhancing team familiarity and mobilizing family support (pathway one). Organizations could make sure that familiar teams stay together and become increasingly familiar with each other. However, when mixing up teams seems necessary, one should consider investing in time-efficient interventions to familiarize team members with each other in urgent situations with great shortages in staff. Advised interventions, as part of daily operations, are stand-up meetings and hot debriefings [
55] and considering team familiarity when forecasting work schedules (balancing stability and flexibility). These examples are time efficient and effective techniques to enhance team familiarity in the context of emergency healthcare. Additionally, interventions can be conducted in ‘off the job’ training, by investing in getting to know each other’s strengths, weaknesses, preferences, and styles.
Second, to enhance team resilience by family support, organizations should think about policies to stimulate and facilitate the work–life balance of healthcare workers. This social support aids employees with the necessary resources to cope with and recover from stressful events [
38]. Hospitals have asked much of their healthcare workers. Post pandemic, and with considerable elective healthcare to catch up on, policy makers and organizations should question the pressure they put upon healthcare workers and their work–life balance, and therefore, the support they can receive.
Third, our study shows that transformational leadership, self-efficacy, and optimism help increase individual resilience, which to a limited extent also makes teams more resilient. The findings of pathway two also offer areas of intervention for organizations. Leaders should be aware that a transformational leadership style contributes to the resilience of their team members, and should draw attention to times when challenges have been overcome, and stimulate individuals to communicate with each other and jointly think about how to overcome new challenges. In order to do so, leaders should be visible and ensure that concerns have been heard, and provide support to reduce concerns as much as possible.
Fourth, organizations can also incorporate interventions with regards to employees’ optimism and self-efficacy. Hiring or forming teams with optimistic people with high self-efficacy benefits the organization by ensuring employee mental wellbeing, without denying that employees who have less of these characteristics can be an asset to the organization for many other reasons. It is also advised to be aware of colleagues who lack or have lower degrees of optimism or self-efficacy since these employees might be more prone to stress, and therefore, organizations should pay more attention to these individuals. Indeed, for this latter group of employees in particular, transformational leaders can make a difference.
4.2. Limitations and Future Research
Several limitations of this study must be considered. First, data were collected at one hospital in the Netherlands. Although significant results were found and the relative amounts of COVID-19 patients and working methods were comparable in other hospitals during the data collection, future research with larger sample sizes and in different contexts is needed to explore the generalizability of the results. A second limitation concerns the subjective measurements of the variables, as the respondents were asked to assess themselves and their team. Although this approach comes with benefits, such as individuals knowing more about themselves than others might be aware of [
56], particularly when it concerns topics such as their own resilience, self-assessment also comes with disadvantages. One potential issue is that of “common method bias”. However, the common latent factor method showed no such bias. Third, although efforts have been made in maximizing the validity of the study in relation to our operationalization and measurement, we adopted validated English questionnaires and translated and administered them in Dutch. We, therefore, did not use earlier validated scales of our variables in the Dutch language. Finally, although we insinuated causality between our variables, a cross-sectional design does not allow us to examine causal direction. Future research using experimental or longitudinal design is recommended to gain more insight on the relationships between the studied constructs.
For future research, we suggest the following directions. First, this study applies a capacity perspective on resilience, rather than resilience as a personality trait or process. Other resilience perspectives also require future research attention. For example, the process perspective of structuring feedback and adaptation [
14] offers fruitful avenues for future research, which might result in relevant organizational design interventions for management. Moreover, we specified our conceptual model based on careful literature review and context assessment, but some of the literature does mention other potentially relevant constructs. For example, since the COVID-19 pandemic affected the entire hospital, it could be interesting to study resilience at the organizational level to explore the capacity of a hospital to bounce back and recover from an impactful event. Future research is needed to gain a more comprehensive understanding of individual, team, and organizational resilience as a capacity, process, or trait.
Second, team familiarity was shown to be an important predictor of team resilience but did not necessarily make individuals more resilient. As mentioned earlier, the emergency healthcare context within this study has been characterized by a lack of slack resources, with work that cannot be postponed. It remains unclear if in a context rich in slack resources, team familiarity leads to higher levels of individual resilience. It is recommended to examine under which conditions team familiarity does or does not increase individual and team resilience. Moreover, it is debatable whether extra capacity of new and unknown team members always adds up to benefits for the team, with team familiarity in mind. It is recommended that future research examine whether mixing up teams, or keeping teams together, results in better employee outcomes, including factors such as job satisfaction and absenteeism, and/or better patient outcomes, including factors such as the quality of treatment, survival rates, and satisfaction.
Third, family support seems to have manifested as a different type of resource as expected; not as a buffer for mental health but as a type of support providing individuals with the ability to take over work shifts flexibly or work more hours. Future research could be performed to explore the mechanisms of family support in this context, fulfilling mental support on the one hand, and supporting choices like flexibility in employability on the other hand.
Fourth, due to the exceptional pandemic context and given the role of the (transformational) leader, a fruitful research avenue to explore is whether healthcare workers found mental support at work with their leaders, and to what extent and how this affected resilience. Moreover, as the large span of control of a transformational leader could have been a plausible explanation for the weak indirect effect on team resilience, it is recommended to further examine the effect of the span of control of a leader in relation to the effect on team resilience.
Fifth and finally, this study used the GLT questionnaire consisting of seven transformational leadership behaviors. Future research could explore if certain behaviors have a large influence on team resilience, and create an understanding of why this is the case.








{kind=link}