
The Role of Personalization in the User Experience, Preferences and Engagement with Virtual Reality Environments for Relaxation

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods and Materials
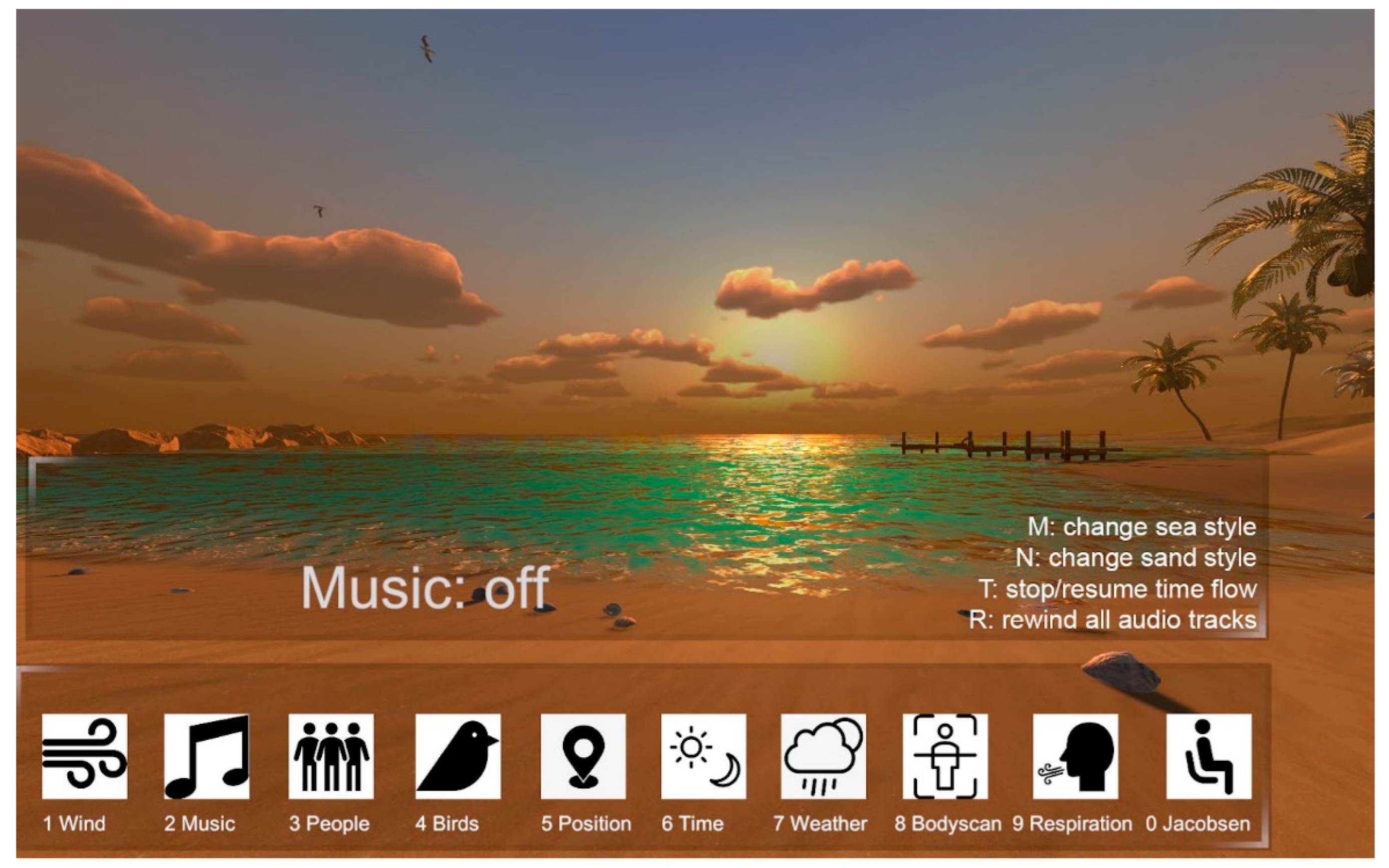
2.1. The Virtual Environment Design
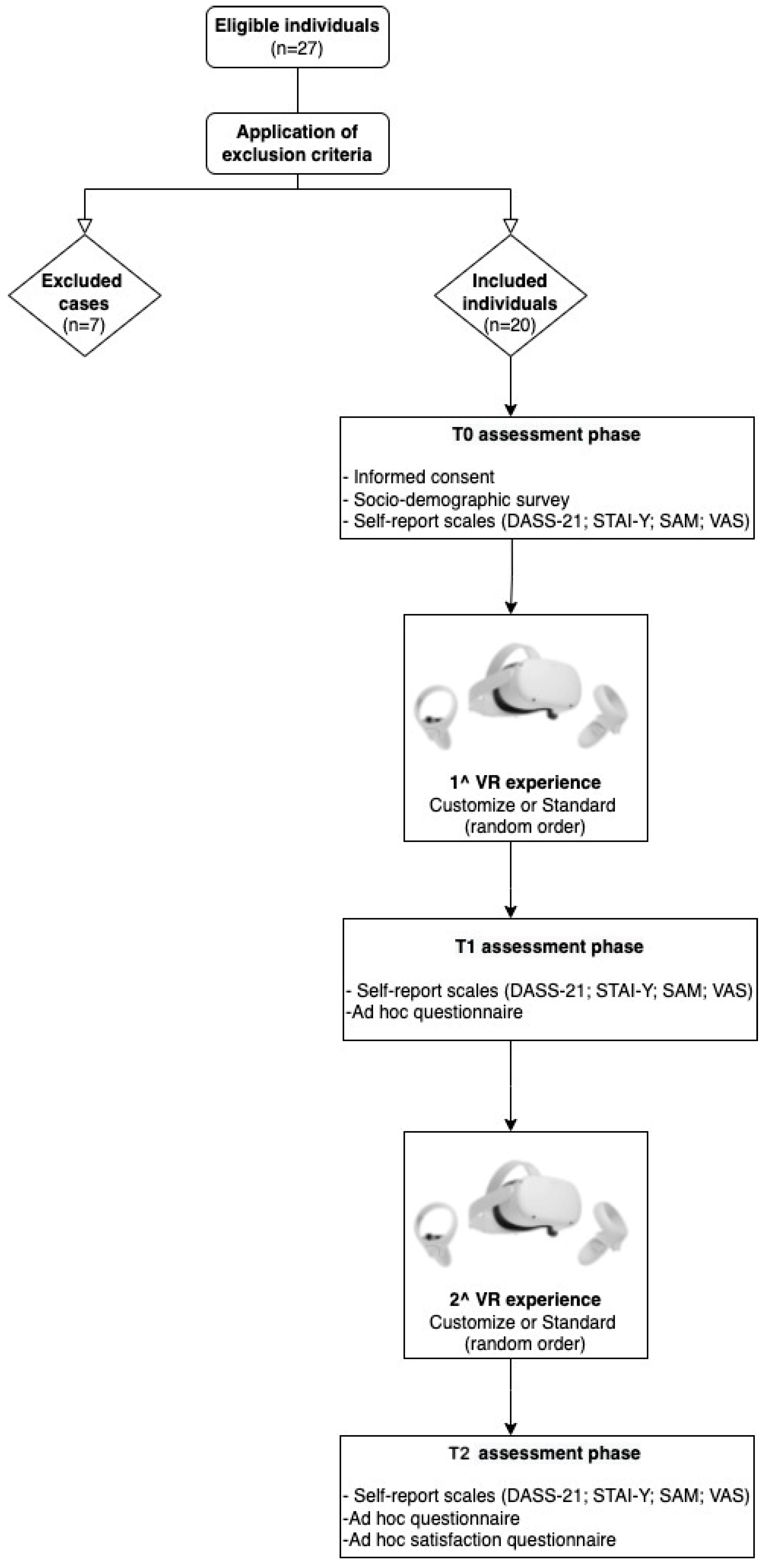
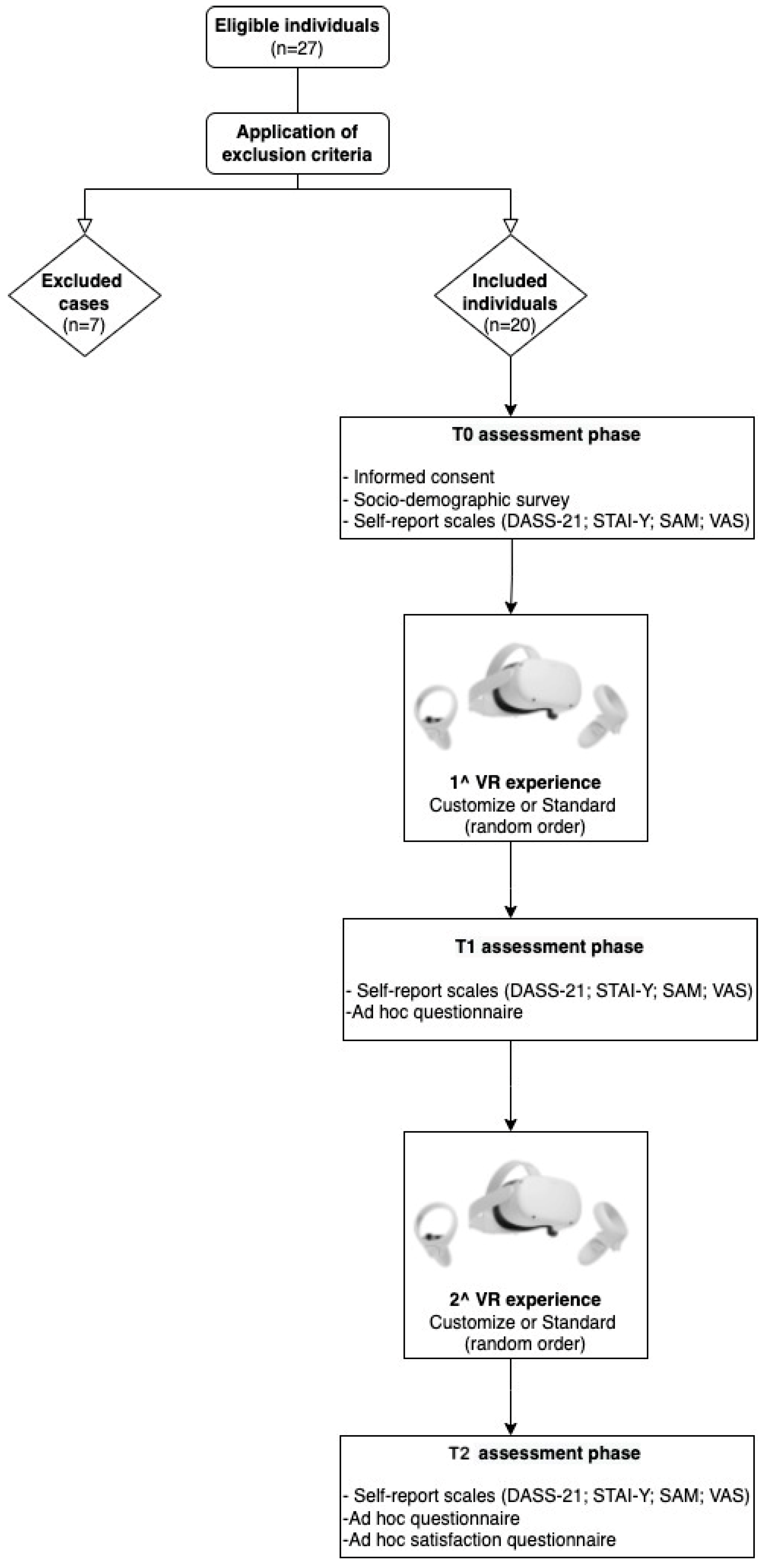
2.2. Procedure
2.3. Materials
3. Results
3.1. Statistical Analysis
3.2. Preliminary Analysis
3.3. Sociodemographic Characteristics of Participants
3.4. Qualitative Results
3.4.1. Is the VRE Preferable with or without the Body Scan Audio Track?
3.4.2. Usability, Physical Discomfort in Wearing the Head-Mounted Display, and Simulator Sickness
3.4.3. Graphics Quality, Synchronization, and Wayfinding VRE-Related
3.4.4. Realism of the Virtual Environments
3.4.5. Preferred VR Environment between Standard and Personalized
3.5. Differences between Self-Report Administration after Standard and Personalized VR Experiences about Immersivity, Sense of Presence, Realism, Engagement, Usability, Subjective Arousal Perception, Sense of Relaxation, and Pleasantness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Spielberger, C.D. Current trends in theory and research on anxiety. In Anxiety; Spielberger, C.D., Ed.; Academic Press: New York, NY, USA; London, UK, 1972; pp. 3–19. ISBN 9780126574012. [Google Scholar] [CrossRef]
- Spielberger, C.D. State-Trait Anxiety Inventory: A Comprensive Bibliography; Consulting Psychologist Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Li, M.; Wang, l.; Jiang, M.; Wu, D.; Tian, T.; Huang, W. Relaxation techniques for depressive disorders in adults: A systematic review and meta-analysis of randomised controlled trials. Int. J. Psychiatry Clin. Pract. 2020, 24, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Balaji, P.A.; Varne, S.R.; Ali, S.S. Psychological effects of yogic practices and transcendental meditation in health and disease. N. Am. J. Med. Sci. 2012, 4, 442–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhuri, A.; Manna, M.; Mandal, K.; Pattanayak, K. Is there any effect of progressive muscle relaxation exercise on anxiety and depression of the patient with coronary artery disease? Int. J. Pharma. Res. Health. Sci. 2020, 8, 3231–3236. [Google Scholar] [CrossRef]
- Toussaint, L.; Nguyen, Q.A.; Roettger, C.; Dixon, K.; Offenbächer, M.; Kohls, N.; Hirsch, J.; Sirois, F. Effectiveness of Progressive Muscle Relaxation, Deep Breathing, and Guided Imagery in Promoting Psychological and Physiological States of Relaxation. Evid.-Based Complement. Altern. Med. 2021, 2021, 5924040. [Google Scholar] [CrossRef]
- Schultchen, D.; Messner, M.; Karabatsiakis, A.; Schillings, C.; Pollatos, O. Effects of an 8-Week Body Scan Intervention on Individually Perceived Psychological Stress and Related Steroid Hormones in Hair. Mindfulness 2019, 10, 2532–2543. [Google Scholar] [CrossRef]
