
Seroprevalence of SARS-CoV-2 Antibodies in Africa: A Systematic Review and Meta-Analysis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Data Management and Study Selection
2.3. Eligibility Criteria
2.4. Quality Assessment
2.5. Data Extraction
2.6. Statistical Analysis
2.7. Subgroup and Sensitivity Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of Included Studies
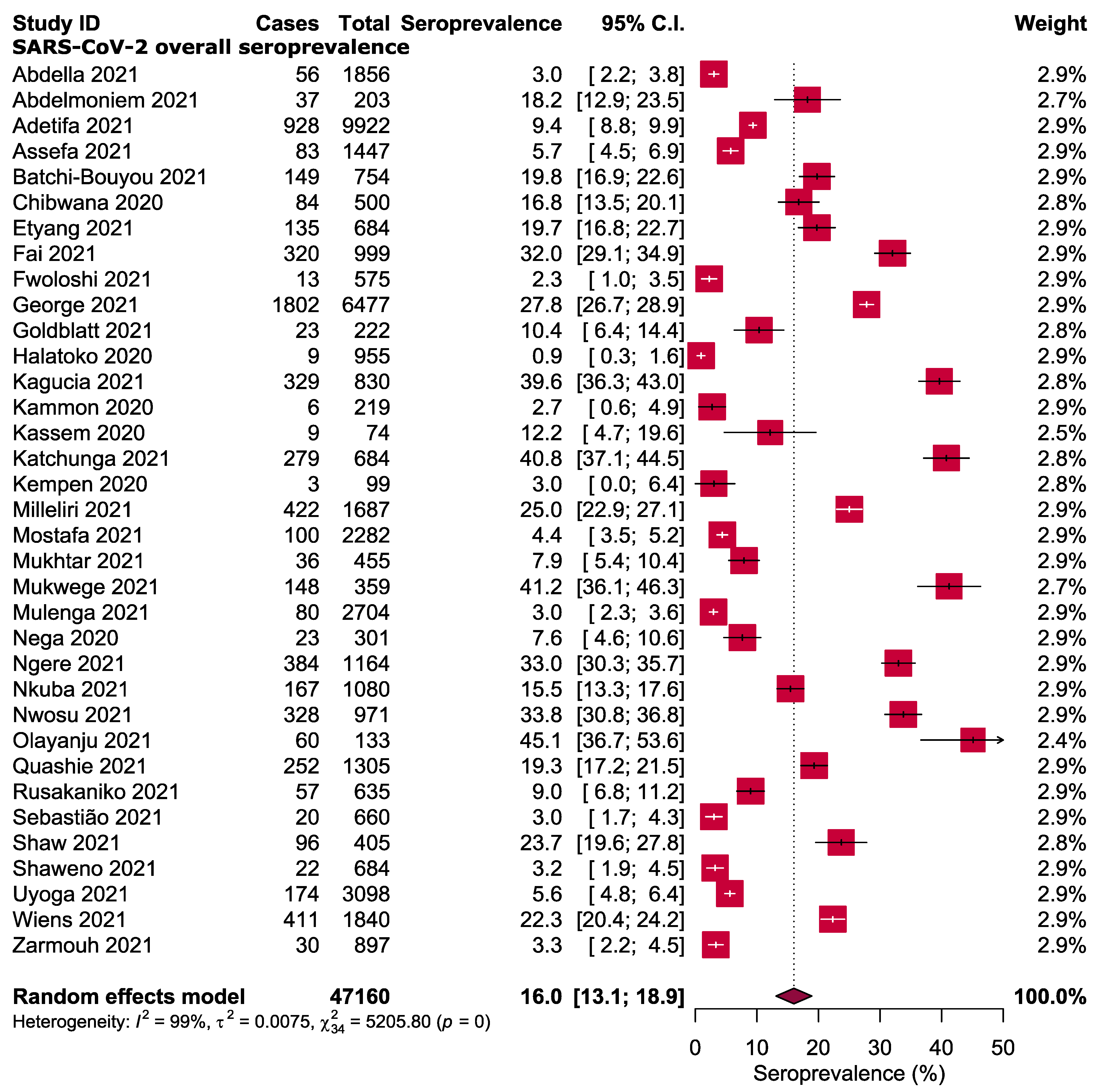
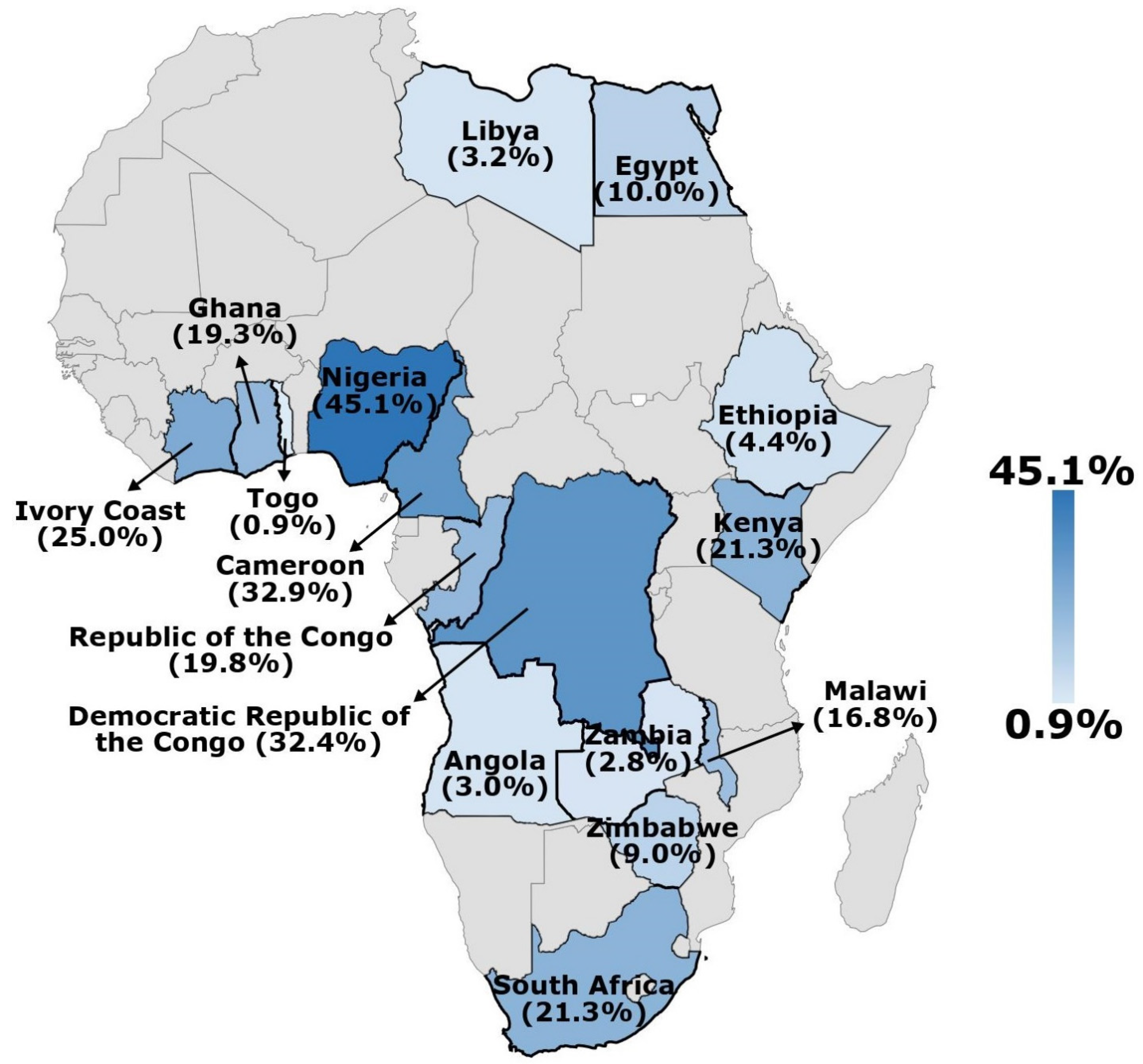
3.3. Seroprevalence of SARS-CoV-2 Antibodies
3.4. Subgroup Analysis
3.5. Quality Assessment and Publication Bias
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 25 February 2022).
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Amadu, I.; Ahinkorah, B.O.; Afitiri, A.-R.; Seidu, A.-A.; Ameyaw, E.K.; Hagan, J.E., Jr.; Duku, E.; Aram, S.A. Assessing sub-regional-specific strengths of healthcare systems associated with COVID-19 prevalence, deaths and recoveries in Africa. PLoS ONE 2021, 16, e0247274. [Google Scholar] [CrossRef] [PubMed]
- Nkengasong, J.N.; Mankoula, W. Looming threat of COVID-19 infection in Africa: Act collectively, and fast. Lancet 2020, 395, 841–842. [Google Scholar] [CrossRef] [Green Version]
- Africa Centres for Disease Control and Prevention. COVID-19 Dashboard. 2022. Available online: https://africacdc.org/covid-19/ (accessed on 25 February 2022).
