
Effects of Different Exercise Therapies on Balance Function and Functional Walking Ability in Multiple Sclerosis Disease Patients—A Network Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Outcomes
2.5. Study Selection
2.6. Data Extraction
2.7. Risk of Bias of Individual Studies
2.8. Data Analysis
3. Results
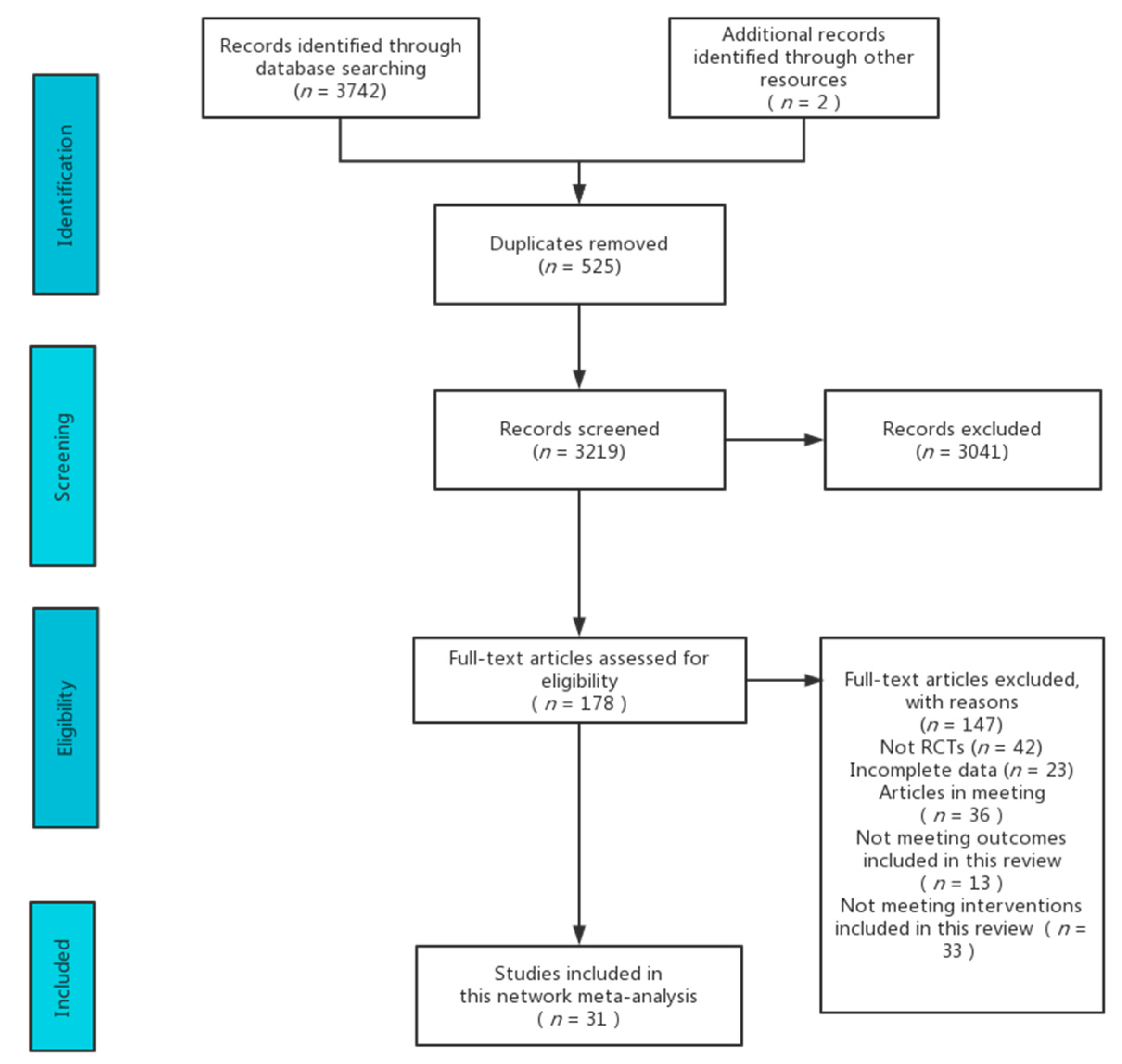
3.1. Study Identification and Selection
3.2. Characteristics of the Included Studies
3.3. Quality Assessment of the Included Studies
3.4. Network Meta-Analysis
3.4.1. Berg Balance Scale (BBS)
3.4.2. Timed-Up-and-Go Score (TUG)
3.5. Publication Bias
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple Sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Correale, J.; Gaitan, M.I.; Ysrraelit, M.C.; Fiol, M.P. Progressive multiple sclerosis: From pathogenic mechanisms to treatment. Brain 2017, 140, 527–546. [Google Scholar] [CrossRef] [PubMed]
- Ontaneda, D.; Thompson, A.J.; Fox, R.J.; Cohen, J.A. Progressive multiple sclerosis: Prospects for disease therapy, repair, and restoration of function. Lancet 2017, 389, 1357–1366. [Google Scholar] [CrossRef]
- Freiha, J.; Riachi, N.; Chalah, M.A.; Zoghaib, R.; Ayache, S.S.; Ahdab, R. Paroxysmal Symptoms in Multiple Sclerosis—A Review of the Literature. J. Clin. Med. 2020, 9, 3100. [Google Scholar] [CrossRef]
- Brownlee, W.J.; Hardy, T.A.; Fazekas, F.; Miller, D.H. Diagnosis of multiple sclerosis: Progress and challenges. Lancet 2017, 389, 1336–1346. [Google Scholar] [CrossRef]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef]
- Dymecka, J.; Gerymski, R.; Tataruch, R.; Bidzan, M. Sense of Coherence and Health-Related Quality of Life in Patients with Multiple Sclerosis: The Role of Physical and Neurological Disability. J. Clin. Med. 2022, 11, 1716. [Google Scholar] [CrossRef]
- Comber, L.; Coote, S.; Finlayson, M.; Galvin, R.; Quinn, G.; Peterson, E. An exploration of fall-related, psychosocial variables in people with multiple sclerosis who have fallen. Br. J. Occup. Ther. 2017, 80, 587–595. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M.; Kwakkel, G.; Dalgas, U.; Feinstein, A.; Heesen, C.; Feys, P.; Thompson, A.J. Exercise in patients with multiple sclerosis. Lancet Neurol. 2017, 16, 848–856. [Google Scholar] [CrossRef]
- Akkan, H.; Kallem Seyyar, G.; Aslan, B.; Karabulut, E. The effect of virtual reality-based therapy on fear of falling in multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2022, 63, 103791. [Google Scholar] [CrossRef]
- Abou, L.; Qin, K.; Alluri, A.; Du, Y.; Rice, L.A. The effectiveness of physical therapy interventions in reducing falls among people with multiple sclerosis: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2022, 29, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Torres-Costoso, A.; Martinez-Vizcaino, V.; Reina-Gutierrez, S.; Alvarez-Bueno, C.; Guzman-Pavon, M.J.; Pozuelo-Carrascosa, D.P.; Fernandez-Rodriguez, R.; Sanchez-Lopez, M.; Cavero-Redondo, I. Effect of Exercise on Fatigue in Multiple Sclerosis: A Network Meta-analysis Comparing Different Types of Exercise. Arch. Phys. Med. Rehabil. 2022, 103, 970. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.M.; Safari, R.; Mercer, T.; Picariello, F.; van der Linden, M.L.; White, C.; Moss-Morris, R.; Norton, S. Which exercise and behavioural interventions show most promise for treating fatigue in multiple sclerosis? A network meta-analysis. Mult. Scler. J. 2021, 27, 1657–1678. [Google Scholar] [CrossRef] [PubMed]
