
The Effect of Core Exercise Using Online Videoconferencing Platform and Offline-Based Intervention in Postpartum Woman with Diastasis Recti Abdominis


Abstract
:1. Introduction
2. Materials and Methods
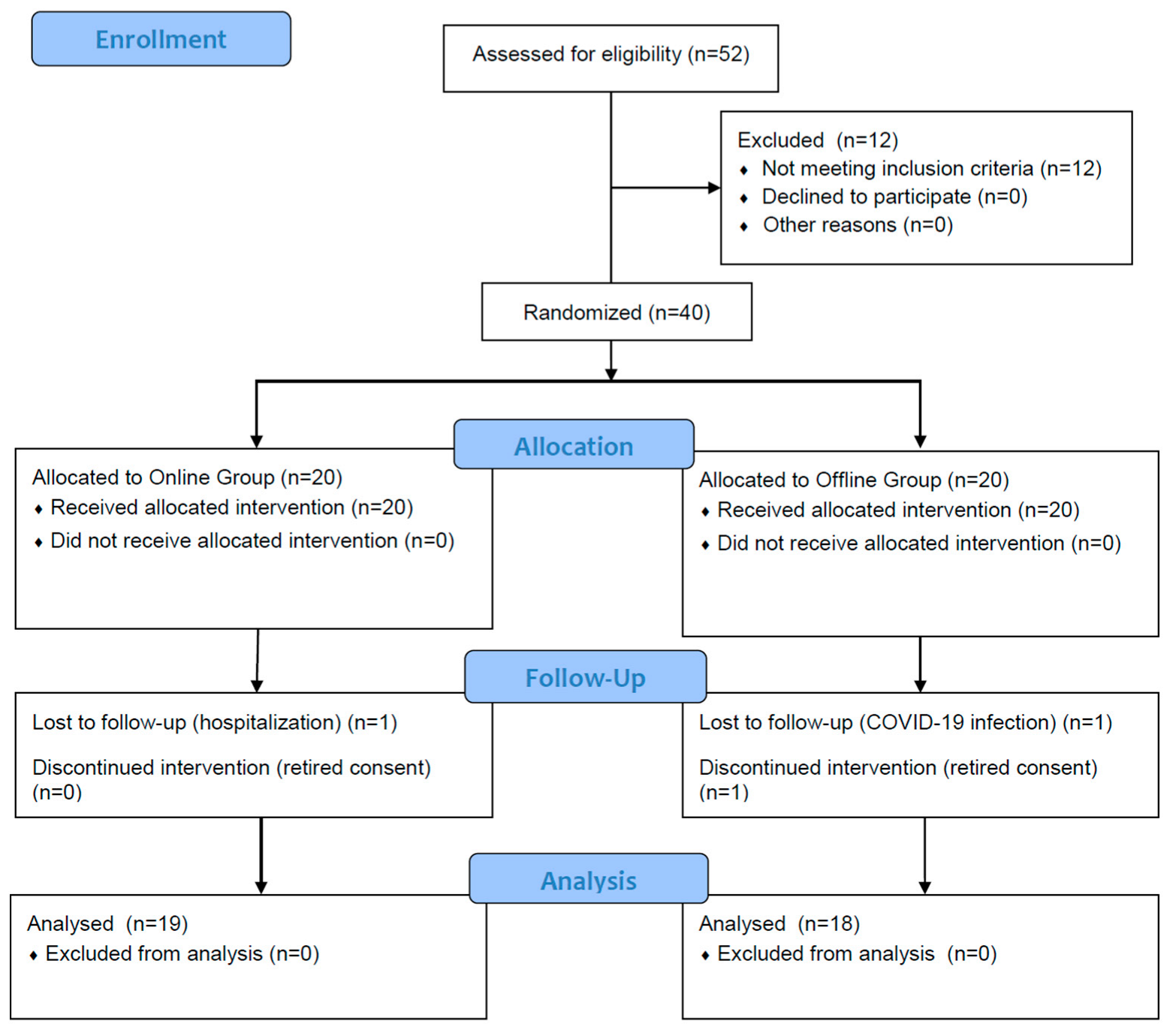
2.1. Study Design
2.2. Participants
2.3. Procedures
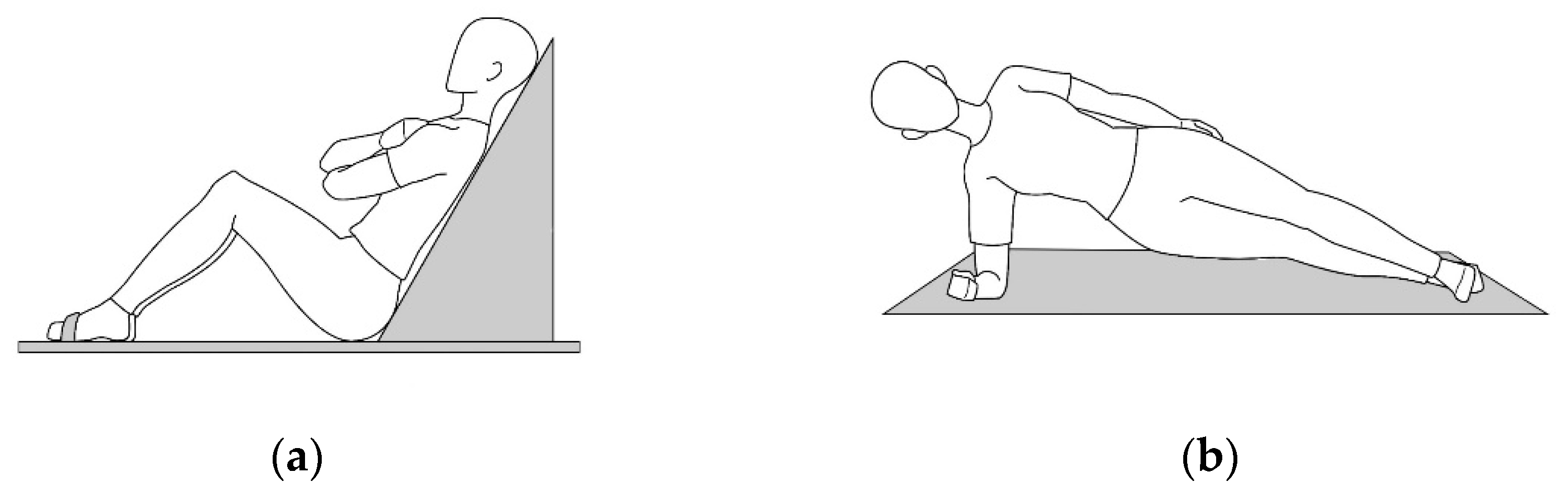
2.3.1. Intervention Protocol
2.3.2. Ultrasound Imaging
2.3.3. Static Trunk Endurance Test
2.3.4. Maternal Quality of Life
2.4. Statistical Analysis
3. Results
3.1. Participants Characteristics
3.2. Inter-Recti Distance
3.3. Muscle Thickness
3.4. Static Trunk Endurance
3.5. Maternal Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nahabedian, M.Y. Management Strategies for Diastasis Recti; Thieme Medical Publishers: New York, NY, USA, 2018; Volume 32, pp. 147–154. [Google Scholar]
- Benjamin, D.; Van de Water, A.; Peiris, C. Effects of exercise on diastasis of the rectus abdominis muscle in the antenatal and postnatal periods: A systematic review. Physiotherapy 2014, 100, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Mota, P.G.F.; Pascoal, A.G.B.A.; Carita, A.I.A.D.; Bø, K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man. Ther. 2015, 20, 200–205. [Google Scholar] [CrossRef] [Green Version]
- Keeler, J.; Albrecht, M.; Eberhardt, L.; Horn, L.; Donnelly, C.; Lowe, D. Diastasis Recti Abdominis. J. Womens Health Phys. Therap. 2012, 36, 131–142. [Google Scholar] [CrossRef]
- Verissimo, P.; Nahas, F.X.; Barbosa, M.V.; de Carvalho Gomes, H.F.; Ferreira, L.M. Is it possible to repair diastasis recti and shorten the aponeurosis at the same time? Aesthetic Plast. Surg. 2014, 38, 379–386. [Google Scholar] [CrossRef] [PubMed]
- Emanuelsson, P.; Gunnarsson, U.; Strigård, K.; Stark, B. Early complications, pain, and quality of life after reconstructive surgery for abdominal rectus muscle diastasis: A 3-month follow-up. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 1082–1088. [Google Scholar] [CrossRef] [Green Version]
- Litos, K. Progressive therapeutic exercise program for successful treatment of a postpartum woman with a severe diastasis recti abdominis. J. Womens Health Phys. Ther. 2014, 38, 58–73. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.G.; Lee, L.J.; McLaughlin, L. Stability, continence and breathing: The role of fascia following pregnancy and delivery. J. Bodyw. Mov. Ther. 2008, 12, 333–348. [Google Scholar] [CrossRef]