- Sauer-Zavala, S.E.; Walsh, E.C.; Eisenlohr-Moul, T.A.; Lykins, E.L. Comparing mindfulness-based intervention strategies: Differential effects of sitting meditation, body scan, and mindful yoga. Mindfulness 2013, 4, 383–388. [Google Scholar] [CrossRef]
- Ussher, M.; Spatz, A.; Copland, C.; Nicolaou, A.; Cargill, A.; Amini-Tabrizi, N.; McCracken, L.M. Immediate effects of a brief mindfulness-based body scan on patients with chronic pain. J. Behav. Med. 2014, 37, 127–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. Fear of COVID-19 and the mental health consequences in America. Psychol. Trauma. 2020, 12, S17–S21. [Google Scholar] [CrossRef]
- Riches, S.; Azevedo, L.; Bird, L.; Pisani, S.; Valmaggia, L. Virtual reality relaxation for the general population: A systematic review. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1707–1727. [Google Scholar] [CrossRef]
- Shah, L.B.I.; Klainin-Yobas, P.; Torres, S.; Kannusamy, P. Efficacy of psychoeducation and relaxation interventions on stress-related variables in people with mental disorders: A literature review. Arch. Psychiatr. Nurs. 2014, 28, 94–101. [Google Scholar] [CrossRef]
- Tyrväinen, L.; Ojala, A.; Korpela, K.; Lanki, T.; Tsunetsugu, Y.; Kagawa, T. The influence of urban green environments on stress relief measures: A field experiment. J. Environ. Psychol. 2014, 38, 1–9. [Google Scholar] [CrossRef]
- Pritchard, A.; Richardson, M.; Sheffield, D.; McEwan, K. The relationship between nature connectedness and eudaimonic well-being: A meta-analysis. J. Happiness Stud. 2020, 21, 1145–1167. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Haro, M.V.; López-del-Hoyo, Y.; Campos, D.; Linehan, M.M.; Hoffman, H.G.; García-Palacios, A.; Borao, L.; García-Campayo, J. Meditation experts try Virtual Reality Mindfulness: A pilot study evaluation of the feasibility and acceptability of Virtual Reality to facilitate mindfulness practice in people attending a Mindfulness conference. PLoS ONE 2017, 12, e0187777. [Google Scholar] [CrossRef]
- Chandrasiri, A.; Collett, J.; Fassbender, E.; De Foe, A. A virtual reality approach to mindfulness skills training. Virtual Real. 2020, 24, 143–149. [Google Scholar] [CrossRef]
- Seabrook, E.; Kelly, R.; Foley, F.; Theiler, S.; Thomas, N.; Wadley, G.; Nedeljkovic, M. Understanding How Virtual Reality Can Support Mindfulness Practice: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e16106. [Google Scholar] [CrossRef] [PubMed]
- Pizzoli, S.F.M.; Triberti, S.; Monzanii, D.; Mazzocco, K.; Kufel, E.; Porebiak, M.; Pravettoni, G. Comparison of relaxation techniques in virtual reality for breast cancer patients. In Proceedings of the 5th Experiment International Conference (exp.at’19), Funchal, Portugal, 12–14 June 2019. [Google Scholar]