- Rouse, B.; Chaimani, A.; Li, T. Network meta-analysis: An introduction for clinicians. Intern. Emerg. Med. 2017, 12, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The Timed up and Go—A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Park, S.-H. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Nascimento, A.S.; Fagundes, C.V.; Mendes, F.A.D.S.; Leal, J.C. Effectiveness of Virtual Reality Rehabilitation in Persons with Multiple Sclerosis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Mult. Scler. Relat. Disord. 2021, 54, 103128. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Jueni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ-Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef]
- Hopp, L. Risk of bias reporting in Cochrane systematic reviews. Int. J. Nurs. Pract. 2015, 21, 683–686. [Google Scholar] [CrossRef]
- Chaimani, A.; Higgins, J.P.T.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical Tools for Network Meta-Analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef] [PubMed]
- Vats, D.; Flegal, J.M.; Jones, G.L. Multivariate output analysis for Markov chain Monte Carlo. Biometrika 2019, 106, 321–337. [Google Scholar] [CrossRef]
- Marotta, N.; Demeco, A.; Moggio, L.; Marinaro, C.; Pino, I.; Barletta, M.; Petraroli, A.; Pepe, D.; Lavano, F.; Ammendolia, A. Comparative effectiveness of breathing exercises in patients with chronic obstructive pulmonary disease. Complement. Ther. Clin. Pract. 2020, 41, 101260. [Google Scholar] [CrossRef]
- Kara, B.; Küçük, F.; Poyraz, E.C.; Tomruk, M.S.; İdıman, E. Different types of exercise in Multiple Sclerosis: Aerobic exercise or Pilates, a single-blind clinical study. J. Back Musculoskelet. Rehabil. 2017, 30, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Gheitasi, M.; Bayattork, M.; Andersen, L.L.; Imani, S.; Daneshfar, A. Effect of twelve weeks pilates training on functional balance of male patients with multiple sclerosis: Randomized controlled trial. J. Bodyw. Mov. Ther. 2021, 25, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Küçük, F.; Kara, B.; Poyraz, E.Ç.; İdiman, E. Improvements in cognition, quality of life, and physical performance with clinical Pilates in multiple sclerosis: A randomized controlled trial. J. Phys. Ther. Sci. 2016, 28, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Kalron, A.; Rosenblum, U.; Frid, L.; Achiron, A. Pilates exercise training vs. physical therapy for improving walking and balance in people with multiple sclerosis: A randomized controlled trial. Clin. Rehabil. 2017, 31, 319–328. [Google Scholar] [CrossRef]
- Asvar, S.; Taghian, F. The Effect of an Eight-week Pilates Training on Interleukine-18 Level, Fatigue, and Balance in Women With Multiple Sclerosis. J. Res. Health 2020, 10, 383–392. [Google Scholar] [CrossRef]
- Abasıyanık, Z.; Ertekin, Ö.; Kahraman, T.; Yigit, P.; Özakbaş, S. The effects of Clinical Pilates training on walking, balance, fall risk, respiratory, and cognitive functions in persons with multiple sclerosis: A randomized controlled trial. EXPLORE 2020, 16, 12–20. [Google Scholar] [CrossRef]
