
Retrospective Analysis of Treatment Outcomes of Maxillary Sinusitis Associated with Medication-Related Osteonecrosis of the Jaw

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Ethical Approval
2.3. Data Examined
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment and Outcome of MRONJ
3.3. Procedures for Maxillary Sinus and Outcome of Sinusitis
3.4. Factors Related to Treatment Outcome of Maxillary Sinusitis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrota, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related os-teonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, T.; Japanese Allied Committee on Osteonecrosis of the Jaw; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position Paper 2017 of the Japanese Allied Committee on Osteonecrosis of the Jaw. J. Bone Miner. Metab. 2016, 35, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxil-lofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws-2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Barone, S.; Diodati, F.; Antonelli, A.; Nocini, R.; Cristofaro, M.G. Can Surgical Management Improve Resolution of Medication-Related Osteonecrosis of the Jaw at Early Stages? A Prospective Cohort Study. J. Oral Maxillofac. Surg. 2020, 78, 1986–1999. [Google Scholar] [CrossRef]
- Favia, G.; Tempesta, A.; Limongelli, L.; Crincoli, V.; Maiorano, E. Medication-related osteonecrosis of the jaw: Surgical or non-surgical treatment? Oral Dis. 2018, 24, 238–242. [Google Scholar] [CrossRef]
- Rupel, K.; Ottaviani, G.; Gobbo, M.; Contardo, L.; Tirelli, G.; Vescovi, P.; Di Lenarda, R.; Biasotto, M. A systematic review of therapeutical approaches in bisphosphonates-related osteonecrosis of the jaw (BRONJ). Oral Oncol. 2014, 50, 1049–1057. [Google Scholar] [CrossRef]
- Fliefel, R.; Tröltzsch, M.; Kühnisch, J.; Ehrenfeld, M.; Otto, S. Treatment strategies and outcomes of bisphosphonate-related osteonecrosis of the jaw (BRONJ) with characterization of patients: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 568–585. [Google Scholar] [CrossRef]
- Hayashida, S.; Soutome, S.; Yanamoto, S.; Fujita, S.; Hasegawa, T.; Komori, T.; Kojima, Y.; Miyamoto, H.; Shibuya, Y.; Ueda, N.; et al. Evaluation of the Treatment Strategies for Medication-Related Osteonecrosis of the Jaws (MRONJ) and the Factors Affecting Treatment Outcome: A Multicenter Retrospective Study with Propensity Score Matching Analysis. J. Bone Miner. Res. 2017, 32, 2022–2029. [Google Scholar] [CrossRef] [Green Version]
- Okuyama, K.; Hayashida, S.; Rokutanda, S.; Kawakita, A.; Soutome, S.; Sawada, S.; Yanamoto, S.; Kojima, Y.; Umeda, M. Surgical strategy for medication-related osteonecrosis of the jaw (MRONJ) on maxilla: A multicenter retrospective study. J. Dent. Sci. 2020, 16, 885–890. [Google Scholar] [CrossRef]
- Sawada, S.; Kojima, Y.; Yasui, H.; Kirihigashi, M.; Yun, Y.; Hayashida, S.; Rokutanda, S.; Soutome, S.; Yanamoto, S.; Umeda, M.; et al. Treatment and outcome of maxillary sinusitis associated with maxillary medication-related osteonecrosis. J. Oral Maxillofac. Surg. Med. Pathol. 2021, 33, 408–415. [Google Scholar] [CrossRef]
