
RANTES and CD40L under Conditions of Long-Term Physical Exercise: A Potential Link to Adaptive Immunity

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Characterization of the Study Cohort
- Chronic heart disease (CHD) with prior myocardial infarction, CABG, PCI, or stroke.
- Family history of cardiovascular disease or stroke in first-degree relatives (only mother or father).
- The presence of one or more metabolic risk factors including overweight (BMI > 25), diabetes mellitus (HbA1c > 6.5% or the presence of antidiabetic medication), dyslipidemia (marked by statin intake), and arterial hypertension (resting SBP > 140 mmHg/resting DBP > 85 mmHg or the presence of antihypertensive medication).
- A positive smoking status.
2.2. Performance and Continuous Physical Activity
2.3. Bicycle Stress Tests
2.4. Formation of Groups and Subgroups in Accordance with Individual Performance
- Group A = subgroups α and γ (n = 27)
- Group B = subgroups β and δ (n = 71)
- ○
- α: initially unathletic (initial performance < 100%), performance gain ≤ 2.9% (n = 9).
- ○
- β: initially unathletic (initial performance < 100%), performance gain > 2.9% (n = 32).
- ○
- γ: initially athletic (initial performance ≥ 100%), performance gain ≤ 2.9% (n = 18).
- ○
- δ: initially athletic (initial performance ≥ 100%), performance gain > 2.9% (n = 39).
2.5. Laboratory Analysis, RANTES, and CD40L ELISA
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Performance Gain
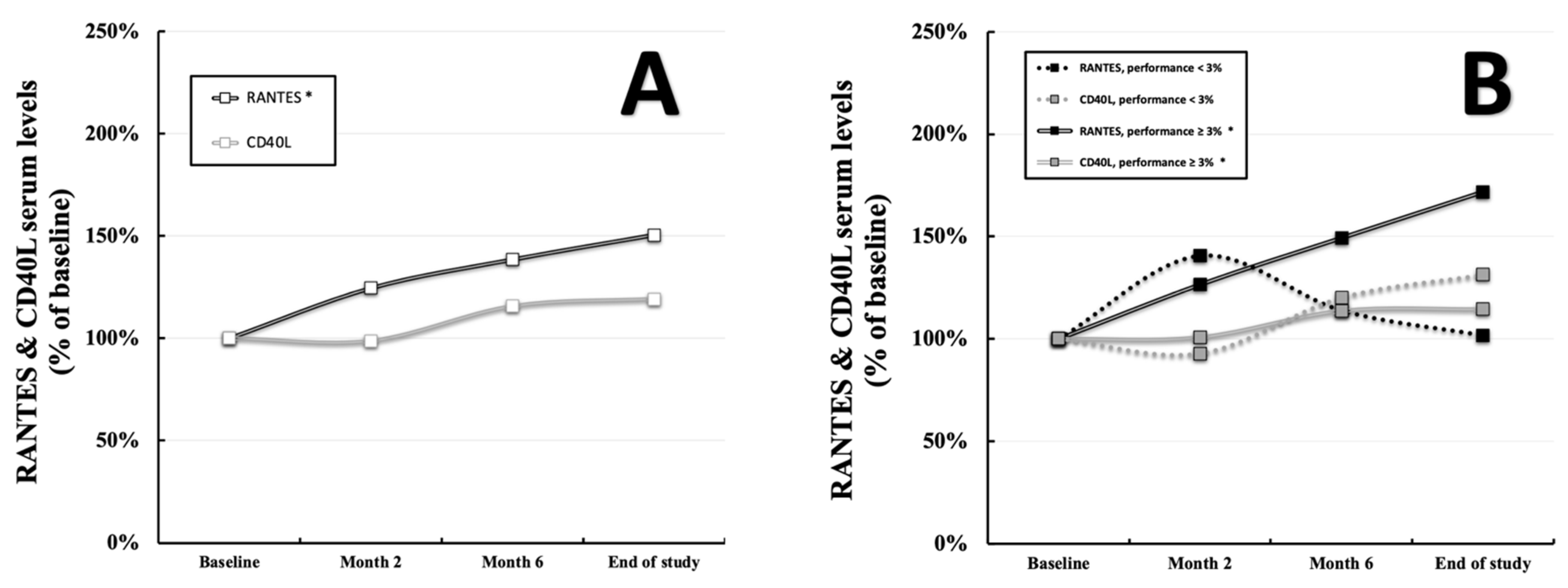
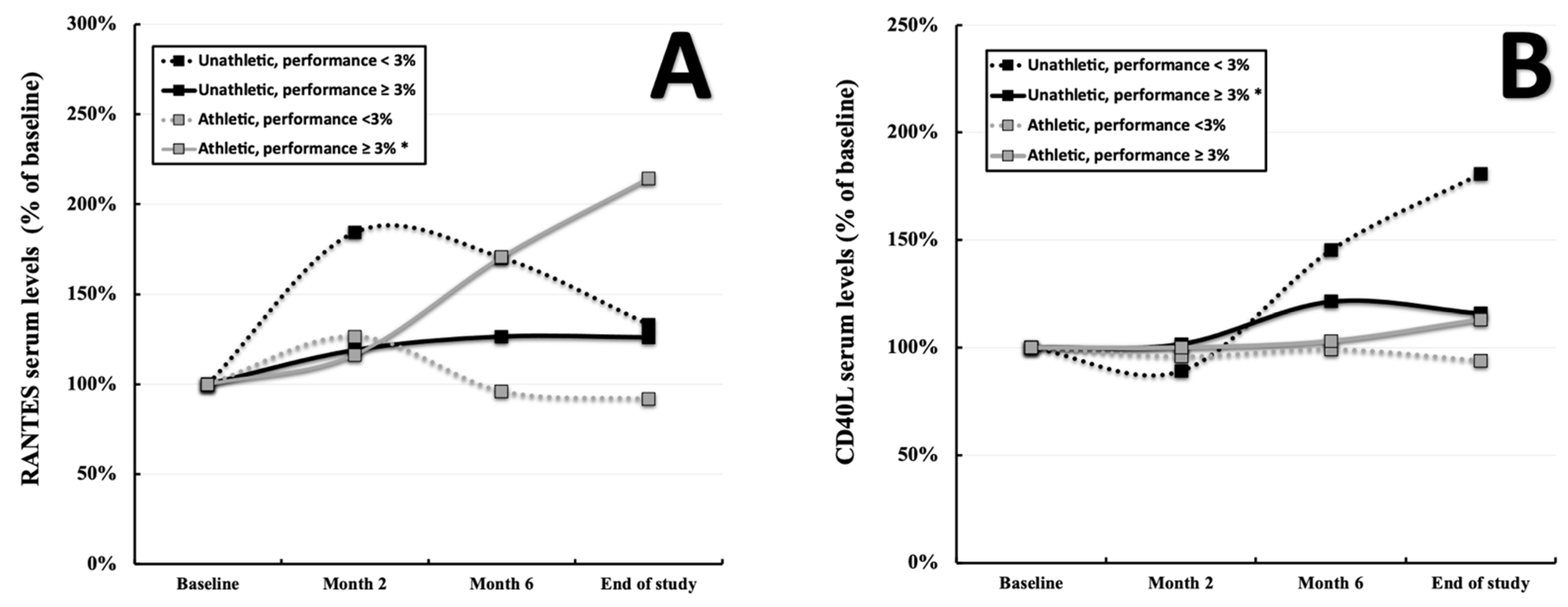
3.2. RANTES and CD40L throughout the Study
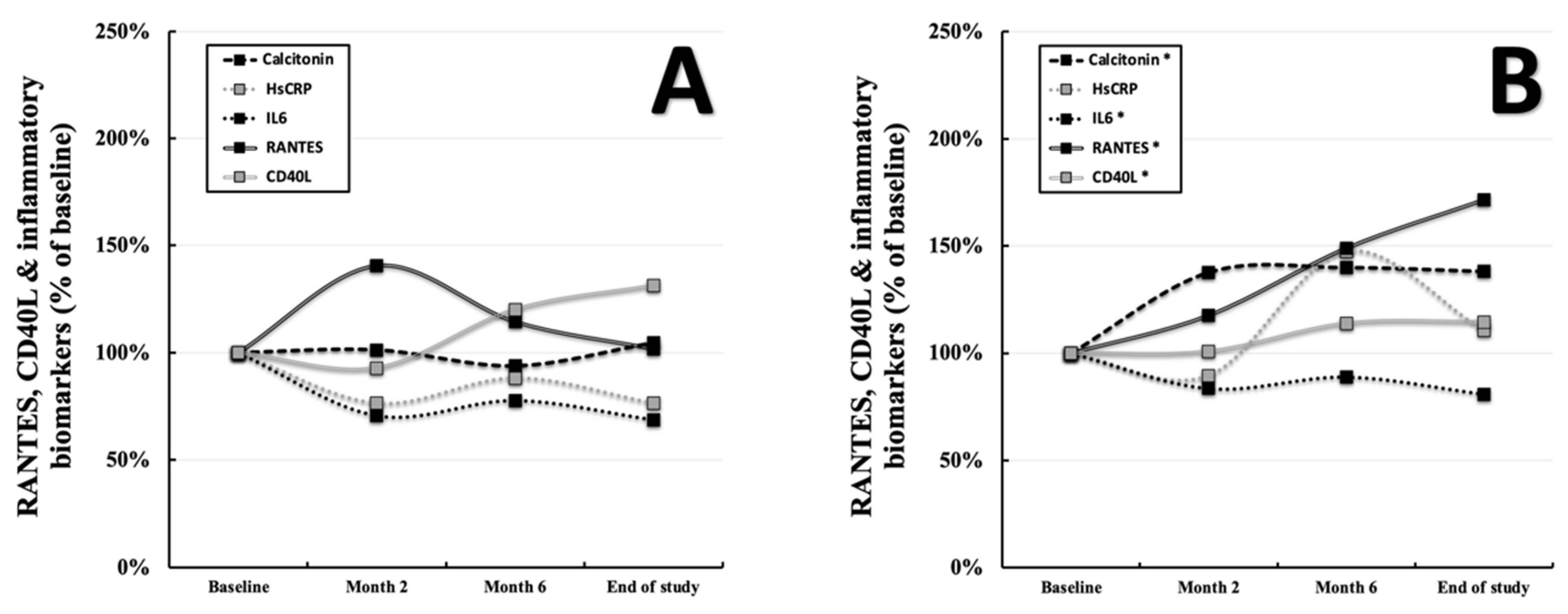
3.3. RANTES, CD40L, and the Development of Inflammatory Biomarkers
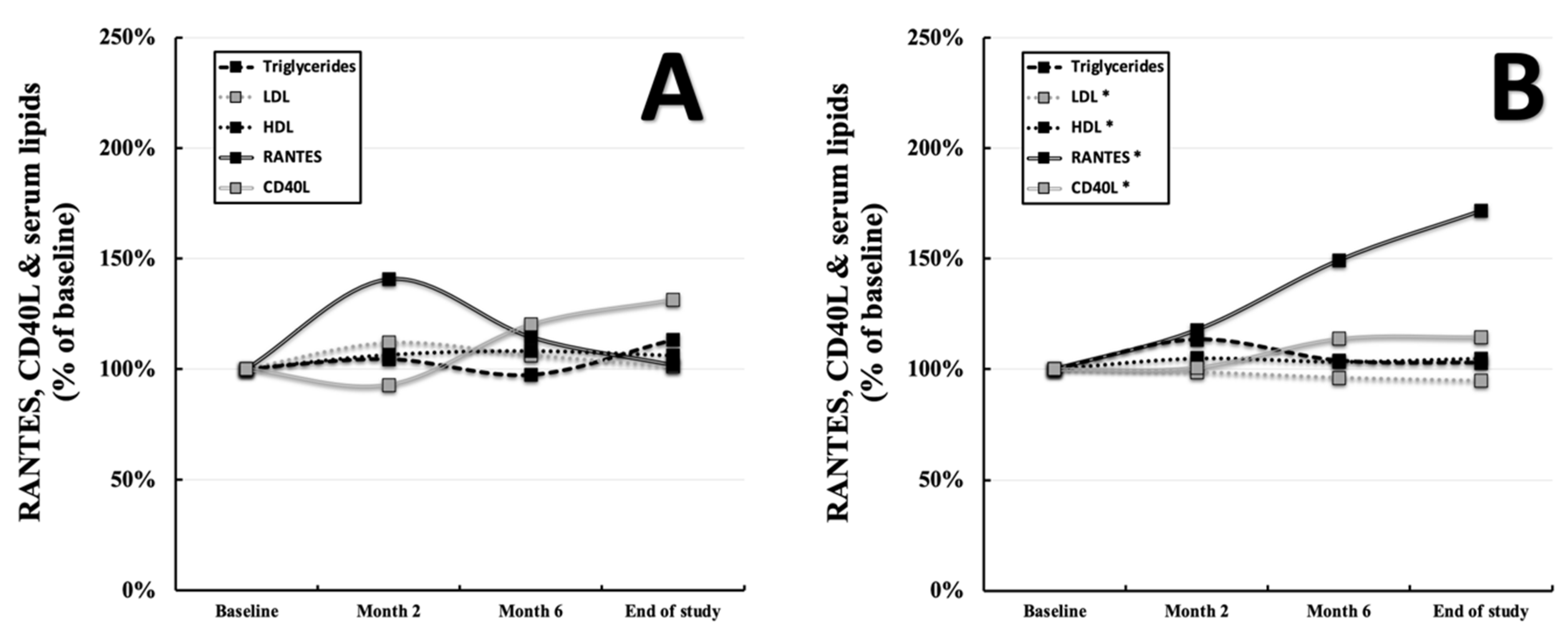
3.4. RANTES, CD40L, and the Development of Serum Lipids
4. Discussion
4.1. Exercise-Induced Changes of RANTES and Inflammatory Markers
4.2. Exercise-Induced Changes of CD40L
4.3. Influence of RANTES and CD40L on Serum Lipids
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef] [PubMed]