- Guclu-Gunduz, A.; Citaker, S.; Irkec, C.; Nazliel, B.; Batur-Caglayan, H.Z. The effects of pilates on balance, mobility and strength in patients with multiple sclerosis. NeuroRehabilitation 2014, 34, 337–342. [Google Scholar] [CrossRef]
- Alguacil Diego, I.M.; Pedrero Hernández, C.; Molina Rueda, F.; Cano de la Cuerda, R. Effects of vibrotherapy on postural control, functionality and fatigue in multiple sclerosis patients: A randomised clinical trial. Neurology 2012, 27, 143–153. [Google Scholar] [CrossRef]
- Schuhfried, O.; Mittermaier, C.; Jovanovic, T.; Pieber, K.; Paternostro-Sluga, T. Effects of whole-body vibration in patients with multiple sclerosis: A pilot study. Clin. Rehabil. 2005, 19, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Broekmans, T.; Roelants, M.; Alders, G.; Feys, P.; Thijs, H.; Eijnde, B.O. Exploring the effects of a 20-week whole-body vibration training programme on leg muscle performance and function in persons with multiple sclerosis. J. Rehabil. Med. 2010, 42, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Aidar, F.J.; Gama de Matos, D.; de Souza, R.F.; Gomes, A.B.; Saavedra, F.; Garrido, N.; Carneiro, A.L.; Reis, V. Influence of aquatic exercises in physical condition in patients with multiple sclerosis. J. Sports Med. Phys. Fit. 2018, 58, 684–689. [Google Scholar] [CrossRef]
- Kargarfard, M.; Shariat, A.; Ingle, L.; Cleland, J.A.; Kargarfard, M. Randomized Controlled Trial to Examine the Impact of Aquatic Exercise Training on Functional Capacity, Balance, and Perceptions of Fatigue in Female Patients With Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2018, 99, 234–241. [Google Scholar] [CrossRef]
- Young, H.J.; Mehta, T.S.; Herman, C.; Wang, F.; Rimmer, J.H. The Effects of M2M and Adapted Yoga on Physical and Psychosocial Outcomes in People With Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2019, 100, 391–400. [Google Scholar] [CrossRef]
- de Oliveira, G.; Tavares, M.D.C.C.G.F.; de Faria Oliveira, J.D.; Rodrigues, M.R.; Santaella, D.F. Yoga Training Has Positive Effects on Postural Balance and Its Influence on Activities of Daily Living in People with Multiple Sclerosis: A Pilot Study. EXPLORE 2016, 12, 325–332. [Google Scholar] [CrossRef]
- Straudi, S.; Martinuzzi, C.; Pavarelli, C.; Sabbagh Charabati, A.; Benedetti, M.G.; Foti, C.; Bonato, M.; Zancato, E.; Basaglia, N. A task-oriented circuit training in multiple sclerosis: A feasibility study. BMC Neurol. 2014, 14, 124. [Google Scholar] [CrossRef]
- Ahmadi, A.; Arastoo, A.A.; Nikbakht, M.; Zahednejad, S.; Rajabpour, M. Comparison of the Effect of 8 weeks Aerobic and Yoga Training on Ambulatory Function, Fatigue and Mood Status in MS Patients. Iran. Red Crescent Med. J. 2013, 15, 449–454. [Google Scholar] [CrossRef]
- Cakit, B.D.; Nacir, B.; Genç, H.; Saraçoglu, M.; Karagöz, A.; Erdem, H.R.; Ergün, U. Cycling Progressive Resistance Training for People with Multiple Sclerosis: A Randomized Controlled Study. Am. J. Phys. Med. Rehabil. 2010, 89, 446–457. [Google Scholar] [CrossRef]
