
Using COMPASS (Context Optimisation Model for Person-Centred Analysis and Systematic Solutions) Theory to Augment Implementation of Digital Health Solutions



Abstract
:1. Introduction
- Evolving study designs that allow an increased implementation of capability innovation;
- Efficacy and safety, such as comparing digital health and social care options to traditional health and social care methods in well-designed large-scale research;
- Greater accountability and feasibility motivate researchers to review why some digital health and social care projects have failed;
- Identifying gaps in planning, dissemination, and enabling the acceptance, adoption, and use of digital health and technologies in health and social care settings is urged by knowledge, attitude, and behaviour;
- While cost-effectiveness implies that interventions utilising digital health technologies can improve safety and quality of care, long-term cost estimates must be reconciled.
2. Materials and Methods
Review of Evidence
3. COMPASS Theoretical Framework and Implementation Model
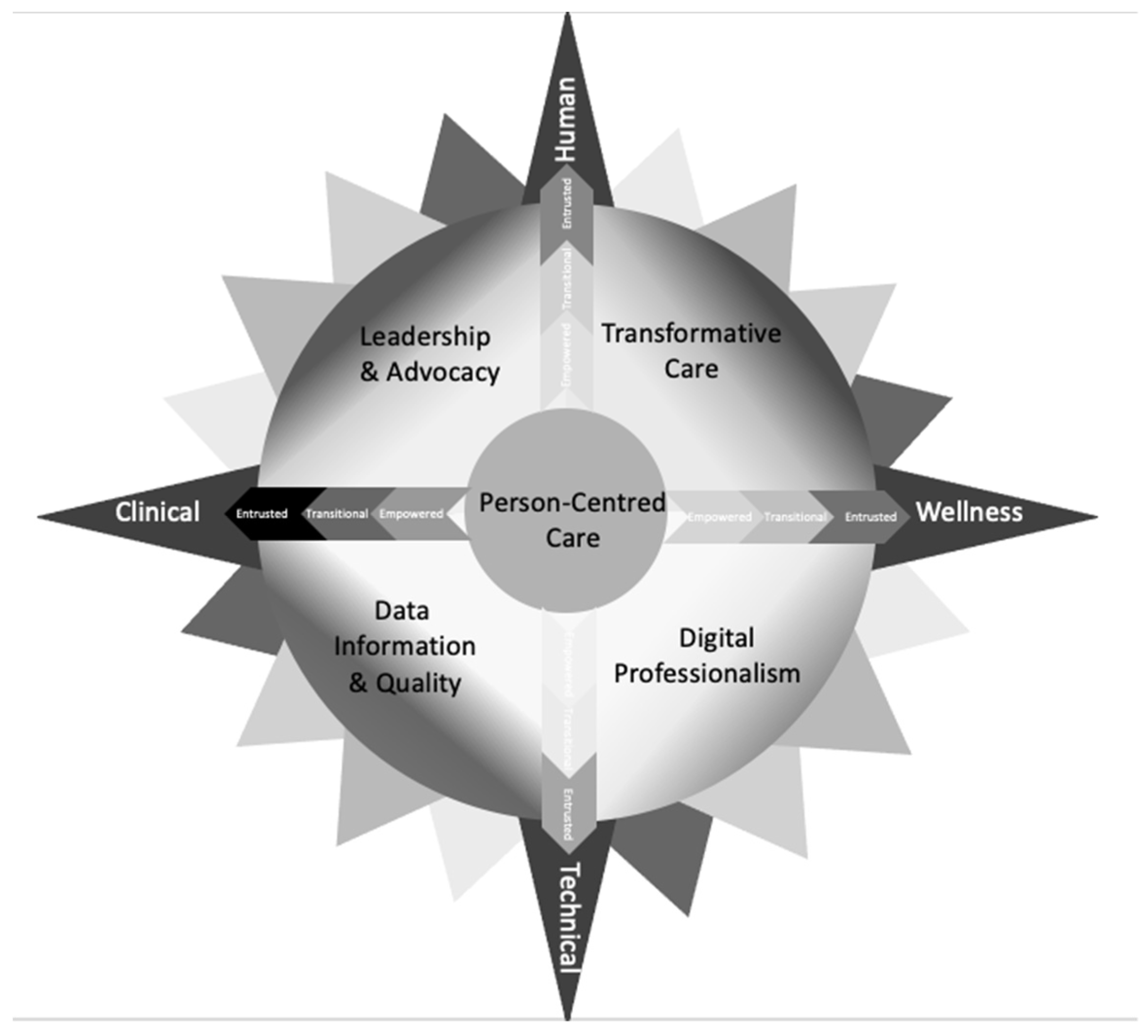
- The navigational compass rose is the inspiration for COMPASS. It is a visual representation of a theoretical framework and implementation model that shows how to plan, develop, implement, and evaluate digital health solutions for digital health and social care providers. The COMPASS theoretical framework contributes to digital health transformation by enabling identification of the foci of digital health issues including human and physical resources and the identification of capability of stakeholders.