- da Silveira, M.P.; da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, É.; Rossi, R.C.; de Resende E Silva, D.T. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2021, 21, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Donlon, T.A.; Krensky, A.M.; Wallace, M.R.; Collins, F.S.; Lovett, M.; Clayberger, C. Localization of a human T-cell-specific gene, RANTES (D17S136E), to chromosome 17q11.2-q12. Genomics 1990, 6, 548–553. [Google Scholar] [CrossRef] [Green Version]
- Blanpain, C.; Buser, R.; Power, C.A.; Edgerton, M.; Buchanan, C.; Mack, M.; Simmons, G.; Clapham, P.R.; Parmentier, M.; Proudfoot, A.E. A chimeric MIP-1alpha/RANTES protein demonstrates the use of different regions of the RANTES protein to bind and activate its receptors. J. Leukoc. Biol. 2001, 69, 977–985. [Google Scholar] [PubMed]
- Schober, A.; Manka, D.; von Hundelshausen, P.; Huo, Y.; Hanrath, P.; Sarembock, I.J.; Ley, K.; Weber, C. Deposition of platelet RANTES triggering monocyte recruitment requires P-selectin and is involved in neointima formation after arterial injury. Circulation 2002, 106, 1523–1529. [Google Scholar] [CrossRef] [Green Version]
- Lechner, J.; von Baehr, V.; Schick, F. RANTES/CCL5 Signaling from Jawbone Cavitations to Epistemology of Multiple Sclerosis-Research and Case Studies. Degener. Neurol. Neuromuscul. Dis. 2021, 11, 41–50. [Google Scholar] [CrossRef]
- Maghazachi, A.A.; Al-Aoukaty, A.; Schall, T.J. CC chemokines induce the generation of killer cells from CD56+ cells. Eur. J. Immunol. 1996, 26, 315–319. [Google Scholar] [CrossRef]
- Culley, F.J.; Pennycook, A.M.; Tregoning, J.S.; Dodd, J.S.; Walzl, G.; Wells, T.N.; Hussell, T.; Openshaw, P.J. Role of CCL5 (RANTES) in viral lung disease. J. Virol. 2006, 80, 8151–8157. [Google Scholar] [CrossRef] [Green Version]
- Tyner, J.W.; Uchida, O.; Kajiwara, N.; Kim, E.Y.; Patel, A.C.; O’Sullivan, M.P.; Walter, M.J.; Schwendener, R.A.; Cook, D.N.; Danoff, T.M.; et al. CCL5-CCR5 interaction provides antiapoptotic signals for macrophage survival during viral infection. Nat. Med. 2005, 11, 1180–1187. [Google Scholar] [CrossRef]