- Kurabayashi, T.; Ida, M.; Yoshino, N.; Hosokawa, A.; Sasaki, T.; Ishii, J.; Kishi, T.; Kusama, M. Usefulness of CT images for diagnosis of odontogenic maxillary sinusitis. Oral Radiol. 1995, 11, 21–30. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B.; American Association of Oral and Max-illofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related os-teonecrosis of the jaws—2009 Update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar] [PubMed]
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonate-Induced Exposed Bone (Osteonecrosis/Osteopetrosis) of the Jaws: Risk Factors, Recognition, Prevention, and Treatment. J. Oral Maxillofac. Surg. 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- Lazarovici, T.S.; Yahalom, R.; Taicher, S.; Elad, S.; Hardan, I.; Yarom, N. Bisphosphonate-Related Osteonecrosis of the Jaws: A Single-Center Study of 101 Patients. J. Oral Maxillofac. Surg. 2009, 67, 850–855. [Google Scholar] [CrossRef]
- Lerman, M.A.; Xie, W.; Treister, N.S.; Richardson, P.G.; Weller, E.A.; Woo, S.B. Conservative management of bisphospho-nate-related osteonecrosis of the jaws: Staging and treatment outcomes. Oral Oncol. 2013, 49, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Hadaya, D.; Soundia, A.; Freymiller, E.; Grogan, T.; Elashoff, D.; Tetradis, S.; Aghaloo, T.L. Nonsurgical Management of Medication-Related Osteonecrosis of the Jaws Using Local Wound Care. J. Oral Maxillofac. Surg. 2018, 76, 2332–2339. [Google Scholar] [CrossRef]
- Vescovi, P.; Campisi, G.; Fusco, V.; Mergoni, G.; Manfredi, M.; Merigo, E.; Solazzo, L.; Gabriele, M.; Gaeta, G.M.; Favia, G.; et al. Surgery-triggered and non surgery-triggered Bisphosphonate-related Osteonecrosis of the Jaws (BRONJ): A retrospective analysis of 567 cases in an Italian multicenter study. Oral Oncol. 2011, 47, 191–194. [Google Scholar] [CrossRef]
- Mücke, T.; Koschinski, J.; Deppe, H.; Wagenpfeil, S.; Pautke, C.; Mitchell, D.A.; Wolff, K.-D.; Hölzle, F. Outcome of treatment and parameters influencing recurrence in patients with bisphosphonate-related osteonecrosis of the jaws. J. Cancer Res. Clin. Oncol. 2010, 137, 907–913. [Google Scholar] [CrossRef]
- Graziani, F.; Vescovi, P.; Campisi, G.; Favia, G.; Gabriele, M.; Gaeta, G.M.; Gennai, S.; Goia, F.; Miccoli, M.; Peluso, F.; et al. Resective Surgical Approach Shows a High Performance in the Management of Advanced Cases of Bisphosphonate-Related Osteonecrosis of the Jaws: A Retrospective Survey of 347 Cases. J. Oral Maxillofac. Surg. 2012, 70, 2501–2507. [Google Scholar] [CrossRef]
- Vescovi, P.; Merigo, E.; Meleti, M.; Manfredi, M.; Guidotti, R.; Nammour, S. Bisphosphonates-related osteonecrosis of the jaws: A concise review of the literature and a report of a single-centre experience with 151 patients. J. Oral Pathol. Med. 2011, 41, 214–221. [Google Scholar] [CrossRef]
