Effect of Transcranial Pulsed Current Stimulation on Fatigue Delay after Medium-Intensity Training



Abstract
:1. Introduction
2. Participants and Methods
2.1. Ethics
2.2. Participants
2.3. Study Design
2.4. Experiment Flow
2.5. Training Protocols
2.6. Experimental Equipment
2.6.1. Transcranial Pulsed Current Stimulation
2.6.2. HRV Test
2.6.3. Blood Collection
2.6.4. Questionnaire for Rated Perceived Exertion (RPE)
2.7. Physiological State Index Test
2.8. Sample Size and Randomization
2.9. Data Processing and Analysis
3. Results
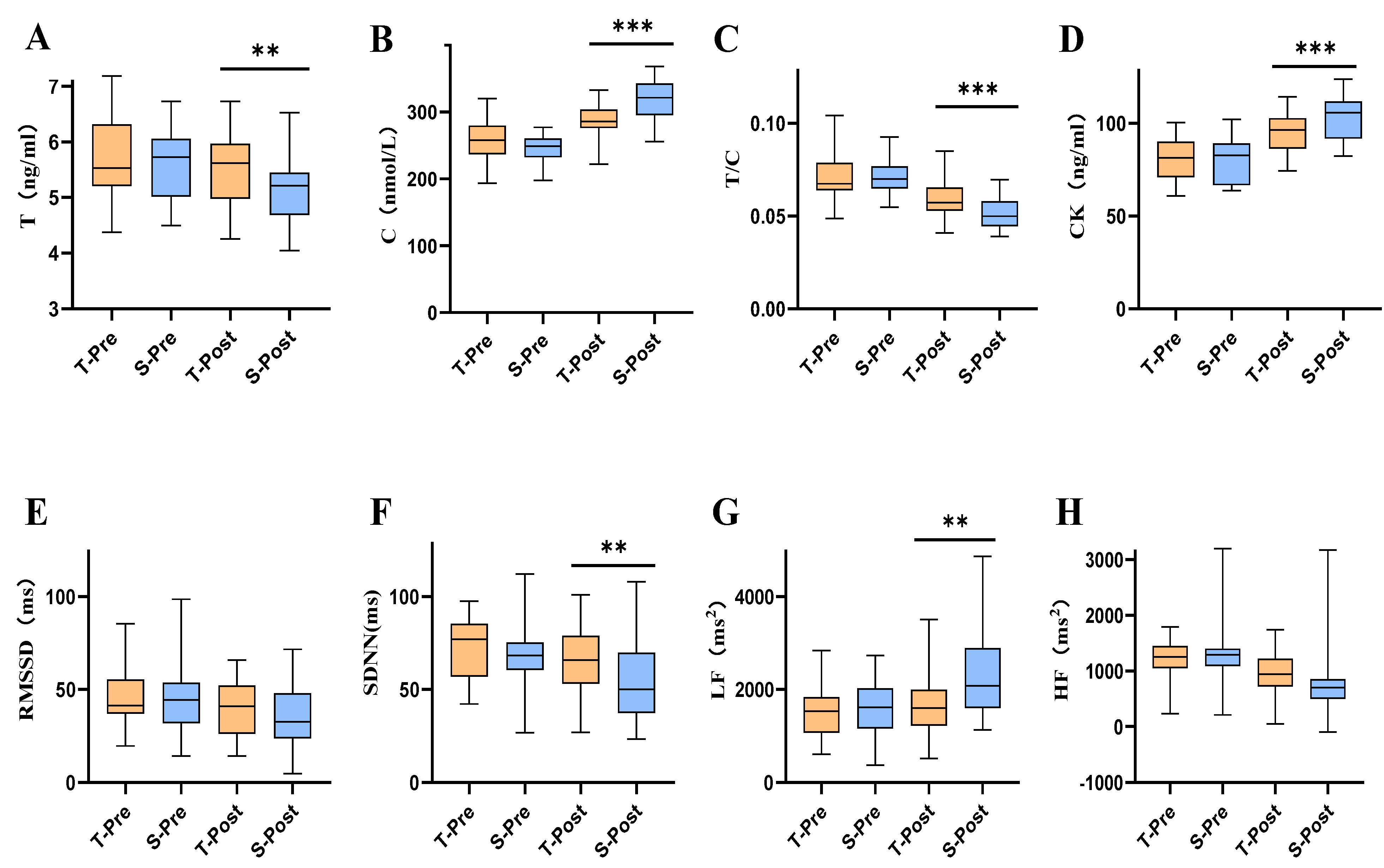
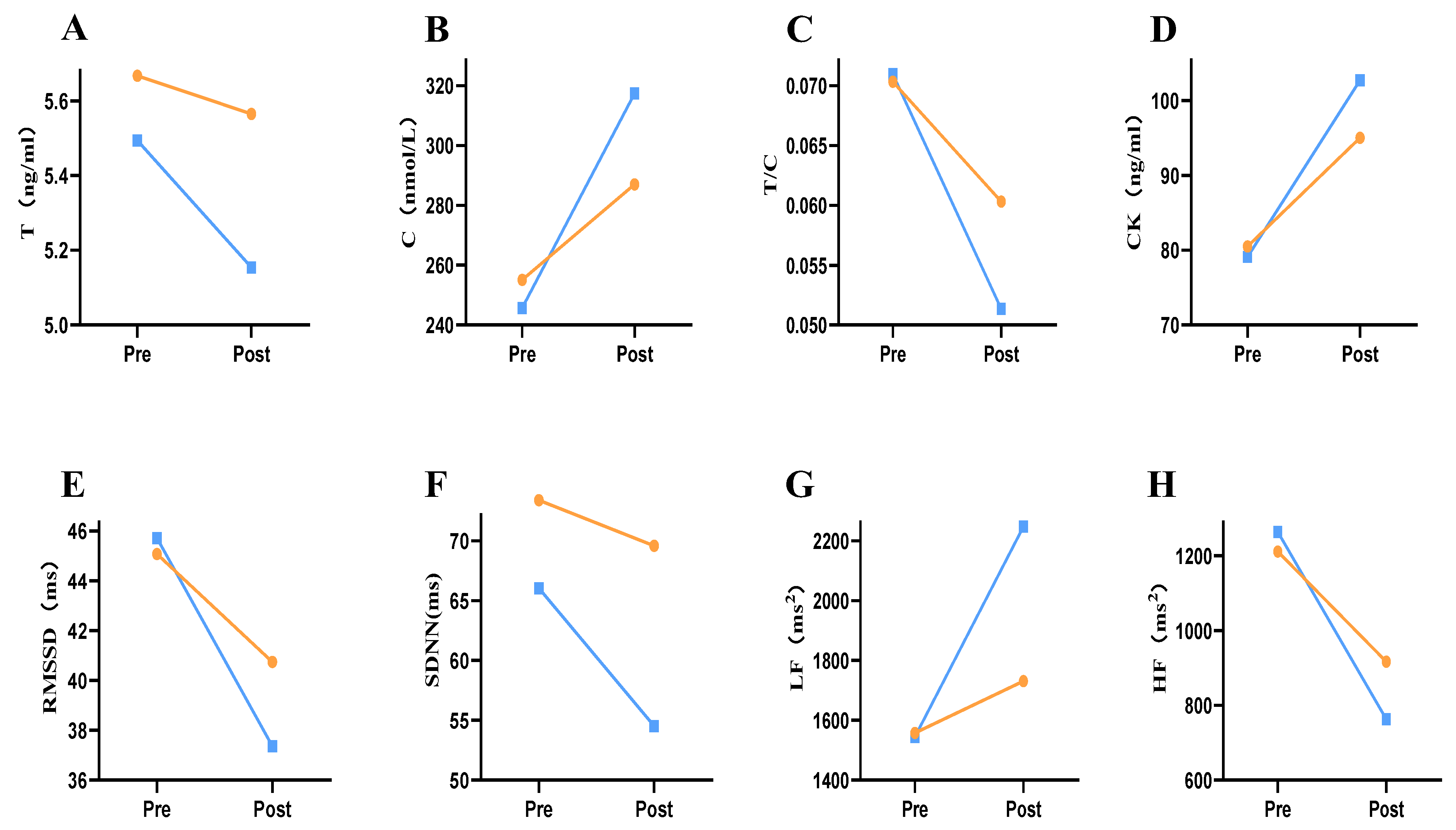
3.1. Changes in Blood Marker Indicators after tPCS Intervention
3.2. Changes in HRV Indicators after tPCS Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Anderson, T.; Lane, A.R.; Hackney, A.C. Cortisol and testosterone dynamics following exhaustive endurance exercise. Eur. J. Appl. Physiol. 2016, 116, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Vitor-Costa, M.; Okuno, N.M.; Bortolotti, H.; Bertollo, M.; Boggio, P.S.; Fregni, F.; Altimari, L.R. Improving cycling performance: Transcranial direct current stimulation increases time to exhaustion in cycling. PLoS ONE 2015, 10, e144916. [Google Scholar] [CrossRef] [PubMed]
- Colzato, L.S.; Nitsche, M.A.; Kibele, A. Noninvasive brain stimulation and neural entrainment enhance athletic performance—A review. J. Cogn. Enhanc. 2017, 1, 73–79. [Google Scholar] [CrossRef]
- Edwards, D.J.; Cortes, M.; Wortman-Jutt, S.; Putrino, D.; Bikson, M.; Thickbroom, G.; Pascual-Leone, A. Transcranial direct current stimulation and sports performance. Front. Hum. Neurosci. 2017, 11, 243. [Google Scholar] [CrossRef] [PubMed]
- Friehs, M.A.; Whelan, E.; Güldenpenning, I.; Krause, D.; Weigelt, M. Stimulating performance: A scoping review on transcranial electrical stimulation effects on olympic sports. Psychol. Sport Exerc. 2021, 59, 102130. [Google Scholar] [CrossRef]
- Cogiamanian, F.; Marceglia, S.; Ardolino, G.; Barbieri, S.; Priori, A. Improved isometric force endurance after transcranial direct current stimulation over the human motor cortical areas. Eur. J. Neurosci. 2007, 26, 242–249. [Google Scholar] [CrossRef]
- Donati, F.; Sian, V.; Biasini, G.M.; da laTorre, X.; Folchitto, F.; Botrè, F. Serum Levels of Brain-Derived Neurotrophic Factor and Other Neurotrophins in Elite Athletes: Potential Markers of the Use of Transcranial Direct Current Stimulation in Sport. Front. Sports Act. Living 2021, 3, 80. [Google Scholar] [CrossRef]
- Park, S.B.; Sung, D.J.; Kim, B.; Kim, S.; Han, J.-K. Transcranial direct current stimulation of motor cortex enhances running performance. PLoS ONE 2019, 14, e0211902. [Google Scholar] [CrossRef]
