
Occupational Low-Dose Radiation Affects the Expression of Immune Checkpoint of Medical Radiologists

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Ethics Statement
2.2. Individual Monitoring of Occupational External Exposure
2.3. Sample Preparation
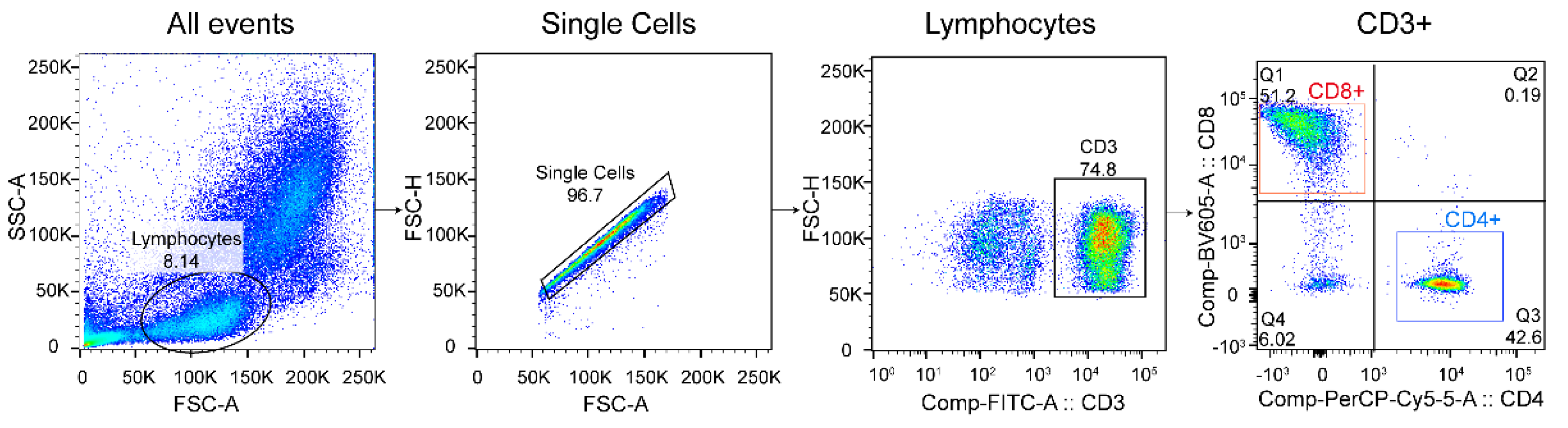
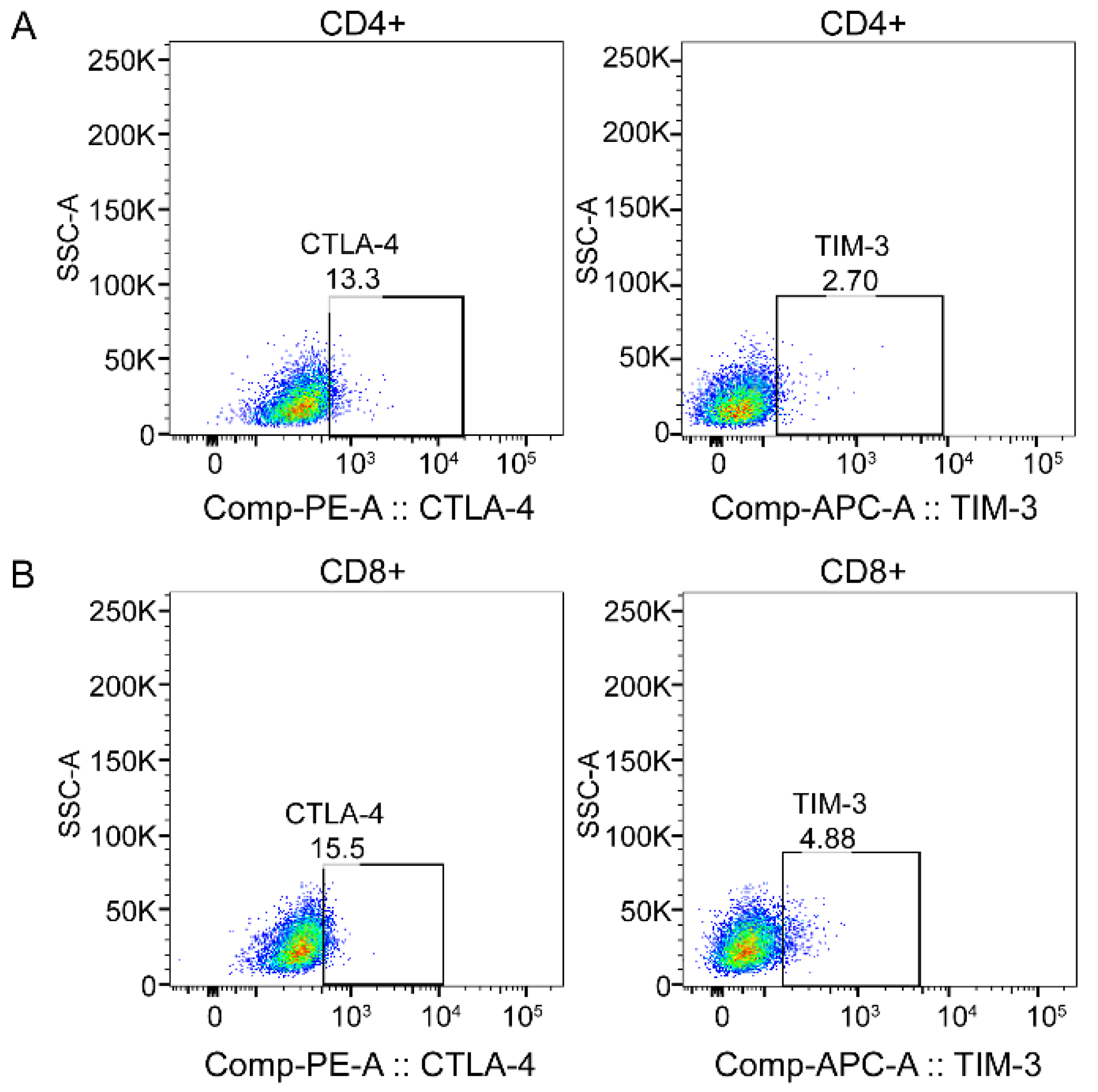
2.4. Flow Cytometry
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Study Population
3.2. Peripheral Blood Results Analysis
3.3. The Relative Expression Levels of CD3+T, CD4+T, and CD8+T Cells and TIM-3 and CTLA-4
3.4. The Relationship between Demographic Characteristics and Percentage of CD4+T and CD8+T Cells and Expression of CTLA-4 and TIM-3
3.5. Relationship between Cumulative Exposure Dose and CTLA-4 and TIM-3 Expression Levels in Peripheral Blood Lymphocytes of Radiation Workers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mettler, F.A., Jr.; Thomadsen, B.R.; Bhargavan, M.; Gilley, D.B.; Gray, J.E.; Lipoti, J.A.; McCrohan, J.; Yoshizumi, T.T.; Mahesh, M. Medical radiation exposure in the us in 2006: Preliminary results. Health Phys. 2008, 95, 502–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, K.-H. General Principles of Radiation Protection in Fields of Diagnostic Medical Exposure. J. Korean Med. Sci. 2016, 31, S6–S9. [Google Scholar] [CrossRef] [PubMed]
- The 2007 Recommendations of the International Commission on Radiological Protection. Ann. ICRP 2007, 37, 1–332.