- Annerstedt, M.; Triberti, S.; Monzani, D.; Mazzocco, K.; Kufel, E.; Porebiak, M.; Pravettoni, G. Inducing physiological stress recovery with sounds of nature in a virtual reality forest-Results from a pilot study. Physiol. Behav. 2013, 118, 240–250. [Google Scholar] [CrossRef]
- Li, H.; Zhang, X.; Wang, H.; Yang, Z.; Liu, H.; Cao, Y.; Zhang, G. Access to Nature via Virtual Reality: A Mini-Review. Front. Psychol. 2021, 12, 725288. [Google Scholar] [CrossRef]
- Gascon, M.; Zijlema, W.; Vert, C.; White, M.P.; Nieuwenhuijsen, M.J. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 2017, 220, 1207–1221. [Google Scholar] [CrossRef]
- White, M.P.; Elliott, L.R.; Grellier, J.; Economou, T.; Bell, S.; Bratman, G.N.; Cirach, M.; Gascon, M.; Lima, M.L.; Fleming, L.E.; et al. Associations between green/blue spaces and mental health across 18 countries. Sci. Rep. 2021, 11, 8903. [Google Scholar] [CrossRef]
- Browning, M.H.E.M.; Mimnaugh, K.J.; van Riper, C.J.; Laurent, H.K.; LaValle, S.M. Can Simulated Nature Support Mental Health? Comparing Short, Single-Doses of 360-Degree Nature Videos in Virtual Reality with the Outdoors. Front. Psychol. 2020, 10, 2667. [Google Scholar] [CrossRef] [Green Version]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef] [PubMed]
- Chirico, A.; Gaggioli, A. When virtual feels real: Comparing emotional responses and presence in virtual and natural environments. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Palanica, A.; Lyons, A.; Cooper, M.; Lee, A.; Fossat, Y. A comparison of nature and urban environments on creative thinking across different levels of reality. J. Environ. Psychol. 2019, 63, 44–51. [Google Scholar] [CrossRef]
- Riva, G. Virtual Reality in Clinical Psychology. In Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Pizzoli, S.F.M.; Mazzocco, K.; Triberti, S.; Monzani, D.; Alcañiz, R.M.L.; Pravettoni, G. User-Centered Virtual Reality for Promoting Relaxation: An Innovative Approach. Front. Psychol. 2019, 10, 479. [Google Scholar] [CrossRef] [Green Version]
- Anderson, A.P.; Mayer, M.D.; Fellows, A.M.; Cowan, D.R.; Hegel, M.T.; Buckey, J.C. Relaxation with immersive natural scenes presented using virtual reality. Aerosp. Med. Hum. Perform. 2017, 88, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Baños, R.M.; Botella, C.; Rubió, I.; Quero, S.; García-Palacios, A.; Alcañiz, M. Presence and emotions in virtual environments: The influence of stereoscopy. Cyberpsychol. Behav. 2008, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Baños, R.M.; Botella, C.; Guillen, V.; García-Palacios, A.; Quero, S.; Bretón-López, J.; Alcañiz, M. An adaptive display to treat stress-related disorders: EMMA’s world. Br. J. Guid. Couns. 2009, 37, 347–356. [Google Scholar] [CrossRef]
- Garrett, J.J. The Elements of User Experience: User-Centered Design for the Web and Beyond; Pearson Education: London, UK, 2010. [Google Scholar]