- Enoka, R.M.; Stuart, D.G. Neurobiology of muscle fatigue. J. Appl. Physiol. 1992, 72, 1631–1648. [Google Scholar] [CrossRef]
- Ma, Z.; Du, X.; Wang, F.; Ding, R.; Li, Y.; Liu, A.; Wei, L.; Hou, S.; Chen, F.; Hu, Q.; et al. Cortical Plasticity Induced by Anodal Transcranial Pulsed Current Stimulation Investigated by Combining Two-Photon Imaging and Electrophysiological Recording. Front. Cell Neurosci. 2019, 13, 400. [Google Scholar] [CrossRef]
- Datta, A.; Dmochowski, J.P.; Guleyupoglu, B.; Bikson, M.; Fregni, F. Cranial electrotherapy stimulation and transcranial pulsed current stimulation: A computer based high-resolution modeling study. Neuroimage 2013, 65, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Jaberzadeh, S.; Bastani, A.; Zoghi, M. Anodal transcranial pulsed current stimulation: A novel technique to enhance corticospinal excitability. Clin. Neurophysiol. 2014, 125, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, A.; Malavera, A.; Doruk, D.; Morales-Quezada, L.; Carvalho, S.; Leite, J.; Fregni, F. Duration dependent effects of transcranial pulsed current stimulation (tPCS) indexed by electroencephalography. Neuromodul. Technol. Neural Interface 2016, 19, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Dissanayaka, T.; Zoghi, M.; Farrell, M.; Egan, G.; Jaberzadeh, S. The Effects of Monophasic Anodal Transcranial Pulsed Current Stimulation on Corticospinal Excitability and Motor Performance in Healthy Young Adults: A Randomized Double-Blinded Sham-Controlled Study. Brain Connect. 2022, 12, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Morales-Quezada, L.; Cosmo, C.; Carvalho, S.; Leite, J.; Castillo-Saavedra, L.; Rozisky, J.R.; Fregni, F. Cognitive effects and autonomic responses to transcranial pulsed current stimulation. Exp. Brain Res. 2015, 233, 701–709. [Google Scholar] [CrossRef] [PubMed]
- McIntire, L.K.; McKinley, R.A.; Nelson, J.M.; Goodyear, C. Transcranial direct current stimulation versus caffeine as a fatigue countermeasure. Brain Stimul. 2017, 10, 1070–1078. [Google Scholar] [CrossRef]
- Muthalib, M.; Kan, B.; Nosaka, K.; Perrey, S. Effects of Transcranial Direct Current Stimulation of the Motor Cortex on Prefrontal Cortex Activation during a Neuromuscular Fatigue Task: An fNIRS Study[M]//Oxygen Transport to Tissue XXXV; Springer: New York, NY, USA, 2013; pp. 73–79. [Google Scholar]
- Hackney, A.C.; Anderson, T.; Dobridge, J. Exercise and Male Hypogonadism: Testosterone, the Hypothalamic-Pituitary-Testicular Axis, and Exercise Training[M]//Male Hypogonadism; Humana Press: Cham, Switzerland, 2017; pp. 257–280. [Google Scholar]
- Brancaccio, P.; Limongelli, F.M.; Maffulli, N. Monitoring of serum enzymes in sport. Br. J. Sports Med. 2006, 40, 96–97. [Google Scholar] [CrossRef]