- Cioffi, D.L.; Fontana, L.; Leso, V.; Dolce, P.; Vitale, R.; Vetrani, I.; Galdi, A.; Iavicoli, I. Low dose ionizing radiation exposure and risk of thyroid functional alterations in healthcare workers. Eur. J. Radiol. 2020, 132, 109279. [Google Scholar] [CrossRef]
- Baselet, B.; Rombouts, C.; Benotmane, R.; Baatout, S.; Aerts, A. Cardiovascular diseases related to ionizing radiation: The risk of low-dose exposure. Int. J. Mol. Med. 2016, 38, 1623–1641. [Google Scholar] [CrossRef] [Green Version]
- Coppeta, L.; Pietroiusti, A.; Neri, A.; Spataro, A.; De Angelis, E.; Perrone, S.; Magrini, A. Risk of radiation-induced lens opacities among surgeons and interventional medical staff. Radiol. Phys. Technol. 2019, 12, 26–29. [Google Scholar] [CrossRef]
- El-Saghire, H.; Michaux, A.; Thierens, H.; Baatout, S. Low doses of ionizing radiation induce immune-stimulatory responses in isolated human primary monocytes. Int. J. Mol. Med. 2013, 32, 1407–1414. [Google Scholar] [CrossRef] [Green Version]
- El-Saghire, H.; Thierens, H.; Monsieurs, P.; Michaux, A.; Vandevoorde, C.; Baatout, S. Gene set enrichment analysis highlights different gene expression profiles in whole blood samples X-irradiated with low and high doses. Int. J. Radiat. Biol. 2013, 89, 628–638. [Google Scholar] [CrossRef]
- Zeegers, D.; Venkatesan, S.; Koh, S.W.; Low, G.K.M.; Srivastava, P.; Sundaram, N.; Sethu, S.; Banerjee, B.; Jayapal, M.; Belyakov, O.; et al. Biomarkers of Ionizing Radiation Exposure: A Multiparametric Approach. Genome Integr. 2017, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Chaudhury, N.K.; Agrawala, P.K.; Adhikari, J.S. Lymphocyte chromosomal aberration assay in radiation biodosimetry. J. Pharm. BioAllied Sci. 2010, 2, 197–201. [Google Scholar] [CrossRef]
- Voisin, P. Standards in biological dosimetry: A requirement to perform an appropriate dose assessment. Mutat. Res. Toxicol. Environ. Mutagen. 2015, 793, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Manda, K.; Glasow, A.; Paape, D.; Hildebrandt, G. Effects of ionizing radiation on the immune system with special emphasis on the immune system with special emphasis on the interaction of dendritic and T cells. Front. Oncol. 2012, 2, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyuleva, I.; Panova, D.; Djounova, J.; Rupova, I.; Penkova, K. Assessment of Some Immune Parameters in Occupationally Exposed Nuclear Power Plants. Dose Response 2015, 13, 1559325815611901. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, J. Functions of Immune Checkpoint Molecules Beyond Immune Evasion. Adv. Exp. Med. Biol. 2020, 1248, 201–226. [Google Scholar] [CrossRef] [PubMed]
- Zamani, M.R.; Aslani, S.; Salmaninejad, A.; Javan, M.R.; Rezaei, N. PD-1/PD-L and autoimmunity: A growing relationship. Cell. Immunol. 2016, 310, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Nabekura, T.; Kanaya, M.; Shibuya, A.; Fu, G.; Gascoigne, N.R.; Lanier, L.L. Costimulatory Molecule DNAM-1 Is Essential for Optimal Differentiation of Memory Natural Killer Cells during Mouse Cytomegalovirus Infection. Immunity 2014, 40, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Allison, J.P. The future of immune checkpoint therapy. Science 2015, 348, 56–61. [Google Scholar] [CrossRef]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Miko, E.; Meggyes, M.; Doba, K.; Barakonyi, A.; Szereday, L. Immune Checkpoint Molecules in Reproductive Immunology. Front. Immunol. 2019, 10, 846. [Google Scholar] [CrossRef]