- Triberti, S.; Barello, S. The quest for engaging AmI: Patient engagement and experience design tools to promote effective assisted living. J. Biomed. Inform. 2016, 63, 150–156. [Google Scholar] [CrossRef]
- Baños, R.M.; Botella, C.; Alcañiz, M.; Liaño, V.; Guerrero, B.; Rey, B. Immersion and emotion: Their impact on the sense of presence. Cyberpsychol. Behav. 2004, 7, 734–741. [Google Scholar] [CrossRef]
- Rey, B.; Montesa, J.; Raya, M.A.; Baños, R.M.; Botella, C. A Preliminary study on the use of an adaptive display for the treatment of emotional disorders. Psychnol. J. 2005, 3, 101–112. [Google Scholar]
- Riva, G.; Mantovani, F.; Capideville, C.S.; Preziosa, A.; Morganti, F.; Villani, D.; Gaggioli, A.; Botella, C.; Alcañiz, M. Affective interactions using virtual reality: The link between presence and emotions. Cyberpsychol. Behav. 2007, 10, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Heyse, J.; Torres Vega, M.; De Jonge, T.; De Backere, F.; De Turck, F. A Personalised Emotion-Based Model for Relaxation in Virtual Reality. Appl. Sci. 2020, 10, 6124. [Google Scholar] [CrossRef]
- Maggio, M.G.; De Cola, M.C.; Latella, D.; Maresca, G.; Finocchiaro, C.; La Rosa, G.; Cimino, V.; Sorbera, C.; Bramanti, P.; De Luca, R.; et al. What about the role of virtual reality in parkinson disease’s cognitive rehabilitation? Preliminary findings from a randomized clinical trial. J. Geriatr. Psychiatry Neurol. 2018, 31, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, R.E.J.; Dijk, A.V.; Verhulp, E.E.; Castro, B.O. Interactive virtual reality assessment of aggressive social information processing in boys with behavior problems: A pilot study. Clin. Psychol. Psychother. 2021, 28, 489–549. [Google Scholar] [CrossRef] [PubMed]
- Wren, A.A.; Neiman, N.; Caruso, T.J.; Rodriguez, S.; Taylor, K.; Madill, M.; Rives, H.; Nguyen, L. Mindfulness-based virtual reality intervention for children and young adults with inflammatory bowel disease: A pilot feasibility and acceptability study. Children 2021, 8, 368. [Google Scholar] [CrossRef]
- Wright, L.; Steptoe, A.; Fancourt, D. Does thinking make it so? Differential associations between adversity worries and experiences and mental health during the COVID-19 pandemic. J. Epidemiol. Community Health 2021, 75, 817–823. [Google Scholar] [CrossRef]
- Zhang, T.; Booth, R.; Jean-Louis, R.; Chan, R.; Yeung, A.; Gratzer, D.; Strudwick, G. A Primer on Usability Assessment Approaches for Health-Related Applications of Virtual Reality. JMIR Serious Games 2020, 8, e18153. [Google Scholar] [CrossRef]
- Nielsen, J. Enhancing the explanatory power of usability heuristics. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI 94), Boston, MA, USA, 24–28 April 1994; pp. 152–158. [Google Scholar]
- Sutcliffe, A.; Gault, B. Heuristic evaluation of virtual reality applications. Interact. Comput. 2004, 16, 831–849. [Google Scholar] [CrossRef]