- Orban, A.; Garg, B.; Sammi, M.K.; Bourdette, D.N.; Rooney, W.D.; Kuehl, K.; Spain, R.I. Effect of High-Intensity Exercise on Multiple Sclerosis Function and Phosphorous Magnetic Resonance Spectroscopy Outcomes. Med. Sci. Sports Exerc. 2019, 51, 1380–1386. [Google Scholar] [CrossRef] [PubMed]
- Gervasoni, E.; Cattaneo, D.; Jonsdottir, J. Effect of treadmill training on fatigue in multiple sclerosis: A pilot study. Int. J. Rehabil. Res. Int. Z. Rehabil. Rev. Int. Rech. Readapt. 2013, 37. [Google Scholar] [CrossRef] [PubMed]
- Tollár, J.; Nagy, F.; Tóth, B.E.; Török, K.; Szita, K.; Csutorás, B.; Moizs, M.; Hortobágyi, T. Exercise Effects on Multiple Sclerosis Quality of Life and Clinical-Motor Symptoms. Med. Sci. Sports Exerc. 2020, 52, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, A.; Arastoo, A.; Nikbakht, M. The effects of a treadmill training programme on balance, speed and endurance walking, fatigue and quality of life in people with multiple sclerosis. Int. SportMed J. 2010, 11, 389–397. [Google Scholar]
- Straudi, S.; Fanciullacci, C.; Martinuzzi, C.; Pavarelli, C.; Rossi, B.; Chisari, C.; Basaglia, N. The effects of robot-assisted gait training in progressive multiple sclerosis: A randomized controlled trial. Mult. Scler. 2016, 22, 373–384. [Google Scholar] [CrossRef]
- Moradi, M.; Sahraian, M.A.; Aghsaie, A.; Kordi, M.R.; Meysamie, A.; Abolhasani, M.; Sobhani, V. Effects of Eight-week Resistance Training Program in Men With Multiple Sclerosis. Asian J. Sports Med. 2015, 6. [Google Scholar] [CrossRef]
- Aidar, F.J.; Carneiro, A.L.; Costa Moreira, O.; Patrocínio de Oliveira, C.E.; Garrido, N.D.; Machado Reis, V.; Raineh, I.; Vilaça, J.M.; Gama de Matos, D. Effects of resistance training on the physical condition of people with multiple sclerosis. J. Sports Med. Phys. Fit. 2018, 58, 1127–1134. [Google Scholar] [CrossRef]
- Moghadasi, A.; Ghasemi, G.; Sadeghi-Demneh, E.; Etemadifar, M. The Effect of Total Body Resistance Exercise on Mobility, Proprioception, and Muscle Strength of the Knee in People With Multiple Sclerosis. J. Sport Rehabil. 2020, 29, 192–199. [Google Scholar] [CrossRef]
- Yazgan, Y.Z.; Tarakci, E.; Tarakci, D.; Ozdincler, A.R.; Kurtuncu, M. Comparison of the effects of two different exergaming systems on balance, functionality, fatigue, and quality of life in people with multiple sclerosis: A randomized controlled trial. Mult. Scler. Relat. Disord. 2020, 39, 101902. [Google Scholar] [CrossRef]
- Molhemi, F.; Monjezi, S.; Mehravar, M.; Shaterzadeh-Yazdi, M.-J.; Salehi, R.; Hesam, S.; Mohammadianinejad, E. Effects of Virtual Reality vs Conventional Balance Training on Balance and Falls in People With Multiple Sclerosis: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2021, 102, 290–299. [Google Scholar] [CrossRef]
- Khalil, H.; Al-Sharman, A.; El-Salem, K.; Alghwiri, A.A.; Al-Shorafat, D.; Khazaaleh, S.; Abu Foul, L. The development and pilot evaluation of virtual reality balance scenarios in people with multiple sclerosis (MS): A feasibility study. NeuroRehabilitation 2018, 43, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Brichetto, G.; Spallarossa, P.; de Carvalho, M.L.L.; Battaglia, M.A. The effect of Nintendo® Wii® on balance in people with multiple sclerosis: A pilot randomized control study. Mult. Scler. 2013, 19, 1219–1221. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Quilis, J.-A.; Gil-Gómez, H.; Gil-Gómez, J.-A.; Albiol-Pérez, S.; Palacios-Navarro, G.; Fardoun, H.M.; Mashat, A.S. Virtual Rehabilitation for Multiple Sclerosis Using a Kinect-Based System: Randomized Controlled Trial. JMIR Serious Games 2014, 2, e2933. [Google Scholar] [CrossRef] [PubMed]