- Roda, W.C.; Varughese, M.B.; Han, D.; Li, M.Y. Why is it difficult to accurately predict the COVID-19 epidemic? Infect. Dis. Model. 2020, 5, 271–281. [Google Scholar] [CrossRef]
- Kimball, A.; Hatfield, K.M.; Arons, M.; James, A.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; Tanwar, S.; Chisty, Z. Asymptomatic and presymptomatic SARS-CoV-2 infections in residents of a long-term care skilled nursing facility—King County, Washington, March 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 377. [Google Scholar] [CrossRef] [Green Version]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [Green Version]
- Sood, N.; Simon, P.; Ebner, P.; Eichner, D.; Reynolds, J.; Bendavid, E.; Bhattacharya, J. Seroprevalence of SARS-CoV-2–Specific Antibodies Among Adults in Los Angeles County, California, on April 10–11, 2020. JAMA 2020, 323, 2425–2427. [Google Scholar] [CrossRef]
- Xu, X.; Sun, J.; Nie, S.; Li, H.; Kong, Y.; Liang, M.; Hou, J.; Huang, X.; Li, D.; Ma, T.; et al. Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China. Nat. Med. 2020, 26, 1193–1195. [Google Scholar] [CrossRef]
- Le Vu, S.; Jones, G.; Anna, F.; Rose, T.; Richard, J.-B.; Bernard-Stoecklin, S.; Goyard, S.; Demeret, C.; Helynck, O.; Escriou, N.; et al. Prevalence of SARS-CoV-2 antibodies in France: Results from nationwide serological surveillance. Nat. Commun. 2021, 12, 3025. [Google Scholar] [CrossRef]
- Munster, V.J.; Koopmans, M.; van Doremalen, N.; van Riel, D.; de Wit, E. A novel coronavirus emerging in China—key questions for impact assessment. N. Engl. J. Med. 2020, 382, 692–694. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Alam, S.S.; Kundu, S.; Hossan, T.; Kamal, M.A.; Cavestro, C.J. Prevalence of headache in patients with coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis of 14,275 patients. Front. Neurol. 2020, 11, 562634. [Google Scholar] [CrossRef] [PubMed]
- Saniasiaya, J.; Islam, M.A.; Abdullah, B.J.O.H.; Surgery, N. Prevalence and characteristics of taste disorders in cases of COVID-19: A meta-analysis of 29,349 patients. Otolaryngol. Head Neck Surg. 2021, 165, 33–42. [Google Scholar] [CrossRef]
- Hajissa, K.; Islam, M.A.; Sanyang, A.M.; Mohamed, Z. Prevalence of intestinal protozoan parasites among school children in africa: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2022, 16, e0009971. [Google Scholar] [CrossRef]
- Chang, C.-T.; Ang, J.-Y.; Islam, M.A.; Chan, H.-K.; Cheah, W.-K.; Gan, S.H. Prevalence of Drug-Related Problems and Complementary and Alternative Medicine Use in Malaysia: A Systematic Review and Meta-Analysis of 37,249 Older Adults. Pharmaceuticals 2021, 14, 187. [Google Scholar] [CrossRef]
- Abdella, S.; Riou, S.; Tessema, M.; Assefa, A.; Seifu, A.; Blachman, A.; Abera, A.; Moreno, N.; Irarrazaval, F.; Tollera, G.; et al. Prevalence of SARS-CoV-2 in urban and rural Ethiopia: Randomized household serosurveys reveal level of spread during the first wave of the pandemic. EClinicalMedicine 2021, 35, 100880. [Google Scholar] [CrossRef]
- Abdelmoniem, R.; Fouad, R.; Shawky, S.; Amer, K.; Elnagdy, T.; Hassan, W.A.; Ali, A.M.; Ezzelarab, M.; Gaber, Y.; Badary, H.A.; et al. SARS-CoV-2 infection among asymptomatic healthcare workers of the emergency department in a tertiary care facility. J. Clin. Virol. 2021, 134, 104710. [Google Scholar] [CrossRef]
- Adetifa, I.M.; Uyoga, S.; Gitonga, J.N.; Mugo, D.; Otiende, M.; Nyagwange, J.; Karanja, H.K.; Tuju, J.; Wanjiku, P.; Aman, R.; et al. Temporal trends of SARS-CoV-2 seroprevalence in transfusion blood donors during the first wave of the COVID-19 epidemic in Kenya. medRxiv 2021. [Google Scholar] [CrossRef]
- Assefa, N.; Regassa, L.D.; Teklemariam, Z.; Oundo, J.; Madrid, L.; Dessie, Y.; Scott, J. Seroprevalence of anti-SARS-CoV-2 antibodies in women attending antenatal care in eastern Ethiopia: A facility-based surveillance. BMJ Open 2021, 11, e055834. [Google Scholar] [CrossRef]
- Batchi-Bouyou, A.L.; Ingoba, L.L.; Ndounga, M.; Vouvoungui, J.C.; Mapanguy, C.C.M.; Boumpoutou, K.R.; Ntoumi, F.J.D. High SARS-CoV-2 IgG/IGM seroprevalence in asymptomatic Congolese in Brazzaville, the Republic of Congo. Int. J. Infect. Dis. 2021, 106, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Chibwana, M.; Jere, K.; Kamng’ona, R.; Mandolo, J.; Katunga-Phiri, V.; Tembo, D.; Mitole, N.; Musasa, S.; Sichone, S.; Lakudzala, A.; et al. High SARS-CoV-2 seroprevalence in health care workers but relatively low numbers of deaths in urban Malawi [version 2; peer review: 2 approved]. Wellcome Open Res. 2020, 5, 199. [Google Scholar] [CrossRef]
