4.1. Estimation of Incidence Rates of Neonatal and Perinatal Outcomes in the Valencia Region
The occurrence rate of seven perinatal and neonatal outcomes in the Valencia Region has been estimated, building from the results obtained as a part of the WHO-GVS-MCC global study [
10]. Interestingly, all of the previous outcomes were identified during the first week of the life of the newborn.
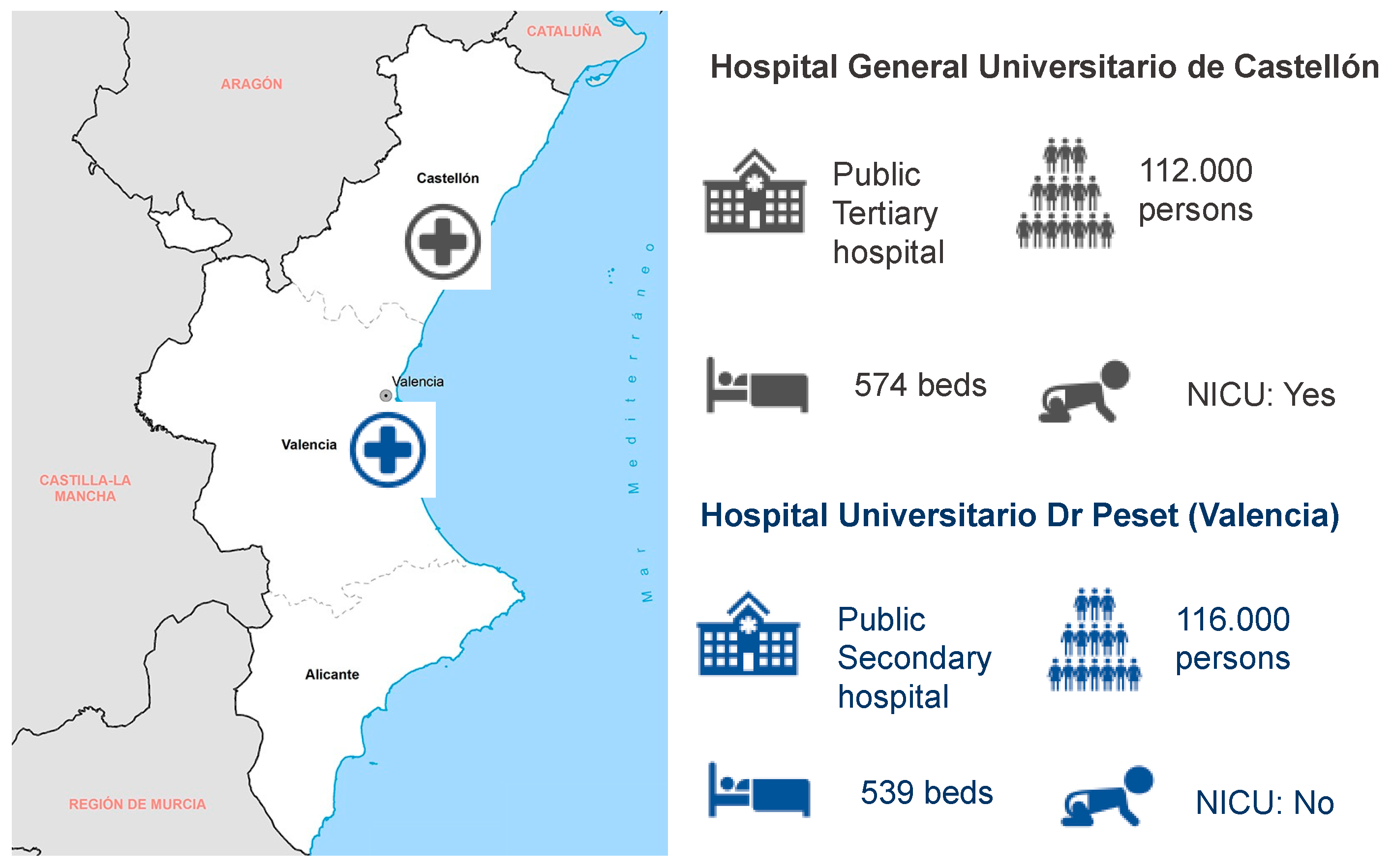
Overall, more than double the outcomes of interest were recruited in Castellón GUH (411), in comparison to Dr. Peset UH (193). This is explained by the nature of the Castellón GUH hospital, which is a reference tertiary hospital. In contrast to Dr. Peset UH, which is a secondary hospital, Castellón GUH hospital has a neonatal intensive care unit. As a consequence, although the catchment population of both hospitals is similar, Castellon GUH also receives the potential preterm neonates corresponding to other secondary hospitals in the Castellon province. This is not the case for the Dr. Peset hospital, which only admits preterm births of >32 weeks of gestation, thus outcomes such as SGA, PTB, or ND are more unlikely.