- van Aert, R.C.M.; Wicherts, J.M.; van Assen, M.A.L.M. Publication bias examined in meta-analyses from psychology and medicine: A meta-meta-analysis. PLoS ONE 2019, 14, e0215052. [Google Scholar] [CrossRef]
- Momsen, A.-M.H.; Ortenblad, L.; Maribo, T. Effective rehabilitation interventions and participation among people with multiple sclerosis: An overview of reviews. Ann. Phys. Rehabil. Med. 2022, 65, 101529. [Google Scholar] [CrossRef]
- Legault, Z.; Znaty, A.; Smith, S.; Boudrias, M.-H. Yoga Interventions Used for the Rehabilitation of Stroke, Parkinson’s Disease, and Multiple Sclerosis: A Scoping Review of Clinical Research. J. Altern. Complement. Med. 2021, 27, 1023–1057. [Google Scholar] [CrossRef]
- Luu, K.; Hall, P.A. Hatha Yoga and Executive Function: A Systematic Review. J. Altern. Complement. Med. 2016, 22, 125–133. [Google Scholar] [CrossRef]
- Quinn, G.; Comber, L.; McGuigan, C.; Galvin, R.; Coote, S. Discriminative ability and clinical utility of the Timed Up and Go (TUG) in identifying falls risk in people with multiple sclerosis: A prospective cohort study. Clin. Rehabil. 2019, 33, 317–326. [Google Scholar] [CrossRef]
- Corvillo, I.; Varela, E.; Armijo, F.; Alvarez-Badillo, A.; Armijo, O.; Maraver, F. Efficacy of aquatic therapy for multiple sclerosis: A systematic review. Eur. J. Phys. Rehabil. Med. 2017, 53, 944–952. [Google Scholar] [CrossRef]
- Cohen, E.T.; Cleffi, N.; Ingersoll, M.; Karpatkin, H. Blood-Flow Restriction Training for a Person With Primary Progressive Multiple Sclerosis: A Case Report. Phys. Ther. 2021, 101, pzaa224. [Google Scholar] [CrossRef]
- Amedoro, A.; Berardi, A.; Conte, A.; Pelosin, E.; Valente, D.; Maggi, G.; Tofani, M.; Galeoto, G. The effect of aquatic physical therapy on patients with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2020, 41, 102022. [Google Scholar] [CrossRef] [PubMed]
- Salem, Y.; Scott, A.H.; Karpatkin, H.; Concert, G.; Haller, L.; Kaminsky, E.; Weisbrot, R.; Spatz, E. Community-based group aquatic programme for individuals with multiple sclerosis: A pilot study. Disabil. Rehabil. 2011, 33, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Becker, B.E. Aquatic Therapy in Contemporary Neurorehabilitation: An Update. PM&R 2020, 12, 1251–1259. [Google Scholar] [CrossRef]
- Plecash, A.R.; Leavitt, B.R. Aquatherapy for neurodegenerative disorders. J. Huntingt. Dis. 2014, 3, 5–11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| #1 | Search “Multiple Sclerosis” [MeSh] |
| #2 | Search (Multiple Sclerosis [Title/Abstract]) OR (MS [Title/Abstract]) OR (Relapsing-remitting Multiple Sclerosis [Title/Abstract]) OR (RRMS [Title/Abstract]) OR (Multilocular Sclerosis [Title/Abstract]) |
| #3 | Search #1 OR #2 |
| #4 | Search “Exercise” [MeSh] |