- Stanney, K.M.; Mollaghasemi, M.; Reeves, L.; Breaux, R.; Graeber, D.A. Usability engineering of virtual environments (VEs): Identifying multiple criteria that drive effective VE system design. Int. J. Hum.-Comput. Stud. 2003, 58, 447–481. [Google Scholar] [CrossRef]
- Czajkowski, S.M.; Powell, L.H.; Adler, N.; Naar-King, S.; Reynolds, K.D.; Hunter, C.M.; Laraia, B.; Olster, D.H.; Perna, F.M.; Charlson, M.E. From ideas to efficacy: The ORBIT model for developing behavioral treatments for chronic diseases. Health Psychol. 2015, 34, 971–982. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness; Delacorte: New York, NY, USA, 1990. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Bernstein, D.A.; Borkovec, T.D. Progressive Relaxation Training: A Manual for Helping Professions; Research Press: Champaign, IL, USA, 1973. [Google Scholar]
- Bernstein, D.A.; Carlson, C.R.; Schmidt, J.E. Progressive relaxation: Abbreviated methods. In Principles and Practice of Stress Management; Lehrer, P.M., Woolfolk, R.L., Sime, W.E., Eds.; The Guilford Press: New York, NY, USA, 2007; pp. 88–122. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory (Form Y1-Y2); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory (Form Y), Italian version; Pedrabissi, L., Santinello, M., Eds.; Mind Garden: Redwood City, CA, USA; Giunti Psychometrics: Firenze, Italy, 2018. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef]
- Ames, S.L.; Wolffsohn, J.S.; Mcbrien, N.A. The development of a symptom questionnaire for assessing virtual reality viewing using a head-mounted display. Optom. Vis. Sci. 2005, 82, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chirico, A.; Maiorano, P.; Indovina, P.; Milanese, C.; Giordano, G.G.; Alivernini, F.; Iodice, G.; Gallo, L.; De Pietro, G.; Giordano, A.; et al. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J. Cell. Physiol. 2019, 235, 5353–5362. [Google Scholar] [CrossRef] [PubMed]
- Witmer, B.G.; Singer, M.J. Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence Teleoperators Virtual Environ. 1998, 7, 225–240. [Google Scholar] [CrossRef]
- Bradley, M.M.; Lang, P.J. Measuring emotion: The self-assessment manikin and the semantic differential. J. Behav. Ther. Exp. Psychiatry 1994, 25, 49–59. [Google Scholar] [CrossRef]
- Morris, J.D. Observations: SAM: The self-assessment manikin: An efficient cross-cultural measurement of emotional response. J. Advert. Res. 1995, 35, 63–68. [Google Scholar]
- IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- George, D.; Mallery, M. SPSS for Windows Step by Step: A Simple Guide and Reference, 17.0 Update, 10th ed.; Pearson: Boston, MA, USA, 2010. [Google Scholar]