- Jacobsen, C.; Metzler, P.; Obwegeser, J.A.; Zemann, W.; Graetz, K.W. Osteopathology of the jaw associated with bone re-sorption inhibitors: What have we learned in the last 8 years? Swiss Med. Wkly. 2012, 142, w13605. [Google Scholar] [PubMed] [Green Version]
- Schubert, M.; Klatte, I.; Linek, W.; Müller, B.; Döring, K.; Eckelt, U.; Hemprich, A.; Berger, U.; Hendricks, J. The Saxon Bisphosphonate Register–Therapy and prevention of bisphosphonate-related osteonecrosis of the jaws. Oral Oncol. 2012, 48, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Kobn, N. Disease stage and mode of therapy are important determinants of treatment outcome for medica-tionrelated osteonecrosis of the jaw. J. Oral Maxillofac Surg. 2015, 73, S94–S100. [Google Scholar] [CrossRef] [PubMed]
- Mücke, T.; Koerdt, S.; Jung, M.; Mitchell, D.; Wolff, K.-D.; Kesting, M.R.; Loeffelbein, D.J. The role of mylohyoid flap in the treatment of bisphosphonate-related osteonecrosis of the jaws. J. Cranio-Maxillofac. Surg. 2016, 44, 369–373. [Google Scholar] [CrossRef]
- Nisi, M.; La Ferla, F.; Karapetsa, D.; Gennai, S.; Ramaglia, L.; Graziani, F.; Gabriele, M. Conservative surgical management of patients with bisphosphonate-related osteonecrosis of the jaws: A series of 120 patients. Br. J. Oral Maxillofac. Surg. 2016, 54, 930–935. [Google Scholar] [CrossRef]
- Kim, H.Y.; Lee, S.-J.; Kim, S.M.; Myoung, H.; Hwang, S.J.; Choi, J.-Y.; Lee, J.-H.; Choung, P.-H.; Kim, M.J.; Seo, B.M. Extensive Surgical Procedures Result in Better Treatment Outcomes for Bisphosphonate-Related Osteonecrosis of the Jaw in Patients with Osteoporosis. J. Oral Maxillofac. Surg. 2016, 75, 1404–1413. [Google Scholar] [CrossRef] [Green Version]
- Zirk, M.; Kreppel, M.; Buller, J.; Pristup, J.; Peters, F.; Dreiseidler, T.; Zinser, M.; Zöller, J.E. The impact of surgical intervention and antibiotics on MRONJ stage II and III—Retrospective study. J. Cranio-Maxillofac. Surg. 2017, 45, 1183–1189. [Google Scholar] [CrossRef]
- Mast, G.; Otto, S.; Mücke, T.; Schreyer, C.; Bissinger, O.; Kolk, A.; Wolff, K.D.; Ehrenfeld, M.; Stürzenbaum, S.R.; Pautke, C. Incidence of maxillary sinusitis and oro-antral fistulae in bisphosphonate-related osteonecrosis of the jaw. J. Cranio-Maxillofac. Surg. 2012, 40, 568–571. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Yokoi, H.; Ikeda, T.; Kawada, M.; Saito, K. Relationships of opacification in the nasal sinuses, rhinosinusitis, and antiresorptive agent-related osteonecrosis of the jaw. Auris Nasus Larynx 2020, 47, 996–1002. [Google Scholar] [CrossRef]
- Maurer, P.; Sandulescu, T.; Kriwalsky, M.; Rashad, A.; Hollstein, S.; Stricker, I.; Hölzle, F.; Kunkel, M. Bisphosphonate-related osteonecrosis of the maxilla and sinusitis maxillaris. Int. J. Oral Maxillofac. Surg. 2011, 40, 285–291. [Google Scholar] [CrossRef]