- Selmi, O.; Ouergui, I.; Levitt, E.D.; Marzouki, H.; Knechtle, B.; Nikolaidis, P.T.; Bouassida, A. Training, psychometric status, biological markers and neuromuscular fatigue in soccer. Biol. Sport 2022, 39, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Segerstrom, S.C.; Nes, L.S. Heart rate variability reflects self-regulatory strength, effort, and fatigue. Psychol. Sci. 2007, 18, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Vanderhasselt, M.A.; Boggio, P.S.; Fregni, F.; Dantas, E.M.; Mill, J.G.; Lotufo, P.A.; Benseñor, I.M. Polarity-and valence-dependent effects of prefrontal transcranial direct current stimulation on heart rate variability and salivary cortisol. Psychoneuroendocrinology 2013, 38, 58–66. [Google Scholar] [CrossRef]
- Yang, D.; Shin, Y.I.; Hong, K.S. Systemic Review on Transcranial Electrical Stimulation Parameters and EEG/fNIRS Features for Brain Diseases. Front. Neurosci. 2021, 15, 274. [Google Scholar] [CrossRef] [PubMed]
- Antal, A.; Alekseichuk, I.; Bikson, M.; Brockmöller, J.; Brunoni, A.R.; Chen, R.; Cohen, L.G.; Dowthwaite, G.; Ellrich, J.; Flöel, A.; et al. Low intensity transcranial electric stimulation: Safety, ethical, legal regulatory and application guidelines. Clin. Neurophysiol. 2017, 128, 1774–1809. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; American Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Skinner, J.; Hutsler, E.; Bergsteinova, V.; Buskirk, E.R. The validity and reliability of a rating scale of perceived exertion. Med. Sci. Sports 1973, 5, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Stamford, B.A. Validity and reliability of subjective ratings of perceived exertion during work. Ergonomics 1976, 19, 53–60. [Google Scholar] [CrossRef]
- Patel, M.; Lal, S.K.L.; Kavanagh, D.; Rossiter, P. Applying neural network analysis on heart rate variability data to assess driver fatigue. Expert Syst. Appl. 2011, 38, 7235–7242. [Google Scholar] [CrossRef]
- Tabben, M.; Ihsan, M.; Ghoul, N.; Coquart, J.; Chaouachi, A.; Chaabene, H.; Tourny, C.; Chamari, K. Cold Water Immersion Enhanced Athletes’ Wellness and 10-m Short Sprint Performance 24-h After a Simulated Mixed Martial Arts Combat. Front. Physiol. 2018, 9, 1542. [Google Scholar] [CrossRef]
- Young, H.A.; Benton, D. Heart-rate variability: A biomarker to study the influence of nutrition on physiological and psychological health? Behav. Pharmacol. 2018, 29, 140. [Google Scholar] [CrossRef]
- Hecksteden, A.; Skorski, S.; Schwindling, S.; Hammes, D.; Pfeiffer, M.; Kellmann, M.; Ferrauti, A.; Meyer, T. Blood-borne markers of fatigue in competitive athletes–results from simulated training camps. PLoS ONE 2016, 11, e0148810. [Google Scholar] [CrossRef]
