
Evaluation of an Oral Care Program to Improve the Oral Health of Home-Dwelling Older People

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
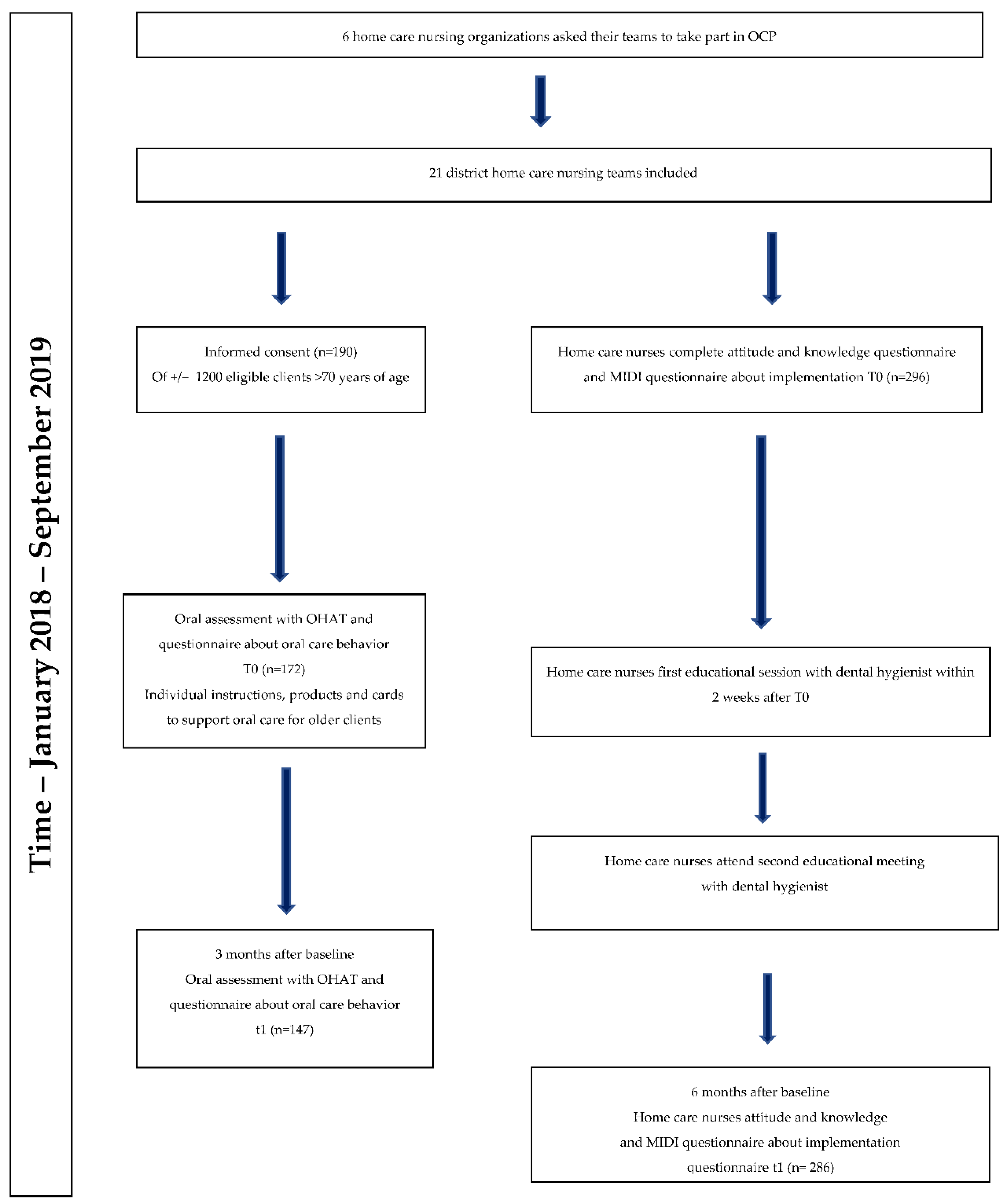
2.1. Design and Implementation of the ‘Oral Care Program’ (OCP)
- Home care nurses: (a) A general but tailored educational course about oral health (care) and the relationship with general health, based on the results of the baseline questionnaire about knowledge and attitudes of the home care nurses. The first course outlined the importance of oral health and the relationship with general health and wellbeing, and provided specific information about oral health problems in older people. (b) An in-depth module about the current guidelines for daily oral care including optional training of the practical skills. Apart from the guidelines [25] and practical information about (daily) oral care, the course included specific treatment and prevention of oral health problems in older people, e.g., dry mouth. The courses were given by a dental hygienist who is trained as a lecturer and dental hygienist at the school of Dental Hygiene Groningen. (c) Contact with a dental hygienist designated to the home care nursing team. The full courses and other detailed information about the OCP are available upon request by the first author.