- Danneels, L.A.; Vanderstraeten, G.G.; Cambier, D.C.; Witvrouw, E.E.; Stevens, V.K.; De Cuyper, H.J. A functional subdivision of hip, abdominal, and back muscles during asymmetric lifting. Spine 2001, 26, E114–E121. [Google Scholar] [CrossRef]
- El-Rich, M.; Shirazi-Adl, A.; Arjmand, N. Muscle activity, internal loads, and stability of the human spine in standing postures: Combined model and in vivo studies. Spine 2004, 29, 2633–2642. [Google Scholar] [CrossRef]
- Sitilertpisan, P.; Pirunsan, U.; Puangmali, A.; Ratanapinunchai, J.; Kiatwattanacharoen, S.; Neamin, H.; Laskin, J.J. Comparison of lateral abdominal muscle thickness between weightlifters and matched controls. Phys. Ther. Sport 2011, 12, 171–174. [Google Scholar] [CrossRef]
- Fast, A.; Shapiro, D.; Ducommun, E.J.; Friedmann, L.W.; Bouklas, T.; Floman, Y. Low-back pain in pregnancy. Spine 1987, 12, 368–371. [Google Scholar] [CrossRef]
- Wilhelmsson, S.; Fagevik Olsen, M.; Staalesen, T.; Elander, A.; Nygren-Bonnier, M. Abdominal plasty with and without plication-effects on trunk muscles, lung function, and self-rated physical function. J. Plast. Surg. Hand Surg. 2017, 51, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Acharry, N.; Kutty, R.K. Abdominal Exercise with Bracing, a Therapeutic Efficacy in Reducing Diastasis-Recti among Postpartal Females. Int. J. Physiother. Res. 2015, 3, 999–1005. [Google Scholar] [CrossRef]
- Poyatos-Leon, R.; Garcia-Hermoso, A.; Sanabria-Martinez, G.; Alvarez-Bueno, C.; Cavero-Redondo, I.; Martinez-Vizcaino, V. Effects of exercise-based interventions on postpartum depression: A meta-analysis of randomized controlled trials. Birth 2017, 44, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Sampselle, C.M.; Seng, J.; Yeo, S.; Killion, C.; Oakley, D. Physical activity and postpartum well-being. J. Obstet. Gynecol. Neonatal Nurs. 1999, 28, 41–49. [Google Scholar] [CrossRef]
- Pruett, M.D.; Caputo, J.L. Exercise guidelines for pregnant and postpartum women. Strength Cond. J. 2011, 33, 100–103. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19): Weekly Epidemiological Update; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Rosen, M.J. Telerehabilitation. NeuroRehabilitation 1999, 12, 11–26. [Google Scholar] [CrossRef]