- The COMPASS mnemonic summarises the steps involved in how to conduct digital health research. Each letter of the mnemonic represents a step in the process of planning, developing, implementing, and evaluating digital health research. By ensuring that components of the research process are included in each suggested solution, the mnemonic aids digital health transformation.
3.1. Overview
3.2. Layer 1: Core and Quadrants
3.2.1. Person-Centred Care
3.2.2. Leadership and Advocacy
3.2.3. Transformative Care
3.2.4. Digital Professionalism
3.2.5. Data Informatics and Quality
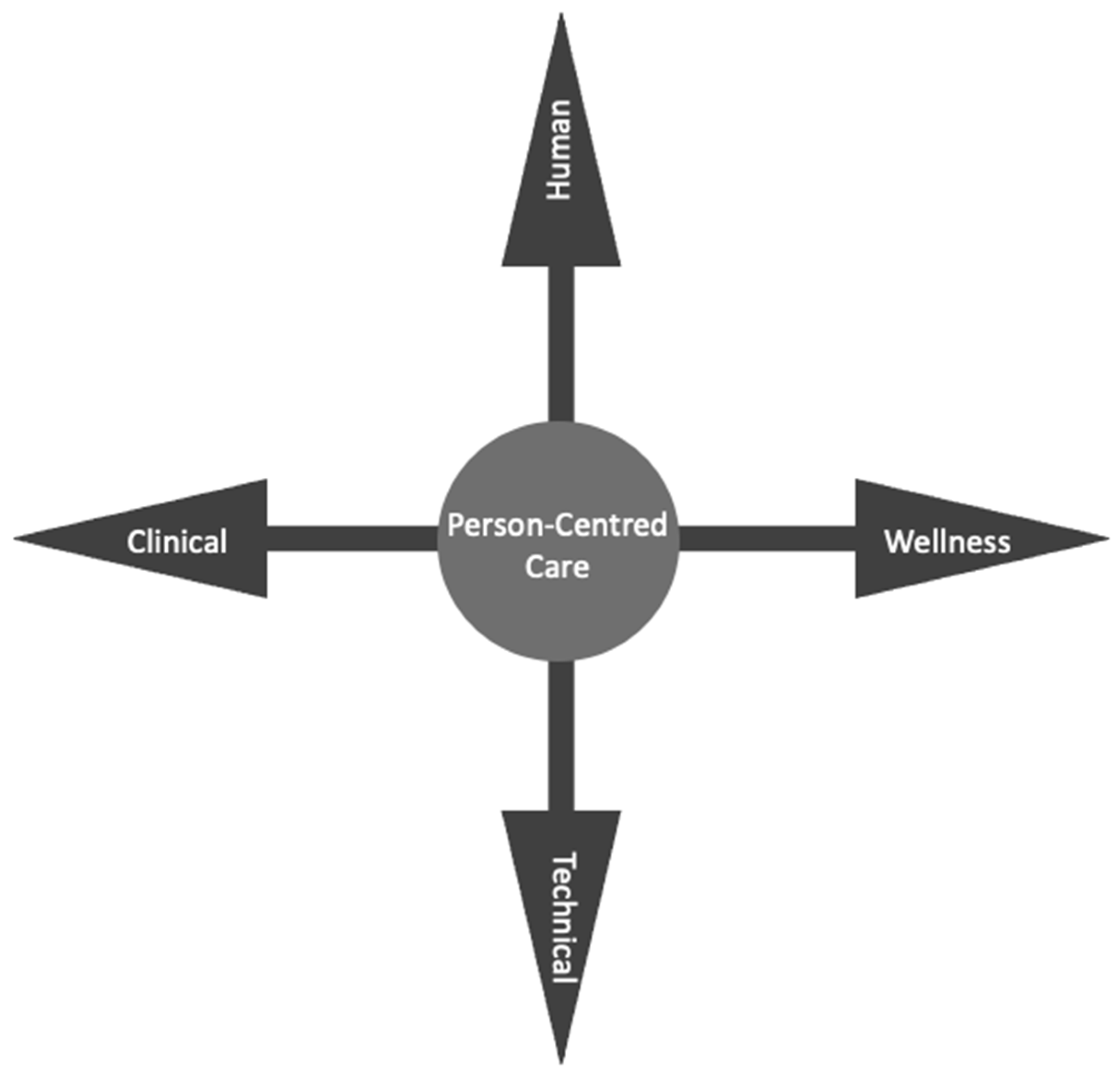
3.3. The Main Compass Points
3.4. COMPASS Directions Continuums
3.4.1. Layer 2a: Human and Technical Continuum
3.4.2. Layer 2b: Clinical and Wellness Continuum
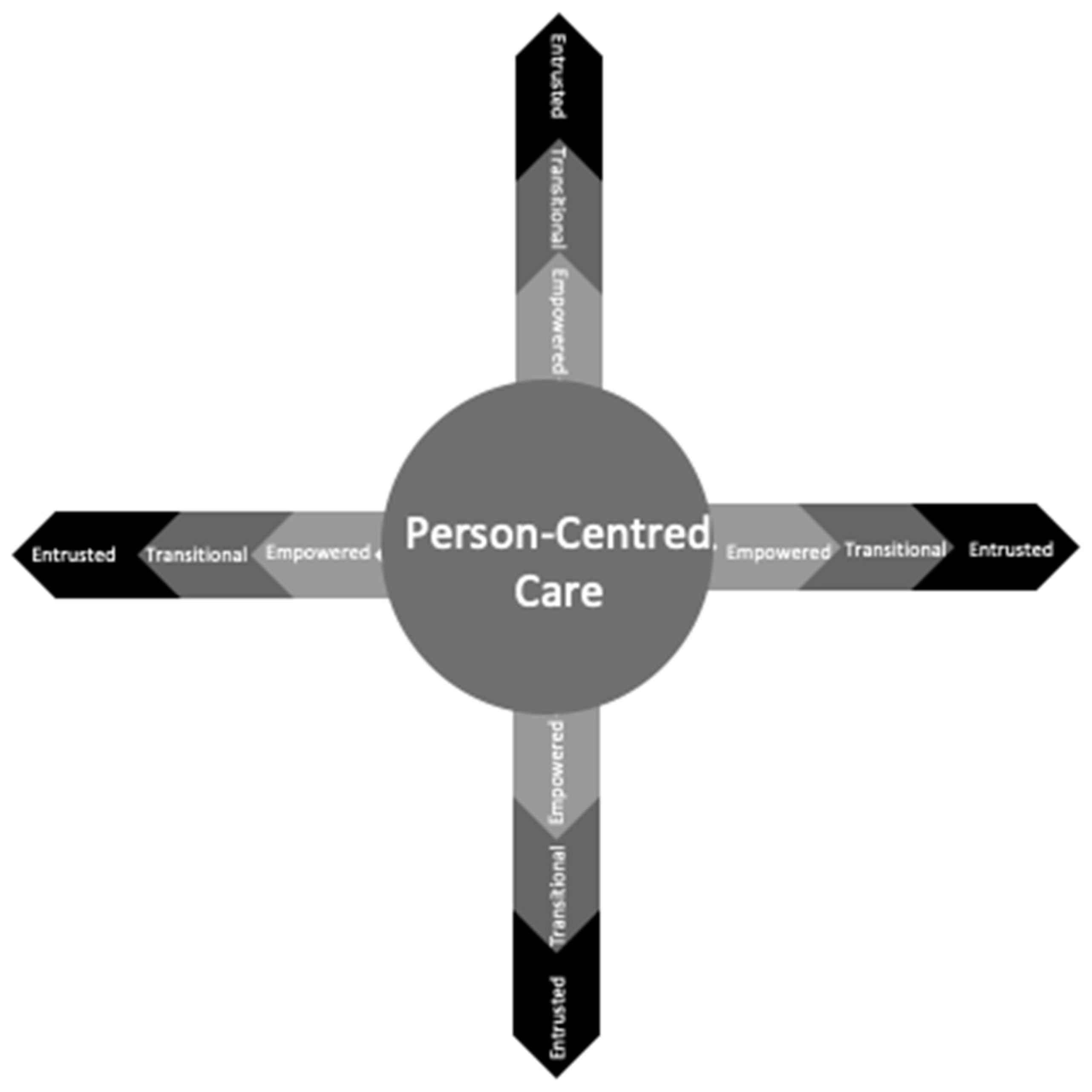
3.4.3. Layer 3: Capability Continuum
Empowered
Transitional
Entrusted
3.4.4. How to Use the Capability Continuum
3.5. COMPASS Mnemonic
3.5.1. Aim and Purpose
- Context—circumstance, situation, place, or time where digital transformation can influence health and social care safety, and quality;