- Home-dwelling older people in a home care setting: (a) A magazine with information about oral hygiene procedures, creating awareness of the importance of oral health (care). (b) A weekly calendar to support and give reminders of oral care with facts, reminders and suggestions. (c) Tailored oral care advice and instructions of a dental hygienist based on oral assessments and current guidelines in home care nursing. (d) Cards with tailored instructions for adequate oral health self-care [31]; for example, for older people with full dentures, the cards provided stepwise information about the daily oral care of the dentures and how to clean and store dentures. The cards could be put up in the bathroom. (e) Oral health care products. The products that were given were applicable to the older person. We provided toothbrushes, denture cases, denture brushes, interdental brushes, toothpicks and hourglasses to support brush time; according to the dental status, the appropriate products were provided.
- Dental hygienists: (a) Dental hygienists were allocated to a home care nursing team to answer questions or help with issues about oral health care.
2.2. Study Design
2.3. Sample and Recruitment
2.4. Data Collection and Measurements
Implementation Assessment Instruments
Instruments Assessing the Impact of the OCP on Home Care Nurses
- MIDI—measurement instrument for determinants of innovations
- Questionnaire attitude and knowledge
Instruments Assessing the Impact on Oral Health of Older People
- Questionnaire older people—oral (self) care
- Oral Health Assessment Tool (OHAT)—older people’s oral health
2.5. Ethics
2.6. Analysis
2.6.1. Data Analysis Regarding the Impact of the OCP on Home Care Nurses
2.6.2. Data Analysis Regarding the Impact of the OCP on Home-Dwelling Older People
Validity and Reliability
3. Results
3.1. Response and Results of the MIDI Questionnaire
- -
- Characteristics of the user: The HCNs and older people showed that HCNs expected that the OCP would make older people aware of the importance of oral health and most of the HCNs stated that they found oral health important for their clients. Additionally, HCNs considered it their job to observe the oral health of older people. After six months, even more HCNs than at baseline stated that the OCP was not time consuming for them, although the number of colleagues actually participating in the OCP decreased after six months.
- -
- The innovation (OCP): A positive attitude of HCNs towards the OCP at baseline and after six months was shown; more HCNs agreed that the OCP was not too complicated for them and the OCP fitted well with their daily work and was suitable for their clients.
- -
- The organization: HCNs care about the opinion of the manager, the organization, their colleagues/team members. After six months of working with the OCP, there were more agreements about participating in the OCP; HCNs were enabled to work with the OCP more, they knew more about the content of the OCP, and information was easily accessible. Additionally, HCNs were more positive after six months than at baseline about their ability to perform oral care and to assess older people’s oral (health) care.
- -
- Social-political context: The OCP matched well within current laws, rules and guidelines/procedures, and this scored more positively after six months.