- Etyang, A.O.; Lucinde, R.; Karanja, H.; Kalu, C.; Mugo, D.; Nyagwange, J.; Gitonga, J.; Tuju, J.; Wanjiku, P.; Karani, A.; et al. Seroprevalence of Antibodies to SARS-CoV-2 among Health Care Workers in Kenya. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 74, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Fai, K.N.; Corine, T.M.; Bebell, L.M.; Mbroingong, A.B.; Nguimbis, E.T.; Nsaibirni, R.; Mbarga, N.F.; Eteki, L.; Nikolay, B.; Essomba, R.G. Serologic Response to SARS-CoV-2 in an African Population. Sci. Afr. 2021, 12, e00802. [Google Scholar] [CrossRef] [PubMed]
- Fwoloshi, S.; Hines, J.Z.; Barradas, D.T.; Yingst, S.; Siwingwa, M.; Chirwa, L.; Zulu, J.E.; Banda, D.; Wolkon, A.; Nikoi, K. Prevalence of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) among Health Care Workers—Zambia, July 2020. Clin. Infect. Dis. 2021, 3, e1321–e1328. [Google Scholar] [CrossRef]
- George, J.A.; Khoza, S.; Mayne, E.; Dlamini, S.; Kone, N.; Jassat, W.; Chetty, K.; Centner, C.M.; Pillay, T.; Maphayi, M.; et al. Sentinel seroprevalence of SARS-CoV-2 in Gauteng Province, South Africa, August—October 2020. South Afr. Med. J. Suid-Afrik. Tydskr. Vir Geneeskd. 2021, 111, 1078–1083. [Google Scholar] [CrossRef]
- Goldblatt, D.; Johnson, M.; Falup-Pecurariu, O.; Ivaskeviciene, I.; Spoulou, V.; Tamm, E.; Wagner, M.; Zar, H.J.; Bleotu, L.; Ivaskevicius, R.; et al. Cross-sectional prevalence of SARS-CoV-2 antibodies in healthcare workers in paediatric facilities in eight countries. J. Hosp. Infect. 2021, 110, 60–66. [Google Scholar] [CrossRef]
- Halatoko, W.A.; Konu, Y.R.; Gbeasor-Komlanvi, F.A.; Sadio, A.J.; Tchankoni, M.K.; Komlanvi, K.S.; Salou, M.; Dorkenoo, A.M.; Maman, I.; Agbobli, A.J. Prevalence of SARS-CoV-2 among high-risk populations in Lomé (Togo) in 2020. PLoS ONE 2020, 15, e0242124. [Google Scholar] [CrossRef]
- Kagucia, E.W.; Gitonga, J.N.; Kalu, C.; Ochomo, E.; Ochieng, B.; Kuya, N.; Karani, A.; Nyagwange, J.; Karia, B.; Mugo, D.; et al. Anti-SARS-CoV-2 IgG antibody seroprevalence among truck drivers and assistants in Kenya. Open Forum Infect. Dis. 2021, 8, ofab314. [Google Scholar] [CrossRef]
- Kammon, A.M.; El-Arabi, A.A.; Erhouma, E.A.; Mehemed, T.M.; Mohamed, O.A. Seroprevalence of antibodies against SARS-CoV-2 among public community and health-care workers in Alzintan City of Libya. medRxiv 2020. [Google Scholar] [CrossRef]
- Kassem, A.M.; Talaat, H.; Shawky, S.; Fouad, R.; Amer, K.; Elnagdy, T.; Hassan, W.A.; Tantawi, O.; Abdelmoniem, R.; Gaber, Y.; et al. SARS-CoV-2 infection among healthcare workers of a gastroenterological service in a tertiary care facility. Arab. J. Gastroenterol. 2020, 21, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Katchunga, P.B.; Murhula, A.; Akilimali, P.; Zaluka, J.C.; Karhikalembu, R.; Makombo, M.; Bisimwa, J.; Mubalama, E. Séroprévalence des anticorps anti-SARS-CoV-2 parmi les voyageurs et travailleurs dépistés à la clinique Saint Luc de Bukavu, à l’Est de la République Démocratique du Congo, de mai en août 2020. Pan Afr. Med. J. 2021, 38, 93. [Google Scholar] [CrossRef] [PubMed]
- Kempen, J.H.; Abashawl, A.; Suga, H.K.; Difabachew, M.N.; Kempen, C.J.; Debele, M.T.; Menkir, A.A.; Assefa, M.T.; Asfaw, E.H.; Habtegabriel, L.B.; et al. SARS-CoV-2 Serosurvey in Addis Ababa, Ethiopia. Am. J. Trop. Med. Hyg. 2020, 103, 2022–2023. [Google Scholar] [CrossRef] [PubMed]
- Milleliri, J.M.; Coulibaly, D.; Nyobe, B.; Rey, J.-L.; Lamontagne, F.; Hocqueloux, L.; Giaché, S.; Valery, A.; Prazuck, T. SARS-CoV-2 infection in Ivory Coast: A serosurveillance survey among gold mine workers. Am. J. Trop. Med. Hyg. 2021, 104, 1709. [Google Scholar] [CrossRef]
- Mostafa, A.; Kandil, S.; El-Sayed, M.H.; Girgis, S.; Hafez, H.; Yosef, M.; Saber, S.; Ezzelarab, H.; Ramadan, M.; Algohary, E.; et al. SARS-CoV-2 seroconversion among 4040 Egyptian healthcare workers in 12 resource-limited healthcare facilities: A prospective cohort study. Int. J. Infect. Dis. 2021, 104, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, A.; Afishawy, M.; Alkhatib, E.; Hosny, M.; Ollaek, M.; Elsayed, A.; Salem, M.R.; Ghaith, D. Asymptomatic SARS-CoV-2 infection among healthcare workers in a non-COVID-19 Teaching University Hospital. J. Public Health Res. 2021, 10, 2102. [Google Scholar] [CrossRef] [PubMed]