- Van Coillie, S.; Wiernicki, B.; Xu, J. Molecular and Cellular Functions of CTLA-4. Adv. Exp. Med. Biol. 2020, 1248, 7–32. [Google Scholar] [CrossRef]
- Chikuma, S. CTLA-4, an Essential Immune-Checkpoint for T-Cell Activation. Curr. Top. Microbiol. Immunol. 2017, 410, 99–126. [Google Scholar] [CrossRef]
- Mitsuiki, N.; Schwab, C.; Grimbacher, B. What did we learn from CTLA-4 insufficiency on the human immune system? Immunol. Rev. 2019, 287, 33–49. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Fueyo, A.; Tian, J.; Picarella, D.; Domenig, C.; Zheng, X.X.; Sabatos, C.A.; Manlongat, N.; Bender, O.; Kamradt, T.; Kuchroo, V.K.; et al. Tim-3 inhibits T helper type 1-mediated auto- and alloimmune responses and promotes immunological tolerance. Nat. Immunol. 2003, 4, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Gaetani, S.; Monaco, F.; Bracci, M.; Ciarapica, V.; Impollonia, G.; Valentino, M.; Tomasetti, M.; Santarelli, L.; Amati, M. DNA damage response in workers exposed to low-dose ionising radiation. Occup. Environ. Med. 2018, 75, 724–729. [Google Scholar] [CrossRef]
- Qian, Q.-Z.; Cao, X.-K.; Liu, H.-Y.; Shen, F.-H.; Wang, Q.; Tong, J.-W. Analysis of Hemogram of Radiation Workers in Tangshan, China. J. Clin. Lab. Anal. 2016, 30, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Kusunoki, Y.; Yamaoka, M.; Kubo, Y.; Hayashi, T.; Kasagi, F.; Douple, E.B.; Nakachi, K. T-cell immunosenescence and inflammatory response in atomic bomb survivors. Radiat. Res. 2010, 174, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, E.H.; Nemhauser, J.B.; Smith, J.M.; Kazzi, Z.N.; Farfán, E.B.; Chang, A.S.; Naeem, S.F. Acute radiation syndrome: Assessment and management. South. Med. J. 2010, 103, 541–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumniczky, K.; Impens, N.; Armengol, G.; Candéias, S.; Georgakilas, A.G.; Hornhardt, S.; Martin, O.A.; Rödel, F.; Schaue, D. Low dose ionizing radiation effects on the immune system. Environ. Int. 2020, 149, 106212. [Google Scholar] [CrossRef]
- Ishii, K.; Hosoi, Y.; Yamada, S.; Ono, T.; Sakamoto, K. Decreased Incidence of Thymic Lymphoma in AKR Mice as a Result of Chronic, Fractionated Low-Dose Total-Body X Irradiation. Radiat. Res. 1996, 146, 582. [Google Scholar] [CrossRef]
- Shigematsu, A.; Adachi, Y.; Koike-Kiriyama, N.; Suzuki, Y.; Iwasaki, M.; Koike, Y.; Nakano, K.; Mukaide, H.; Imamura, M.; Ikehara, S. Effects of low-dose irradiation on enhancement of immunity by Dendritic Cells. J. Radiat. Res. 2007, 48, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Barber, D.L.; Wherry, E.J.; Masopust, D.; Zhu, B.; Allison, J.P.; Sharpe, A.H.; Freeman, G.J.; Ahmed, R. Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 2006, 439, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Joller, N.; Kuchroo, V.K. Tim-3, Lag-3, and TIGIT. Curr. Top Microbiol. Immunol. 2017, 410, 127–156. [Google Scholar] [PubMed] [Green Version]