- Park, J.; Alfafara, A.M.; Park, Y.L.; Bae, J.; Kim, S. Medication-related osteonecrosis of the maxilla: Prognosis of oral surgery combined with endoscopic sinus surgery. Oral Dis. 2020, 27, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Kawakita, A.; Ueda, N.; Funahara, R.; Tachibana, A.; Kobayashi, M.; Kondou, E.; Takeda, D.; Kojima, Y.; Sato, S.; et al. A multicenter retrospective study of the risk factors associated with medication-related osteonecrosis of the jaw after tooth extraction in patients receiving oral bisphosphonate therapy: Can primary wound closure and a drug holiday really prevent MRONJ? Osteoporos. Int. 2017, 28, 2465–2473. [Google Scholar] [CrossRef] [PubMed]
- Cano-Durán, J.A.; Peña-Cardelles, J.-F.; Ortega-Concepción, D.; Paredes-Rodríguez, V.M.; García-Riart, M.; López-Quiles, J. The role of Leucocyte-rich and platelet-rich fibrin (L-PRF) in the treatment of the medication-related osteonecrosis of the jaws (MRONJ). J. Clin. Exp. Dent. 2017, 9, e1051–e1059. [Google Scholar] [CrossRef] [PubMed]
- Berrone, M.; Florindi, F.U.; Carbone, V.; Aldiano, C.; Pentenero, M. Stage 3 Medication-Related Osteonecrosis of the Posterior Maxilla: Surgical Treatment Using a Pedicled Buccal Fat Pad Flap: Case Reports. J. Oral Maxillofac. Surg. 2015, 73, 2082–2086. [Google Scholar] [CrossRef]
- Jose, A.; Rawat, A.; Nagori, S.A.; Arya, S.; Shukla, D. Outcomes of sequestrectomy and buccal fat pad reconstruction in the management of medication-related osteonecrosis of the jaws. Oral Maxillofac. Surg. 2022, 26, 147–153. [Google Scholar] [CrossRef]
- Freiberger, J.J.; Padilla-Burgos, R.; Chhoeu, A.H.; Kraft, K.H.; Boneta, O.; Moon, R.E.; Piantadosi, C.A. Hyperbaric oxygen treatment and bisphosphonate-induced osteonecrosis of the jaw: A case series. J. Oral Maxillofac. Surg. 2007, 65, 1321–1327. [Google Scholar] [CrossRef]
- Altay, M.A.; Tasar, F.; Tosun, E.; Kan, B. Low-Level Laser Therapy Supported Surgical Treatment of Bisphosphonate Related Osteonecrosis of Jaws: A Retrospective Analysis of 11 Cases. Photomed. Laser Surg. 2014, 32, 468–475. [Google Scholar] [CrossRef]
- Merigo, E.; Cella, L.; Oppici, A.; Cristina Arbasi, M.; Clini, F.; Fontana, M.; Fornaini, C. Combined approach to treat medi-cation-related osteonecrosis of the jaws. J. Lasers Med. Sci. 2018, 9, 92–100. [Google Scholar] [CrossRef] [Green Version]
- Coropciuc, R.; Grisar, K.; Aerden, T.; Schol, M.; Schoenaers, J.; Politis, C. Medication-related osteonecrosis of the jaw in oncological patients with skeletal metastases: Conservative treatment is effective up to stage 2. Br. J. Oral Maxillofac. Surg. 2017, 55, 787–792. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Kim, J.W.; Kim, S.J. Does the addition of bone morphogenetic protein 2 to platelet-rich fibrin improve healing after treatment for medication-related osteonecrosis of the jaw? J. Oral Maxillofac. Surg. 2017, 75, 1176–1184. [Google Scholar] [CrossRef] [Green Version]
- Agrillo, A.; Filiaci, F.; Ramieri, V.; Riccardi, E.; Quarato, D.; Rinna, C.; Gennaro, P.; Cascino, F.; Mitro, V.; Ungari, C. Bisphosphonate-related osteonecrosis of the jaw (BRONJ): 5 year experience in the treatment of 131 cases with ozone therapy. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1741–1747. [Google Scholar]