- Ank, N.; Petersen, K.; Malmgaard, L.; Mogensen, S.C.; Paludan, S.R. Age-dependent role for CCR5 in antiviral host defense against herpes simplex virus type 2. J. Virol. 2005, 79, 9831–9841. [Google Scholar] [CrossRef] [Green Version]
- Baturcam, E.; Abubaker, J.; Tiss, A.; Abu-Farha, M.; Khadir, A.; Al-Ghimlas, F.; Al-Khairi, I.; Cherian, P.; Elkum, N.; Hammad, M.; et al. Physical exercise reduces the expression of RANTES and its CCR5 receptor in the adipose tissue of obese humans. Mediat. Inflamm. 2014, 2014, 627150. [Google Scholar] [CrossRef] [PubMed]
- Hoff, P.; Belavý, D.L.; Huscher, D.; Lang, A.; Hahne, M.; Kuhlmey, A.K.; Maschmeyer, P.; Armbrecht, G.; Fitzner, R.; Perschel, F.H.; et al. Effects of 60-day bed rest with and without exercise on cellular and humoral immunological parameters. Cell. Mol. Immunol. 2015, 12, 483–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lederman, S.; Yellin, M.J.; Krichevsky, A.; Belko, J.; Lee, J.J.; Chess, L. Identification of a Novel Surface Protein on Activated CD4+ T Cells That Induces Contact-dependent B Cell Differentiation (Help). J. Exp. Med. 1992, 175, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Cleary, A.M.; Fortune, S.M.; Yellin, M.J.; Chess, L.; Lederman, S. Opposing roles of CD95 (Fas/APO-1) and CD40 in the death and rescue of human low density tonsillar B cells. J. Immunol. 1995, 155, 3329–3337. [Google Scholar]
- Szmitko, P.E.; Wang, C.H.; Weisel, R.D.; de Almeida, J.R.; Anderson, T.J.; Verma, S. New markers of inflammation and endothelial cell activation: Part, I. Circulation 2003, 108, 1917–1923. [Google Scholar] [CrossRef]
- Stout, R.D.; Suttles, J.; Xu, J.; Grewal, I.S.; Flavell, R.A. Impaired T cell-mediated macrophage activation in CD40 ligand-deficient mice. J. Immunol. 1996, 156, 8–11. [Google Scholar]