- Khan, A.F. Assessment of Midlife career Stress on Indian Managers. Ph.D Thesis, Aligarh Muslim University, Aligarh, India, 2015. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, M.; Brantley, S.; Feng, J. A mini review of presence and immersion in virtual reality. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2021, 65, 1099–1103. [Google Scholar] [CrossRef]
- Villani, D.; Riva, G. New technologies for relaxation: The role of presence. Psychol. Assoc. 2007, 14, 260–274. [Google Scholar] [CrossRef] [Green Version]
- Rotter, J.B. Generalized expectancies for internal versus external control of reinforcement. Psychol. Monogr. 1966, 80, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iachini, T.; Maffei, L.; Masullo, M.; Senese, V.P.; Rapuano, M.; Pascale, A.; Sorrentino, F.; Ruggiero, G. The experience of virtual reality: Are individual differences in mental imagery associated with sense of presence? Cogn. Process. 2019, 20, 291–298. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Data collection Method | Analysis Captured |
|---|---|
| Socio-Demographic Survey | Descriptive analysis. Frequencies, means, and standard deviations related to socio-demographics variables. |
| Virtual Reality Symptom Questionnaire | Descriptive analysis. Frequencies related to cybersickness variables. |
| Questionnaire inspired by the Presence Questionnaire and the Immersive Tendencies Questionnaire | Descriptive analysis. Means and standard deviations. ANOVAs repeated measures to compare the self-report scores taken at two different time points. |
| Open-Ended Question–VR scenario preferred | Descriptive analysis. Thematic analysis, frequencies related to which VR scenario was preferred. |
| Ad Hoc Satisfaction Questionnaire | Descriptive analysis. Frequencies. |
| Depression, Anxiety and Stress Scale-21 State-Trait Anxiety Inventory-Y Self-Assessment Manikin Visual Analogue Scale | ANOVAs repeated measures and Paired-samples t-tests. |
| Randomization Order Group | M (SD) | F (1,18) | p | |
|---|---|---|---|---|
| SAM_V_T1 | 1 2 | 3.5 (1.1) 2.8 (1.5) | 1.47 | ns |
| SAM_A_T1 | 1 2 | 5.2 (2.4) 7.2 (1.9) | 4.13 | ns |
| SAM_D_T1 | 1 2 | 4.8 (2.2) 6.2 (1.7) | 2.55 | ns |
| VAS_RELAX_T1 | 1 2 | 7.8 (1.6) 8.2 (1.1) | 0.43 | ns |
| VAS_PRESENCE_T1 | 1 2 | 6.6 (2.4) 7.9 (2.1) | 1.67 | ns |
| SAM_V_T2 | 1 2 | 2.4 (0.8) 2.1 (1.3) | 0.64 | ns |
| SAM_A_T2 | 1 2 | 5.8 (2.7) 7.4 (2.1) | 2.22 | ns |
| SAM_D_T2 | 1 2 | 5.6 (1.7) 6.4 (1.7) | 1.18 | ns |
| VAS_RELAX_T2 | 1 2 | 7.6 (0.9) 8.4 (0.9) | 2.95 | ns |
| VAS_PRESENCE_T2 | 1 2 | 7.6 (0.9) 8.4 (0.9) | 3.43 | ns |
| STAI-Y1_T1 | 1 2 | 28.2 (7.6) 27.1 (4.5) | 0.16 | ns |
| STAI-Y1_T2 | 1 2 | 25.2 (3.9) 25.6 (4.7) | 0.04 | ns |
| REALISM_T1 | 1 2 | 100.2 (14.3) 103.2 (19.8) | 0.15 | ns |
| REALISM_T2 | 1 2 | 105.1 (17.5) 108.6 (12.9) | 0.26 | ns |
| ENGAGEMENT_T1 | 1 2 | 10.9 (2.2) 10.6 (2.9) | 0.07 | ns |
| ENGAGEMENT_T2 | 1 2 | 10.3 (2.9) 12.3 (1.4) | 3.82 | ns |
| IMMERSIVITY_T1 | 1 2 | 11.8 (5.5) 13.9 (3.1) | 1.81 | ns |