- Morales-Quezada, L.; Leite, J.; Carvalho, S.; Castillo-Saavedra, L.; Cosmo, C.; Fregni, F. Behavioral effects of transcranial pulsed current stimulation (tPCS): Speed-accuracy tradeoff in attention switching task. Neurosci. Res. 2016, 109, 48–53. [Google Scholar] [CrossRef]
- Karkoulias, K.; Habeos, I.; Charokopos, N.; Tsiamita, M.; Mazarakis, A.; Pouli, A.; Spiropoulos, K. Hormonal responses to marathon running in non-elite athletes. Eur. J. Int. Med. 2008, 19, 598–601. [Google Scholar] [CrossRef]
- França, S.C.A.; Barros Neto, T.L.; Agresta, M.C.; Lotufo, R.F.M.; Kater, C.E. Divergent responses of serum testosterone and cortisol in athlete men after a marathon race. Arq. Bras. Endocrinol. Metabol. 2006, 50, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Ko, D.H.; Kim, S.E.; Lee, J.Y. Prevalence of Low Testosterone According to Health Behavior in Older Adults Men. Healthcare 2020, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Slivka, D.R.; Hailes, W.S.; Cuddy, J.S.; Ruby, B.C. Effects of 21 days of intensified training on markers of overtraining. J. Strength Cond. Res. 2010, 24, 2604–2612. [Google Scholar] [CrossRef] [PubMed]
- Raastad, T.; Glomsheller, T.; Bjøro, T.; Hallén, J. Changes in human skeletal muscle contractility and hormone status during 2 weeks of heavy strength training. Eur. J. Appl. Physiol. 2001, 84, 54–63. [Google Scholar] [CrossRef]
- Martínez-Montoro, J.I.; Molina-Vega, M.; Asenjo-Plaza, M.; García-Ruiz, M.C.; Varea-Marineto, E.; Plaza-Andrade, I.; Álvarez-Millán, J.J.; Cabezas-Sánchez, P.; Tinahones, F.J.; Fernández-García, J.C. Adiposity is Associated with Decreased Serum 17-Hydroxyprogesterone Levels in Non-Diabetic Obese Men Aged 18–49: A Cross-Sectional Study. J. Clin. Med. 2020, 9, 3873. [Google Scholar] [CrossRef] [PubMed]
- Crewther, B.; Keogh, J.; Cronin, J.; Keogh, J. Possible stimuli for strength and power adaptation. Sports Med. 2006, 36, 215–238. [Google Scholar] [CrossRef]
- Aufegger, L.; Wasley, D. Salivary cortisol and alpha-amylase are modulated by the time and context of musical performance. Int. J. Stress Manag. 2018, 25, 81. [Google Scholar] [CrossRef]
- Peeters, G.; Van Schoor, N.M.; Visser, M.; Knol, D.L.; Eekhoff, E.M.W.; de Ronde, W.; Lips, P. Relationship between cortisol and physical performance in older persons. Clin. Endocrinol. 2007, 67, 398–406. [Google Scholar] [CrossRef]
- Gardner, M.P.; Lightman, S.L.; Gallacher, J.; Hardy, R.; Kuh, D.; Ebrahim, S.; Bayer, A.; Ben-Shlomo, Y.; Halcyon Study Team. Diurnal cortisol patterns are associated with physical performance in the Caerphilly Prospective Study. Int. J. Epidemiol. 2011, 40, 1693–1702. [Google Scholar] [CrossRef]
- Arruda, A.F.; Aoki, M.S.; Freitas, C.G.; Drago, G.; Oliveira, R.; Crewther, B.T.; Moreira, A. Influence of competition playing venue on the hormonal responses, state anxiety and perception of effort in elite basketball athletes. Physiol. Behav. 2014, 130, 1–5. [Google Scholar] [CrossRef]