The data analysis performed in the present study yielded incidence rates of the outcomes of interest for the Valencia region (
Figure 2) that are in line with the previously reported rates in Spain and Europe for the LBW, PTB, SB, and ND outcomes ([
13,
14,
17,
18,
19],
Figure 5). The rates for SGA are also resembling the rates reported for Europe [
15], but we could not find any literature reporting the specific rates for Spain.
Strikingly, in contrast with the previous literature, we observe a higher microcephaly incidence rate (
Figure 5). The incidence rate of congenital microcephaly in the Valencia Region was 13 per 1000 live births at both sites, whereas the incidence of congenital microcephaly previously reported were 0.15 and 0.29 per 1000 live births in Europe and Spain [
16], respectively. The determination of congenital microcephaly is highly dependent on the measuring procedures and the training of the staff at each hospital. Most of the neonatal microcephalies identified are unlikely to be congenital microcephalies (e.g., caused by cytomegalovirus or Zika infection in the mother), but temporary microcephalies produced by cranial molding at birth or other reasons. As a matter of fact, the literature reports that the measurement of the cranial perimeter (CP) is prone to errors, thus the recommendation of measuring at least three times for confirmation of microcephaly [
20].
In Castellón GUH and Dr. Peset UH, the cranial perimeter was measured and registered only once by the nurses (not the pediatricians participating in the study), regardless of the percentile corresponding to the measurement. The lack of a second and third measurement by the pediatricians and the tendency for errors in the CP measurement might be the reason why such a high incidence rate for CM is observed. The doctors reported that most of the cranial perimeter anomalies observed were barely meeting the microcephaly percentile criteria and therefore it is highly unlikely that all of them are real congenital microcephalies. Thus, the incidence rates presented in the results have to be interpreted with caution, as these are probably overestimated.
In Dr. Peset UH, all the mothers of the suspected microcephaly cases are taken a urine sample and tested in the lab for cytomegalovirus, as this is the most frequent reason for congenital microcephaly [
21,
22]. The doctors did not identify any positive cytomegalovirus diagnosis for the CM cases reported in the present study, supporting the hypothesis of measurement errors as the main reason for the higher CM incidence rates.
Finally, it was challenging to find consistent and comparable rates for neonatal infections in Europe and Spain in the existing literature. Thus, we did not provide a comparison for the neonatal infection outcome in
Figure 5. Nevertheless, in comparison with other LMICs also participating in the WHO-GVS-MCC study [
10], the Valencian rates were considerably lower, except for meningitis (
Supplementary Figure S1). It is also worth mentioning two points that might have influenced the incidence rates of infection in the present study:
neonatal infections were not followed-up outside of the facility, therefore, these rates are likely lower than the true rates reported in the present study.
currently, the general procedure, even in the cases of infection suspicion (e.g., after a prolonged premature membrane break), is to not test for microbiological confirmation of the infection, but to monitor the evolution of infection and the neonate constants. Thus, it is likely that some cases of infection have not been reported as such as they did not have a lab confirmation, underestimating the incidence rates reported.
The interpretation of the estimated incidence rates in the Valencia Region should be done with caution, as Castellón GUH is a tertiary referral hospital to which all complicated pregnancies are referred and may show higher rates than the national average reported. Moreover, the identification of SGA, and CM outcomes was not always systematic and standardized, so it is likely that some cases have been missed during the study period, therefore affecting the accuracy of the incidence rates. However, the overall estimations for the two hospitals are still informative and representative of the Valencia Region.
The estimation of the incidence rates of these neonatal outcomes in the Valencia Region is crucial for the post-authorization safety assessment of newly introduced vaccines. This is currently of relevance, as several new vaccines have been recently introduced (e.g., Zika or COVID-19) or will be soon introduced (e.g., RSV) in the immunization schedule of the pregnant women population.