- Azma, K.; RezaSoltani, Z.; Rezaeimoghaddam, F.; Dadarkhah, A.; Mohsenolhosseini, S. Efficacy of tele-rehabilitation compared with office-based physical therapy in patients with knee osteoarthritis: A randomized clinical trial. J. Telemed. Telecare 2018, 24, 560–565. [Google Scholar] [CrossRef]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The role of telehealth in reducing the mental health burden from COVID-19. Telemed. J. e-Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Hong, J.; Kim, J.; Kim, S.W.; Kong, H.J. Effects of home-based tele-exercise on sarcopenia among community-dwelling elderly adults: Body composition and functional fitness. Exp. Gerontol. 2017, 87, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Marshall, C.J.; Dobson, F.; Kasza, J.; Lonsdale, C.; Hinman, R.S. Does a Web-Based Exercise Programming System Improve Home Exercise Adherence for People with Musculoskeletal Conditions?: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2019, 98, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Tsai, L.L.Y.; McNamara, R.J.; Dennis, S.M.; Moddel, C.; Alison, J.A.; McKenzie, D.K.; McKeough, Z.J. Satisfaction and experience with a supervised home-based real-time videoconferencing telerehabilitation exercise program in people with chronic obstructive pulmonary disease (COPD). Int. J. Telerehabil. 2016, 8, 27. [Google Scholar] [CrossRef] [PubMed]
- Bursch, S.G. Interrater reliability of diastasis recti abdominis measurement. Phys. Ther. 1987, 67, 1077–1079. [Google Scholar] [CrossRef] [PubMed]
- Artal, R.; O’Toole, M. Guidelines of the American College of Obstetricians and Gynecologists for exercise during pregnancy and the postpartum period. Br. J. Sports Med. 2003, 37, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akuthota, V.; Ferreiro, A.; Moore, T.; Fredericson, M. Core stability exercise principles. Curr. Sports Med. Rep. 2008, 7, 39–44. [Google Scholar] [CrossRef]
- Cadore, E.; González-Izal, M.; Pallarés, J.; Rodriguez-Falces, J.; Häkkinen, K.; Kraemer, W.; Pinto, R.; Izquierdo, M. Muscle conduction velocity, strength, neural activity, and morphological changes after eccentric and concentric training. Scand. J. Med. Sci. Sports 2014, 24, e343–e352. [Google Scholar] [CrossRef]
- Whittaker, J.L.; Teyhen, D.S.; Elliott, J.M.; Cook, K.; Langevin, H.M.; Dahl, H.H.; Stokes, M. Rehabilitative ultrasound imaging: Understanding the technology and its applications. J. Orthop. Sports Phys. Ther. 2007, 37, 434–449. [Google Scholar] [CrossRef]
- Misuri, G.; Colagrande, S.; Gorini, M.; Iandelli, I.; Mancini, M.; Duranti, R.; Scano, G. In vivo ultrasound assessment of respiratory function of abdominal muscles in normal subjects. Eur. Respir. J. 1997, 10, 2861–2867. [Google Scholar] [CrossRef] [Green Version]