- Kern, R.; Panis, C. CTLA-4 Expression and Its Clinical Significance in Breast Cancer. Arch. Immunol. Et Ther. Exp. 2021, 69, 16. [Google Scholar] [CrossRef] [PubMed]
- Lo, B.; Zhang, K.; Lu, W.; Zheng, L.; Zhang, Q.; Kanellopoulou, C.; Zhang, Y.; Liu, Z.; Fritz, J.M.; Marsh, R.; et al. Patients with LRBA deficiency show CTLA4 loss and immune dysregulation responsive to abatacept therapy. Science 2015, 349, 436–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, P.-J.; Li, Y.; Sun, S. On the significance of Tim-3 expression in pancreatic cancer. Saudi J. Biol. Sci. 2017, 24, 1754–1757. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wang, Y.; Liu, X.R.; Hong, S.R.; Yao, J. Downregulated Tim-3 expression is responsible for the incidence and development of colorectal cancer. Oncol. Lett. 2018, 16, 1059–1066. [Google Scholar] [CrossRef] [Green Version]
- Pandey, R.; Shankar, B.S.; Sharma, D.; Sainis, K.B. Low dose radiation induced immunomodulation: Effect on macrophages and CD8+T cells. Int. J. Radiat. Biol. 2005, 81, 801–812. [Google Scholar] [CrossRef]
- Wilkins, R.C.; Wilkinson, D.; Maharaj, H.P.; Bellier, P.V.; Cybulski, M.B.; McLean, J.R. Differential apoptotic response to ionizing radiation in subpopulations of human. Mutat. Res. 2002, 513, 27–36. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Radiation Workers (n = 100) | Control Group (n = 107) | χ2 | p | |
|---|---|---|---|---|---|
| Age (year) | ≤38 | 52 (52.0%) | 55 (51.4%) | 0.007 | 0.931 |
| >38 | 48 (48.0%) | 52 (48.6%) | |||
| BMI (kg/m2) | <18.5 | 3 (3%) | 1 (0.9%) | 4.919 | 0.171 |
| 18.5~23.9 | 26 (26.0%) | 18 (16.8%) | |||
| 23.9~27.9 | 55 (55.0%) | 62 (57.9%) | |||
| >27.9 | 16 (16.0%) | 26 (24.3%) | |||
| Current smoking status | Yes | 24 (24.0%) | 68 (63.6%) | 32.749 | <0.001 |
| No | 76 (76.0%) | 39 (36.4%) | |||
| Current alcohol consumption | Yes | 40 (40.0%) | 72 (67.3%) | 15.503 | <0.001 |
| No | 60 (60.0%) | 35 (32.7%) | |||
| Length of service (year) | 13.3 ± 1.1 | ||||
| Type of work | interventional radiology | 55 (55.0%) | |||
| radiotherapy | 12 (12.0%) | ||||
| diagnostic radiology | 28 (28.0%) | ||||
| nuclear medicine | 5 (5.0%) | ||||
| Cumulative dose (mSv) | 5.70 ± 0.48 | ||||
| Variables | Radiation Workers (n = 100) | Control Group (n = 107) | Model 1 | Model 2 | ||
|---|---|---|---|---|---|---|
| Z | p | χ2 | p | |||
| WBC (109/L) | 6.67 (5.75, 8.24) | 7.17 (6.14, 7.82) | −1.381 | 0.167 | 0.106 | 0.745 |
| LY (109/L) | 2.23 (1.87, 2.54) | 2.38 (1.95, 2.72) | −1.427 | 0.154 | 0.001 | 0.973 |
| RBC (1012/L) | 5.06 (4.82, 5.28) | 5.17 (4.97, 5.39) | −2.570 | 0.010 | 6.563 | 0.010 |
| Hb (g/L) | 146.50 (141.00, 152.75) | 156.81 (152.00, 163.00) | −7.236 | <0.001 | 40.357 | <0.001 |
| PLT (109/L) | 238.00 (207.25, 279.75) | 267.67 (225.00, 298.00) | −2.996 | 0.003 | 2.523 | 0.112 |
| Cells | Radiation Workers (n = 100) | Control Group (n = 107) | Z (p) |
|---|---|---|---|
| M (P25, P75) | M (P25, P75) | ||
| CD3+ (%) | 61.34 (55.58, 67.90) | 63.30 (58.10, 68.80) | −1.574 (0.115) |