- Mukwege, D.; Byabene, A.K.; Akonkwa, E.M.; Dahma, H.; Dauby, N.; Buhendwa, J.-P.C.; Le Coadou, A.; Montesinos, I.; Bruyneel, M.; Cadière, G.-B.; et al. High SARS-CoV-2 Seroprevalence in Healthcare Workers in Bukavu, Eastern Democratic Republic of Congo. Am. J. Trop. Med. Hyg. 2021, 104, 1526. [Google Scholar] [CrossRef]
- Mulenga, L.B.; Hines, J.Z.; Fwoloshi, S.; Chirwa, L.; Siwingwa, M.; Yingst, S.; Wolkon, A.; Barradas, D.T.; Favaloro, J.; Zulu, J.E.; et al. Prevalence of SARS-CoV-2 in six districts in Zambia in July, 2020: A cross-sectional cluster sample survey. Lancet Glob. Health 2021, 9, e773–e781. [Google Scholar] [CrossRef]
- Nega, B.; Addissie, A.; Mamo, G.; Deyessa, N.; Abebe, T.; Abagero, A.; Ayele, W.; Abebe, W.; Haile, T.; Argaw, R.; et al. Sero-prevalence of anti-SARS-CoV-2 Antibodies in Addis Ababa, Ethiopia. bioRxiv 2020. [Google Scholar] [CrossRef]
- Ngere, I.A.; Dawa, J.; Hunsperger, E.; Otieno, N.; Masika, M.; Amoth, P.; Makayotto, L.; Nasimiyu, C.; Gunn, B.M.; Nyawanda, B.; et al. High seroprevalence of SARS-CoV-2 but low infection fatality ratio eight months after introduction in Nairobi, Kenya. Int. J. Infect. Dis. 2021, 112, 25–34. [Google Scholar] [CrossRef]
- Nkuba, A.N.; Makiala, S.M.; Guichet, E.; Tshiminyi, P.M.; Bazitama, Y.M.; Yambayamba, M.K.; Kazenza, B.M.; Kabeya, T.M.; Matungulu, E.B.; Baketana, L.K.; et al. High prevalence of anti-SARS-CoV-2 antibodies after the first wave of COVID-19 in Kinshasa, Democratic Republic of the Congo: Results of a cross-sectional household-based survey. Wellcome Open Res. 2021, 6, 173. [Google Scholar] [CrossRef]
- Nwosu, K.; Fokam, J.; Wanda, F.; Mama, L.; Orel, E.; Ray, N.; Meke, J.; Tassegning, A.; Takou, D.; Mimbe, E.; et al. SARS-CoV-2 antibody seroprevalence and associated risk factors in an urban district in Cameroon. Nat. Commun. 2021, 12, 5851. [Google Scholar] [CrossRef] [PubMed]
- Olayanju, O.; Bamidele, O.; Edem, F.; Eseile, B.; Amoo, A.; Nwaokenye, J.; Udeh, C.; Oluwole, G.; Odok, G.; Awah, N. SARS-CoV-2 Seropositivity in Asymptomatic Frontline Health Workers in Ibadan, Nigeria. Am. J. Trop. Med. Hyg. 2021, 104, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Quashie, P.K.; Mutungi, J.K.; Dzabeng, F.; Oduro-Mensah, D.; Opurum, P.C.; Tapela, K.; Udoakang, A.J.; Asante, I.; Paemka, L.; WACCBIP COVID-19 Team. Trends of SARS-CoV-2 antibody prevalence in selected regions across Ghana. medRxiv 2021. [Google Scholar] [CrossRef]
- Rusakaniko, S.; Sibanda, E.N.; Mduluza, T.; Tagwireyi, P.; Dhlamini, Z.; Ndhlovu, C.E.; Chandiwana, P.; Chiwambutsa, S.; Lim, R.M.; Scott, F. SARS-CoV-2 Serological testing in frontline health workers in Zimbabwe. PLoS Negl. Trop. Dis. 2021, 15, e0009254. [Google Scholar] [CrossRef]
- Sebastião, C.S.; Galangue, M.; Gaston, C.; Van-Dunen, R.; Jandondo, D.; Neto, Z.; de Vasconcelos, J.N.; Morais, J. Serological identification of past and recent SARS-CoV-2 infection through antibody screening in Luanda, Angola. Health Sci. Rep. 2021, 4, e280. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.A.; Meiring, M.; Cummins, T.; Chegou, N.N.; Claassen, C.; Du Plessis, N.; Flinn, M.; Hiemstra, A.; Kleynhans, L.; Leukes, V.; et al. Higher SARS-CoV-2 seroprevalence in workers with lower socioeconomic status in Cape Town, South Africa. PLoS ONE 2021, 16, e0247852. [Google Scholar] [CrossRef]
- Shaweno, T.; Abdulhamid, I.; Bezabih, L.; Teshome, D.; Derese, B.; Tafesse, H.; Shaweno, D. Seroprevalence of SARS-CoV-2 antibody among individuals aged above 15 years and residing in congregate settings in Dire Dawa city administration, Ethiopia. Trop. Med. Health 2021, 49, 55. [Google Scholar] [CrossRef] [PubMed]
- Uyoga, S.; Adetifa, I.M.; Karanja, H.K.; Nyagwange, J.; Tuju, J.; Wanjiku, P.; Aman, R.; Mwangangi, M.; Amoth, P.; Kasera, K.J.S. Seroprevalence of anti–SARS-CoV-2 IgG antibodies in Kenyan blood donors. Science 2021, 371, 79–82. [Google Scholar] [CrossRef]
- Wiens, K.E.; Mawien, P.N.; Rumunu, J.; Slater, D.; Jones, F.K.; Moheed, S.; Caflisch, A.; Bior, B.K.; Jacob, I.A.; Lako, R.L.; et al. Seroprevalence of Severe Acute Respiratory Syndrome Coronavirus 2 IgG in Juba, South Sudan, 2020(1). Emerg. Infect. Dis. 2021, 27, 1598–1606. [Google Scholar] [CrossRef]