- Hides, J.A.; Miokovic, T.; Belavy, D.L.; Stanton, W.R.; Richardson, C.A. Ultrasound imaging assessment of abdominal muscle function during drawing-in of the abdominal wall: An intrarater reliability study. J. Orthop. Sports Phys. Ther. 2007, 37, 480–486. [Google Scholar] [CrossRef] [Green Version]
- Thabet, A.A.; Alshehri, M.A. Efficacy of deep core stability exercise program in postpartum women with diastasis recti abdominis: A randomised controlled trial. J. Musculoskelet. Neuronal Interact. 2019, 19, 62. [Google Scholar] [PubMed]
- Stuge, B.; Lærum, E.; Kirkesola, G.; Vøllestad, N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: A randomized controlled trial. Spine 2004, 29, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Tanvi, A.; Shalini, G.; Parul, R.; Gaurav, S. Effect of proprioceptive neuromuscular facilitation program on muscle endurance, strength, pain, and functional performance in women with post-partum lumbo-pelvic pain. IOSR J. Dent. Med. Sci. 2013, 7, 60–67. [Google Scholar]
- Carrick-Ranson, G.; Sloane, N.M.; Howden, E.J.; Bhella, P.S.; Sarma, S.; Shibata, S.; Fujimoto, N.; Hastings, J.L.; Levine, B.D. The effect of lifelong endurance exercise on cardiovascular structure and exercise function in women. J. Physiol. 2020, 598, 2589–2605. [Google Scholar] [CrossRef] [PubMed]
- Aarts, H.; Paulussen, T.; Schaalma, H. Physical exercise habit: On the conceptualization and formation of habitual health behaviours. Health Educ. Res. 1997, 12, 363–374. [Google Scholar] [CrossRef] [Green Version]
- Daley, A. Exercise and depression: A review of reviews. J. Clin. Psychol. Med. Settings 2008, 15, 140. [Google Scholar] [CrossRef]
- Darbandi, S.; Darbandi, M.; Khorshid, H.R.K.; Sadeghi, M.R. Yoga can improve assisted reproduction technology outcomes in couples with infertility. Reprod. Health 2018, 1, 2. [Google Scholar]
- Wallace, J.; Raglin, J.; Jastremski, C. Twelve month adherence of adults who joined a fitness program with a spouse vs without a spouse. J. Sports Med. Phys. Fitness 1995, 35, 206–213. [Google Scholar]
- Jarvis-Selinger, S.; Chan, E.; Payne, R.; Plohman, K.; Ho, K. Clinical telehealth across the disciplines: Lessons learned. Telemed. J. e-Health 2008, 14, 720–725. [Google Scholar] [CrossRef]