- Optimisation—methodologies adopted to ensure evidence-based therapeutic interventions that influence effective use of digital technologies to prevent, manage, or treat health disorders or diseases;
- Model—plans, designs, implementations, and evaluations which best provide representations of digital technology within health and social care, learning approaches that contribute to safety and quality;
- Person-centred—values, holistic lens and inclusive goals facilitated by digital technology-enabled care, giving individuals authority to better engage with and control their health;
- Analysis—rigour, reliability, and validity ensuring detailed examination of digital transformations in health and social care to understand the nature or determine essential features;
- Systematic—methods required to develop and deliver a transformative approach in digital health and social care that is logical, repeatable, and able to be learned as an organised approach;
- Solution—research impact, transformation, and future directions. The solution resolves a concern using a transformative approach in digital health and social care.
3.5.2. How to Use the COMPASS Mnemonic
4. Discussion
Why the COMPASS Is Different
5. Limitations
6. Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Brice, S.; Almond, H. Health professional digital capabilities frameworks: A scoping review. J. Multidiscip. Healthc. 2020, 13, 1375. [Google Scholar] [CrossRef] [PubMed]
- Fadahunsi, K.P.; O’Connor, S.; Akinlua, J.T.; Wark, P.A.; Gallagher, J.; Carroll, C.; Car, J.; Majeed, A.; O’Donoghue, J. Information Quality Frameworks for Digital Health Technologies: Systematic Review. J. Med. Internet Res. 2021, 23, e23479. [Google Scholar] [CrossRef] [PubMed]
- Stephanie, L.; Sharma, R.S. Digital health eco-systems: An epochal review of practice-oriented research. Int. J. Inf. Manag. 2020, 53, 102032. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce, 2030; World Health Organization: Geneva, Switzerland, 2016; ISBN 9789241511131.
- The Association of Medical Research Charities (AMRC). Navigating the Digital Health Ethics Landscape: A Framework for Understanding Ethical Principles for Digital Health. 2019. Available online: https://www.amrc.org.uk/navigating-the-digital-health-ethics-landscape-a-framework-for-understanding-ethical-principles-for-digital-health (accessed on 3 June 2022).