4.2. Applicability of GAIA Definitions to Neonatal Outcomes
From the total number of outcomes screened, Castellón GUH was able to recruit 69% of the cases and Dr. Peset UH recruited 83.4% of the cases. The most common reason for exclusion from the study was the parents refusing to sign the informed consent, especially for those neonates presenting severe outcomes, which were more frequent at Castellón GUH. This was particularly difficult for those neonates admitted to the NICU in the case of the Castellón GUH, which explains the lower percentage of recruitment at the Castellon site. Dr. Peset UH also reported better access to the parents and therefore a swifter informed consent form signature process.
The present results highlighted the high applicability of several of the GAIA definitions to the neonatal outcomes recruited in the Valencian hospitals. The results showed that the case definitions for PTB, LBW, ND, and NI were generally applicable for all the recruited cases, whereas those for SB, CM, and SGA had limited applicability (
Figure 3). These findings are in line with the results obtained in the global WHO-GVS-MCC study [
9,
10].
Even though the applicability of the GAIA definition for NI was high (73.3%-
Figure 3), four of the recruited NI cases were not classified into any of the GAIA diagnostic certainty levels as the lab confirmation of the diagnosis was missing. The reason behind this is that the standard hospital procedure, even in the cases of infection suspicion (e.g., after a prolonged premature membrane break), is to not test at the microbiology lab, but to monitor the evolution of infection and the neonate constants.
None of the SGA cases could be classified in any of the GAIA diagnostic certainty levels for SGA (
Figure 3). The main reason for the misclassification was that the frequency of the balance calibration was unknown, therefore, the GAIA definition considered that the weight was not obtained using appropriate criteria to be classified as level 3. Despite the doctors not being able to determine when exactly the balance was calibrated, it was confirmed that the balance was regularly calibrated by hospital technicians. Consequently, the SGA GAIA definition was considered too strict and will need to be redefined, as the rest of the criteria in the definition were met in all the SGA cases recruited.
Moreover, insufficient information to distinguish between antepartum and intrapartum stillbirth, as there was no record of signs of life prior to the onset of labor and there was very little information on gestational age in that particular case.
With respect to CM, 64% of the recruited cases were not classified into any of the GAIA levels of diagnostic certainty (
Figure 3,
Supplementary Table S1). The most frequent reasons for not meeting the GAIA definition criteria (therefore, unclassified) were that microcephaly was not diagnosed based on the ICD code algorithm (in the 100% of unclassified cases) and that head circumference was not 2SD below mean or the third percentile according to GA and gender on Intergrowth-21 chart (in 88.2% of the unclassified cases) (
Supplementary Table S2).
The use of GAIA case definitions might be challenging in LMIC, as the proposed criteria for some definitions may exceed clinical capacity at some sites [
9,
10]. The fact that the GAIA definitions had limited applicability in a developed country such as Spain, is a clear indication that the definitions will be more challenging to implement in low-medium income countries, with more reduced infrastructure and pregnancy data availability. Consequently, the study highlighted that the definitions have to be revisited and adjusted for a more efficient application at the site level [
11].
4.3. Applicability of GAIA Definitions to Maternal Immunization
Regarding the data for maternal immunization, the vaccination exposure information was collected for the 93.9% of pregnant women, emphasizing the high quality of the Valencian Vaccine Registry. Only 6.1% of the mothers had an unknown vaccination status, and those were either immigrants (with less reliable control of the vaccination during pregnancy) or were vaccinated in private hospitals (therefore no record of their vaccination status in the public Valencian Vaccine Registry).
Furthermore, 86.7% of the pregnant women were vaccinated, proving a high vaccination coverage in this particular subpopulation in the region of Valencia, and overall in Spain.
The level 1–2 criteria “immunization recorded in medical records by a health care worker who administered/witnessed the administration of vaccine” was interpreted as primary source medical records, such as the ANC card, vaccine card, or vaccine register. Secondary source medical records, such as the case sheet or the birth recorded, were accepted in level 3.
Several aspects of the definition relating to the vaccine and disease were open to interpretation. For level 1, “date/time” was interpreted as both date and time of administration, and “details of vaccine” as the vaccine lot number, and either the name of the disease or the name of the vaccine. For level 2, “details of the disease” were interpreted as either the name of the disease or the name of the vaccine, or the lot number were required. To ensure standardization between studies, these aspects of the definition should be further specified.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}