- Zarmouh, A.; Elaswdi, H.; Elakhtel, E.; Abufalgha, K.; Taraina, M. Epidemiology of COVID-19 in Misrata, Libya: A Population-Based Surveillance Study. Open J. Epidemiol. 2021, 11, 101. [Google Scholar] [CrossRef]
- Shakiba, M.; Nazari, S.S.H.; Mehrabian, F.; Rezvani, S.M.; Ghasempour, Z.; Heidarzadeh, A. Seroprevalence of COVID-19 virus infection in Guilan province, Iran. medRxiv 2020. [Google Scholar] [CrossRef]
- Doi, A.; Iwata, K.; Kuroda, H.; Hasuike, T.; Nasu, S.; Kanda, A.; Nagao, T.; Nishioka, H.; Tomii, K.; Morimoto, T. Estimation of seroprevalence of novel coronavirus disease (COVID-19) using preserved serum at an outpatient setting in Kobe, Japan: A cross-sectional study. Clin. Epidemiol. Glob. Health 2020, 11, 100–747. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.; Riahi, S.M.; Shiadeh, M.N.; Esfandyari, S.; Mokdad, A.H.; Hotez, P.J.; Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 27, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Bobrovitz, N.; Arora, R.K.; Cao, C.; Boucher, E.; Liu, M.; Donnici, C.; Yanes-Lane, M.; Whelan, M.; Perlman-Arrow, S.; Chen, J. Global seroprevalence of SARS-CoV-2 antibodies: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0252617. [Google Scholar] [CrossRef]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; De Ridder, D.; Petrovic, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): A population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Zejda, J.E.; Brożek, G.M.; Kowalska, M.; Barański, K.; Kaleta-Pilarska, A.; Nowakowski, A.; Xia, Y.; Buszman, P. Seroprevalence of Anti-SARS-CoV-2 antibodies in a random sample of inhabitants of the katowice region, Poland. Int. J. Environ. Res. Public Health 2021, 18, 3188. [Google Scholar] [CrossRef]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra-Walker, R.; Tedrow, J.; Bogan, A.; et al. COVID-19 antibody seroprevalence in Santa Clara County, California. Int. J. Epidemiol. 2021, 50, 410–419. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Tesoriero, J.M.; Rosenthal, E.M.; Chung, R.; Barranco, M.A.; Styer, L.M.; Parker, M.M.; John Leung, S.-Y.; Morne, J.E.; Greene, D.; et al. Cumulative incidence and diagnosis of SARS-CoV-2 infection in New York. Ann. Epidemiol. 2020, 48, 23–29.e24. [Google Scholar] [CrossRef]
- Murhekar, M.V.; Bhatnagar, T.; Selvaraju, S.; Saravanakumar, V.; Thangaraj, J.W.V.; Shah, N.; Kumar, M.S.; Rade, K.; Sabarinathan, R.; Asthana, S.; et al. SARS-CoV-2 antibody seroprevalence in India, August–September, 2020: Findings from the second nationwide household serosurvey. Lancet Glob. Health 2021, 9, e257–e266. [Google Scholar] [CrossRef]
- Hallal, P.C.; Hartwig, F.P.; Horta, B.L.; Silveira, M.F.; Struchiner, C.J.; Vidaletti, L.P.; Neumann, N.A.; Pellanda, L.C.; Dellagostin, O.A.; Burattini, M.N.; et al. SARS-CoV-2 antibody prevalence in Brazil: Results from two successive nationwide serological household surveys. Lancet Glob. Health 2020, 8, e1390–e1398. [Google Scholar] [CrossRef]
- Naranbhai, V.; Chang, C.C.; Beltran, W.F.G.; Miller, T.E.; Astudillo, M.G.; Villalba, J.A.; Yang, D.; Gelfand, J.; Bernstein, B.E.; Feldman, J.; et al. High Seroprevalence of Anti-SARS-CoV-2 Antibodies in Chelsea, Massachusetts. J. Infect. Dis. 2020, 222, 1955–1959. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, J.F.; Hoffman, T.; Esmaeilzadeh, M.; Olsen, B.; Winter, R.; Amer, S.; Molnár, C.; Svalberg, A.; Lundkvist, Å. High seroprevalence of SARS-CoV-2 in elderly care employees in Sweden. Infect. Ecol. Epidemiol. 2020, 10, 1789036. [Google Scholar] [CrossRef]
- George, C.E.; Inbaraj, L.R.; Chandrasingh, S.; de Witte, L.P. High seroprevalence of COVID-19 infection in a large slum in South India; what does it tell us about managing a pandemic and beyond? Epidemiol. Infect. 2021, 149, e39. [Google Scholar] [CrossRef] [PubMed]
- West, R.; Kobokovich, A.; Connell, N.; Gronvall, G.K. COVID-19 Antibody Tests: A Valuable Public Health Tool with Limited Relevance to Individuals. Trends Microbiol. 2020, 29, 214–223. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody Responses to SARS-CoV-2 in Patients With Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Fathi, M.; Vakili, K.; Sayehmiri, F.; Mohamadkhani, A.; Ghanbari, R.; Hajiesmaeili, M.; Rezaei-Tavirani, M. Seroprevalence of Immunoglobulin M and G Antibodies against SARS-CoV-2 Virus: A Systematic Review and Meta-Analysis Study. Iran. J. Immunol. 2021, 18, 34–46. [Google Scholar] [PubMed]