- Slimani, M.; Cheour, F.; Moalla, W.; Baker, J.S. Hormonal responses to a rugby match: A brief review. J. Sports Med. Phys. Fit 2018, 58, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Souglis, A.; Bogdanis, G.C.; Giannopoulou, I.; Papadopoulos, C.; Apostolidis, N. Comparison of inflammatory responses and muscle damage indices following a soccer, basketball, volleyball and handball game at an elite competitive level. Res. Sports Med. 2015, 23, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Mehrsafar, A.H.; Rosa, M.A.S.; Zadeh, A.M.; Gazerani, P. A feasibility study of application and potential effects of a single session transcranial direct current stimulation (tDCS) on competitive anxiety, mood state, salivary levels of cortisol and alpha amylase in elite athletes under a real-world competition. Physiol. Behav. 2020, 227, 113173. [Google Scholar] [CrossRef] [PubMed]
- Raimundo, R.J.S.; Uribe, C.E.; Brasil-Neto, J.P. Lack of clinically detectable acute changes on autonomic or thermoregulatory functions in healthy subjects after transcranial direct current stimulation (tDCS). Brain Stimul. 2012, 5, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Duarte, I.; Gebodh, N.; Schestatsky, P.; Guleyupoglu, B.; Reato, D.; Bikson, M.; Fregni, F. Transcranial electrical stimulation: Transcranial direct current stimulation (tDCS), transcranial alternating current stimulation (tACS), transcranial pulsed current stimulation (tPCS), and transcranial random noise stimulation (tRNS). In The Stimulated Brain; Elsevier: Amsterdam, The Netherlands, 2014; pp. 35–59. [Google Scholar]
- Feng, F.; Liu, Y. Monitoring of some biochemical indexes of classical young wrestlers during high-intensity training. J. Shanghai Inst. Phys. Educ. 2005, 2, 55–58. [Google Scholar]
- Chen, Y.; Huang, W. Study on the characteristics of physiological and biochemical indexes of athletes with different sword types in fencing. China Sports Sci. Technol. 2008, 2, 116–120. [Google Scholar]
- Zeng, C.; Wang, W.; Chen, C.; Zhang, C.; Cheng, B. Sex differences in time-domain and frequency-domain heart rate variability measures of fatigued drivers. Int. J. Environ. Res. Public Health 2020, 17, 8499. [Google Scholar] [CrossRef]
- Farinatti, P.; Cordeiro, R.; Vogel, M.; Machado, S.; Monteiro, W. Postexercise blood pressure and autonomic responses after aerobic exercise following anodal tDCS applied over the medial prefrontal cortex. Neurosci. Lett. 2019, 711, 134444. [Google Scholar] [CrossRef]
- Thorpe, R.T.; Strudwick, A.J.; Buchheit, M.; Atkinson, G.; Drust, B.; Gregson, W. Monitoring fatigue during the in-season competitive phase in elite soccer players. Int. J. Sports Physiol. Perform. 2015, 10, 958–964. [Google Scholar] [CrossRef]