- Kwon, Y.-D.; Lee, D.-W.; Choi, B.-J.; Lee, J.-W.; Kim, D.-Y. Short-term teriparatide therapy as an adjunctive modality for bisphosphonate-related osteonecrosis of the jaws. Osteoporos. Int. 2012, 23, 2721–2725. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Antonelli, A.; Chiarella, E.; Baudi, F.; Barni, T.; Di Vito, A. The Case of Medication-Related Osteonecrosis of the Jaw Addressed from a Pathogenic Point of View. Innovative Therapeutic Strategies: Focus on the Most Recent Discoveries on Oral Mesenchymal Stem Cell-Derived Exosomes. Pharmaceuticals 2020, 13, 423. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Kim, Y.-N.; Kim, H.; Lee, B.-K. Effect of Human Umbilical Cord Matrix-Derived Mesenchymal Stem Cells on Bisphosphonate-Related Osteonecrosis of the Jaw. Tissue Eng. Regen. Med. 2021, 18, 975–988. [Google Scholar] [CrossRef] [PubMed]
- Ronen, O.; Marshak, T.; Uri, N.; Gruber, M.; Haberfeld, O.; Paz, D.; Stein, N.; Cohen-Kerem, R. Direct maxillary irrigation therapy in non-operated chronic sinusitis: A prospective randomised controlled trial. J. Laryngol. Otol. 2021, 136, 229–236. [Google Scholar] [CrossRef]
- Gay, I.; Elidan, J.; Chisin, R. Irrigation of the Maxillary Sinus by Canine Fossa Puncture: Experience with 202 Patients. Ann. Otol. Rhinol. Laryngol. 1983, 92, 528–529. [Google Scholar] [CrossRef]
- Hong, S.O.; Shim, G.-J.; Kwon, Y.-D. Novel approach to the maxillary sinusitis after sinus graft. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 1–4. [Google Scholar] [CrossRef]
- Kojima, Y.; Kawaoka, Y.; Sawada, S.; Hayashida, S.; Okuyama, K.; Yutori, H.; Kawakita, A.; Ishida, S.; Soutome, S.; Yanamoto, S.; et al. Clinical significance of periosteal reaction as a predictive factor for treatment outcome of medica-tion-related osteonecrosis of the jaw. J. Bone Min. Metab. 2019, 37, 913–919. [Google Scholar] [CrossRef]
- Soutome, S.; Yanamoto, S.; Sumi, M.; Hayashida, S.; Kojima, Y.; Sawada, S.; Rokutanda, S.; Iwai, H.; Saito, T.; Umeda, M. Effect of periosteal reaction in medication-related osteonecrosis of the jaw on treatment outcome after surgery. J. Bone Miner. Metab. 2020, 39, 302–310. [Google Scholar] [CrossRef]
- Soutome, S.; Otsuru, M.; Hayashida, S.; Yanamoto, S.; Sasaki, M.; Takagi, Y.; Sumi, M.; Kojima, Y.; Sawada, S.; Iwai, H.; et al. Periosteal reaction of medication-related osteonecrosis of the jaw (MRONJ): Clinical significance and changes during conservative therapy. Support. Care Cancer 2021, 29, 6361–6368. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number of Patients/Mean ± Standard Division | |
|---|---|---|
| Sex | male | 7 |
| female | 27 | |
| Age | (years) | 74.7 ± 11.7 |
| Primary disease | osteoporosis | 17 |
| malignant tumor | 17 | |
| Stage of MRONJ | stage 1 | 1 |
| stage 2 | 10 | |
| stage 3 | 23 | |
| Antiresorptive agent | BP | 23 |
| Dmab | 7 | |
| BP → Dmab | 4 | |
| Duration of administration | (weeks) | 59.8 ± 37.0 |
| Use of corticosteroid | (−) | 26 |
| (+) | 8 | |
| Diabetes | (−) | 28 |
| (+) | 6 | |