- Shaw, J.A.; Donia, J. The Sociotechnical Ethics of Digital Health: A Critique and Extension of Approaches From Bioethics. Front. Digit. Health 2021, 3, 725088. [Google Scholar] [CrossRef] [PubMed]
- Arora, C. Digital health fiduciaries: Protecting user privacy when sharing health data. Ethics Inf. Technol. 2019, 21, 181–196. [Google Scholar] [CrossRef] [Green Version]
- Mather, C.; Cummings, E. Promoting participatory health: Connecting nurses and consumers at point of care to enhance safety and quality in Australia. Stud. Health Technol. Inform. 2019, 266, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Aickelin, U.; Chapman, W.; Hart, G. Health Informatics—Ambitions and Purpose. Front. Digit. Health 2019, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathews, S.C.; McShea, M.J.; Hanley, C.L.; Ravitz, A.; Labrique, A.B.; Cohen, A.B. Digital health: A path to validation. NPJ Digit. Med. 2019, 2, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening Research Considerations; No. WHO/RHR/19.9; World Health Organization: Geneva, Switzerland, 2019.
- CANZUK International. CANZUK International: Policies & Campaign Proposals; Archived 5 November 2020, at the Wayback Machine; CANZUK International: Toronto, ON, Canada, 2022. [Google Scholar]
- Armitage, A. Comparing the Policy of Aboriginal Assimilation: Australia, Canada, and New Zealand; UBC Press: Vancouver, BC, Canada, 1995. [Google Scholar]
- Australian Digital Health Agency. National Nursing and Midwifery Digital Health Capability Framework; Australian Government: Sydney, NSW, Australia, 2020.
- Australian Digital Health Agency and the Australian Medical Council. Capability Framework in Digital Health in Medicine; Australian Government: Sydney, NSW, Australia, 2021.
- Department of Health. Digital Health Capability Framework for Allied Health Professionals; Victorian Government: Melbourne, VIC, Australia, 2021.
- Digital Health Canada. Competency Requirements: Health Informatics Professional; Digital Health Canada: Toronto, ON, Canada, 2019. [Google Scholar]
- Health Education England. A Health and Care Digital Capability Framework. 2018. Available online: https://www.hee.nhs.uk/sites/default/files/documents/Digital%20Literacy%20Capability%20Framework%202018.pdf (accessed on 15 April 2022).
- College Development Network. Digital Capability: A Scottish Landscape Review. 2020. Available online: https://www.cdn.ac.uk/ (accessed on 15 April 2022).
- Office of Nursing and Midwifery Services Director and Northern Ireland Practice and Education Council for Nursing and Midwifery. All-Ireland Nursing & Midwifery Digital Health Capability Framework; Office of the Chief Clinical Officer: Dublin, Ireland; NIPEC: Belfast, Ireland, 2020. [Google Scholar]
- Ministry of Health—Manatū Hauora. Digital Health Strategic Framework. New Zealand. Available online: https://www.health.govt.nz/our-work/digital-health/digital-health-strategic-framework#:~:text=The%20Digital%20Health%20Strategic%20Framework,digital%20technologies%20and%20accessible%20data (accessed on 15 April 2022).