| #5 | Search (exercise [Title/Abstract]) OR (exercise intervention [Title/Abstract]) OR (exercise training [Title/Abstract]) OR (training [Title/Abstract]) OR (physical training [Title/Abstract]) OR (physical exercise [Title/Abstract]) OR (sports training [Title/Abstract]) OR (nurse intervention [Title/Abstract] |
| #6 | Search #4 OR #5 |
| #7 | Search #3 AND #6 |
| Author | Country | Year | Age (Mean + SD) | Total/Man/Woman | Intervention 1/Length (Weeks)/Frequency (Weeks)/Duration (Minutes) | Intervention 2/Length (Weeks)/Frequency (Weeks)/Duration (Minutes) | Control Group | Outcome |
|---|---|---|---|---|---|---|---|---|
| Ahmadi | Iran | 2010 | T: 36.8 (9.17) C: 36.7 (9.32) | T: 10/NA/NA C: 10/NA/NA | Aerobic training 8 weeks 3 times a week 30 min | NA | No exercise | BBS |
| Ahmadi | Iran | 2013 | T1: 36.8 (9.17) T2: 32.27 (8.68) C: 36.7 (9.32) | T1: 10/NA/NA T2: 11/NA/NA C: 10/NA/NA | Aerobic training 8 weeks 3 times a week 30 min | Yoga training 8 weeks 3 times a week 60 min | No exercise | BBS |
| Gervasoni | Italy | 2014 | T: 49.6 (9.4) C: 45.7 (8.9) | T: 15/NA/NA C: 15/NA/NA | Aerobic training 2 weeks 6 times a week 45 min | NA | No exercise | BBS |
| Straudi | Italy | 2015 | T: 52.26 (11.11) C: 54.12 (11.44) | T: 27/10/17 C: 25/8/17 | Aerobic training 2 weeks 2 times a week 30 min | NA | Usual care | BBS, TUG |
| Tollar | Hungary | 2019 | T: 48.1 (5.65) C: 44.4 (6.76) | T: 14/1/13 C: 12/1/11 | Aerobic training 5 weeks 5 times a week 40 min | No exercise | BBS | |
| Cakt | Turkey | 2010 | T1: 36.4 (10.5) T2: 35.5 (10.9) C: 43 (10.2) | T1: 14/5/9 T2: 9/3/6 C: 10/2/8 | Aerobic training 8 weeks 2 times a week 20 min | Resistance training 8 weeks 2 times a week 20 min | No exercise | TUG |
| Orban | USA | 2019 | T: 44.7 (9.4) C: 48.7 (8.4) | T: 10/1/9 C: 7/2/5 | Aerobic training 8 weeks 4 times a week 30 min | No exercise | TUG | |
| Straudi | Italy | 2013 | T: 49.92 (7.51) C: 55.25 (13.82) | T: 12/5/7 C: 12/2/10 | Aerobic training 6 weeks 2 times a week 30 min | No exercise | TUG | |
| Asvar | Iran | 2020 | T: 32.1 (13) C: 33.9 (6) | T: 15/0/15 C: 15/0/15 | Pilates training 8 weeks 3 times a week 60 min | No exercise | BBS | |
| Gheitasi | Iran | 2020 | T: 30.6 (5.27) C: 32.1 (6.3) | T: 15/15/0 C: 15/15/0 | Pilates training 12 weeks 3 times a week 50 min | No exercise | BBS, TUG | |
| Gunduz | Turkey | 2014 | T: 36 (29-40) C:36 (27-45) | T: 18/NA/NA C: 8/NA/NA | Pilates training 8 weeks 2 times a week 60 min | Usual care | BBS, TUG | |
| Karlon | Israel | 2016 | T: 42.9 (7.2) C: 44.3 (6.6) | T: 23/8/14 C: 22/8/15 | Pilates training 12 weeks 1 time a week 30 min | Usual care | BBS, TUG | |
| Kara | Turkey | 2017 | T1: 49.77 (8.95) T2: 43.03 (10.26) C: 44.42 (5.98) | T1: 9/NA/NA T2: 26/NA/NA C: 21/NA/NA | Pilates training 8 weeks 2 times a week 45 min | Aerobic training 8 weeks 2 times a week 45 min | No exercise | BBS |
| Kucuk | Turkey | 2016 | T: 47.2 (9.5) C: 49.7 (8.9) | T: 11/NA/NA C: 9/NA/NA | Pilates training 8 weeks 2 times a week 60 min | Usual care | BBS | |
| Zuhal | Turkey | 2019 | T: 42.5 (6.76) C: 48.24 (11.79) | T: 16/NA/NA C: 17/NA/NA | Pilates training 8 weeks 3 times a week 60 min | Usual care | TUG | |