- Peng, X.; Su, Y.; Hu, Z.; Sun, X.; Li, X.; Dolansky, M.A.; Qu, M.; Hu, X. Home-based telehealth exercise training program in Chinese patients with heart failure: A randomized controlled trial. Medicine 2018, 97, e12069. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Online Group (n = 19) | Offline Group (n = 18) | t (p) | ||
|---|---|---|---|---|
| Age | (year) | 31.68 ± 3.92 | 32.72 ± 2.54 | −0.951 (0.348) |
| Height | (cm) | 163.19 ± 4.87 | 161.65 ± 6.85 | 0.791 (0.434) |
| Weight | (kg) | 58.74 ± 6.80 | 59.56 ± 6.57 | −0.370 (0.714) |
| BMI | (kg/m²) | 21.97 ± 1.87 | 22.78 ± 1.95 | −1.284 (0.208) |
| Birth Weight | (kg) | 3.11 ± 0.43 | 3.07 ± 0.42 | 0.309 (0.759) |
| Delivery type | ||||
| Vaginal | N (%) | 9 (24%) | 6 (16%) | |
| Cesarean | 10 (27%) | 12 (32%) | ||
| Location | Online Group (n = 19) | Offline Group (n = 18) | t (p) | |
|---|---|---|---|---|
| 2.5 cm above umbilicus | Pre-test | 1.99 ± 0.26 | 1.92 ± 0.30 | |
| Post-test | 1.37 ± 0.40 | 1.18 ± 0.30 | ||
| Difference | −0.62 ± 0.27 | −0.74 ± 0.23 | 1.471 (0.150) | |
| t (p) | 10.143 (0.000) | 13.745 (0.000) |
| Online Group (n = 19) | Offline Group (n = 18) | t (p) | ||
|---|---|---|---|---|
| EO | Pre-test | 0.33 ± 0.04 | 0.34 ± 0.04 | |
| Post-test | 0.36 ± 0.04 | 0.38 ± 0.03 | ||
| Difference | 0.03 ± 0.02 | 0.04 ± 0.02 | −0.637 (0.528) | |
| t (p) | 6.245 (0.000) | 8.030 (0.000) | ||
| IO | Pre-test | 0.54 ± 0.06 | 0.51 ± 0.05 | |
| Post-test | 0.61 ± 0.07 | 0.60 ± 0.06 | ||
| Difference | 0.06 ± 0.03 | 0.08 ± 0.04 | −1.295 (0.204) | |
| t (p) | 8.182 (0.000) | 8.517 (0.000) | ||
| TrA | Pre-test | 0.31 ± 0.02 | 0.33 ± 0.03 | |
| Post-test | 0.35 ± 0.03 | 0.37 ± 0.03 | ||
| Difference | 0.04 ± 0.03 | 0.04 ± 0.02 | −0.805 (0.426) | |
| t (p) | 6.067 (0.000) | 8.271 (0.000) | ||
| RA (Left) | Pre-test | 0.74 ± 0.06 | 0.77 ± 0.06 | |
| Post-test | 0.84 ± 0.05 | 0.89 ± 0.07 | ||
| Difference | 0.08 ± 0.03 | 0.11 ± 0.05 | −2.599 (0.014) | |
| t (p) | 11.071 (0.000) | 10.614 (0.000) | ||
| RA (Right) | Pre-test | 0.71 ± 0.07 | 0.76 ± 0.07 | |
| Post-test | 0.83 ± 0.06 | 0.89 ± 0.06 | ||
| Difference | 0.11 ± 0.04 | 0.13 ± 0.04 | −1.017 (0.316) | |
| t (p) | 11.444 (0.000) | 14.577 (0.000) | ||
| Online Group (n = 19) | Offline Group (n = 18) | t (p) | ||
|---|---|---|---|---|
| Trunk Flexor | Pre-test | 97.71 ± 35.05 | 106.08 ± 39.75 | |
| Post-test | 113.40 ± 34.91 | 123.81 ± 37.69 | ||
| Difference | 15.69 ± 6.92 | 17.73 ± 8.86 | −0.782 (0.439) | |
| t (p) | 9.883 (0.000) | 8.491 (0.000) | ||
| Left Side Bridge | Pre-test | 29.15 ± 12.11 | 32.00 ± 13.25 | |
| Post-test | 34.83 ± 11.09 | 40.88 ± 12.49 | ||