- Almond, H. Exploring the Experiences of and Engagement with Australia’s Shared Digital Health Record by People Living with Complex Chronic Conditions in a Rural Community. Doctoral Dissertation, University of Tasmania, Hobart, Australia, 2018. [Google Scholar]
- Kreps, G. Online information and communication systems to enhance health outcomes through communication convergence. Hum. Commun. Res. 2017, 43, 518–530. [Google Scholar] [CrossRef]
- Mather, C.; Cummings, E. Developing and sustaining digital professionalism: A model for assessing readiness of healthcare environments and capability of nurses. BMJ Health Care Inform. 2019, 26, e100062. [Google Scholar] [CrossRef] [Green Version]
- Kushniruk, A.; Nohr, C.; Borycki, E. Human factors for more usable and safer health information technology: Where are we now and where do we go from here? Yearb. Med. Inform. 2016, 25, 120–125. [Google Scholar]
- Touchie, C.; Ten Cate, O. The promise, perils problems and progress of competency-based medical education. Med. Educ. 2016, 50, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Principles of Behavior Modification; Prentice-Hall: New York, NY, USA, 1969; p. 1. [Google Scholar]
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change of smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Title | Profession | Core Purpose | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Domain 6 | Domain 7 |
|---|---|---|---|---|---|---|---|---|---|---|
| Australia 2020 [14] | National Nursing and Midwifery Digital Health Capability Framework | Nursing and Midwifery | Person/woman-centred, safe, quality and connected care | Digital Professionalism | Leadership and Advocacy | Data and Information Quality | Information-enable care | Technology | ||
| Australia 2021 [15] | A Capability Framework in Digital Health in Medicine | Medical education | Culturally safe, people, and value-based care | Professionalism and Interagency Action | Integrated health settings and access | Appraisal and risk | Data and information Quality | Medicine Ethics and law | Future Preparedness | Health System Innovation |
| Australia 2021 [16] | Digital health capability framework for allied health professionals | Allied Health | Safe and high-quality patient care | The digital workplace | Digital Professionalism | Data and informatics | Digital transformation | |||
| Canada 2019 [17] | Digital Health Canada Competency Requirements | Health informatician | Information Management | Technology Eco System | Clinical and Health Services | Canadian Health System | Healthcare Transformation | Project Management | ||
| England 2018 [18] | A Health and Care Digital Capabilities Framework | Health and Care | Person Centre Digital Literacy | Information, data, and content | Teaching and learning and self-development | Communication, collaboration, and participation | Digital identity, wellbeing, safety, and security | Technical proficiency | Creation and innovation and research | |
| Scotland 2020 [19] | Digital Capability: A Scottish Landscape Review | Lecturers | Identifying staff digital skill needs | Who needs what at which level | The development of those skills | Implementing a data-driven approach to learning and teaching | Ensuring an effective and resilient digital infrastructure | |||
| Ireland 2021 [20] | All-Ireland Nursing and Midwifery Digital Health Capability Framework | Nursing and Midwifery | Digital professionalism | Leadership and Advocacy | Data Information and Quality | Information-enable care | Technology | |||
| New Zealand (n.d.) [21] | Digital Health strategic Framework | Public health and disability system | Person and whanau centred. Customer driven | Delivering and improving digital health services ecosystem | Enabling the ecosystem | Digital Environment | Digital and data delivery principles |
| Empowered | Transitional | Entrusted | |
|---|---|---|---|
| Knowledge | Foundational | Proficient | Advanced practice |
| Skills | Able | Discern | Competent/Capable |
| Behaviour/Ability | Receptive | Motivated | Change champion/Leader |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mather, C.; Almond, H. Using COMPASS (Context Optimisation Model for Person-Centred Analysis and Systematic Solutions) Theory to Augment Implementation of Digital Health Solutions. Int. J. Environ. Res. Public Health 2022, 19, 7111. https://doi.org/10.3390/ijerph19127111
Mather C, Almond H. Using COMPASS (Context Optimisation Model for Person-Centred Analysis and Systematic Solutions) Theory to Augment Implementation of Digital Health Solutions. International Journal of Environmental Research and Public Health. 2022; 19(12):7111. https://doi.org/10.3390/ijerph19127111
Chicago/Turabian StyleMather, Carey, and Helen Almond. 2022. "Using COMPASS (Context Optimisation Model for Person-Centred Analysis and Systematic Solutions) Theory to Augment Implementation of Digital Health Solutions" International Journal of Environmental Research and Public Health 19, no. 12: 7111. https://doi.org/10.3390/ijerph19127111
APA StyleMather, C., & Almond, H. (2022). Using COMPASS (Context Optimisation Model for Person-Centred Analysis and Systematic Solutions) Theory to Augment Implementation of Digital Health Solutions. International Journal of Environmental Research and Public Health, 19(12), 7111. https://doi.org/10.3390/ijerph19127111