| CD4−CD8+ (%) | 40.55 (33.20, 47.63) | 36.70 (29.90, 43.60) | −2.513 (0.012) |
| CD8+CTLA-4+ (%) | 7.51 (4.17, 10.25) | 7.78 (4.84, 10.90) | −0.982 (0.326) |
| CD8+TIM3+ (%) | 3.45 (2.19, 5.08) | 3.53 (2.27, 4.96) | −0.339 (0.735) |
| CD4+CD8− (%) | 48.90 (41.53, 57.90) | 51.57 (44.40, 59.30) | −1.800 (0.072) |
| CD4+CTLA-4+ (%) | 5.25 (3.37, 7.26) | 7.29 (4.73, 10.70) | −4.680 (<0.001) |
| CD4+TIM3+ (%) | 4.26 (3.38, 5.84) | 5.25 (4.13, 5.99) | −2.634 (0.008) |
| Variables | CD4+ (%) | CD8+ (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Radiation Workers (n = 100) | Control Group (n = 107) | χ2 (p) a | Radiation Workers (n = 100) | Control Group (n = 107) | χ2 (p) a | |||||
| n | M (P25, P75) | n | M (P25, P75) | n | M (P25, P75) | n | M (P25, P75) | |||
| Age (year) | ||||||||||
| ≤38 | 52 | 48.00 (41.23, 53.60) | 55 | 52.00 (43.70, 58.20) | 0.142 (0.706) | 52 | 41.40 (33.73, 47.93) | 55 | 36.70 (32.20, 42.90) | 1.720 (0.190) |
| >38 | 48 | 49.13 (42.58, 59.65) | 52 | 51.57 (44.40, 60.48) | 0.050 (0.824) | 48 | 39.98 (30.85, 47.40) | 52 | 36.79 (27.70, 43.60) | 2.920 (0.087) |
| χ2 (p) b | 2.046 (0.153) | 0.018 (0.894) | 1.484 (0.223) | 0.420 (0.517) | ||||||
| BMI | ||||||||||
| <18.5 | 3 | 41.90 (22.40) | 1 | 73.40 | 25.926 (<0.001) | 3 | 45.00 (42.90) | 1 | 51.8 | 34.436 (<0.001) |
| 18.5~23.9 | 26 | 50.20 (40.48, 60.90) | 18 | 52.50 (44.83, 59.58) | 0.065 (0.799) | 26 | 38.65 (28.65, 47.48) | 18 | 36.45 (30.33, 44.90) | 0.026 (0.871) |
| 23.9~27.9 | 55 | 49.13 (43.10, 58.70) | 62 | 51.10 (43.10, 58.58) | 1.194 (0.275) | 55 | 40.46 (32.50, 48.50) | 62 | 36.35 (29.00, 43.60) | 3.250 (0.071) |
| >27.9 | 16 | 47.05 (40.35, 50.45) | 26 | 51.95 (44.40, 59.93) | 4.081 (0.043) | 16 | 43.70 (37.05, 47.10) | 26 | 36.79 (32.38, 43.28) | 4.504 (0.034) |
| χ2 (p) b | 5.322 (0.150) | 5.485 (0.140) | 4.924 (0.177) | 2.859 (0.414) | ||||||
| Current smoking | ||||||||||
| Yes | 24 | 50.35 (40.85, 59.65) | 68 | 54.10 (46.73, 60.88) | 2.111 (0.146) | 24 | 40.23 (32.68, 50.48) | 68 | 36.05 (28.40, 43.15) | 5.151 (0.023) |
| No | 76 | 48.30 (41.53, 54.83) | 39 | 48.30 (40.90, 53.70) | 1.423 (0.233) | 76 | 40.85 (33.33, 47.38) | 39 | 38.20 (32.80, 45.50) | 0.921 (0.337) |
| χ2 (p) b | 0.655 (0.418) | 12.261 (<0.001) | 0.046 (0.830) | 4.075 (0.044) | ||||||
| Current drinking | ||||||||||
| Yes | 40 | 48.90 (41.25, 59.03) | 72 | 51.68 (44.50, 59.90) | 0.126 (0.722) | 40 | 40.55 (33.25, 47.85) | 72 | 36.74 (30.25, 43.60) | 1.504 (0.220) |
| No | 60 | 48.75 (42.03, 53.68) | 35 | 51.10 (44.30, 59.10) | 0.017 (0.896) | 60 | 40.58 (32.83, 47.63) | 35 | 36.70 (29.50, 42.90) | 4.451 (0.035) |
| χ2 (p) b | 0.006 (0.937) | 0.000 (0.999) | 0.016 (0.899) | 0.655 (0.418) | ||||||
| Variables | CD8+CTLA-4+ (%) | CD8+TIM-3+ (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Radiation Workers (n = 100) | Control Group (n = 107) | χ2 (p) a | Radiation Workers (n = 100) | Control Group (n = 107) | χ2 (p) a | |||||
| n | M (P25, P75) | n | M (P25, P75) | n | M (P25, P75) | n | M (P25, P75) | |||
| Age (year) | ||||||||||