3.2. Response on the Attitude and Knowledge Questionnaire for Home Care Nurses
3.3. Response and Characteristics of the Older People
3.4. Evaluation of Impact of the OCP on Patients’ Oral Health
4. Discussion
4.1. The in Co-Creation Developed, Person-Centered and Tailor-Made OCP Resulted in a Significant Improvement in the Oral Health and Oral Hygiene of Older People after Three Months
4.2. Limitations and Strengths of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tuuliainen, E.; Autonen-Honko Nen, K.; Nihtilä, A.; Komulainen, K.; Nykänen, I.; Hartikainen, S.; Ahonen, R.; Tiihonen, M.; Suominen, A. Oral Health and Hygiene and Association of Functional Ability: A Cross-Sectional Study among Old Home Care Clients. Oral Health Prev. Dent. 2020, 18, 1–10. [Google Scholar]
- Hakeem, F.F.; Bernabé, E.; Sabbah, W. Association between oral health and frailty: A systematic review of longitudinal studies. Gerodontology 2019, 36, 205–215. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Sakuramoto, A.; Sugita, H.; Hasegawa, K.; Horii, N.; Sawada, T.; Shinmura, K.; Kishimoto, H. Relationship between oral environment and frailty among older adults dwelling in a rural Japanese community: A cross-sectional observational study. BMC Oral Health 2019, 19, 23. [Google Scholar] [CrossRef] [Green Version]
- Hoeksema, A.R.; Peters, L.L.; Raghoebar, G.M.; Meijer, H.J.A.; Vissink, A.; Visser, A. Oral health status and need for oral care of care-dependent indwelling elderly: From admission to death. Clin. Oral Investig. 2017, 21, 2189–2196. [Google Scholar] [CrossRef] [Green Version]
- D’Aiuto, F.; Gkranias, N.; Bhowruth, D.; Khan, T.; Orlandi, M.; Suvan, J.; Masi, S.; Tsakos, G.; Hurel, S.; Hingorani, A.D.; et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: A 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 954–965. [Google Scholar] [CrossRef]
- Huppertz, V.A.L.; van der Putten, G.J.; Halfens, R.J.G.; Schols, J.M.G.A.; de Groot, L.C.P.G.M. Association between Malnutrition and Oral Health in Dutch Nursing Home Residents: Results of the LPZ Study. J. Am. Med. Dir. Assoc. 2017, 18, 948–954. [Google Scholar] [CrossRef]
- Johansson, L.; Sherina, N.; Kharlamova, N.; Potempa, B.; Larsson, B.; Israelsson, L.; Potempa, J.; Rantapää-Dahlqvist, S.; Lundberg, K. Concentration of antibodies against Porphyromonas gingivalis is increased before the onset of symptoms of rheumatoid arthritis. Arthritis Res. Ther. 2016, 18, 201. [Google Scholar] [CrossRef] [Green Version]
- van der Maarel-Wierink, C.D.; Vanobbergen, J.N.; Bronkhorst, E.M.; Schols, J.M.; de Baat, C. Oral health care and aspiration pneumonia in frail older people: A systematic literature review. Gerodontology 2013, 30, 3–9. [Google Scholar] [CrossRef]
- Wagley, S.; Marra, K.V.; Salhi, R.A.; Gautam, S.; Campo, R.; Veale, P.; Veale, J.; Arroyo, J.G. Periodontal Disease and Age-related Macular Degeneration: Results From the National Health and Nutrition Examination Survey III. Retina 2015, 35, 982–988. [Google Scholar] [CrossRef]
- Everaars, B.; Jerković-Ćosić, K.; Bleijenberg, N.; de Wit, N.J.; van der Heijden, G.J. Exploring Associations between Oral Health and Frailty in Community-Dwelling Older People. J. Frailty Aging 2021, 10, 56–62. [Google Scholar] [CrossRef]
- Paganini-Hill, A.; White, S.C.; Atchison, K.A. Dental Health Behaviors, Dentition, and Mortality in the Elderly: The Leisure World Cohort Study. J. Aging Res. 2011, 2011, 156061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, M.H.; Vissink, A.; Spoorenberg, S.L.W.; Wynia, K.; Visser, A. Self-reported oral health problems and the ability to organize dental care of community-dwelling elderly aged ≥75 years. BMC Oral Health 2020, 20, 185. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Hirano, H.; Arai, H.; Morishita, S.; Ohara, Y.; Edahiro, A.; Murakami, M.; Shimada, H.; Kikutani, T.; Suzuki, T. Relationship between Frailty and Oral Function in Community-Dwelling Elderly Adults. J. Am. Geriatr. Soc. (JAGS) 2017, 65, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, S.E.; Papachristou, E.; Watt, R.G.; Tsakos, G.; Lennon, L.T.; Papacosta, A.O.; Moynihan, P.; Sayer, A.A.; Whincup, P.H.; Wannamethee, S.G. Influence of Poor Oral Health on Physical Frailty: A Population-Based Cohort Study of Older British Men. J. Am. Geriatr. Soc. (JAGS) 2018, 66, 473–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics Netherlands Gezondheid en Zorggebruik; Persoonskenmerken. Available online: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83005NED/table?ts=1605541195693 (accessed on 16 December 2020).