- Canova, V.; Lederer Schläpfer, H.; Piso, R.J.; Droll, A.; Fenner, L.; Hoffmann, T.; Hoffmann, M. Transmission risk of SARS-CoV-2 to healthcare workers–observational results of a primary care hospital contact tracing. Swiss Med. Wkly. 2020, 150, w20257. [Google Scholar] [CrossRef]
- Wilson, N.; Norton, A.; Young, F.; Collins, D. Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: A narrative review. Anaesthesia 2020, 75, 1086–1095. [Google Scholar] [CrossRef]
- Godderis, L.; Boone, A.; Bakusic, J. COVID-19: A new work-related disease threatening healthcare workers. Occup. Med. 2020, 70, 315–316. [Google Scholar] [CrossRef] [PubMed]
- Hossain, A.; Nasrullah, S.M.; Tasnim, Z.; Hasan, M.K.; Hasan, M.M. Seroprevalence of SARS-CoV-2 IgG antibodies among health care workers prior to vaccine administration in Europe, the USA and East Asia: A systematic review and meta-analysis. EClinicalMedicine 2021, 33, 100770. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Seroprevalence of SARS-CoV-2 antibodies and associated factors in health care workers: A systematic review and meta-analysis. J. Hosp. Infect. 2020, 108, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Sahu, A.K.; Amrithanand, V.; Mathew, R.; Aggarwal, P.; Nayer, J.; Bhoi, S. COVID-19 in health care workers–A systematic review and meta-analysis. Am. J. Emerg. Med. 2020, 38, 1727–1731. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G.; Brüggemann, Y.; Kaba, H.E.J.; Steinmann, J.; Pfaender, S.; Scheithauer, S.; Steinmann, E. Potential sources, modes of transmission and effectiveness of prevention measures against SARS-CoV-2. J. Hosp. Infect. 2020, 106, 678–697. [Google Scholar] [CrossRef]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions With the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [Green Version]
- Castilla, J.; Fresán, U.; Trobajo-Sanmartín, C.; Guevara, M. Altitude and SARS-CoV-2 Infection in the First Pandemic Wave in Spain. Int. J. Environ. Res. Public Health 2021, 18, 2578. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study ID [References] | Country | Study Period | Sample Size | Target Population | Recruitment Location | Method | Investigated Antibodies |
|---|---|---|---|---|---|---|---|
| Abdella 2021 [19] | Ethiopia | July to September 2020 | 1856 | General population | Community based | RDT | IgM/IgG |
| Abdelmoniem 2021 [20] | Egypt | 1 to 14 June 2020 | 203 | HCWs | Hospital | RDT | IgM and IgG |
| Adetifa 2021 [21] | Kenya | April to September 2020 | 9922 | Blood donors | Blood transfusion centre | ELISA | IgG |
| Assefa 2021 [22] | Ethiopia | March to April 2021 | 1447 | Pregnant women | Health facilities | RDT | Total antibodies |
| Batchi-Bouyou 2021 [23] | The Republic of Congo | April to July 2020 | 754 | General population | Community based | RDT | IgM and IgG |
| Chibwana 2020 [24] | Malawi | 22 May to 19 June 2020 | 500 | HCWs | Hospital | ELISA | IgG |
| Etyang 2021 [25] | Kenya | 30 July to 4 December 2020 | 684 | HCWs | Hospital | ELISA | IgG |
| Fai 2021 [26] | Cameroon | June to August 2020 | 999 | Symptomatic and Asymptomatic | Community and Hospital | RDT | IgM and IgG |
| Fwoloshi 2021 [27] | Zambia | July 2020 | 575 | HCWs | Health facilities | ELISA | IgG |
| George 2021 [28] | South Africa | August to October 2020 | 6477 | Outpatient | Hospital | CLIA | IgM and IgG |
| Goldblatt 2021 [29] | South Africa | 1 May to mid-July 2020 | 222 | HCWs | Hospital | ELISA | IgG |
| Halatoko 2020 [30] | Togo | April to May 2020 | 955 | Non-Specific | Multiple settings | RDT | IgM and IgG |
| Kagucia 2021 [31] | Kenya | September to October 2020 | 830 | Others | Community based | ELISA | IgG |
| Kammon 2020 [32] | Libya | April to May 2020 | 219 | General population | Community and Hospital | RDT | IgM/IgG |
| Kassem 2020 [33] | Egypt | 1 to 14 June 2020 | 74 | HCWs | Hospital | RDT | IgM and IgG |
| Katchunga 2021 [34] | DRC | May to August 2020 | 684 | Others | Health facilities | RDT | IgM and IgG |
| Kempen 2020 [35] | Ethiopia | May 2020 | 99 | General population | Health facilities | CMIA | IgG |