| Leukocyte | (×103/μL) | 6.77 ± 2.86 |
| Albumin | (g/dL) | 3.50 ± 0.45 |
| Sequester separation | (−) | 19 |
| (+) | 15 | |
| Periosteal reaction | (−) | 25 |
| (+) | 9 | |
| Postoperative antibiotics | (−) | 29 |
| (+) | 5 | |
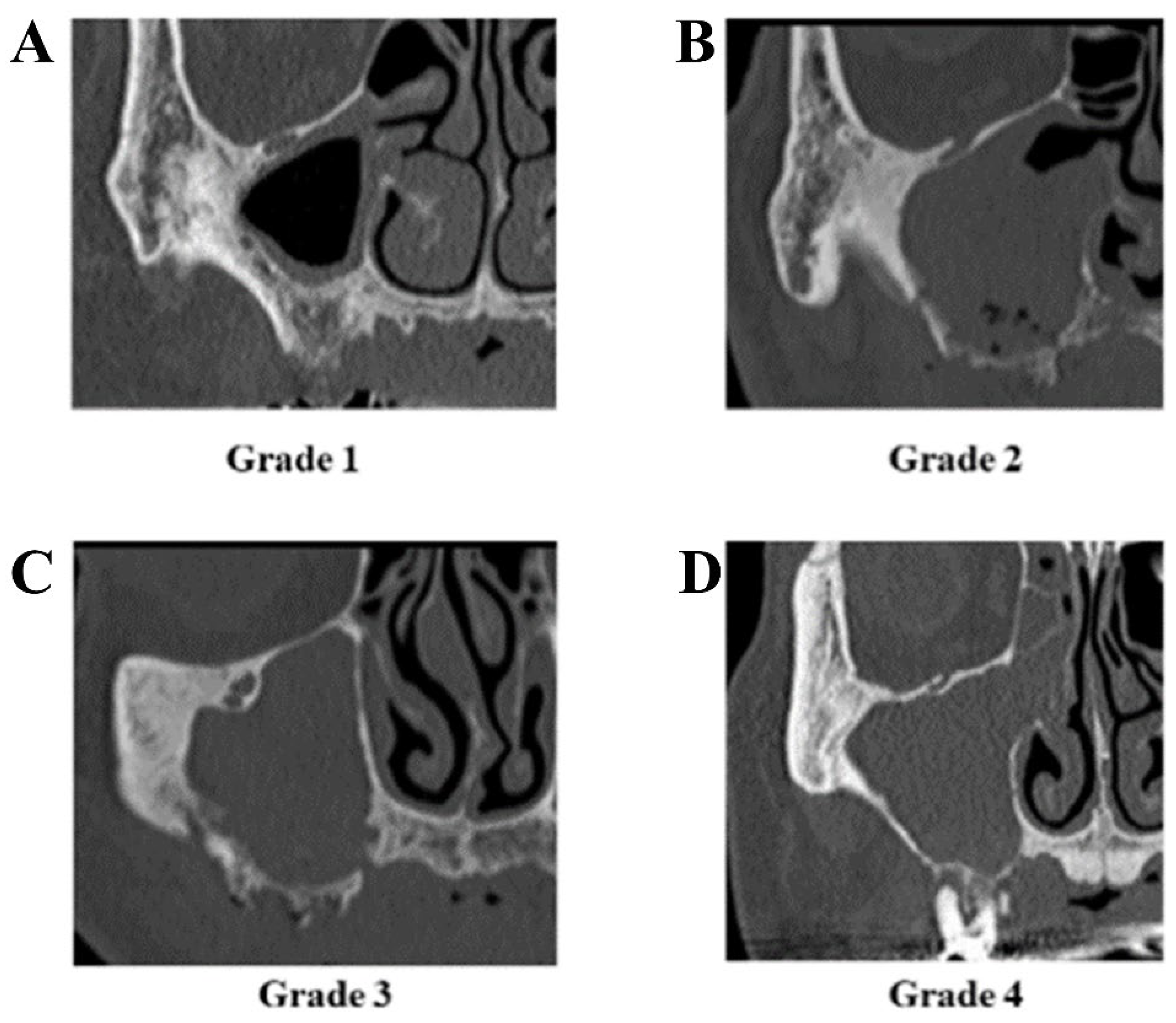
| Grade of sinusitis | grade 1 | 7 |
| grade 2 | 9 | |
| grade 3 | 1 | |
| grade 4 | 17 | |
| Total | 34 |
| Procedures for Maxillary Sinus | Grade of Maxillary Sinusitis | Total | |||
|---|---|---|---|---|---|
| Grade 1 | Grade 2 | Grade 3 | Grade 4 | ||
| None | 7 | 6 | 1 | 7 | 21 |
| Intraoperative irrigation | 0 | 3 | 0 | 10 | 13 |
| Total | 7 | 9 | 1 | 17 | 34 |
| Variable | The Outcome of Maxillary Sinusitis | p-Value | ||
|---|---|---|---|---|
| No Change/Worsening | Improvement | |||
| Sex | male | 2 | 5 | 0.555 |
| female | 11 | 16 | ||
| Age | (years) | 69.7 ± 12.2 | 77.7 ± 10.5 | 0.299 |
| Primary disease | osteoporosis | 5 | 12 | 0.241 |
| malignant tumor | 8 | 9 | ||
| Stage of MRONJ | stage 1–2 | 7 | 4 | 0.042 |
| stage 3 | 6 | 17 | ||
| Antiresorptive agent | BP | 7 | 16 | 0.164 |
| Dmab/BP → Dmab | 6 | 5 | ||
| Duration of administration | (weeks) | 52.9 ± 32.0 | 64.5 ± 40.2 | 0.090 |
| Use of corticosteroid | (−) | 9 | 17 | 0.352 |
| (+) | 4 | 4 | ||
| Diabetes | (−) | 11 | 17 | 0.584 |
| (+) | 2 | 4 | ||
| Leukocyte | (×103/μL) | 6.68 ± 2.38 | 6.83 ± 3.19 | 0.825 |
| Albumin | (g/dL) | 3.40 ± 0.41 | 3.56 ± 0.47 | 0.679 |
| Sequester separation | (−) | 9 | 10 | 0.191 |
| (+) | 4 | 11 | ||
| Periosteal reaction | (−) | 10 | 15 | 0.525 |
| (+) | 3 | 6 | ||
| Postoperative antibiotics | (−) | 11 | 18 | 0.647 |
| (+) | 2 | 3 | ||
| Grade of sinusitis | grade 1–2 | 8 | 8 | 0.164 |
| grade 3–4 | 5 | 13 | ||
| Procedure to the maxillary sinus | none | 10 | 11 | 0.143 |
| irrigation | 3 | 10 | ||
| Outcome of MRONJ | non-healing | 4 | 1 | 0.059 |
| healing | 9 | 20 | ||
| Total | 13 | 21 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otsuru, M.; Hayashida, S.; Morishita, K.; Murata, M.; Soutome, S.; Sasaki, M.; Takagi, Y.; Sumi, M.; Umeda, M. Retrospective Analysis of Treatment Outcomes of Maxillary Sinusitis Associated with Medication-Related Osteonecrosis of the Jaw. Int. J. Environ. Res. Public Health 2022, 19, 7430. https://doi.org/10.3390/ijerph19127430
Otsuru M, Hayashida S, Morishita K, Murata M, Soutome S, Sasaki M, Takagi Y, Sumi M, Umeda M. Retrospective Analysis of Treatment Outcomes of Maxillary Sinusitis Associated with Medication-Related Osteonecrosis of the Jaw. International Journal of Environmental Research and Public Health. 2022; 19(12):7430. https://doi.org/10.3390/ijerph19127430
Chicago/Turabian StyleOtsuru, Mitsunobu, Saki Hayashida, Kota Morishita, Maho Murata, Sakiko Soutome, Miho Sasaki, Yukinori Takagi, Misa Sumi, and Masahiro Umeda. 2022. "Retrospective Analysis of Treatment Outcomes of Maxillary Sinusitis Associated with Medication-Related Osteonecrosis of the Jaw" International Journal of Environmental Research and Public Health 19, no. 12: 7430. https://doi.org/10.3390/ijerph19127430