- Ebbens, O.; Lawant, M.J.; Schuller, A.A. Tandartsbezoek van 65-plussers; onderzoek uit een algemene praktijk in Drenthe. Ned. Tijdschr. Voor Tandheelkd. 2018, 125, 151–155. Available online: https://www.narcis.nl/publication/RecordID/oai:pure.rug.nl:publications%2Fe3a3755e-6943-45e8-93a4-32d4341724ed (accessed on 29 April 2022). [CrossRef]
- Ishimaru, M.; Ono, S.; Morita, K.; Matsui, H.; Yasunaga, H. Domiciliary dental care among homebound older adults: A nested case–control study in Japan. Geriatr. Gerontol. Int. 2019, 19, 679–683. [Google Scholar] [CrossRef]
- Niesten, D.; Gerritsen, A.E.; Leve, V. Barriers and Facilitators to Integrate Oral Health care for Older Adults in General (Basic) Care in East Netherlands. Part 2 Functional Integration. Gerodontology 2021, 38, 154–165. [Google Scholar] [CrossRef]
- Niesten, D.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Oral health care behavior and frailty-related factors in a care-dependent older population. J. Dent. 2017, 61, 39–47. [Google Scholar] [CrossRef]
- Ohi, T.; Sai, M.; Kikuchi, M.; Hattori, Y.; Tsuboi, A.; Hozawa, A.; Ohmori-Matsuda, K.; Tsuji, I.; Watanabe, M. Determinants of the Utilization of Dental Services in a Community-Dwelling Elderly Japanese Population. Tohoku J. Exp. Med. 2009, 218, 241–249. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.B.; Thomson, W.M. ‘Not on the radar’: Dentists’ perspectives on the oral health care of dependent older people. Gerodontology 2017, 34, 90–100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. World Health Statistics. Available online: https://www.who.int/data/gho/publications/world-health-statistics (accessed on 17 May 2021).
- Vektis. Factsheet Wijkverpleging. 2020. Available online: https://www.vektis.nl/intelligence/publicaties/factsheet-wijkverpleging. (accessed on 4 December 2021).
- Verpleegkundigen &Verzorgenden Nederland, (V&VN). Protocollen Vilans. 2020. Available online: https://www.vilans.nl/vilans/media/documents/publicaties/lijst-protocollen-december-2020.pdf (accessed on 4 December 2021).
- Delgado, A.M.; Prihoda, T.; Nguyen, C.; Hicks, B.; Smiley, L.; Taverna, M. Professional caregivers’ oral care beliefs and beliefs for elderly clients ageing in place. J. Dent. Hyg. 2016, 90, 244–248. [Google Scholar] [PubMed]
- Lewis, A.; Harvey, G.; Hogan, M.; Kitson, A. Can oral healthcare for older people be embedded into routine community aged care practice? A realist evaluation using normalisation process theory. Int. J. Nurs. Stud. 2019, 94, 32–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmi, R.; Tolvanen, M.; Suhonen, R.; Lahti, S.; Närhi, T. Knowledge, perceived skills and activities of nursing staff to support oral home care among older domiciliary care clients. Scand. J. Caring Sci. 2018, 32, 1342. [Google Scholar] [CrossRef]
- Cheng, Y.; Ping, C.; Ho, C.; Lan, S.; Hsieh, Y. Home-care aides’ self-perception of oral health-care provision competency for community-dwelling older people. Int. Dent. J. 2019, 69, 158–164. [Google Scholar] [CrossRef]
- Prayoonwong, T.; Wiwatkhunupakan, T.; Lasuka, D.; Srisilapanan, P. Development of a community-based oral healthcare model for Thai dependent older people. Gerodontology 2015, 33, 545. [Google Scholar] [CrossRef]
- Ho, B.V.; van der Maarel-Wierink, C.D.; Rollman, A.; Weijenberg, R.A.F.; Lobbezoo, F. ‘Don’t forget the mouth!’: A process evaluation of a public oral health project in community-dwelling frail older people. BMC Oral Health 2021, 21, 536. [Google Scholar] [CrossRef]
- Actiz, Brache Thuiszorg Nederland (BTN), Verpleegkundigen &Verzorgenden Nederland (V&VN) Toewerken naar Voldoende Gekwalificeerdeverpleegkundigen in de Wijkverpleging. 2017. Available online: https://www.venvn.nl/media/wyad103y/2018-herziening-overgangsregeling-toewerken-naar-voldoende-gwalificeerde-verpleegkundigen-def.pdf (accessed on 4 December 2021).