| IMMERSIVITY_T2 | 1 2 | 17.2 (1.5) 16.1 (2.4) | 1.11 | ns |
| USABILITY_T1 | 1 2 | 17.1 (3.1) 14.1 (3.7) | 3.86 | ns |
| USABILITY_T2 | 1 2 | 16.5 (3.5) 15.1 (3.4) | 0.82 | ns |
| EMOTIONAL STATE_T1 | 1 2 | 46.7 (7.5) 43.8 (8.4) | 0.66 | ns |
| EMOTIONAL STATE_T2 | 1 2 | 45.7 (7.1) 47.3 (6.1) | 0.30 | ns |
| Questionnaire | M (SD) |
|---|---|
| DASS_Tot | 9.9 (6.9) |
| DASS_D | 2.5 (2.5) |
| DASS_A | 1.7 (1.9) |
| DASS_S | 5.7 (3.6) |
| STAI_Y2 | 34.9 (6.1) |
| STAI_Y1 (T0) | 32.7 (9.1) |
| STAI Y1 (st) | 27.7 (6.1) |
| STAI Y1 (p) | 25.4 (4.2) |
| SAM_V (T0) | 3.3 (0.7) |
| SAM_V (st) | 3.2 (1.3) |
| SAM_V (p) | 2.2 (1.1) |
| SAM_A (T0) | 5.5 (1.7) |
| SAM_A (st) | 6.2 (2.4) |
| SAM_A (p) | 6.6 (2.5) |
| SAM_D (T0) | 5.5 (1.4) |
| SAM_D (st) | 5.5 (2.1) |
| SAM_D (p) | 6 (1.7) |
| VAS_Relax (T0) | 5.9 (1.6) |
| VAS_Relax (st) | 8 (1.3) |
| VAS_Relax (p) | 8.2 (1.6) |
| VAS_Sense of Presence (st) | 7.3 (2.3) |
| VAS_Sense of Presence (p) | 8 (1.1) |
| Realism (st) | 101.7 (16.9) |
| Realism (p) | 106.9 (15.1) |
| Engagement (st) | 10.8 (2.6) |
| Engagement (p) | 11.3 (2.5) |
| Immersivity (st) | 12.9 (4.5) |
| Immersivity (p) | 16.6 (2.1) |
| Usability (st) | 15.6 (3.7) |
| Usability (p) | 15.8 (3.4) |
| Emotional_state (st) | 45.3 (7.9) |
| Emotional state (p) | 46.5 (6.4) |
| Main Theme | User Quotes |
|---|---|
| „Relaxing as in reality“ | „Especially for the birdsong which is what I feel when I rest in the country“ (Participant 2). „I preferred the personalized environment because it reflects more of a context in which I relax in reality“ (Participant 9). „I find it easier to relax in the mountains“ (Participant 10). „Because, even in reality, when I have to relax I choose to go to the seaside“ (Participant 11). „The elements around me reflected an environment that generally makes me feel good, and relaxed“ (Participant 8). „If I want to take a break from everything, I usually go to the mountains“ (Participant 3). „I could select a context that generally relaxes me“ (Participant 13). „I usually feel more comfortable at the seaside, that’s why I chose it“ (Participant 6). „I prefer the seaside to the countryside in reality. I can associate it more with a sense of relaxation“ (Participant 16). „There were elements that helped me to relax as in everyday life“ (Participant 5). „This is very similar to my favourite place in reality“ (Participant 7). „It is similar to the place where I feel better about relaxing“ (Participant 17). „Because it represents a context that recalls the relaxing places in reality, and this was helpful“ (Participant 18). „I could recreate a more similar environment to the one that really relaxes me“ (Participant 14). „It was similar to the beach I choose to relax“ (Participant 12). „The seaside is one of the environment that I choose when I want to relax and disconnect my head“ (Participant 19). |