| ≤38 | 52 | 7.18 (4.03, 9.42) | 55 | 7.26 (4.60, 11.10) | 0.166 (0.684) | 52 | 3.98 (2.36, 5.48) | 55 | 3.70 (2.81, 4.96) | 1.395 (0.237) |
| >38 | 48 | 8.01 (4.38, 10.78) | 52 | 8.06 (5.41, 9.98) | 0.671 (0.413) | 48 | 2.99 (2.08, 4.45) | 52 | 3.52 (1.66, 4.95) | 0.016 (0.898) |
| χ2 (p) b | 1.405 (0.236) | 0.258 (0.612) | 0.176 (0.675) | 0.480 (0.488) | ||||||
| BMI | ||||||||||
| <18.5 | 3 | 8.70 (8.65) | 1 | 1.78 | 27.725 (<0.001) | 3 | 3.65 (2.20) | 1 | 8.17 | 37.381 (<0.001) |
| 18.5~23.9 | 26 | 7.50 (3.90, 10.53) | 18 | 7.42 (4.61, 9.68) | 0.782 (0.376) | 26 | 3.34 (2.20, 5.28) | 18 | 3.73 (2.11, 4.41) | 0.005 (0.945) |
| 23.9~27.9 | 55 | 8.04 (5.10, 12.60) | 62 | 7.67 (4.91, 11.68) | 1.285 (0.257) | 55 | 3.27 (2.04, 4.45) | 62 | 3.59 (2.26, 5.09) | 4.973 (0.026) |
| >27.9 | 16 | 3.87 (2.57, 7.81) | 26 | 8.32 (5.23, 10.52) | 3.749 (0.053) | 16 | 4.53 (2.54, 8.71) | 26 | 3.52 (2.49, 4.45) | 6.661 (0.010) |
| χ2 (p) b | 4.729 (0.193) | 3.005 (0.391) | 8.803 (0.032) | 3.218 (0.359) | ||||||
| Current smoking | ||||||||||
| Yes | 24 | 7.89 (4.66, 9.98) | 68 | 8.87 (4.90, 11.95) | 0.400 (0.527) | 24 | 3.94 (2.44, 6.31) | 68 | 4.13 (2.25, 4.96) | 6.209 (0.013) |
| No | 76 | 7.32 (4.03, 10.38) | 39 | 6.88 (4.76, 8.87) | 0.640 (0.424) | 76 | 3.26 (2.14, 4.82) | 39 | 3.45 (2.27, 5.01) | 2.782 (0.095) |
| χ2 (p) b | 0.394 (0.530) | 0.611 (0.434) | 6.712 (0.010) | 1.045 (0.307) | ||||||
| Current drinking | ||||||||||
| Yes | 40 | 7.98 (4.08, 11.00) | 72 | 7.93 (4.79, 11.35) | 0.124 (0.725) | 40 | 3.39 (2.34, 4.83) | 72 | 4.00 (2.44, 5.06) | 3.472 (0.062) |
| No | 60 | 7.26 (4.17, 10.25) | 35 | 6.95 (4.84, 9.04) | 3.261 (0.071) | 60 | 3.59 (2.08, 5.57) | 35 | 3.31 (1.92, 4.36) | 1.521 (0.217) |
| χ2 (p) b | 0.419 (0.518) | 0.351 (0.554) | 0.006 (0.937) | 0.816 (0.366) | ||||||
| Variables | CD4+CTLA-4+ (%) | CD4+TIM-3+ (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Radiation Workers (n = 100) | Control Group (n = 107) | χ2 (p) a | Radiation Workers (n = 100) | Control Group (n = 107) | χ2 (p) a | |||||
| n | M (P25, P75) | n | M (P25, P75) | n | M (P25, P75) | n | M (P25, P75) | |||
| Age (year) | ||||||||||
| ≤38 | 52 | 5.43 (3.50, 7.26) | 55 | 8.24 (4.93, 12.00) | 11.762 (0.001) | 52 | 4.03 (3.17, 5.84) | 55 | 5.26 (4.55, 6.05) | 1.357 (0.244) |
| >38 | 48 | 5.06 (2.96, 7.26) | 52 | 6.62 (4.46, 9.27) | 5.835 (0.016) | 48 | 4.33 (3.60, 5.86) | 52 | 4.78 (3.64, 5.90) | 0.265 (0.607) |
| χ2 (p) b | 0.323 (0.570) | 4.768 (0.029) | 0.285 (0.593) | 1.154 (0.283) | ||||||
| BMI | ||||||||||
| <18.5 | 3 | 4.99 (4.46) | 1 | 4.46 | 31.157 (<0.001) | 3 | 2.86 (2.80) | 1 | 2.86 | 487.409 (<0.001) |
| 18.5~23.9 | 26 | 4.76 (3.42, 7.20) | 18 | 8.08 (4.04, 12.05) | 4.079 (0.043) | 26 | 4.26 (3.53, 5.58) | 18 | 5.18 (4.04, 6.32) | 1.091 (0.296) |
| 23.9~27.9 | 55 | 5.43 (3.78, 6.54) | 62 | 6.78 (4.97, 10.43) | 6.382 (0.012) | 55 | 3.87 (3.36, 5.30) | 62 | 4.70 (3.99, 6.06) | 0.010 (0.920) |
| >27.9 | 16 | 4.17 (2.09, 7.88) | 26 | 7.93 (4.84, 11.48) | 5.132 (0.023) | 16 | 6.06 (3.82, 11.58) | 26 | 5.25 (4.51, 5.81) | 10.901 (0.001) |
| χ2 (p) b | 0.393 (0.942) | 3.383 (0.336) | 10.513 (0.015) | 11.640 (0.009) | ||||||