- Fleuren, M.A.H.; Paulussen, T.G.W.M.; van Dommelen, P.; van Buuren, S. Towards a measurement instrument for determinants of innovations. Int. J. Qual. Health Care 2014, 26, 501–510. [Google Scholar] [CrossRef] [Green Version]
- Dutch Association of Elderly Care Physicians (Verenso) Richtlijn Mondzorg voor Zorgafhankelijke Cliënten in Verpleeghuizen. 2007. Available online: https://www.verenso.nl/_asset/_public/Richtlijnen_kwaliteit/richtlijnen/database/Richtlijnmondzorg.pdf (accessed on 29 April 2022).
- Weening-Verbree, L.F.; Schuller, A.A.; Cheung, S.S.L.; Zuidema, S.U.; Schans, C.V.D.; Hobbelen, J. Barriers and facilitators of oral health care experienced by nursing home staff. Geriatr. Nurs. 2021, 42, 799–805. [Google Scholar] [CrossRef]
- Weening-Verbree, L.F. Masterthesis Mondzorg, Hoe Wordt Het Mogelijk? Master’s Thesis, University of Utrecht, Utrecht, The Netherlands, 2009; pp. 1–25. [Google Scholar]
- Qualtrics Qualtrics. Available online: www.qualtrics.com (accessed on 30 September 2020).
- Chalmers, J.M.; King, P.L.; Spencer, A.J.; Wright, F.; Carter, K.D. The Oral Health Assessment Tool-Validity and reliability. Aust. Dent. J. 2005, 50, 191–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinheiro, J.C.; Bates, D.M. Mixed-Effects Models in S and S-PLUS; Springer Science & Business Media: New York, NY, USA, 2000. [Google Scholar]
- Czwikla, J.; Herzberg, A.; Kapp, S.; Kloep, S.; Rothgang, H.; Nitschke, I.; Haffner, C.; Hoffmann, F. Effectiveness of a Dental Intervention to Improve Oral Health among Home Care Recipients: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 9339. [Google Scholar] [CrossRef] [PubMed]
- Janssens, B.; De Visschere, L.; van der Putten, G.J.; de Lugt-Lustig, K.; Schols, J.M.G.A.; Vanobbergen, J. Effect of an oral healthcare protocol in nursing homes on care staffs’ knowledge and attitude towards oral health care: A cluster-randomised controlled trial. Gerodontology 2016, 33, 275–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, L.; Fletcher, J.; Goodenough, B.; Jeon, Y.; Etherton-Beer, C.; MacAndrew, M.; Beattie, E. A Systematic Review of Interventions to Change Staff Care Practices in Order to Improve Resident Outcomes in Nursing Homes. PLoS ONE 2015, 10, e0140711. [Google Scholar] [CrossRef] [PubMed]
- Weening-Verbree, L.; Huisman-de Waal, G.; van Dusseldorp, L.; van Achterberg, T.; Schoonhoven, L. Oral health care in older people in long term care facilities: A systematic review of implementation strategies. Int. J. Nurs. Stud. 2013, 50, 569–582. [Google Scholar] [CrossRef]
- Fasbender, U.; van der Heijden, B.I.J.M.; Grimshaw, S. Job satisfaction, job stress and nurses’ turnover intentions: The moderating roles of on-the-job and off-the-job embeddedness. J. Adv. Nurs. 2019, 75, 327–337. [Google Scholar] [CrossRef]
- Lundberg, A.; Hillebrecht, A.; McKenna, G.; Srinivasan, M. COVID-19: Impacts on oral healthcare delivery in dependent older adults. Gerodontology 2021, 38, 174–178. [Google Scholar] [CrossRef]