| Milleliri 2021 [36] | Ivory Coast | July to October 2020 | 1687 | Others | Community based | RDT | IgG/IgM |
| Mostafa 2021 [37] | Egypt | April to June 2020 | 2282 | HCWs | Health facilities | RDT | IgM and IgG |
| Mukhtar 2021 [38] | Egypt | May to June 2020 | 455 | HCWs | Hospital | RDT and CLIA | IgG |
| Mukwege 2021 [39] | DRC | July to August 2020 | 359 | HCWs | Hospital | RDT and ELISA | IgM and IgG |
| Mulenga 2021 [40] | Zambia | 4 to 27 July 2020 | 2704 | General population | Community based | ELISA | IgG |
| Nega 2020 [41] | Ethiopia | 23 to 28 April 2020 | 301 | General population | Community based | RDT | IgG/IgM |
| Ngere 2021 [42] | Kenya | November 2020 | 1164 | General population | Community based | EIA | IgM and IgG |
| Nkuba 2021 [43] | DRC | October to November 2020 | 1080 | General population | Community based | Luminex-based assay | IgG |
| Nwosu 2021 [44] | Cameroon | October to November 2020 | 971 | General population | Community based | RDT | IgM/IgG |
| Olayanju 2021 [45] | Nigeria | December 2019 to April 2020 | 133 | HCWs | Hospital | ELISA | IgG |
| Quashie 2021 [46] | Ghana | July to September 2020 | 1305 | Non-Specific | Multiple settings | RDT | IgM and IgG |
| Rusakaniko 2021 [47] | Zimbabwe | June 2020 | 635 | HCWs | Health facilities | RDT | IgG and IgM |
| Sebastião 2021 [48] | Angola | July to September 2020 | 660 | General population | community based | ELFA | IgM and IgG |
| Shaw 2021 [49] | South Africa | 17 August to 4 September | 405 | Others | Community based | CMIA | IgG |
| Shaweno 2021 [50] | Ethiopia | June to July 2020 | 684 | General population | Community based | CMIA | IgG |
| Uyoga 2021 [51] | Kenya | April to June 2020 | 3098 | Blood donors | Blood transfusion centre | ELISA | IgG |
| Wiens 2021 [52] | South Sudan | August to September 2020 | 1840 | General population | Community based | ELISA | IgG |
| Zarmouh 2021 [53] | Libya | 18 to 21 April 2020 | 897 | General population | Community based | CLIA | IgM and IgG |
| Subgroups | Pooled Seroprevalence [95% CIs] (%) | Number of Studies Analysed | Total Number of Patients |
|---|---|---|---|
| Antibody isotypes | |||
| Overall IgG | 14.6 [12.2–17.1] | 30 | 34,113 |
| Overall IgM | 11.5 [8.7–14.2] | 15 | 10,882 |
| IgG and IgM | 6.6 [4.9–8.3] | 9 | 7557 |
| Antibody tests | |||
| Rapid diagnostic test | 15.5 [11.0–20.1] | 15 | 14,372 |
| Enzyme-linked immunosorbent assay | 16.5 [12.2–20.8] | 10 | 20,508 |
| Chemiluminescent microparticle immunoassay | 9.8 [0.0–20.7] | 3 | 1188 |
| Chemiluminescence Immunoassay | 15.6 [0.0–39.6] | 2 | 7347 |
| Target population | |||
| General population | 11.7 [7.4–16.0] | 13 | 13,229 |
| Healthcare workers | 16.3 [11.5–21.2] | 11 | 6122 |
| Blood donors | 7.5 [3.8–11.2] | 2 | 13,020 |
| Pregnant women | 5.7 [4.5–6.9] | 1 | 1447 |
| Settings | |||
| Community | 16.7 [11.7–21.8] | 14 | 15,833 |
| Hospital | 21.9 [14.8–29.0] | 9 | 9107 |
| Healthcare facilities | 10.6 [5.1–16.1] | 6 | 5722 |
| Blood transfusion centre | 7.5 [3.8–11.2] | 2 | 13,020 |
| Regions | |||
| Northern Africa | 6.5 [4.1–8.9] | 6 | 4130 |
| Central Africa | 26.5 [14.6–38.4] | 7 | 5507 |
| Eastern Africa | 12.1 [8.8–15.3] | 15 | 26,339 |
| Western Africa | 22.0 [6.7–37.6] | 4 | 4080 |
| Southern Africa | 20.7 [10.4–31.1] | 3 | 7104 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hajissa, K.; Islam, M.A.; Hassan, S.A.; Zaidah, A.R.; Ismail, N.; Mohamed, Z. Seroprevalence of SARS-CoV-2 Antibodies in Africa: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 7257. https://doi.org/10.3390/ijerph19127257
Hajissa K, Islam MA, Hassan SA, Zaidah AR, Ismail N, Mohamed Z. Seroprevalence of SARS-CoV-2 Antibodies in Africa: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(12):7257. https://doi.org/10.3390/ijerph19127257
Chicago/Turabian StyleHajissa, Khalid, Md Asiful Islam, Siti Asma Hassan, Abdul Rahman Zaidah, Nabilah Ismail, and Zeehaida Mohamed. 2022. "Seroprevalence of SARS-CoV-2 Antibodies in Africa: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 12: 7257. https://doi.org/10.3390/ijerph19127257
APA StyleHajissa, K., Islam, M. A., Hassan, S. A., Zaidah, A. R., Ismail, N., & Mohamed, Z. (2022). Seroprevalence of SARS-CoV-2 Antibodies in Africa: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(12), 7257. https://doi.org/10.3390/ijerph19127257