| Gerson | Brazil | 2016 | T: 46 (8) C: 45 (9) | T: 6/NA/NA C: 6/NA/NA | Yoga training 24 weeks 2 times a week 60 min | No exercise | BBS | |
| Yazgan | Turkey | 2020 | T: 47.76 (10.53) C: 40.66 (8.82) | T: 15/2/13 C: 15/2/13 | VR training (Nintendo® Wii®) 8 weeks 2 times a week 60 min | No exercise | BBS, TUG | |
| Khalil | Jordan | 2019 | T: 39.88 (12.75) C: 34.87 (8.98) | T: 16/4/12 C: 16/6/10 | VR training (VR scenarios) 6 weeks 3 times a week 30 min | Usual care | BBS, TUG | |
| Brichetto | Italy | 2013 | NA | T: 18/NA/NA C: 18/NA/NA | VR training (Nintendo® Wii®) 4 weeks 3 times a week 60 min | Usual care | BBS | |
| Lozana | Spain | 2014 | T: 48.33 (10.82) C: 40.6 (9.24) | T: 6/3/3 C: 5/4/1 | VR training (Kinect games) 10 weeks 1 time a week 60 min | No exercise | BBS, TUG | |
| Molhemi | Iran | 2020 | T: 36.8 (8.4) C: 41.6 (8.4) | T: 19/7/12 C: 20/8/12 | VR training (Kinect games) 6 weeks 3 times a week 35 min | Usual care | BBS, TUG | |
| Tollar | Hungary | 2019 | T: 48.2 (5.48) C: 44.4 (6.76) | T: 14/2/12 C: 12/1/11 | VR training (Nintendo® Wii®) 5 weeks 5 times a week 40 min | No exercise | BBS | |
| Aidar | Brazil | 2018 | T: 41.3 (7.3) C: 43.6 (7.6) | T: 13/4/9 C: 13/5/8 | Aquatic training 12 weeks 3 times a week 45–60 min | No exercise | BBS, TUG | |
| Kargarfard | Iran | 2017 | T: 36.5 (9) C: 36.2 (7.4) | T: 17/NA/NA C: 15/NA/NA | Aquatic training 8 weeks 3 times a week 60 min | No exercise | BBS | |
| Aidar | Brazil | 2018 | T: 42.8 (8) C: 43.6 (7.7) | T: 11/4/7 C: 12/4/8 | Resistance training 12 weeks 3 times a week 45–60 min | No exercise | BBS, TUG | |
| Moradi | Iran | 2015 | T: 34.38 (11.07) C: 33.13 (7.08) | T: 8/NA/NA C: 10/NA/NA | Resistance training 8 weeks 6 times a week 30 min | No exercise | TUG | |
| Moghadasi | Iran | 2020 | T: 37.62 (4.58) C: 34.72 (5.01) | T: 16/NA/NA C: 11/NA/NA | Resistance training 8 weeks 3 times a week 30 min | No exercise | TUG | |
| Alguacil | Spain | 2012 | T: 44 (20) C: 43 (17) | T: 15/7/8 C: 17/9/8 | Whole-body vibration training 5 days 1 time a day 10 min | No exercise | BBS, TUG | |
| Broekmans | Belgium | 2010 | T: 46.1 (2.1) C: 49.7 (3.3) | T: 11/7/4 C: 14//11/3 | Whole-body vibration training 20 weeks 2 times a week 10 min | No exercise | TUG | |
| Schuhfried | Austria | 2005 | T: 49.3 (13.3) C: 46 (12.7) | T: 6/1/5 C: 6/2/4 | Whole-body vibration training 2 weeks 4 times a week 15 min | Usual care | TUG | |
| Young | USA | 2018 | T: 48.35 (9.95) C: 47.29 (10.33) | T: 26/6/20 C: 29/4/24 | Yoga training 8 weeks 3 times a week 40 min | No exercise | TUG |
| YOGA | VR | AEO | AQU | RT | PILATES | WBV | CON |
|---|---|---|---|---|---|---|---|
| YOGA | −1.38 (−4.92, 2.16) | −1.49 (−4.92, 1.93) | −2.07 (−6.42, 2.28) | −2.06 (−8.83, 4.70) | −2.80 (−6.35, 0.76) | −3.05 (−9.42, 3.31) | −5.50 (−8.45, −2.55) |
| 1.38 (−2.16, 4.92) | VR | −0.11 (−3.09, 2.86) | −0.69 (−4.44, 3.07) | −0.68 (−7.08, 5.72) | −1.42 (−4.22, 1.39) | −1.67 (−7.65, 4.30) | −4.12 (−6.09, −2.15) |
| 1.49 (−1.93, 4.92) | 0.11 (−2.86, 3.09) | AEO | −0.58 (−4.46, 3.31) | −0.57 (−7.04, 5.90) | −1.30 (−4.24, 1.63) | −1.56 (−7.61, 4.49) | −4.01 (−6.20, −1.81) |
| 2.07 (−2.28, 6.42) | 0.69 (−3.07, 4.44) | 0.58 (−3.31, 4.46) | AQU | 0.01 (−6.87, 6.89) | −0.73 (−4.50, 3.04) | −0.98 (−7.47, 5.50) | −3.43 (−6.63, −0.23) |