- Smith, B.J.; Helgeson, M.; Prosa, B.; Finlayson, T.L.; Orozco, M.; Asgari, P.; Pierce, I.; Norman, G.; Aronoff-Spencer, E. Longitudinal analysis of cost and dental utilization patterns for older adults in outpatient and long-term care settings in Minnesota. PLoS ONE 2020, 15, e0232898. [Google Scholar] [CrossRef]
- Goodman, D.; Ogrinc, G.; Davies, L.; Baker, G.R.; Barnsteiner, J.; Foster, T.C.; Gali, K.; Hilden, J.; Horwitz, L.; Kaplan, H.C.; et al. Explanation and elaboration of the SQUIRE (Standards for Quality Improvement Reporting Excellence) Guidelines, V.2.0: Examples of SQUIRE elements in the healthcare improvement literature. BMJ Qual. Saf. 2016, 25, e7. [Google Scholar] [CrossRef] [Green Version]
- Ogrinc, G.; Davies, L.; Goodman, D.; Batalden, P.; Davidoff, F.; Stevens, D. Squire 2.0 (Standards for Quality Improvement Reporting Excellence): Revised Publication Guidelines From a Detailed Consensus Process. Am. J. Crit. Care 2015, 25, 986–992. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statements—Attitude Items | T0 n = 173 (%) | T1 n = 114 (%) | ||
|---|---|---|---|---|
| Agree | Do Not Agree | Agree | Do Not Agree | |
| I think clients think a healthy mouth is important | 84 | 16 | 83 | 17 |
| Our clients do not ask support for oral care | 65 | 35 | 70 | 30 |
| I think it is important to take care of clients’ oral care | 100 | 0 | 97 | 3 |
| I have enough skills to perform oral care | 79 | 21 | 89 | 11 |
| I have enough time to perform oral care | 72 | 28 | 72 | 28 |
| There are enough materials available to perform oral care (toothbrushes etcetera) | 46 | 53 | 54 | 46 |
| I think oral care should be part of the clients’ general personal care plan | 92 | 8 | 92 | 8 |
| I feel insecure to perform oral care for clients | 8 | 92 | 7 | 93 |
| I think it is an unpleasant task to perform oral care for clients | 11 | 89 | 12 | 88 |
| I think it is difficult to perform oral care for clients | 16 | 84 | 15 | 85 |
| Characteristics | n = 172 | n * | % |
|---|---|---|---|
| Mean age (SD) | 82.9 (7.7) | ||
| Gender, women | 136 | 72 | |
| Dental status | |||
| Natural teeth | 27 | 16 | |
| Dentures | 90 | 52 | |
| Dentures/natural teeth | 35 | 20 | |
| Dental implants/dentures | 20 | 12 | |
| Dental visits | |||
| Visits a dental professional (yes) | 76 | 44 | |
| Visited a dentist in the past 2 years (yes) | 74 | 43 | |
| Oral (self) care | |||
| Tooth brushing, two times a day or more | 45 | 83 | 54 |
| Tooth brushing, less than two times a day | 38 | 83 | 46 |
| Interdental cleaning daily (yes) | 25 | 73 | 34 |
| Denture cleaning with water and soap | 26 | 145 | 18 |
| Client does oral care him/herself | 156 | 91 |
| Sum Sq | Mean Sq | F Value | p Value | |
|---|---|---|---|---|
| Gender | 0.263 | 0.263 | 0.162 | 0.688 |
| Age | 5.549 | 5.549 | 3.416 | 0.067 |
| factor(dental status) | 13.867 | 4.622 | 2.845 | 0.039 * |
| dental visits | 6.194 | 6.194 | 3.813 | 0.052 |
| factor(team) | 43.389 | 3.099 | 1.908 | 0.029 * |
| factor(time) | 14.026 | 14.026 | 8.634 | 0.000 ** |
| factor(Team):factor(Time) | 38.713 | 2.765 | 1.702 | 0.061 |
| Estimate | Std. Error | df | t Value | p Value | |
|---|---|---|---|---|---|
| (Intercept) | 6.540 | 1.363 | 147.425 | 4.799 | 0.000 ** |