- Al Haddad, H.; Laursen, P.B.; Chollet, D.; Ahmaidi, S.; Buchheit, M. Reliability of resting and postexercise heart rate measures. Int. J. Sports Med. 2011, 32, 598–605. [Google Scholar] [CrossRef]
- Garet, M.; Tournaire, N.; Roche, F.; Laurent, R.; LAcour, J.R.; Barthélémy, J.C.; Pichot, V. Individual interdependence between nocturnal ANS activity and performance in swimmers. Med. Sci. Sports Exerc. 2004, 36, 2112–2118. [Google Scholar] [CrossRef] [PubMed]
- Pichot, V.; Roche, F.; Gaspoz, J.; Enjolras, F.; Antoniadis, A.; Minini, P.; Costes, F.; Busso, T.; Lacour, J.R.; Barthélémy, J.C. Relation between heart rate variability and training load in middle-distance runners. Med. Sci. Sports Exerc. 2000, 32, 1729–1736. [Google Scholar] [CrossRef] [PubMed]
- Botek, M.; McKune, A.J.; Krejci, J.; Stejskal, P.; Gaba, A. Change in performance in response to training load adjustment based on autonomic activity. Int. J. Sports Med. 2014, 35, 482–488. [Google Scholar] [CrossRef]
- Bernardi, L.; Leuzzi, S.; Radaelli, A.; Passino, C.; Johnston, J.A.; Sleight, P. Low-frequency spontaneous fluctuations of RR interval and blood pressure in conscious humans: A baroreceptor or central phenomenon? Clin. Sci. 1994, 87, 649–654. [Google Scholar] [CrossRef]
- Uusitalo, A.; Uusitalo, A.J.; Rusko, H.K. Endurance training, overtraining and baroreflex sensitivity in female athletes. Occup. Health Ind. Med. 1999, 1, 48. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, R.A.; Farinatti, P.D.T.V.; Fontes, E.B.; da Silva Soares, P.P.; da Cunha, F.A.; Gurgel, J.L.; Porto, F.; Cyrino, E.S.; Okano, A.H. Transcranial direct current stimulation influences the cardiac autonomic nervous control. Neurosci. Lett. 2011, 497, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Aubert, A.E.; Seps, B.; Beckers, F. Heart rate variability in athletes. Sports Med. 2003, 33, 889–919. [Google Scholar] [CrossRef] [PubMed]
- Kliszczewicz, B.; Williamson, C.; Bechke, E.; McKenzie, M.; Hoffstetter, W. Autonomic response to a short and long bout of high-intensity functional training. J. Sports Sci. 2018, 36, 1872–1879. [Google Scholar] [CrossRef]
- Pichon, A.P.; de Bisschop, C.; Roulaud, M.; Denjean, A.; Papelier, Y. Spectral analysis of heart rate variability during exercise in trained subjects. Med. Sci. Sports Exerc. 2004, 36, 1702–1708. [Google Scholar] [CrossRef]
- Casadei, B.; Moon, J.; Johnston, J.; Caiazza, A.; Sleight, P. Is respiratory sinus arrhythmia a good index of cardiac vagal tone in exercise? J. Appl. Physiol. 1996, 81, 556–564. [Google Scholar] [CrossRef]