| Difference | 5.68 ± 5.51 | 8.88 ± 5.50 | −1.770 (0.085) | |
| t (p) | 4.492 (0.001) | 6.856 (0.000) | ||
| Right Side Bridge | Pre-test | 30.83 ± 10.92 | 34.38 ± 14.85 | |
| Post-test | 37.35 ± 11.00 | 45.61 ± 13.68 | ||
| Difference | 6.52 ± 6.85 | 11.23 ± 5.63 | −2.278 (0.029) | |
| t (p) | 4.147 (0.001) | 8.470 (0.000) |
| Online Group (n = 19) | Offline Group (n = 18) | t (p) | ||
|---|---|---|---|---|
| Psychological/Baby | Pre-test | 19.07 ± 2.68 | 17.80 ± 2.12 | |
| Post-test | 22.74 ± 2.18 | 19.53 ± 2.46 | ||
| Difference | 3.66 ± 2.49 | 1.73 ± 2.43 | 2.359 (0.024) | |
| t (p) | 6.253 (0.000) | 3.031 (0.008) | ||
| Socioeconomic | Pre-test | 21.04 ± 3.91 | 20.16 ± 1.75 | |
| Post-test | 22.71 ± 2.85 | 21.33 ± 1.97 | ||
| Difference | 1.67 ± 1.77 | 1.18 ± 1.72 | 0.844 (0.405) | |
| t (p) | 3.996 (0.001) | 2.902 (0.010) | ||
| Relational/Spouse Partner | Pre-test | 20.20 ± 3.59 | 20.10 ± 2.08 | |
| Post-test | 23.16 ± 3.23 | 20.94 ± 3.31 | ||
| Difference | 2.96 ± 2.72 | 0.84 ± 3.14 | 2.163 (0.038) | |
| t (p) | 4.610 (0.000) | 1.136 (0.272) | ||
| Relational/Family-Friends | Pre-test | 19.20 ± 2.34 | 18.80 ± 2.57 | |
| Post-test | 19.91 ± 2.25 | 19.76 ± 1.62 | ||
| Difference | 0.69 ± 2.03 | 0.96 ± 1.73 | −0.416 (0.680) | |
| t (p) | 1.445 (0.167) | 2.343 (0.032) | ||
| Health & Functioning | Pre-test | 17.71 ± 2.34 | 17.94 ± 2.46 | |
| Post-test | 20.79 ± 1.96 | 21.49 ± 1.77 | ||
| Difference | 3.08 ± 2.65 | 3.55 ± 1.82 | −0.614 (0.544) | |
| t (p) | 4.935 (0.000) | 8.259 (0.000) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Yi, D.; Yim, J. The Effect of Core Exercise Using Online Videoconferencing Platform and Offline-Based Intervention in Postpartum Woman with Diastasis Recti Abdominis. Int. J. Environ. Res. Public Health 2022, 19, 7031. https://doi.org/10.3390/ijerph19127031
Kim S, Yi D, Yim J. The Effect of Core Exercise Using Online Videoconferencing Platform and Offline-Based Intervention in Postpartum Woman with Diastasis Recti Abdominis. International Journal of Environmental Research and Public Health. 2022; 19(12):7031. https://doi.org/10.3390/ijerph19127031
Chicago/Turabian StyleKim, Seohee, Donghyun Yi, and Jongeun Yim. 2022. "The Effect of Core Exercise Using Online Videoconferencing Platform and Offline-Based Intervention in Postpartum Woman with Diastasis Recti Abdominis" International Journal of Environmental Research and Public Health 19, no. 12: 7031. https://doi.org/10.3390/ijerph19127031