| factor(Time)2 | −0.821 | 0.152 | 154.928 | −5.390 | 0.000 ** |
| Gender | −0.135 | 0.257 | 150.563 | −0.526 | 0.599 |
| Age | −0.029 | 0.016 | 148.550 | −1.787 | 0.076 |
| factor(DentalstatusFac)1 | −0.918 | 0.358 | 168.304 | −2.561 | 0.011 * |
| factor(DentalstatusFac)2 | −0.167 | 0.390 | 144.763 | −0.429 | 0.669 |
| factor(DentalstatusFac)4 | −0.713 | 0.434 | 149.107 | −1.643 | 0.102 |
| DentVisit | −0.413 | 0.231 | 292.885 | −1.790 | 0.075 |
| factor(Team)1 | −0.046 | 0.838 | 174.374 | −0.055 | 0.956 |
| factor(Team)2 | 0.012 | 0.550 | 143.240 | 0.022 | 0.983 |
| factor(Team)3 | −0.276 | 0.600 | 147.408 | −0.460 | 0.647 |
| factor(Team)4 | −0.650 | 0.716 | 145.290 | −0.908 | 0.366 |
| factor(Team)5 | 0.148 | 0.627 | 144.668 | 0.237 | 0.813 |
| factor(Team)6 | −0.619 | 0.550 | 146.395 | −1.126 | 0.262 |
| factor(Team)7 | −1.660 | 0.618 | 151.270 | −2.686 | 0.008 ** |
| factor(Team)9 | 0.119 | 0.558 | 144.741 | 0.213 | 0.831 |
| factor(Team)10 | 0.696 | 0.598 | 149.620 | 1.165 | 0.246 |
| factor(Team)11 | 0.490 | 0.704 | 141.697 | 0.697 | 0.487 |
| factor(Team)12 | −0.316 | 1.195 | 170.085 | −0.265 | 0.792 |
| factor(Team)13 | −0.018 | 0.711 | 146.791 | −0.025 | 0.980 |
| factor(Team)14 | −1.00 | 0.778 | 169.624 | −1.289 | 0.199 |
| factor(Team)15 | 0.635 | 0.691 | 145.441 | 0.919 | 0.359 |
| Dental Status | n at t0 and t1 | Mean OHAT Sum Score T0 | SD of Mean OHAT T0 | Mean OHAT Sum Score T1 | SD of Mean OHAT T1 | MD | SD of MD | t Value | p Value |
|---|---|---|---|---|---|---|---|---|---|
| Natural dentition | 27 | 3.30 | 2..20 | 2.85 | 2.14 | 0.44 | 1.91 | 1.21 | 0.24 |
| Full dentures | 75 | 2.85 | 1.89 | 1.85 | 1.40 | 1.00 | 1.82 | 4.750 | 0.00 ** |
| Dentures and natural teeth | 29 | 3.76 | 1.94 | 2.83 | 1.37 | 0.93 | 2.02 | 2.49 | 0.02 * |
| Dentures on implants | 16 | 2.95 | 1.36 | 2.06 | 1.61 | 0.81 | 1.72 | 1.89 | 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weening-Verbree, L.F.; Schuller, A.A.; Zuidema, S.U.; Hobbelen, J.S.M. Evaluation of an Oral Care Program to Improve the Oral Health of Home-Dwelling Older People. Int. J. Environ. Res. Public Health 2022, 19, 7251. https://doi.org/10.3390/ijerph19127251
Weening-Verbree LF, Schuller AA, Zuidema SU, Hobbelen JSM. Evaluation of an Oral Care Program to Improve the Oral Health of Home-Dwelling Older People. International Journal of Environmental Research and Public Health. 2022; 19(12):7251. https://doi.org/10.3390/ijerph19127251
Chicago/Turabian StyleWeening-Verbree, Lina F., Annemarie A. Schuller, Sytse U. Zuidema, and Johannes S. M. Hobbelen. 2022. "Evaluation of an Oral Care Program to Improve the Oral Health of Home-Dwelling Older People" International Journal of Environmental Research and Public Health 19, no. 12: 7251. https://doi.org/10.3390/ijerph19127251
APA StyleWeening-Verbree, L. F., Schuller, A. A., Zuidema, S. U., & Hobbelen, J. S. M. (2022). Evaluation of an Oral Care Program to Improve the Oral Health of Home-Dwelling Older People. International Journal of Environmental Research and Public Health, 19(12), 7251. https://doi.org/10.3390/ijerph19127251