- Kiss, O.; Sydó, N.; Vargha, P.; Vágó, H.; Czimbalmos, C.; Édes, E.; Zima, E.; Apponyi, G.; Merkely, G.; Sydó, T.; et al. Detailed heart rate variability analysis in athletes. Clin. Autonom. Res. 2016, 26, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Bonato, M.; Agnello, L.; Galasso, L.; Montaruli, A.; Roveda, E.; Merati, G.; La Torre, A.; Vitale, J.A. Acute modification of cardiac autonomic function of high-intensity interval training in collegiate male soccer players with different chronotype: A cross-over study. J. Sports Sci. Med. 2017, 16, 286. [Google Scholar] [PubMed]
- Stanley, J.; Peake, J.M.; Buchheit, M. Cardiac parasympathetic reactivation following exercise: Implications for training prescription. Sports Med. 2013, 43, 1259–1277. [Google Scholar] [CrossRef] [PubMed]
- Kliszczewicz, B.M.; Esco, M.R.; Quindry, J.C.; Blessing, D.L.; Oliverm, G.D.; Taylor, K.L.; Price, B.M. Autonomic Responses to an Acute Bout of High-Intensity Body Weight Resistance Exercise vs. Treadmill Running. J. Strength Cond. Res. 2016, 30, 1050–1058. [Google Scholar] [CrossRef]
- Manzi, V.; Castagna, C.; Padua, E.; Lombardo, M.; D’Ottavio, S.; Massaro, M.; Volterrani, M.; Iellamo, F. Dose-response relationship of autonomic nervous system responses to individualized training impulse in marathon runners. Am. J. Physiol. Heart Circ. Physiol. 2009, 296, H1733–H1740. [Google Scholar] [CrossRef] [PubMed]
- Alon, G.; Yungher, D.A.; Shulman, L.M.; Rogers, M.W. Safety and immediate effect of noninvasive transcranial pulsed current stimulation on gait and balance in Parkinson disease. Neurorehab. Neural Repair 2012, 26, 1089–1095. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Experimental Group | Comparison Group | p-Value | |
|---|---|---|---|
| Age/years | 20.47 ± 0.72 | 20.63 ± 1.46 | 0.683 |
| Height/cm | 177.89 ± 7.24 | 178.37 ± 6.40 | 0.832 |
| Weight/kg | 73.97 ± 10.99 | 70.58 ± 8.96 | 0.315 |
| Training years | 4.12 ± 0.99 | 4.00 ± 0.75 | 0.688 |
| Day | Total Training Distance | Main Training Time/min | Auxiliary Training Time/min | Borg |
|---|---|---|---|---|
| First day | 20 km | 138 min | 42 min | 8.53 ± 0.67 |
| Second day | 14 km | 108 min | 72 min | 8.26 ± 0.44 |
| Third day | 22 km | 144 min | 36 min | 8.80 ± 0.75 |
| Fourth day | 16 km | 113 min | 67 min | 8.36 ± 0.60 |
| Fifth day | 18 km | 124 min | 56 min | 9.00 ± 0.68 |
| Sixth day | 14 km | 110 min | 70 min | 8.66 ± 0.65 |
| Seventh day | 18 km | 120 min | 50 min | 8.93 ± 0.72 |
| Indicators | F | p | Indicators | F | p | ||
|---|---|---|---|---|---|---|---|
| T (ng/mL) | Time | 9.330 | 0.003 | RMSSD/ms | Time | 8.254 | 0.006 |
| group | 2.813 | 0.099 | group | 0.157 | 0.694 | ||
| Time × group | 1.535 | 0.220 | SDNN/ms | Time × group | 0.828 | 0.367 | |
| C (nmol/L) | Time | 97.966 | 0.000 | Time | 16.366 | 0.000 | |