- Wang, J.H.; Zhang, Y.W.; Zhang, P.; Deng, B.Q.; Ding, S.; Wang, Z.K.; Wu, T.; Wang, J. CD40 ligand as a potential biomarker for atherosclerotic instability. Neurol. Res. 2013, 35, 693–700. [Google Scholar] [CrossRef] [Green Version]
- Grewal, I.S.; Xu, J.; Flavell, R.A. Impairment of antigen-specific T-cell priming in mice lacking CD40 ligand. Nature 1995, 378, 617–620. [Google Scholar] [CrossRef]
- Sia, J.K.; Bizzell, E.; Madan-Lala, R.; Rengarajan, J. Engaging the CD40-CD40L pathway augments T-helper cell responses and improves control of Mycobacterium tuberculosis infection. PLoS Pathog. 2017, 13, e1006530. [Google Scholar] [CrossRef]
- Chamekh, M. CD40-CD40L interaction in immunity against protozoan infections. J. Biomed. Biotechnol. 2007, 2007, 59430. [Google Scholar] [CrossRef]
- Thomsen, A.R.; Nansen, A.; Christensen, J.P.; Andreasen, S.Ø.; Marker, O. CD40 ligand is pivotal to efficient control of virus replication in mice infected with lymphocytic choriomeningitis virus. J. Immunol. 1998, 161, 4583–4590. [Google Scholar] [PubMed]
- Geertsema, L.; Lucas, S.J.; Cotter, J.D.; Hock, B.; McKenzie, J.; Fernyhough, L.J. The cardiovascular risk factor, soluble CD40 ligand (CD154), but not soluble CD40 is lowered by ultra-endurance exercise in athletes. Br. J. Sports Med. 2011, 45, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Bjørnstad, H.H.; Bruvik, J.; Bjørnstad, A.B.; Hjellestad, B.L.; Damås, J.K.; Aukrust, P. Exercise training decreases plasma levels of soluble CD40 ligand and P-selectin in patients with chronic heart failure. Eur. J. Cardiovasc. Prev. Rehabil. 2008, 15, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Schönbauer, R.; Lichtenauer, M.; Paar, V.; Emich, M.; Fritzer-Szekeres, M.; Schukro, C.; Strametz-Juranek, J.; Sponder, M. Regular Training Increases sTWEAK and Its Decoy Receptor sCD163-Does Training Trigger the sTWEAK/sCD163-Axis to Induce an Anti-Inflammatory Effect? J. Clin. Med. 2020, 9, 1899. [Google Scholar] [CrossRef]