| 2.06 (−4.70, 8.83) | 0.68 (−5.72, 7.08) | 0.57 (−5.90, 7.04) | −0.01 (−6.89, 6.87) | RT | −0.74 (−7.14, 5.67) | −0.99 (−9.29, 7.31) | −3.44 (−9.53, 2.65) |
| 2.80 (−0.76, 6.35) | 1.42 (−1.39, 4.22) | 1.30 (−1.63, 4.24) | 0.73 (−3.04, 4.50) | 0.74 (−5.67, 7.14) | PILATES | −0.25 (−6.24, 5.73) | −2.70 (−4.69, −0.71) |
| 3.05 (−3.31, 9.42) | 1.67 (−4.30, 7.65) | 1.56 (−4.49, 7.61) | 0.98 (−5.50, 7.47) | 0.99 (−7.31, 9.29) | 0.25 (−5.73, 6.24) | WBV | −2.45 (−8.09, 3.19) |
| 5.50 (2.55, 8.45) | 4.12 (2.15, 6.09) | 4.01 (1.81, 6.20) | 3.43 (0.23, 6.63) | 3.44 (−2.65, 9.53) | 2.70 (0.71, 4.69) | 2.45 (−3.19, 8.09) | CON |
| AQU | AEO | VR | PILATES | WBV | YOGA | RT | CON |
|---|---|---|---|---|---|---|---|
| AQU | 1.05 (−2.34, 4.44) | 1.13 (−2.32, 4.58) | 1.22 (−2.11, 4.56) | 1.48 (−1.95, 4.92) | 2.28 (−6.86, 11.42) | 1.79 (−1.59, 5.18) | 2.58 (−0.72, 5.88) |
| −1.05 (−4.44, 2.34) | AEO | 0.08 (−1.20, 1.36) | 0.17 (−0.76, 1.10) | 0.43 (−0.80, 1.66) | 1.23 (−7.33, 9.79) | 0.74 (−0.19, 1.67) | 1.53 (0.75, 2.31) |
| −1.13 (−4.58, 2.32) | −0.08 (−1.36, 1.20) | VR | 0.09 (−1.00, 1.19) | 0.35 (−1.04, 1.74) | 1.15 (−7.43, 9.73) | 0.66 (−0.63, 1.95) | 1.45 (0.45, 2.45) |
| −1.22 (−4.56, 2.11) | −0.17 (−1.10, 0.76) | −0.09 (−1.19, 1.00) | PILATES | 0.26 (−0.82, 1.34) | 1.06 (−7.48, 9.59) | 0.57 (−0.41, 1.55) | 1.36 (0.88, 1.83) |
| −1.48 (−4.92, 1.95) | −0.43 (−1.66, 0.80) | −0.35 (−1.74, 1.04) | −0.26 (−1.34, 0.82) | WBV | 0.80 (−7.78, 9.38) | 0.31 (−0.88, 1.51) | 1.10 (0.15, 2.05) |
| −2.28 (−11.42, 6.86) | −1.23 (−9.79, 7.33) | −1.15 (−9.73, 7.43) | −1.06 (−9.59, 7.48) | −0.80 (−9.38, 7.78) | YOGA | −0.49 (−9.05, 8.07) | 0.30 (−8.22, 8.82) |
| −1.79 (−5.18, 1.59) | −0.74 (−1.67, 0.19) | −0.66 (−1.95, 0.63) | −0.57 (−1.55, 0.41) | −0.31 (−1.51, 0.88) | 0.49 (−8.07, 9.05) | RT | 0.79 (0.02, 1.55) |
| −2.58 (−5.88, −0.72) | −1.53 (−2.31, −0.75) | −1.45 (−2.45, −0.45) | −1.36 (−1.83, −0.88) | −1.10 (−2.05, −0.15) | −0.30 (−8.82, 8.22) | −0.79 (−1.55, −0.02) | CON |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hao, Z.; Zhang, X.; Chen, P. Effects of Different Exercise Therapies on Balance Function and Functional Walking Ability in Multiple Sclerosis Disease Patients—A Network Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 7175. https://doi.org/10.3390/ijerph19127175
Hao Z, Zhang X, Chen P. Effects of Different Exercise Therapies on Balance Function and Functional Walking Ability in Multiple Sclerosis Disease Patients—A Network Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2022; 19(12):7175. https://doi.org/10.3390/ijerph19127175
Chicago/Turabian StyleHao, Zikang, Xiaodan Zhang, and Ping Chen. 2022. "Effects of Different Exercise Therapies on Balance Function and Functional Walking Ability in Multiple Sclerosis Disease Patients—A Network Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 19, no. 12: 7175. https://doi.org/10.3390/ijerph19127175
APA StyleHao, Z., Zhang, X., & Chen, P. (2022). Effects of Different Exercise Therapies on Balance Function and Functional Walking Ability in Multiple Sclerosis Disease Patients—A Network Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 19(12), 7175. https://doi.org/10.3390/ijerph19127175