| „Reminiscence“ | „The countryside scenario reminds me of the area from which I come. This makes me feel at home“ (Participant 1). |
| „Control“ | „The very fact of having been able to choose“ (Participant 15). „I chose the mountain environment because I associated many beautiful memories with it“ (Participant 9). „Also because, as a child, I always went to the seaside and it was beautiful. This context somehow reminded me of it“ (Participant 19) „I decided what to insert in the environment. Then I liked it more!“ (Participant 17). „„First of all because I could decide“ (Participant 19). „It was my choice“ (Participant 16). |
| „Realism of the stimuli“ | „In the standard context I found more elements similar to reality, I felt more comfortable“ (Participant 20). „The seaside seemed more like reality and, although it was not the environment I had chosen, in the end I preferred it“ (Participant 4). |
| t (1,19) | p | |
|---|---|---|
| STAI Y1 (T0)/STAI Y1 (st) | 3.20 | <0.01 |
| STAI Y1 (T0)/STAI Y1 (p) | 4.97 | <0.001 |
| STAI Y1 (st)/STAI Y1 (p) | 2.20 | <0.05 |
| SAM_V (T0)/SAM_V (st) | 0.42 | ns |
| SAM_V (T0)/SAM_V (p) | 3.80 | <0.01 |
| SAM_V (st)/SAM_V (p) | 2.97 | <0.01 |
| SAM_A (T0)/SAM_A (st) | −1.58 | ns |
| SAM_A (T0)/SAM_A (p) | −2.46 | <0.05 |
| SAM_A (st)/SAM_A (p) | −1.29 | ns |
| VAS_relax (T0)/VAS_relax (st) | −6.25 | <0.001 |
| VAS_relax (T0)/VAS_relax (p) | −2.52 | <0.05 |
| VAS_relax (st)/VAS_relax (p) | −9.95 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardini, S.; Gabrielli, S.; Dianti, M.; Novara, C.; Zucco, G.M.; Mich, O.; Forti, S. The Role of Personalization in the User Experience, Preferences and Engagement with Virtual Reality Environments for Relaxation. Int. J. Environ. Res. Public Health 2022, 19, 7237. https://doi.org/10.3390/ijerph19127237
Pardini S, Gabrielli S, Dianti M, Novara C, Zucco GM, Mich O, Forti S. The Role of Personalization in the User Experience, Preferences and Engagement with Virtual Reality Environments for Relaxation. International Journal of Environmental Research and Public Health. 2022; 19(12):7237. https://doi.org/10.3390/ijerph19127237
Chicago/Turabian StylePardini, Susanna, Silvia Gabrielli, Marco Dianti, Caterina Novara, Gesualdo M. Zucco, Ornella Mich, and Stefano Forti. 2022. "The Role of Personalization in the User Experience, Preferences and Engagement with Virtual Reality Environments for Relaxation" International Journal of Environmental Research and Public Health 19, no. 12: 7237. https://doi.org/10.3390/ijerph19127237
APA StylePardini, S., Gabrielli, S., Dianti, M., Novara, C., Zucco, G. M., Mich, O., & Forti, S. (2022). The Role of Personalization in the User Experience, Preferences and Engagement with Virtual Reality Environments for Relaxation. International Journal of Environmental Research and Public Health, 19(12), 7237. https://doi.org/10.3390/ijerph19127237