- Sponder, M.; Campean, I.A.; Emich, M.; Fritzer-Szekeres, M.; Litschauer, B.; Graf, S.; Dalos, D.; Strametz-Juranek, J. Long-term physical activity leads to a significant increase in serum sRAGE levels: A sign of decreased AGE-mediated inflammation due to physical activity? Heart Vessels 2018, 33, 893–900. [Google Scholar] [CrossRef] [Green Version]
- Lenz, M.; Schönbauer, R.; Stojkovic, S.; Lichtenauer, M.; Paar, V.; Gatterer, C.; Schukro, C.; Emich, M.; Fritzer-Szekeres, M.; Strametz-Juranek, J.; et al. Long-term physical activity modulates adipsin and ANGPTL4 serum levels, a potential link to exercise-induced metabolic changes. Panminerva Med. 2021. [Google Scholar] [CrossRef]
- Du Bois, D.; Du Bois, E.F. A formula to estimate the approximate surface area if height and weight be known. 1916. Nutrition 1989, 5, 303–311. [Google Scholar]
- Abubaker, J.; Tiss, A.; Abu-Farha, M.; Al-Ghimlas, F.; Al-Khairi, I.; Baturcam, E.; Cherian, P.; Elkum, N.; Hammad, M.; John, J.; et al. DNAJB3/HSP-40 cochaperone is downregulated in obese humans and is restored by physical exercise. PLoS ONE 2013, 8, e69217. [Google Scholar] [CrossRef] [Green Version]
- Henderson, S.A.; Graham, H.K.; Mollan, R.A.; Riddoch, C.; Sheridan, B.; Johnston, H. Calcium homeostasis and exercise. Int. Orthop. 1989, 13, 69–73. [Google Scholar] [CrossRef]
- Dick, S.A.; Epelman, S. Chronic Heart Failure and Inflammation: What Do We Really Know? Circ. Res. 2016, 119, 159–176. [Google Scholar] [CrossRef] [Green Version]
- Schmid, A.; Bala, M.; Leszczak, S.; Ober, I.; Buechler, C.; Karrasch, T. Pro-inflammatory chemokines CCL2, chemerin, IP-10 and RANTES in human serum during an oral lipid tolerance test. Cytokine 2016, 80, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Bursill, C.A.; Castro, M.L.; Beattie, D.T.; Nakhla, S.; van der Vorst, E.; Heather, A.K.; Barter, P.J.; Rye, K.A. High-density lipoproteins suppress chemokines and chemokine receptors in vitro and in vivo. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1773–1778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steven, S.; Dib, M.; Hausding, M.; Kashani, F.; Oelze, M.; Kröller-Schön, S.; Hanf, A.; Daub, S.; Roohani, S.; Gramlich, Y.; et al. CD40L controls obesity-associated vascular inflammation, oxidative stress, and endothelial dysfunction in high fat diet-treated and db/db mice. Cardiovasc. Res. 2018, 114, 312–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group α | Group β | Group γ | Group δ | Total Cohort | |
|---|---|---|---|---|---|
| Parameters: | Gain ≤ 2.9% (n = 9) | Gain > 2.9% (n = 32) | Gain ≤ 2.9% (n = 18) | Gain > 2.9% (n = 39) | (n = 98) |
| Age (years) | 50.3 ± 6.1 | 48.6 ± 7.9 | 50.4 ± 6.5 | 49.1 ± 6.0 | 49.3 ± 6.7 |
| Female sex (%) | 55.6% | 46.9% | 38.9% | 28.2% | 38.8% |
| Performance baseline (%) | 87.4% ± 9.9% | 88.8% ± 7.1% | 122.0% ± 16.8% | 116.0% ± 15.9% | 105.6% ± 19.7% |
| Performance study end (%) | 87.0% ± 9.1% | 101.0% ± 10.0% | 118.2% ± 18.0% | 128.2% ± 15.6% | 113.7% ± 20.0% |
| Performance gain (%) | −2.7% ± 4.3% | 12.2% ± 7.1% | −3.8% ± 4.9% | 12.1% ± 5.6% | 7.8% ± 9.1% |
| Body composition: | |||||
| BMI (kg/m2) | 27.8 ± 4.2 | 28.5 ± 5.2 | 27.2 ± 3.8 | 26.8 ± 3.3 | 27.5 ± 4.2 |
| End of study BMI (kg/m2) | 27.7 ± 4.6 | 28.2 ± 4.8 | 27.3 ± 4.1 | 26.7 ± 3.2 | 27.4 ± 4.1 |
| Body fat (%) | 33.9% ± 3.3% | 31.6% ± 6.7% | 26.8% ± 9.1% | 27.8% ± 11.8% | 29.4% ± 9.5% |
| End of study body fat (%) | 31.5% ± 6.1% | 29.7% ± 7.3% | 26.7% ± 8.3% | 23.4% ± 8.41% | 26.3% ± 8.3% |
| Body muscle (%) | 32.2% ± 3.7% | 33.9% ± 4.1% | 34.3% ± 3.8% | 36.1% ± 4.0% | 34.7% ± 4.1% |
| End of study body muscle (%) | 32.4% ± 3.3% | 34.3% ± 4.5% | 34.4% ± 3.9% | 36.2% ± 3.9% | 34.9% ± 4.2% |
| Body water (%) | 48.6% ± 2.4% | 50.3% ± 4.9% | 53.8% ± 6.7% | 54.2% ± 5.9% | 52.3% ± 5.9% |
| End of study body water (%) | 50.4% ± 4.5% | 52.1% ± 5.5% | 53.9% ± 6.1% | 56.3% ± 6.2% | 53.9% ± 4.2% |
| Risk factors: | |||||
| Pack years | 22.4 ± 21.4 | 18.9 ± 15.8 | 12.2 ± 9.2 | 16.3 ± 14.6 | 17.1 ± 14.9 |
| Diabetes mellitus (%) | 11.1% | 3.1% | 5.6% | 0.0% | 3.1% |
| Hypertension (%) | 33.3% | 43.8% | 33.3% | 23.1% | 32.7% |