| Current smoking | ||||||||||
| Yes | 24 | 5.67 (3.48, 8.25) | 68 | 6.78 (4.81, 10.58) | 2.597 (0.107) | 24 | 5.58 (4.07, 7.74) | 68 | 5.02 (3.89, 6.01) | 4.589 (0.032) |
| No | 76 | 5.03 (3.25, 6.67) | 39 | 7.87 (4.47, 11.00) | 17.838 (<0.001) | 76 | 3.83 (3.17, 5.30) | 39 | 5.26 (4.39, 5.99) | 0.053 (0.818) |
| χ2 (p) b | 0.820 (0.365) | 0.199 (0.656) | 7.253 (0.007) | 0.406 (0.524) | ||||||
| Current drinking | ||||||||||
| Yes | 40 | 5.52 (3.86, 7.46) | 72 | 6.78 (4.92, 10.68) | 4.389 (0.036) | 40 | 4.36 (3.71, 6.13) | 72 | 5.07 (3.95, 6.04) | 1.480 (0.224) |
| No | 60 | 5.09 (2.87, 6.62) | 35 | 7.91 (4.24, 10.90) | 14.643 (<0.001) | 60 | 3.79 (3.16, 5.38) | 35 | 5.26 (4.42, 5.90) | 0.372 (0.542) |
| χ2 (p) b | 0.644 (0.422) | 0.009 (0.924) | 0.131 (0.718) | 2.131 (0.144) | ||||||
| Cumulative Dose (mSv) | n | CTLA-4+CD8+T(%) | TIM-3+CD8+T(%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M (P25, P75) | β (95% CI) | χ2 | p | M (P25, P75) | β (95% CI) | χ2 | p | ||
| 0~1.73 | 28 | 6.25 (2.90, 8.70) | Ref | 4.07 (2.52, 5.90) | Ref | ||||
| 1.73~4.33 | 23 | 5.75 (3.41, 8.04) | −0.587 (−3.170, 1.996) | 0.198 | 0.656 | 3.76 (2.20, 5.04) | −0.895 (−3.112, 1.322) | 0.626 | 0.429 |
| 4.33~8.65 | 27 | 8.04 (6.45, 10.10) | 2.604 (−0.353, 5.561) | 2.978 | 0.084 | 4.14 (2.36, 5.51) | 0.605 (−1.934, 3.143) | 0.218 | 0.641 |
| 8.65~ | 22 | 9.66 (5.25, 16.55) | 6.130 (1.800, 10.459) | 7.700 | 0.006 | 2.47 (1.70, 3.26) | −2.506 (−6.223, 1.211) | 1.746 | 0.186 |
| Cumulative Dose (mSv) | n | CTLA-4+CD4+T(%) | TIM-3+CD4+T(%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| M (P25, P75) | β (95% CI) | χ2 | p | M (P25, P75) | β (95% CI) | χ2 | p | ||
| 0~1.73 | 28 | 4.67 (2.90, 6.70) | Ref | 4.21 (3.53, 7.20) | Ref | ||||
| 1.73~4.33 | 23 | 4.97 (2.37, 6.72) | −0.245 (−1.807, 1.317) | 0.094 | 0.759 | 3.76 (3.08, 5.92) | −1.405 (−3.000, 0.190) | 2.980 | 0.084 |
| 4.33~8.65 | 27 | 5.43 (4.52, 8.01) | 1.643 (−0.145, 3.431) | 3.243 | 0.072 | 4.36 (3.65, 5.30) | −3.130 (−4.957, −1.304) | 11.282 | 0.001 |
| 8.65~ | 22 | 5.32 (3.34, 7.52) | 1.770 (−0.848, 4.388) | 1.755 | 0.185 | 4.29 (3.02, 5.79) | −4.150 (−6.825, −1.476) | 9.252 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Hao, C.; Dai, K.; Li, Y.; Jiao, J.; Niu, Z.; Xu, X.; Deng, X.; He, J.; Yao, W. Occupational Low-Dose Radiation Affects the Expression of Immune Checkpoint of Medical Radiologists. Int. J. Environ. Res. Public Health 2022, 19, 7105. https://doi.org/10.3390/ijerph19127105
Wang C, Hao C, Dai K, Li Y, Jiao J, Niu Z, Xu X, Deng X, He J, Yao W. Occupational Low-Dose Radiation Affects the Expression of Immune Checkpoint of Medical Radiologists. International Journal of Environmental Research and Public Health. 2022; 19(12):7105. https://doi.org/10.3390/ijerph19127105
Chicago/Turabian StyleWang, Chen, Changfu Hao, Kai Dai, Yuzheng Li, Jie Jiao, Zhuoya Niu, Xiao Xu, Xuedan Deng, Jing He, and Wu Yao. 2022. "Occupational Low-Dose Radiation Affects the Expression of Immune Checkpoint of Medical Radiologists" International Journal of Environmental Research and Public Health 19, no. 12: 7105. https://doi.org/10.3390/ijerph19127105