| group | 14.084 | 0.000 | group | 3.671 | 0.060 | ||
| Time × group | 14.478 | 0.000 | LF/ms2 | Time × group | 1.937 | 0.169 | |
| T/C | Time | 76.102 | 0.003 | Time | 19.263 | 0.000 | |
| group | 4.445 | 0.039 | group | 7.032 | 0.010 | ||
| Time × group | 8.024 | 0.006 | Time × group | 7.032 | 0.01 | ||
| CK (ng/mL) | Time | 90.626 | 0.000 | HF/ms2 | Time | 109.850 | 0.000 |
| group | 2.393 | 0.127 | group | 0.203 | 0.654 | ||
| Time × group | 5.171 | 0.027 | Time × group | 7.410 | 0.009 |
| Indicators | Test Time | Experimental Group | Control Group | T | p | Rate of Change Difference |
|---|---|---|---|---|---|---|
| T (ng/mL) | Pre-training | 5.677 ± 0.708 | 5.565 ± 0.589 | 0.608 | 0.545 | 4.313% |
| Post-training | 5.494 ± 0.658 | 5.155 ± 0.552 | 2.162 | 0.035 | ||
| C (nmol/L) | Pre-training | 255.112 ± 31.098 | 245.701 ± 18.050 | 1.434 | 0.157 | 16.700% |
| Post-training | 287.021 ± 27.151 | 317.465 ± 34.937 | −3.769 | 0.000 | ||
| T/C | Pre-training | 0. 070 ± 0.013 | 0.071 ± 0.009 | −0.228 | 0.821 | 13.884% |
| Post-training | 0.060 ± 0.010 | 0.051 ± 0.008 | 3.753 | 0.000 | ||
| CK (ng/mL) | Pre-training | 80.509 ± 10.382 | 79.113 ± 11.745 | 0.488 | 0.627 | 11.848% |
| Post-training | 95.041 ± 10.811 | 102.765 ± 11.389 | −2.694 | 0.009 | ||
| RMSSD/ms | Pre-training | 45.080 ± 14.236 | 45.716 ± 17.882 | 0.153 | 0.879 | 8.655% |
| Post-training | 40.744 ± 14.537 | 37.36 ± 16.73 | 0.836 | 0.407 | ||
| SDNN/ms | Pre-training | 73.399 ± 15.579 | 69.601 ± 16.900 | 0.905 | 0.369 | 11.624% |
| Post-training | 66.05 ± 18.010 | 54.541 ± 23.767 | 2.114 | 0.039 | ||
| LF/ms2 | Pre-training | 1557.930 ± 590.033 | 1544.173 ± 579.528 | 0.091 | 0.928 | 34.418% |
| Post-training | 1731.498 ± 752.877 | 2247.697 ± 839.009 | −2.508 | 0.015 | ||
| HF/ms2 | Pre-training | 1211.880 ± 338.954 | 1264.589 ± 485.907 | −0.487 | 0.628 | 15.341% |
| Post-training | 917.129 ± 400.070 | 763.014 ± 578.380 | 1.200 | 0.235 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Q.; Fang, G.; Zhao, J.; Liu, J. Effect of Transcranial Pulsed Current Stimulation on Fatigue Delay after Medium-Intensity Training. Int. J. Environ. Res. Public Health 2022, 19, 7042. https://doi.org/10.3390/ijerph19127042
Wu Q, Fang G, Zhao J, Liu J. Effect of Transcranial Pulsed Current Stimulation on Fatigue Delay after Medium-Intensity Training. International Journal of Environmental Research and Public Health. 2022; 19(12):7042. https://doi.org/10.3390/ijerph19127042
Chicago/Turabian StyleWu, Qingchang, Guoliang Fang, Jiexiu Zhao, and Jian Liu. 2022. "Effect of Transcranial Pulsed Current Stimulation on Fatigue Delay after Medium-Intensity Training" International Journal of Environmental Research and Public Health 19, no. 12: 7042. https://doi.org/10.3390/ijerph19127042