| Dyslipidemia (%) | 33.3% | 25.0% | 38.9% | 28.2% | 29.6% |
| Overweight (%) | 66.8% | 68.8% | 66.7% | 63.2% | 65.9% |
| Positive cardiac history (%) | 11.1% | 15.6% | 5.6% | 23.1% | 16.3% |
| Positive family history (%) | 66.8% | 43.8% | 50.0% | 38.5% | 44.9% |
| Laboratory values: | |||||
| Creatinine (mg/dL) | 0.8 ± 0.1 | 0.8 ± 0.2 | 0.9 ± 0.2 | 0.9 ± 0.2 | 0.9 ± 0.2 |
| Triglycerides (mg/dL) | 154 ± 86 | 149 ± 100 | 111 ± 72 | 119 ± 62 | 131 ± 81 |
| HDL-cholesterol (mg/dL) | 52 ± 19 | 56 ± 22 | 62 ± 12 | 60 ± 15 | 59 ± 17 |
| LDL-cholesterol (mg/dL) | 126 ± 50 | 117 ± 32 | 112 ± 29 | 116 ± 35 | 117 ± 34 |
| HbA1c (rel.%) | 5.5% ± 0.4% | 5.4% ± 0.8% | 5.5% ± 0.9% | 5.2% ± 0.3% | 5.3% ± 0.6% |
| proBNP (pg/mL) | 39 ± 27 | 59 ± 54 | 50 ± 35 | 32 ± 21 | 45 ± 39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenz, M.; Schönbauer, R.; Stojkovic, S.; Lee, J.; Gatterer, C.; Lichtenauer, M.; Paar, V.; Emich, M.; Fritzer-Szekeres, M.; Strametz-Juranek, J.; et al. RANTES and CD40L under Conditions of Long-Term Physical Exercise: A Potential Link to Adaptive Immunity. Int. J. Environ. Res. Public Health 2022, 19, 8658. https://doi.org/10.3390/ijerph19148658
Lenz M, Schönbauer R, Stojkovic S, Lee J, Gatterer C, Lichtenauer M, Paar V, Emich M, Fritzer-Szekeres M, Strametz-Juranek J, et al. RANTES and CD40L under Conditions of Long-Term Physical Exercise: A Potential Link to Adaptive Immunity. International Journal of Environmental Research and Public Health. 2022; 19(14):8658. https://doi.org/10.3390/ijerph19148658
Chicago/Turabian StyleLenz, Max, Robert Schönbauer, Stefan Stojkovic, Jonghui Lee, Constantin Gatterer, Michael Lichtenauer, Vera Paar, Michael Emich, Monika Fritzer-Szekeres, Jeanette Strametz-Juranek, and et al. 2022. "RANTES and CD40L under Conditions of Long-Term Physical Exercise: A Potential Link to Adaptive Immunity" International Journal of Environmental Research and Public Health 19, no. 14: 8658. https://doi.org/10.3390/ijerph19148658